
Follow up of the Humoral Response in Healthcare Workers after the Administration of Two Dose of the Anti SARS-CoV-2 Vaccines—Effectiveness in Delta Variant Breakthrough Infections

 , , and
, , and 
Abstract
:1. Introduction
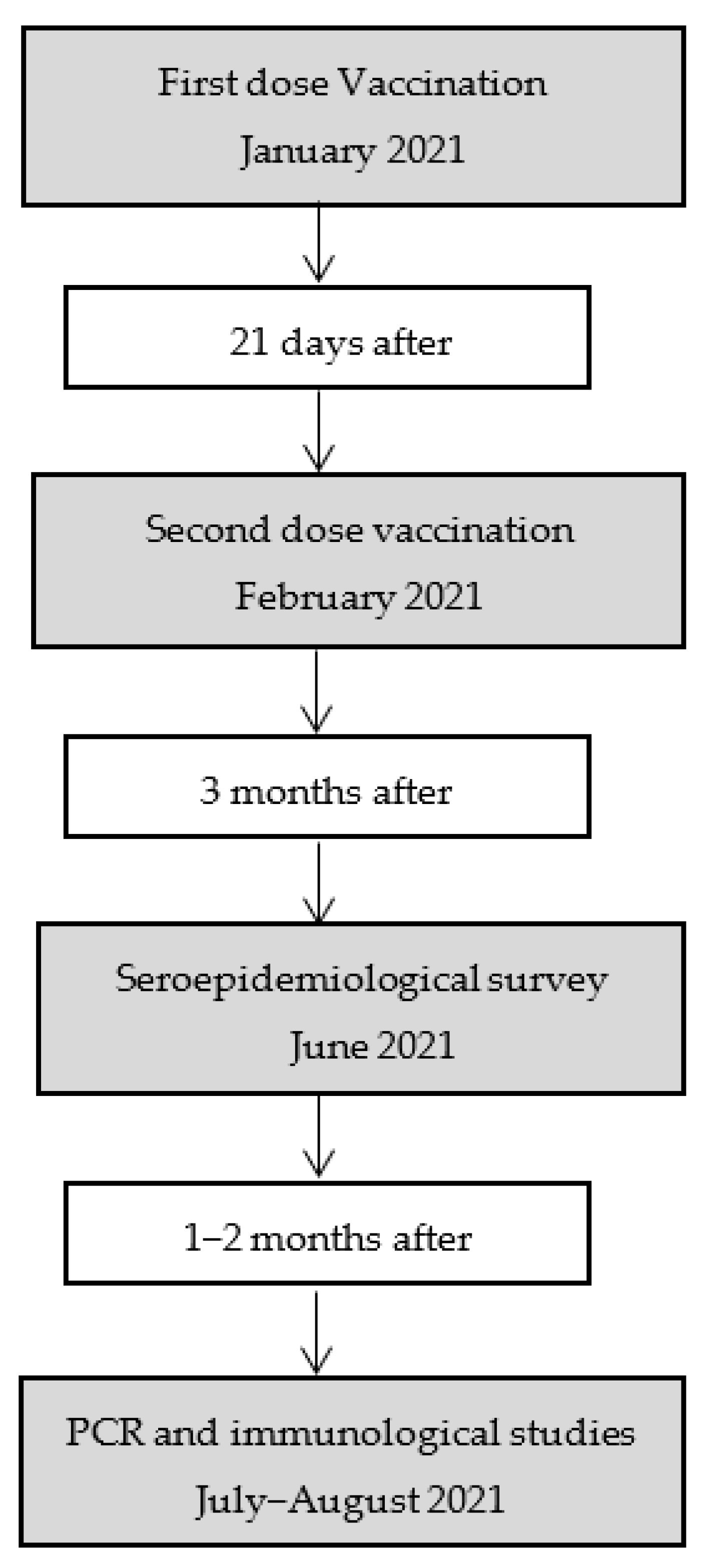
2. Material and Methods
2.1. Laboratory Analysis
2.2. Statistical Analysis
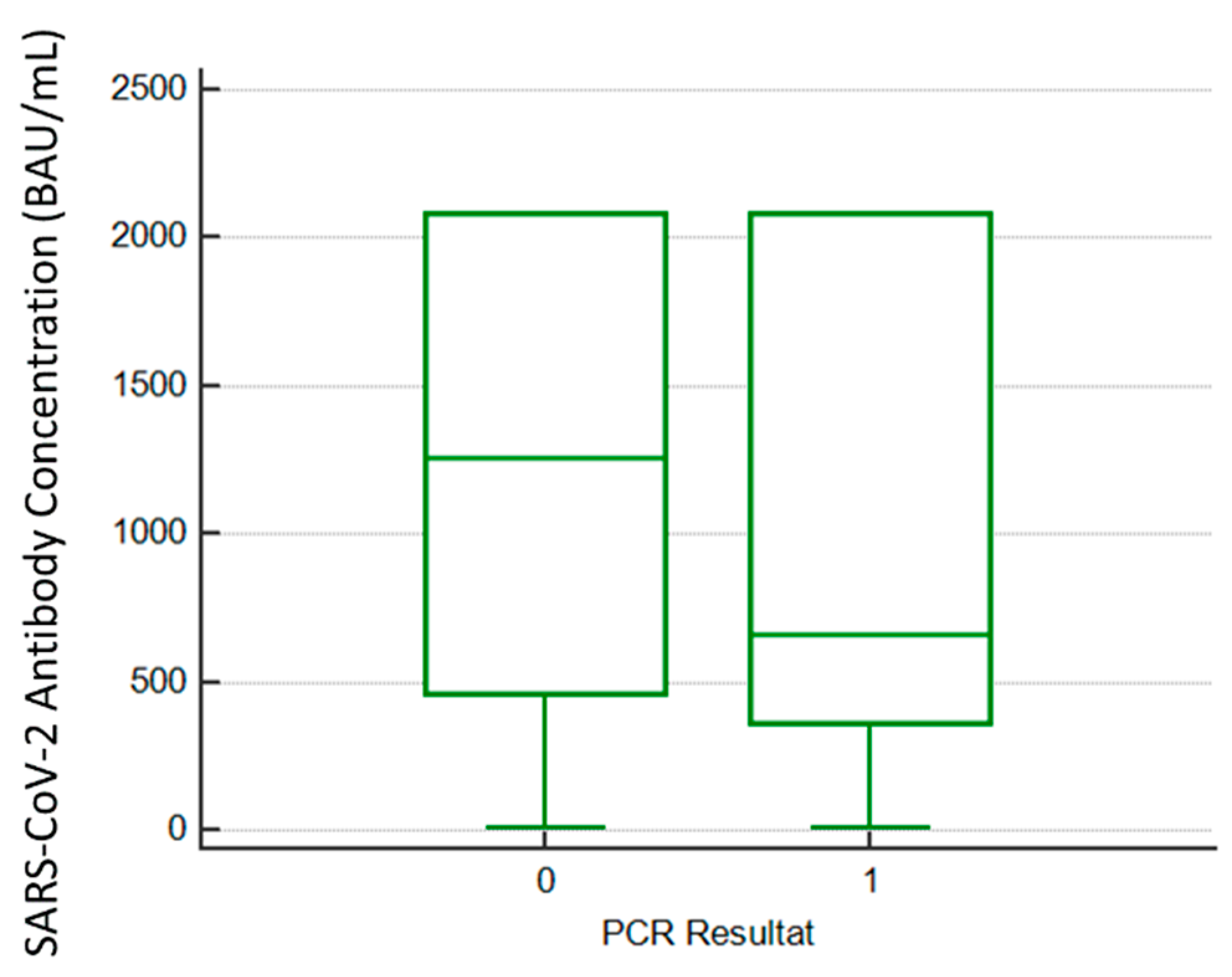
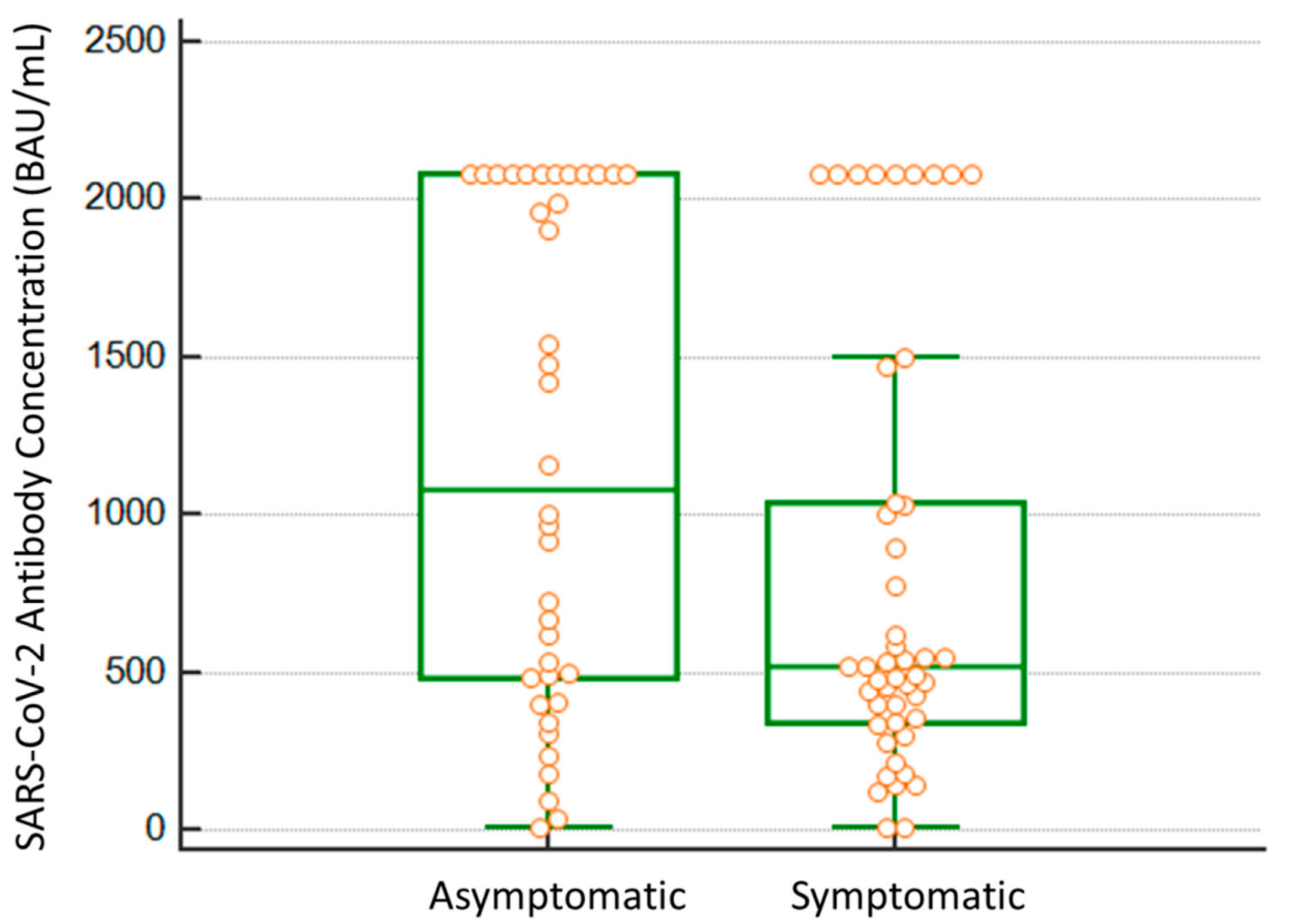
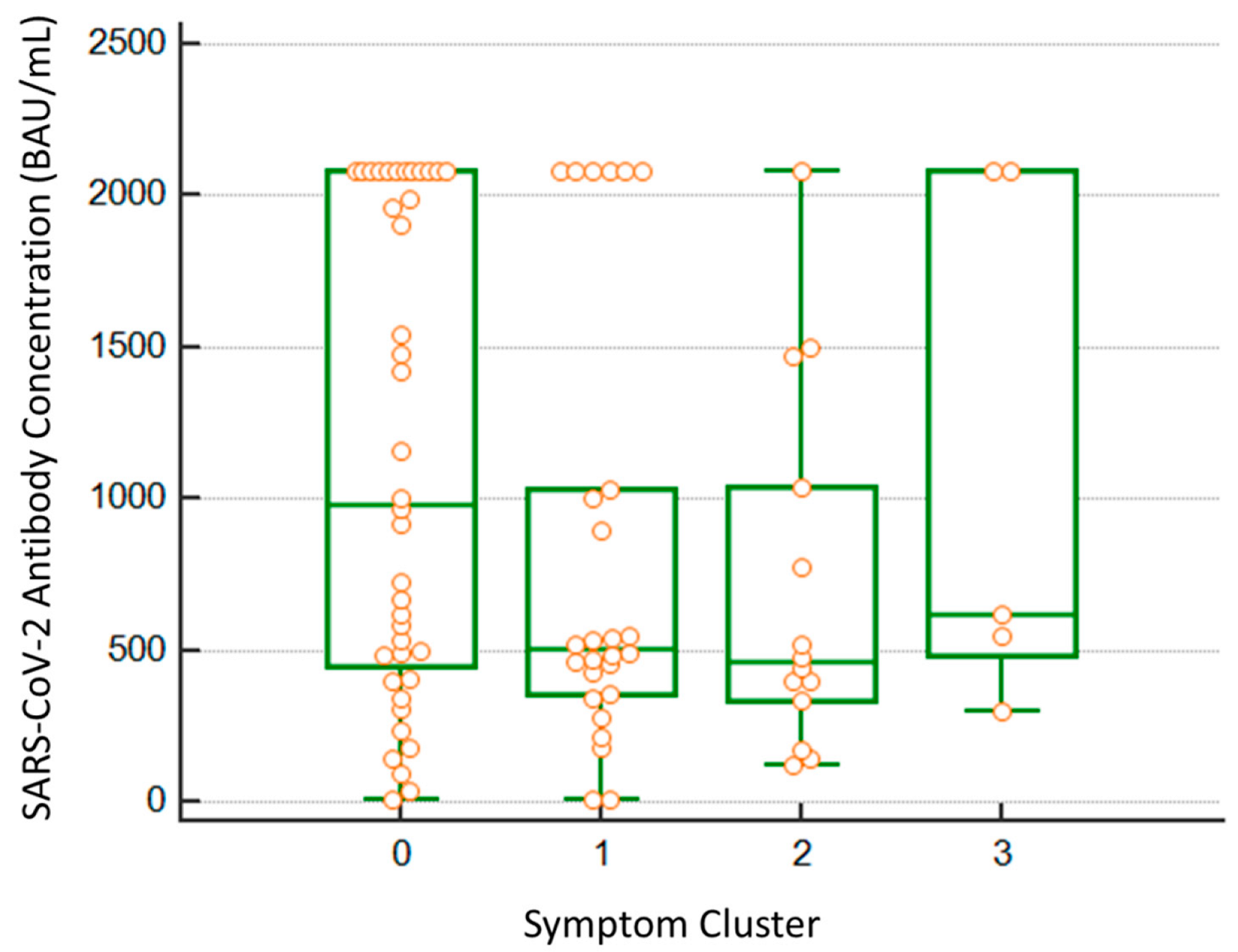
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jalkanen, P.; Kolehmainen, P.; Häkkinen, H.K.; Huttunen, M.; Tähtinen, P.A.; Lundberg, R.; Maljanen, S.; Reinholm, A.; Tauriainen, S.; Pakkanen, S.H.; et al. COVID-19 mRNA vaccine induced antibody responses against three SARS-CoV-2 variants. Nat. Commun. 2021, 12, 3991. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Silva, J.; Reis, T.; Lopes, C.; Batista-Silva, R.; Ribeiro, R.; Marques, G.; Pacheco, V.; Rodrigues, T.; Afonso, A.; Pinheiro, V.; et al. Humoral response to the SARS-CoV-2 BNT162b2 mRNA vaccine: Real-world data from a large cohort of healthcare workers. Vaccine 2022, 40, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody persistence through 6 months after the second dose of mRNA-1273 vaccine for COVID-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef] [PubMed]
- Barouch, D.H.; Stephenson, K.E.; Sadoff, J.; Yu, J.; Chang, A.; Gebre, M.; McMahan, K.; Liu, J.; Chandrashekar, A.; Patel, S.; et al. Durable humoral and cellular immune responses 8 months after Ad26.COV2.S vaccination. N. Engl. J. Med. 2021, 385, 951–953. [Google Scholar] [CrossRef]
- Barallat, J.; Fernández-Rivas, G.; Quirant-Sánchez, B.; González, V.; Doladé, M.; Martinez-Caceres, E.; Piña, M.; Matllo, J.; Estrada, O.; Blanco, I. Seroprevalence of SARSCoV-2 IgG specific antibodies among healthcare workers in the Northern Metropolitan Area of Barcelona, Spain, after the first pandemic wave. PLoS ONE 2020, 15, e0244348. [Google Scholar] [CrossRef]
- Rose, R.; Neumann, F.; Grobe, O.; Lorentz, T.; Fickenscher, H.; Krumbholz, A. Humoral immune response after different SARS-CoV-2 vaccination regimens. BMC Med. 2022, 20, 31. [Google Scholar] [CrossRef]
- Naranbhai, V.; St Denis, K.J.; Lam, E.C.; Ofoman, O.; Garcia-Beltran, W.F.; Mairena, C.B.; Bhan, A.K.; Gainor, J.F.; Balazs, A.B.; Iafrate, A.J.; et al. Neutralization breadth of SARS-CoV-2 viral variants following primary series and booster SARS-CoV-2 vaccines in patients with cancer. Cancer Cell 2022, 40, 103–108.e2. [Google Scholar] [CrossRef]
- Nevermann, N.; Wiering, L.; Wu, H.; Moroder, P.; Brandl, A.; Globke, B.; Krenzien, F.; Raschzok, N.; Schöning, W.; Lurje, G.; et al. Transplantation programs facing lack of empirical evidence on SARS-CoV-2 vaccination: A society recommendation consensus update. Transpl. Infect. Dis. 2021, 23, e13696. [Google Scholar] [CrossRef]
- Spiera, R.; Jinich, S.; Jannat-Khah, D. Rituximab, but not other antirheumatic therapies, is associated with impaired serological response to SARS- CoV-2 vaccination in patients with rheumatic diseases. Ann. Rheum. Dis. 2021, 80, 1357–1359. [Google Scholar] [CrossRef]
- Bouton, T.C.; Lodi, S.; Turcinovic, J.; Weber, S.E.; Quinn, E.; Korn, C.; Steiner, J.; Schechter-Perkins, E.M.; Duffy, E.; Ragan, E.J.; et al. COVID-19 vaccine impact on rates of SARS-CoV-2 cases and post vaccination strain sequences among healthcare workers at an urban academic medical center: A prospective cohort study. Open Forum Infect. Dis. 2021, 8, ofab465. [Google Scholar] [CrossRef]
- Núñez López, C.; González de Abreu, J.M.; Pérez-Blanco, V.; de Miguel Buckley, R.; Romero Gómez, M.P.; Díaz-Menéndez, M.; La Paz Health Care Workers Vaccination Study Group. Effectiveness of the BNT162b2 mRNA COVID-19 vaccine in Spanish healthcare workers. Enferm. Infecc. Microbiol. Clín. 2021. [Google Scholar] [CrossRef]
- Kilpeläinen, A.; Jimenez-Moyano, E.; Blanch-Lombarte, O.; Ouchi, D.; Peña, R.; Quirant-Sanchez, B.; Chamorro, A.; Blanco, I.; Martínez-Caceres, E.; Paredes, R.; et al. Highly Functional Cellular Immunity in SARS-CoV-2 Non-Seroconvertors is Associated with Immune Protection. Available online: https://www.biorxiv.org/content/10.1101/2021.05.04.438781v1 (accessed on 4 April 2022).
- Mateus, J.; Dan, J.M.; Zhang, Z.; Rydyznski Moderbacher, C.; Lammers, M.; Goodwin, B.; Sette, A.; Crotty, S.; Weiskopf, D. Low-dose mRNA-1273 COVID-19 vaccine generates durable memory enhanced by cross-reactive T cells. Science 2021, 374, eabj9853. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.D.; Wang, E.; Garrigan, E.; Goodwin, B.; Sutherland, A.; Tarke, A.; Chang, J.; Gálvez, R.I.; Mateus, J.; Ramirez, S.I.; et al. Development of a T cell-based immunodiagnostic system to effectively distinguish SARS-CoV-2 infection and COVID-19 vaccination status. Cell Host Microbe 2022, 30, 388–399.e3. [Google Scholar] [CrossRef]
- Mateus, J.; Grifoni, A.; Tarke, A.; Sidney, J.; Ramirez, S.I.; Dan, J.M.; Burger, Z.C.; Rawlings, S.A.; Smith, D.M.; Phillips, E.; et al. Selective and cross-reactive SARSCoV-2 T cell epitopes in unexposed humans. Science 2020, 370, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Tarke, A.; Sidney, J.; Kidd, C.K.; Dan, J.M.; Ramirez, S.I.; Yu, E.D.; Mateus, J.; da Silva Antunes, R.; Moore, E.; Rubiro, P.; et al. Comprehensive analysis of T cell immunodominance and immunoprevalence of SARS-CoV-2 epitopes in COVID-19 cases. Cell Rep. Med. 2021, 2, 100204. [Google Scholar] [CrossRef] [PubMed]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Gal Levin, E.; Rubin, C.; Indenbaum, V.; et al. COVID-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1629–1630. [Google Scholar] [CrossRef]
- First WHO International Standard for anti-SARS-CoV-2 Immunoglobulin (Human). NIBSC code: 20/136. Instructions for Use (Version 2.0, Dated 17 December 2020). Available online: https://www.nibsc.org/documents/ifu/20-136.pdf (accessed on 2 December 2021).
- Ten Brinke, A.; Marek-Trzonkowska, N.; Mansilla, M.J.; Turksma, A.W.; Piekarska, K.; Iwaszkiewicz-Grześ, D.; Passerini, L.; Locafaro, G.; Puñet-Ortiz, J.; van Ham, S.M.; et al. Monitoring T-cell responses in translational studies: Optimization of dye-based proliferation assay for evaluation of antigen-specific responses. Front. Immunol. 2017, 8, 1870. [Google Scholar] [CrossRef]
- Overview of Testing for SARS-CoV-2 (COVID-19). Centers for the Diseases Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html#print (accessed on 16 December 2021).
- Chvatal-Medina, M.; Mendez-Cortina, Y.; Patiño, P.J.; Velilla, P.A.; Rugeles, M.T. Antibody responses in COVID-19: A review. Front. Immunol. 2021, 12, 633184. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef]
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.W. Omicron variant (B.1.1.529): Infectivity, vaccine breakthrough, and antibody resistance. J. Chem. Inf. Model. 2022, 62, 412–422. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.L.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.; Lutrick, K.; et al. Interim estimates of vaccine effectiveness of BNT162b2 and mRNA-1273 COVID-19 vaccines in preventing SARS-CoV-2 infection among health care personnel, first responders, and other essential and frontline workers—Eight U.S. locations, December 2020–March 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Nanduri, S.; Pilishvili, T.; Derado, G.; Soe, M.M.; Dollard, P.; Wu, H.; Li, Q.; Bagchi, S.; Dubendris, H.; Link-Gelles, R.; et al. Effectiveness of pfizer-bioNTech and moderna vaccines in preventing SARS-CoV-2 infection among nursing home residents before and during widespread circulation of the SARS-CoV-2 B.1.617.2 (delta) variant—National healthcare safety network, 1 March–1 August 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1163–1166. [Google Scholar] [CrossRef]
- Kertes, J.; Gez, S.B.; Saciuk, Y.; Supino-Rosin, L.; Stein, N.S.; Mizrahi-Reuveni, M.; Zohar, A.E. Effectiveness of mRNA BNT162b2 vaccine 6 months after vaccination among patients in large health maintenance organization, Israel. Emerg. Infect. Dis. 2022, 28, 338–346. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Kristiansen, P.A.; Page, M.; Bernasconi, V.; Mattiuzzo, G.; Dull, P.; Makar, K.; Plotkin, S.; Knezevic, I. WHO international standard for anti-SARS-CoV-2 immunoglobulin. Lancet 2021, 397, 1347–1348. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a fourth dose of COVID-19 mRNA vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants n (%) | |
|---|---|
| Sex | |
| Male | 959 (19.18) |
| Female | 4019 (80.38) |
| Not informed | 22 (0.44) |
| Age | |
| 18–34 | 1309 (26.18) |
| 35–54 | 2246 (44.92) |
| ≥55 | 961 (19.22) |
| Not informed | 484 (9.68) |
| Job Location | |
| Primary Care * | 2556 (51.12) |
| Tertiary Care ** | 2444 (48.88) |
| Health Care position | |
| Nurse | 1681 (33.62) |
| Physician | 914 (18.28) |
| Health Care Support Services | 755 (15.1) |
| Laboratory Technician | 252 (5.04) |
| Administrative Healthcare | 996 (19.92) |
| Other | 395 (7.9) |
| Not informed | 7 (0.14) |
| Previous COVID-19 Diagnosis | |
| Yes | 828 (16.56) |
| No | 4139 (82.78) |
| N/A | 33 (0.66) |
| Type of vaccine | |
| Pfizer | 4519 (90.38) |
| Moderna | 285 (5.7) |
| Others | 10 (0.2) |
| Not informed | 186 (3.72) |
| Vaccination Dosages | |
| One | 166 (3.32) |
| Complete (2 doses) | 4368 (87.36) |
| Not vaccination | 182 (3.64) |
| Not informed | 284 (5.68) |
| Category | N | % |
|---|---|---|
| No symptoms | 40 | 47.1 |
| ‘Flu-Like’ with fever | 26 | 30.6 |
| ‘Flu-Like’ no fever | 14 | 16.5 |
| Gastrointestinal | 5 | 5.9 |
| Participant 1 | Participant 2 | Reference Values | ||
|---|---|---|---|---|
| Min. | Max. | |||
| Total lymphocytes (cell/uL) | 1700 | 1200 | 1200 | 3500 |
| CD19+ lymphocytes (cell/uL) | 58 | 58 | 100 | 500 |
| CD19+ lymphocytes (%) | 3.4 | 4.8 | 6 | 19 |
| CD3+ lymphocytes (cell/uL) | 1027 | 628 | 700 | 2100 |
| CD3+ lymphocytes (%) | 60.4 | 52.3 | 55 | 83 |
| CD4+ lymphocytes (cell/uL) | 493 | 416 | 700 | 1800 |
| CD4+ lymphocytes (%) | 29 | 34.7 | 30 | 50 |
| CD8+ lymphocytes (cell/uL) | 332 | 188 | 430 | 1500 |
| CD8+ lymphocytes (%) | 19.5 | 15.7 | 18 | 40 |
| IgG immunoglobulin | 339 | 621 | 700 | 1400 |
| IgA immunoglobulin | 45 | 150 | 70 | 400 |
| IgM immunoglobulin | 41 | 30 | 40 | 230 |
| SARS-CoV-2 T cell reactivity | Positive | Positive | Absence | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Rivas, G.; Barallat, J.; Quirant-Sánchez, B.; González, V.; Doladé, M.; Martinez-Caceres, E.; Piña, M.; Matllo, J.; Blanco, I.; Cardona, P.-J. Follow up of the Humoral Response in Healthcare Workers after the Administration of Two Dose of the Anti SARS-CoV-2 Vaccines—Effectiveness in Delta Variant Breakthrough Infections. Viruses 2022, 14, 1385. https://doi.org/10.3390/v14071385
Fernández-Rivas G, Barallat J, Quirant-Sánchez B, González V, Doladé M, Martinez-Caceres E, Piña M, Matllo J, Blanco I, Cardona P-J. Follow up of the Humoral Response in Healthcare Workers after the Administration of Two Dose of the Anti SARS-CoV-2 Vaccines—Effectiveness in Delta Variant Breakthrough Infections. Viruses. 2022; 14(7):1385. https://doi.org/10.3390/v14071385
Chicago/Turabian StyleFernández-Rivas, Gema, Jaume Barallat, Bibiana Quirant-Sánchez, Victoria González, María Doladé, Eva Martinez-Caceres, Monica Piña, Joan Matllo, Ignacio Blanco, and Pere-Joan Cardona. 2022. "Follow up of the Humoral Response in Healthcare Workers after the Administration of Two Dose of the Anti SARS-CoV-2 Vaccines—Effectiveness in Delta Variant Breakthrough Infections" Viruses 14, no. 7: 1385. https://doi.org/10.3390/v14071385
APA StyleFernández-Rivas, G., Barallat, J., Quirant-Sánchez, B., González, V., Doladé, M., Martinez-Caceres, E., Piña, M., Matllo, J., Blanco, I., & Cardona, P. -J. (2022). Follow up of the Humoral Response in Healthcare Workers after the Administration of Two Dose of the Anti SARS-CoV-2 Vaccines—Effectiveness in Delta Variant Breakthrough Infections. Viruses, 14(7), 1385. https://doi.org/10.3390/v14071385