
Systemic Autoimmune Diseases in Patients Hospitalized with COVID-19 in Spain: A Nation-Wide Registry Study

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Outcomes and Mortality Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 39, 1513–1536. [Google Scholar] [CrossRef]
- Moreno-Torres, V.; Muñoz-Serrano, A.; Calderón-Parra, J.; Mills-Sánchez, P.; Pintos-Pascual, I.; Rodríguez-Olleros, C.; Ibánez-Estéllez, F.; Tung-Chen, Y.; Ramos-Martínez, A.; A Vargas-Núñez, J.; et al. Mortality by COVID-19 Before Vaccination—One Year Experience of Hospitalized Patients in Madrid. Int. J. Infect. Dis. 2022, 116, 339–343. [Google Scholar] [CrossRef]
- Graselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Torres, V.; de la Fuente, S.; Mills, P.; Muñoz, A.; Muñez, E.; Ramos, A.; Fernández-Cruz, A.; Arias, A.; Pintos, I.; Vargas, J.A.; et al. Major determinants of death in patients hospitalized with COVID-19 during the first epidemic wave in Madrid, Spain. Medicine 2021, 100, e25634. [Google Scholar] [CrossRef] [PubMed]
- Minotti, C.; Tirelli, F.; Barbieri, E.; Giaquinto, C.; Donà, D. How is immunosuppressive status affecting children and adults in SARS-CoV-2 infection? A Syst. Rev. J. Infect. 2020, 81, e61–e66. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Urbistondo, M.; Gutiérrez-Rojas, Á.; Andrés, A.; Gutiérrez, I.; Escudero, G.; García, S.; Gutiérrez, A.; Sánchez, E.; Herráiz, J.; De La Fuente, S.; et al. Severe Lymphopenia as a Predictor of COVID-19 Mortality in Immunosuppressed Patients. J. Clin. Med. 2021, 10, 3595. [Google Scholar] [CrossRef] [PubMed]
- Bellou, V.; Tzoulaki, I.; van Smeden, M.; Moons, K.G.M.; Evangelou, E.; Belbasis, L. Prognostic factors for adverse outcomes in patients with COVID-19: A field-wide systematic review and meta-analysis. Eur. Respir. J. 2022, 59, 2002964. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. BACC Bay Tocilizumab Trial Investigators. Efficacy of Tocilizumab in Patients Hospitalized with COVID-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Antorán, B.; Sancho-López, A.; Torres, F.; Moreno-Torres, V.; de Pablo-López, I.; García-López, P.; Abad-Santos, F.; Rosso-Fernández, C.M.; Aldea-Perona, A.; Montané, E.; et al. TOCICOV-study group. Combination of Tocilizumab and Steroids to Improve Mortality in Patients with Severe COVID-19 Infection: A Spanish, Multicenter, Cohort Study. Infect. Dis. Ther 2021, 10, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Parra, J.; Cuervas-Mons, V.; Moreno-Torres, V.; Moreno-Torres, V.; de Pablo-López, I.; García-López, P.; Abad-Santos, F.; Rosso-Fernández, C.M.; Aldea-Perona, A.; Méndez-Bailón, M.; et al. SEMI-COVID-19 Network. Influence of chronic use of corticosteroids and calcineurin inhibitors on COVID-19 clinical outcomes: Analysis of a nationwide registry. Int. J. Infect. Dis. 2022, 116, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Wahren-Herlenius, M.; Dörner, T. Immunopathogenic mechanisms of systemic autoimmune disease. Lancet 2013, 382, 819–831. [Google Scholar] [CrossRef]
- Rigante, D.; Esposito, S. Infections and Systemic Lupus Erythematosus: Binding or Sparring Partners? Int. J. Mol. Sci 2015, 16, 17331–17343. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Sanidad. Servicios Sociales e Igualdad. Real decreto 69/2015, de 6 febrero, por el que se regula el Registro de Actividad Sanitaria Especializada. Boletín Del Estado 2015, 35, 1078–1080. Available online: http://www.boe.es/eli/es/rd/2015/02/06/69/con (accessed on 15 March 2022).
- Ramos-Rincon, J.M.; Menchi-Elanzi, M.; Pinargote-Celorio, H.; Mayoral, A.; González-Alcaide, G.; de Mendoza, C.; Barreiro, P.; Gómez-Gallego, F.; Corral, O.; Soriano, V. Trends in hospitalizations and deaths in HIV-infected patients in Spain over two decades. AIDS 2022, 36, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Torres, V.; Tarín, C.; Ruiz-Irastorza, G.; Castejón, R.; Gutiérrez-Rojas, A.; Royuela, A.; Campo, P.D.-D.; Mellor-Pita, S.; Tutor, P.; Rosado, S.; et al. Trends in hospital admissions and death causes in patients with systemic lupus erythematosus: Spanish National Registry. J. Clin. Med. 2021, 10, 5749. [Google Scholar] [CrossRef]
- Charlson, M.; Pompei, P.; Ales, K.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Huang, Y.; Chen, Z.; Wang, Y.; Han, L.; Qin, K.; Huang, W.; Huang, Y.; Wang, H.; Shen, P.; Ba, X.; et al. Clinical characteristics of 17 patients with COVID-19 and systemic autoimmune diseases: A retrospective study. Ann. Rheum. Dis. 2020, 79, 1163–1169. [Google Scholar] [CrossRef]
- Haberman, R.; Axelrad, J.; Chen, A.; Castillo, R.; Yan, D.; Izmirly, P.; Neimann, A.; Adhikari, S.; Hudesman, D.; Scher, J.U. COVID-19 in Immune-Mediated Inflammatory Diseases—Case Series from New York. N. Engl. J. Med. 2020, 383, 85–88. [Google Scholar] [CrossRef]
- Pablos, J.L.; Galindo, M.; Carmona, L.; Lledó, A.; Retuerto, M.; Blanco, R.; Gonzalez, A.; Martinez-Lopez, D.; Castrejón, I.; RIER Investigators Group; et al. Clinical outcomes of hospitalised patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: A multicentric matched cohort study. Ann. Rheum Dis. 2020, 79, 1544–1549. [Google Scholar] [CrossRef]
- Zhong, J.; Shen, G.; Yang, H.; Huang, A.; Chen, X.; Dong, L.; Wu, B.; Su, L.; Hou, X.; Song, S.; et al. COVID-19 in patients with rheumatic disease in Hubei province, China: A multicentre retrospective observational study. Lancet Rheumatol. 2020, 2, e557–e564. [Google Scholar] [CrossRef]
- Fredi, M.; Cavazzana, I.; Moschetti, L.; Andreoli, L.; Franceschini, F.; Brescia Rheumatology COVID-19 Study Group. COVID-19 in patients with rheumatic diseases in northern Italy: A single-centre observational and case-control study. Lancet Rheumatol. 2020, 2, e549–e556. [Google Scholar] [CrossRef]
- Gianfrancesco, M.; Hyrich, K.L.; Al-Adely, S.; Carmona, L.; I Danila, M.; Gossec, L.; Izadi, Z.; Jacobsohn, L.; Katz, P.; Lawson-Tovey, S.; et al. COVID-19 Global Rheumatology Alliance. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: Data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2020, 79, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Hasseli, R.; Mueller-Ladner, U.; Hoyer, B.F.; Krause, A.; Lorenz, H.-M.; Pfeil, A.; Richter, J.; Schäfer, M.; Schmeiser, T.; Strangfeld, A.; et al. Older age, comorbidity, glucocorticoid use and disease activity are risk factors for COVID-19 hospitalisation in patients with inflammatory rheumatic and musculoskeletal diseases. RMD Open 2021, 7, e001464. [Google Scholar] [CrossRef] [PubMed]
- D’Silva, K.M.; Jorge, A.; Cohen, A.; McCormick, N.; Zhang, Y.; Wallace, Z.S.; Choi, H.K. COVID-19 Outcomes in Patients with Systemic Autoimmune Rheumatic Diseases Compared to the General Population: A US Multicenter, Comparative Cohort Study. Arthritis Rheumatol. 2021, 73, 914–920. [Google Scholar] [CrossRef]
- Strangfeld, A.; Schäfer, M.; Gianfrancesco, M.A.; Lawson-Tovey, S.; Liew, J.W.; Ljung, L.; Mateus, E.F.; Richez, C.; Santos, M.J.; Schmajuk, G.; et al. COVID-19 Global Rheumatology Alliance. Factors associated with COVID-19-related death in people with rheumatic diseases: Results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2021, 80, 930–942. [Google Scholar] [CrossRef]
- Montero, F.; Martínez-Barrio, J.; Serrano-Benavente, B.; González, T.; Rivera, J.; Collada, J.M.; Castrejón, I.; Álvaro-Gracia, J. Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: Clinical characteristics of poor outcomes. Rheumatol. Int. 2020, 40, 1593–1598. [Google Scholar] [CrossRef]
- Ayala Gutiérrez, M.D.M.; Rubio-Rivas, M.; Romero Gómez, C.; Sáez, A.M.; de Pedro, I.P.; Homs, N.; García, B.A.; Carvajal, C.C.; Fernández, F.A.; Pérez, J.L.B.; et al. On Behalf of The Semi-COVID-Network. Autoimmune Diseases and COVID-19 as Risk Factors for Poor Outcomes: Data on 13,940 Hospitalized Patients from the Spanish Nationwide SEMI-COVID-19 Registry. J. Clin. Med. 2021, 10, 1844. [Google Scholar] [CrossRef]
- Santos, C.S.; Morales, C.M.; Álvarez, E.D.; Castro, C.Á.; Robles, A.L.; Sandoval, T.P. Determinants of COVID-19 disease severity in patients with underlying rheumatic disease. Clin. Rheumatol. 2020, 39, 2789–2796. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Bachiller-Corral, J.; Boteanu, A.; Garcia-Villanueva, M.J.; de la Puente, C.; Revenga, M.; Diaz-Miguel, M.C.; Rodriguez-Garcia, A.; Morell-Hita, J.L.; Valero, M.; Larena, C.; et al. Risk of Severe COVID-19 Infection in Patients With Inflammatory Rheumatic Diseases. J. Rheumatol. 2021, 48, 1098–1102. [Google Scholar] [CrossRef] [PubMed]
- Freites Nuñez, D.D.; Leon, L.; Mucientes, A.; Rodriguez-Rodriguez, L.; Urgelles, J.F.; García, A.M.; I Colomer, J.; A Jover, J.; Fernandez-Gutierrez, B.; Abasolo, L. Risk factors for hospital admissions related to COVID-19 in patients with autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 2020, 79, 1393–1399. [Google Scholar] [CrossRef] [PubMed]
- Bournia, V.K.; Fragoulis, G.E.; Mitrou, P.; Mathioudakis, K.; Tsolakidis, A.; Konstantonis, G.; Vourli, G.; Paraskevis, D.; Tektonidou, M.G.; Sfikakis, P.P. All-cause mortality in systemic rheumatic diseases under treatment compared with the general population, 2015–2019. RMD Open 2021, 7, e001694. [Google Scholar] [CrossRef] [PubMed]
- Mitratza, M.; Klijs, B.; Hak, A.E.; Kardaun, J.W.P.F.; Kunst, A.E. Systemic autoimmune disease as a cause of death: Mortality burden and comorbidities. Rheumatology 2021, 60, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Hyrich, K.L.; Machado, P.M. Rheumatic disease and COVID-19: Epidemiology and outcomes. Nat. Rev. Rheumatol. 2021, 17, 71–72. [Google Scholar] [CrossRef]
- Raiker, R.; Pakhchanian, H.; De Young, C.; Gupta, L.; Kardeş, S.; Ahmed, S.; Kavadichanda, C. Short term outcomes of COVID-19 in lupus: Propensity score matched analysis from a nationwide multi-centric research network. J. Autoimmu.n 2021, 125, 102730. [Google Scholar] [CrossRef]
- Brito-Zerón, P.; Gracia-Tello, B.; Robles, A.; Alguacil, A.; Bonet, M.; De-Escalante, B.; Noblejas-Mosso, A.; Gómez-De-La-Torre, R.; Akasbi, M.; Pérez-De-Lis, M.; et al. On Behalf of The SarcoGEAS-Semi Registry. Characterization and Outcomes of SARS-CoV-2 Infection in Patients with Sarcoidosis. Viruses 2021, 13, 1000. [Google Scholar] [CrossRef]
- Ruiz-Irastorza, G.; Bertsias, G. Treating systemic lupus erythematosus in the 21st century: New drugs and new perspectives on old drugs. Rheumatology 2020, 59, v69–v81. [Google Scholar] [CrossRef]
- Brito-Zerón, P.; Sisó-Almirall, A.; Flores-Chavez, A.; Retamozo, S.; Ramos-Casals, M. SARS-CoV-2 infection in patients with systemic autoimmune diseases. Clin. Exp. Rheumatol. 2021, 39, 676–687. [Google Scholar] [CrossRef]
- Calderón-Parra, J.; Múñez-Rubio, E.; Fernández-Cruz, A.; García-Sánchez, M.C.; Maderuelo-González, E.; López-Dosil, M.; Calvo-Salvador, M.; Baños-Pérez, I.; Valle-Falcones, M.; Ramos-Martínez, A. Incidence, clinical presentation, relapses and outcome of SARS-CoV-2 infection in patients treated with anti-CD20 monoclonal antibodies. Clin. Infect. Dis. 2022, 74, 1786–1794. [Google Scholar] [CrossRef]
- Barandalla, I.; Alvarez, C.; Barreiro, P.; de Mendoza, C.; González-Crespo, R.; Soriano, V. Impact of scaling up SARS-CoV-2 vaccination on COVID-19 hospitalizations in Spain. Int. J. Infect. Dis. 2021, 112, 81–88. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total N (%) | SADs N (%) | Non-SADs N (%) | p-Value | |
|---|---|---|---|---|
| COVID-19 hospitalized patients | 117,694 | 892 (0.8) | 116,802 (99.2) | |
| Mean age (mean, SD) | 66.5 (18) | 67.5 (15.6) | 66.5 (18) | 0.055 |
| Male sex N (%) | 66,685 (57) | 257 (29) | 66,428 (57) | <0.001 |
| Ethnicity | ||||
| Caucasian | 85,977 (73) | 667 (75) | 85,310 (73) | 0.256 |
| Arabic | 2786 (2) | 25 (3) | 2761 (2) | 0.380 |
| Black | 1592 () | 13 (2) | 1579 (1) | 0.770 |
| Asian | 387 (0.3) | 0 | 387 (0.3) | 0.129 |
| Latin-American | 9296 (8) | 54 (6) | 9242 (8) | 0.043 |
| Hindu | 156 (0.1) | 2 (0.2) | 154 (0.1) | 0.331 |
| Unknown | 17,500 (15) | 131 (15) | 17,369 (15) | 0.920 |
| Total N (%) | SADs N (%) | Non-SADs N (%) | p-Value | |
|---|---|---|---|---|
| High blood pressure | 56,701 (48) | 445 (50) | 56,256 (48) | 0.313 |
| Diabetes mellitus | 28,094 (24) | 184 (21) | 27,910 (24) | 0.023 |
| Uncomplicated | 18,595 (16) | 114 (13) | 18,481 (16) | 0.01 |
| End-organ damage | 9499 (8) | 70 (8) | 9429 (8) | 0.847 |
| Obesity | 13,966 (12) | 101 (11) | 13,865 (12) | 0.674 |
| Ischemic heart disease | 7858 (7) | 56 (6) | 7802 (7) | 0.680 |
| Heart failure | 14,199 (12) | 163 (18) | 14,036 (12) | <0.001 |
| Peripheral vascular disease | 5059 (4) | 68 (8) | 4991 (4) | <0.001 |
| CVA or TIA | 7308 (6) | 58 (7) | 7250 (6) | 0.683 |
| Hemiplejia | 1717 (2) | 11 (1) | 1706 (2) | 0.675 |
| Dementia | 10,146 (9) | 61 (7) | 10,085 (9) | 0.066 |
| Chronic lung disease | 16,814 (14) | 206 (23) | 16,608 (14) | <0.001 |
| Peptic ulcer disease | 341 (0.3) | 3 (0.3) | 338 (0.3) | 0.747 |
| Liver disease | 6001 (5) | 74 (8) | 5927 (5) | <0.001 |
| Mild | 4065 (4) | 61 (7) | 4867 (4) | <0.001 |
| Moderate to severe | 1073 (1) | 13 (2) | 1060 (1) | 0.106 |
| Chronic kidney disease | 13,232 (11) | 160 (18) | 13,072 (11) | <0.001 |
| Localized solid tumor | 433 (0.4) | 3 (0.3) | 430 (0.4) | 1 |
| Metastatic solid tumor | 701 (0.6) | 3 (0.3) | 698 (0.6) | 0.506 |
| Leukemia | 697 (0.6) | 4 (0.4) | 693 (0.6) | 0.825 |
| Lymphoma | 610 (0.5) | 3 (0.3) | 607 (0.5) | 0.638 |
| HIV | 234 (0.2) | 2 (0.2) | 232 (0.2) | 0.699 |
| CCI (mean, SD) | 3.5 (2.6) | 3.9 (2.4) | 3.5 (2.6) | <0.001 |
| Total N (%) | SADs N (%) | Non-SADs N (%) | p-Value | |
|---|---|---|---|---|
| Respiratory insufficiency | 47,529 (40) | 381 (43) | 47,148 (40) | 0.160 |
| ICU admission | 11,449 (10) | 98 (11) | 11,351 (10) | 0.211 |
| Admission length | 10.6 (11.7) | 11.2 (11.6) | 10.6 (11.7) | 0.09 |
| ICU admission length | 15.6 (17.6) | 12.3 (10.5) | 15.6 (17.6) | 0.008 |
| In-hospital mortality | 18,858 (16) | 174 (20) | 18,864 (16) | 0.05 |
| OR (95% CI) | p-Value | |
|---|---|---|
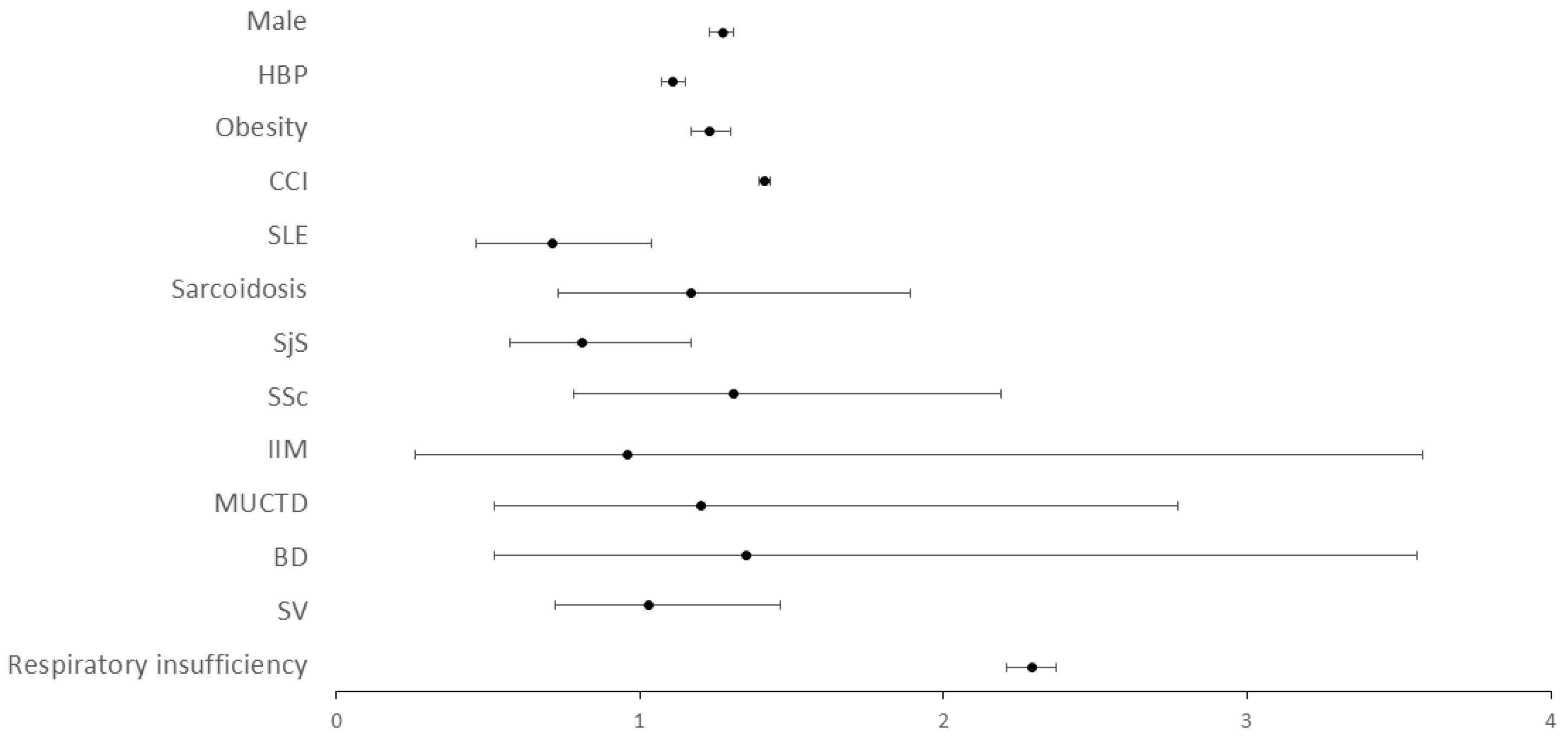
| Male sex | 1.27 (1.23–1.31) | <0.001 |
| High blood pressure | 1.11 (1.07–1.15) | <0.001 |
| Obesity | 1.23 (1.17–1.30) | <0.001 |
| CCI | 1.41 (1.40–1.42) | <0.001 |
| SAD | 0.93 (0.78–1.11) | 0.433 |
| Respiratory insufficiency | 2.92 (2.21–2.37) | <0.001 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Age | 1.05 (1.04–1.07) | <0.001 |
| Heart failure | 1.67 (1.10–2.49) | 0.016 |
| Chronic kidney disease | 1.29 (1.05–1.59) | 0.015 |
| Liver disease | 1.97 (1.13–3.44) | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno-Torres, V.; de Mendoza, C.; Mellor-Pita, S.; Martínez-Urbistondo, M.; Durán-del Campo, P.; Tutor-Ureta, P.; Vázquez-Comendador, J.-M.; Calderón-Parra, J.; Múñez-Rubio, E.; Ramos-Martínez, A.; et al. Systemic Autoimmune Diseases in Patients Hospitalized with COVID-19 in Spain: A Nation-Wide Registry Study. Viruses 2022, 14, 1631. https://doi.org/10.3390/v14081631
Moreno-Torres V, de Mendoza C, Mellor-Pita S, Martínez-Urbistondo M, Durán-del Campo P, Tutor-Ureta P, Vázquez-Comendador J-M, Calderón-Parra J, Múñez-Rubio E, Ramos-Martínez A, et al. Systemic Autoimmune Diseases in Patients Hospitalized with COVID-19 in Spain: A Nation-Wide Registry Study. Viruses. 2022; 14(8):1631. https://doi.org/10.3390/v14081631
Chicago/Turabian StyleMoreno-Torres, Víctor, Carmen de Mendoza, Susana Mellor-Pita, María Martínez-Urbistondo, Pedro Durán-del Campo, Pablo Tutor-Ureta, José-Manuel Vázquez-Comendador, Jorge Calderón-Parra, Elena Múñez-Rubio, Antonio Ramos-Martínez, and et al. 2022. "Systemic Autoimmune Diseases in Patients Hospitalized with COVID-19 in Spain: A Nation-Wide Registry Study" Viruses 14, no. 8: 1631. https://doi.org/10.3390/v14081631
APA StyleMoreno-Torres, V., de Mendoza, C., Mellor-Pita, S., Martínez-Urbistondo, M., Durán-del Campo, P., Tutor-Ureta, P., Vázquez-Comendador, J. -M., Calderón-Parra, J., Múñez-Rubio, E., Ramos-Martínez, A., Fernández-Cruz, A., Castejón, R., & Vargas-Nuñez, J. -A. (2022). Systemic Autoimmune Diseases in Patients Hospitalized with COVID-19 in Spain: A Nation-Wide Registry Study. Viruses, 14(8), 1631. https://doi.org/10.3390/v14081631