
Results of a European-Wide External Quality Assessment (EQA) Scheme for Serological Detection of Anti-SARS-CoV-2 (CoVimm)—Pitfalls of Routine Application

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Preparation
2.3. Laboratory Characterization of EQA Samples
2.4. Sample Characteristics
2.5. Statistical Analysis
3. Results
3.1. Participation and Scope
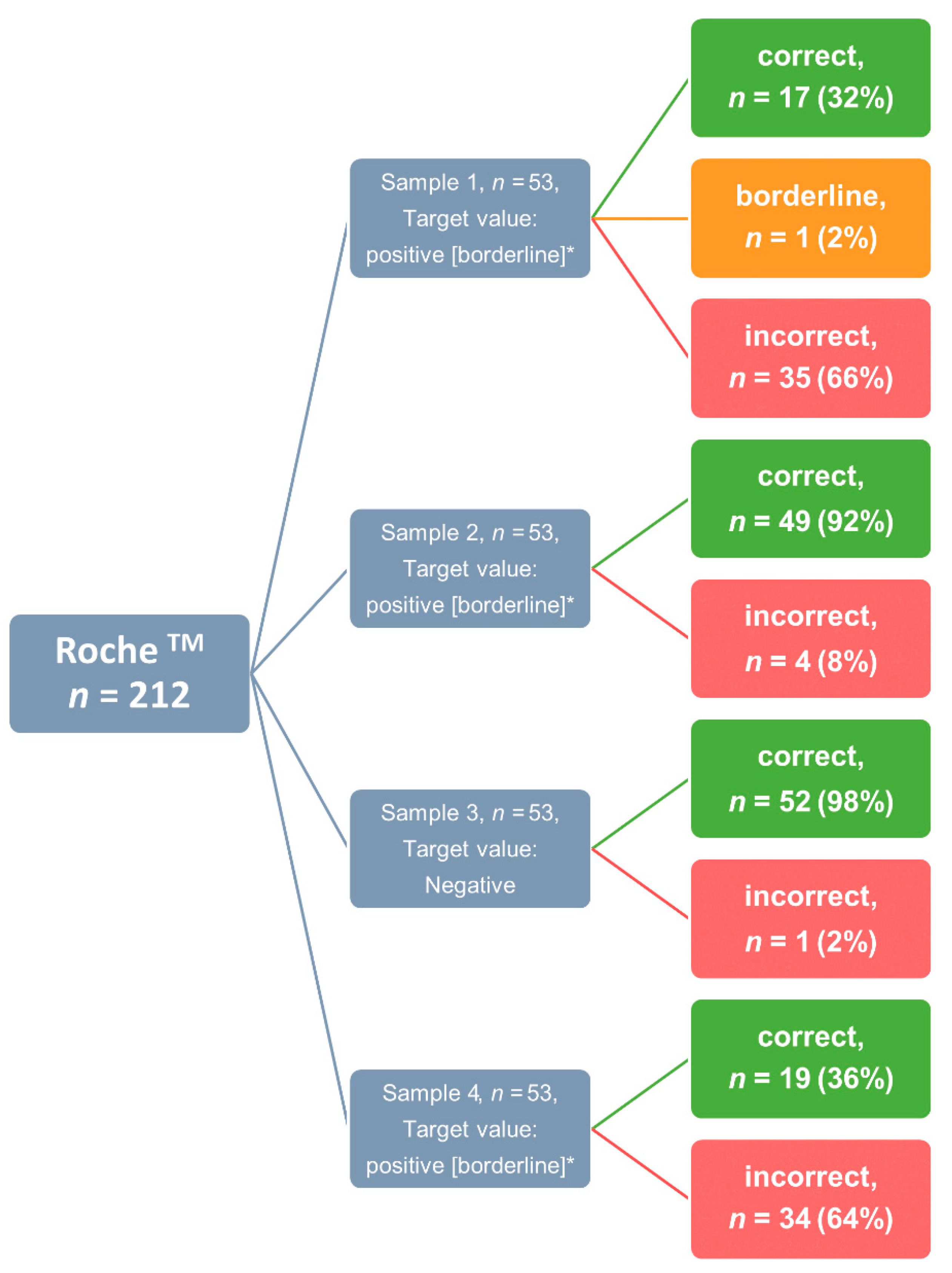
3.2. Success Rate and Sample-Specific Error Rate
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, A.; Jernigan, D.B.; Abdirizak, F.; Abedi, G.; Aggarwal, S.; Albina, D.; Allen, E.; Andersen, L.; Anderson, J.; Anderson, M.; et al. Initial public health response and interim clinical guidance for the 2019 novel coronavirus outbreak—United States, 31 December 2019–4 February 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 140–146. [Google Scholar] [CrossRef]
- Fang, F.C.; Naccache, S.N.; Greninger, A.L. The laboratory diagnosis of coronavirus disease 2019—Frequently asked questions. Clin. Infect. Dis. 2020, 71, 2996–3001. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; Ferrante di Ruffano, L.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 6, CD013652. [Google Scholar] [CrossRef] [PubMed]
- Theel, E.S.; Slev, P.; Wheeler, S.; Couturier, M.R.; Wong, S.J.; Kadkhoda, K. The role of antibody testing for SARS-CoV-2: Is there one? J. Clin. Microbiol. 2020, 58, e00797-20. [Google Scholar] [CrossRef]
- Knezevic, I.; Mattiuzzo, G.; Page, M.; Minor, P.; Griffiths, E.; Nuebling, M.; Moorthy, V. WHO International Standard for evaluation of the antibody response to COVID-19 vaccines: Call for urgent action by the scientific community. Lancet Microbe 2021, 3, e235–e240. [Google Scholar] [CrossRef]
- Tabish, S.A. COVID-19 pandemic: Emerging perspectives and future trends. J. Public Health Res. 2020, 9, 1786. [Google Scholar] [CrossRef]
- Vandenberg, O.; Martiny, D.; Rochas, O.; van Belkum, A.; Kozlakidis, Z. Considerations for diagnostic COVID-19 tests. Nat. Rev. Microbiol. 2021, 19, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Kittel, M.; Muth, M.C.; Zahn, I.; Roth, H.J.; Thiaucourt, M.; Gerhards, C.; Haselmann, V.; Neumaier, M.; Findeisen, P. Clinical evaluation of commercial automated SARS-CoV-2 immunoassays. Int. J. Infect. Dis. 2021, 103, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Cdcgov. Interim Guidelines for COVID-19 Antibody Testing|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html (accessed on 13 May 2022).
- Aloisio, E.; Falvella, F.S.; Carnevale, A.; Panteghini, M. SARS-CoV-2 serologic tests: Do not forget the good laboratory practice. Clin. Chem. Lab. Med. 2021, 59, e175–e177. [Google Scholar] [CrossRef]
- Rumer, L.; Domingo, C.; Donoso Mantke, O.; Dobrydneva, Y.; Greiner, M.; Niedrig, M. Statistical approach for optimization of external quality assurance (EQA) studies of molecular and serological viral diagnostics. Clin. Chem. Lab. Med. 2016, 54, 1589–1598. [Google Scholar] [CrossRef]
- Sciacovelli, L.; Zardo, L.; Secchiero, S.; Plebani, M. Quality specifications in EQA schemes: From theory to practice. Clin. Chim. Acta 2004, 346, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Haselmann, V.; Ozcurumez, M.K.; Klawonn, F.; Ast, V.; Gerhards, C.; Eichner, R.; Costina, V.; Dobler, G.; Geilenkeuser, W.J.; Wolfel, R.; et al. Results of the first pilot external quality assessment (EQA) scheme for anti-SARS-CoV2-antibody testing. Clin. Chem Lab. Med. 2020, 58, 2121–2130. [Google Scholar] [CrossRef] [PubMed]
- Ast, V.; Costina, V.; Eichner, R.; Bode, A.; Aida, S.; Gerhards, C.; Thiaucourt, M.; Dobler, G.; Geilenkeuser, W.-J.; Wölfel, R.; et al. Assessing the quality of serological testing in the COVID-19 pandemic: Results of a European external quality assessment (EQA) scheme for Anti-SARS-CoV-2 antibody detection. J. Clin. Microbiol. 2021, 59, e00559-21. [Google Scholar] [CrossRef]
- Bioanalytik, R.F. Ringversuche Corona-Antikörper 2022. Available online: https://www.rfb.bio/cgi/surveyDetails?rv_type=CoVimm&rvTypeForDetails=CoVimm&year=2022&rv_num=2&analyte=all&searchType=rv_type (accessed on 29 June 2022).
- Liu, G.; Rusling, J.F. COVID-19 antibody tests and their limitations. ACS Sens. 2021, 6, 593–612. [Google Scholar] [CrossRef]
- Arnaout, R.; Lee, R.A.; Lee, G.R.; Callahan, C.; Cheng, A.; Yen, C.F.; Smith, K.P.; Arora, R.; Kirby, J.E. The limit of detection matters: The case for benchmarking severe acute respiratory syndrome coronavirus 2 testing. Clin. Infect. Dis. 2021, 73, e3042–e3046. [Google Scholar] [CrossRef]
- AFP. Antibody Tests Key to Ending COVID-19 Lockdowns-France 24; AFP: Paris, France, 2020. [Google Scholar]
- Royo-Cebrecos, C.; Vilanova, D.; Lopez, J.; Arroyo, V.; Pons, M.; Francisco, G.; Carrasco, M.G.; Pique, J.M.; Sanz, S.; Dobano, C.; et al. Mass SARS-CoV-2 serological screening, a population-based study in the Principality of Andorra. Lancet Reg. Health Eur. 2021, 5, 100119. [Google Scholar] [CrossRef]
- Gray, N.; Calleja, D.; Wimbush, A.; Miralles-Dolz, E.; Gray, A.; De Angelis, M.; Derrer-Merk, E.; Oparaji, B.U.; Stepanov, V.; Clearkin, L.; et al. Is “no test is better than a bad test”? Impact of diagnostic uncertainty in mass testing on the spread of COVID-19. PLoS ONE 2020, 15, e0240775. [Google Scholar] [CrossRef] [PubMed]
- Gigi Gronvall, P.; Nancy Connell, P.; Amanda Kobokovich, M.; Rachel West, P.; Kelsey Lane Warmbrod, M.; Matthew, P. Developing A National Strategy for Serology (Antibody Testing); Shearer, M., Lucia Mullen, M., Tom Inglesby, M., Eds.; The Johns Hopkins Center for Health Security: Baltimore, MD, USA, 2022. [Google Scholar]
- Brownstein, N.C.; Chen, Y.A. Predictive values, uncertainty, and interpretation of serology tests for the novel coronavirus. Sci. Rep. 2021, 11, 5491. [Google Scholar] [CrossRef] [PubMed]
- Abutaleb, J.A.A.Y. Coronavirus Risk Calculations Get Harder as A Study Suggests Rapid Tests May Be Less Effective at Detecting Omicron; The Washington Post: Washington, WA, USA, 2021. [Google Scholar]
- Todd Haugh, S.B. Opinion | Just Because You Test Positive for Antibodies Doesn’t Mean You Have Them; The New York Times: New York, NY, USA, 2020. [Google Scholar]
- Mandavilli, A. Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be; The New York Times: New York, NY, USA, 2020. [Google Scholar]
- Abbott. SARS-CoV-2-Immunassay|Core Laboratory bei Abbott. Available online: https://www.corelaboratory.abbott/int/de/offerings/segments/infectious-disease/sars-cov-2- (accessed on 15 May 2022).
- Weber, B.; Gurtler, L.; Thorstensson, R.; Michl, U.; Muhlbacher, A.; Burgisser, P.; Villaescusa, R.; Eiras, A.; Gabriel, C.; Stekel, H.; et al. Multicenter evaluation of a new automated fourth-generation human immunodeficiency virus screening assay with a sensitive antigen detection module and high specificity. J. Clin. Microbiol. 2002, 40, 1938–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villalta, D.; Martelli, P.; Moratto, A.; Salgarolo, V.; Ligato, E.; Conte, M.; Giacomello, R.; Pellis, T.; De Rosa, R.; Venturini, S.; et al. Diagnostic performance of an automated chemiluminescence immunoassay for SARS-CoV-2 IgG and IgM antibodies detection: A real life experience. Pract. Lab. Med. 2021, 25, e00227. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Proficiency Testing & Medical Laboratory Quality-CLSI. Available online: https://clsi.org/about/blog/using-proficiency-testing-to-improve-medical-laboratory-quality/ (accessed on 15 March 2022).
- U.S. Food & Drug Administration. Emergency Use Authorization|FDA. Available online: https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization (accessed on 10 May 2022).
- Matheeussen, V.; Corman, V.M.; Donoso Mantke, O.; McCulloch, E.; Lammens, C.; Goossens, H.; Niemeyer, D.; Wallace, P.S.; Klapper, P.; Niesters, H.G.; et al. International external quality assessment for SARS-CoV-2 molecular detection and survey on clinical laboratory preparedness during the COVID-19 pandemic, April/May 2020. Eurosurveillance 2020, 25, 2001223. [Google Scholar] [CrossRef] [PubMed]
- Editors, H.C. First Confirmed Case of COVID-19 Found in U.S.-HISTORY. Available online: https://www.history.com/this-day-in-history/first-confirmed-case-of-coronavirus-found-in-us-washington-state (accessed on 10 May 2022).
- Sciacovelli, L.; Padoan, A.; Secchiero, S.; Plebani, M. Serological diagnostic for SARS-CoV-2: An experimental external quality assessment scheme. Clin. Chem. Lab. Med. 2021, 59, 1878–1884. [Google Scholar] [CrossRef] [PubMed]
- Ejazi, S.A.; Ghosh, S.; Ali, N. Antibody detection assays for COVID-19 diagnosis: An early overview. Immunol. Cell Biol. 2021, 99, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Harritshoj, L.H.; Gybel-Brask, M.; Afzal, S.; Kamstrup, P.R.; Jorgensen, C.S.; Thomsen, M.K.; Hilsted, L.; Friis-Hansen, L.; Szecsi, P.B.; Pedersen, L.; et al. Comparison of 16 serological SARS-CoV-2 immunoassays in 16 clinical laboratories. J. Clin. Microbiol. 2021, 59, e02596-20. [Google Scholar] [CrossRef]
- Tre-Hardy, M.; Wilmet, A.; Beukinga, I.; Favresse, J.; Dogne, J.M.; Douxfils, J.; Blairon, L. Analytical and clinical validation of an ELISA for specific SARS-CoV-2 IgG, IgA, and IgM antibodies. J. Med. Virol. 2021, 93, 803–811. [Google Scholar] [CrossRef]
- Roche Diagnostics. Elecsys® Anti-SARS-CoV-2. Available online: https://diagnostics.roche.com/global/en/products/params/elecsys-anti-sars-cov-2.html (accessed on 29 June 2022).
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-spike protein assays to determine SARS-CoV-2 antibody levels: A head-to-head comparison of five quantitative assays. Microbiol. Spectr. 2021, 9, e0024721. [Google Scholar] [CrossRef]
- Chvatal-Medina, M.; Mendez-Cortina, Y.; Patino, P.J.; Velilla, P.A.; Rugeles, M.T. Antibody responses in COVID-19: A review. Front. Immunol. 2021, 12, 633184. [Google Scholar] [CrossRef]
- Beck, E.J.; Hsieh, Y.H.; Fernandez, R.E.; Dashler, G.; Egbert, E.R.; Truelove, S.A.; Garliss, C.; Wang, R.; Bloch, E.M.; Shrestha, R.; et al. Differentiation of SARS-CoV-2 naturally infected and vaccinated individuals in an inner-city emergency department. medRxiv 2021, 21264968. [Google Scholar] [CrossRef]
- Haselmann, V.; Ahmad-Nejad, P.; Geilenkeuser, W.J.; Duda, A.; Gabor, M.; Eichner, R.; Patton, S.; Neumaier, M. Results of the first external quality assessment scheme (EQA) for isolation and analysis of circulating tumour DNA (ctDNA). Clin. Chem. Lab. Med. (CCLM) 2018, 56, 220–228. [Google Scholar] [CrossRef]
- Padoan, A.; Bonfante, F.; Pagliari, M.; Bortolami, A.; Negrini, D.; Zuin, S.; Bozzato, D.; Cosma, C.; Sciacovelli, L.; Plebani, M. Analytical and clinical performances of five immunoassays for the detection of SARS-CoV-2 antibodies in comparison with neutralization activity. EBioMedicine 2020, 62, 103101. [Google Scholar] [CrossRef]
- Bohn, M.K.; Loh, T.P.; Wang, C.B.; Mueller, R.; Koch, D.; Sethi, S.; Rawlinson, W.D.; Clementi, M.; Erasmus, R.; Leportier, M.; et al. IFCC interim guidelines on serological testing of antibodies against SARS-CoV-2. Clin. Chem. Lab. Med. 2020, 58, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- NIBSC. COVID-19-Related Research Reagents. Available online: https://www.nibsc.org/science_and_research/idd/cfar/covid-19_reagents.aspx (accessed on 3 May 2022).
- Commission, R.-J.S.H.-E. Welcome to the Certified Reference Materials catalogue of the JRC. Available online: https://crm.jrc.ec.europa.eu/?ref=1 (accessed on 3 May 2022).
- Miller, W.G.; Jones, G.R.; Horowitz, G.L.; Weykamp, C. Proficiency testing/external quality assessment: Current challenges and future directions. Clin. Chem. 2011, 57, 1670–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| EQA Sample 1 | EQA Sample 2 | EQA Sample 3 | EQA Sample 4 | |
|---|---|---|---|---|
| Roche Elecsys anti-N (COI/result) | negative | >250.00/reactive | negative | negative |
| Roche Elecsys anti-S (U/mL/result) | 30.136/reactive | 147.04/reactive | 0.400/negative | <250.00 reactive |
| Euroimmun anti-N IgG (ratio/result) | 0.37/negative | 0.60/negative | 0.18/negative | 0.35/negative |
| Euroimmun anti-N IgS (ratio/result) | 1.48/reactive | 1.01/borderline | 0.35/negative | 5.05/reactive |
| VNT titer (wildtype) (titer/result) | <5/negative | <5/negative | <5/negative | 10/positive |
| VNT titer (delta) (titer/result) | <5/negative | <5/negative | <5/negative | <5/negative |
| target value—Anti-SARS-CoV-2 IgG total | positive [borderline] * | positive [borderline] | negative | positive [borderline] |
| target value—Anti-N-SARS-CoV-2 IgG | negative | positive [borderline, negative] | negative | negative |
| target value—Anti-S-SARS-CoV-2 IgG | positive [borderline] | positive [borderline] | negative | positive [borderline] |
| (a) | |||||||||||
| Task | n | % | Manufacturer | [n] | [%] | Correct [n] | [%] | Borderline [n] | [%] | Incorrect [n] | [%] |
| Anti-SARS-CoV-2 IgG total | 624 | 49 | Bio-Rad | 4 | 1 | 4 | 100 | ||||
| DiaSys | 8 | 1 | 7 | 88 | 1 | 12 | |||||
| Abbott | 52 | 8 | 40 | 77 | 1 | 2 | 11 | 21 | |||
| Beckman Coulter | 16 | 3 | 12 | 75 | 4 | 25 | |||||
| Euroimmun | 96 | 15 | 88 | 92 | 8 | 8 | |||||
| bioMerieux | 4 | 1 | 4 | 100 | |||||||
| IDS S.A. | 4 | 1 | 3 | 75 | 1 | 25 | |||||
| Roche | 212 | 34 | 137 | 65 | 1 | 0 | 74 | 35 | |||
| lab developed assay | 4 | 1 | 2 | 50 | 2 | 50 | |||||
| Siemens Healthineers | 24 | 4 | 24 | 100 | |||||||
| Siemens Healthineers-Atellica | 16 | 3 | 16 | 100 | |||||||
| SERAMUN Diagnostica | 4 | 1 | 4 | 100 | |||||||
| DiaSorin | 104 | 17 | 98 | 94 | 6 | 6 | |||||
| Virotech Diagnostics | 4 | 1 | 2 | 50 | 2 | 50 | |||||
| others | 24 | 4 | 16 | 67 | 8 | 33 | |||||
| MöLAB | 4 | 1 | 2 | 50 | 1 | 25 | 1 | 25 | |||
| nal von Minden | 16 | 3 | 9 | 56 | 2 | 12 | 5 | 31 | |||
| AESKI.Diagnostics | 4 | 1 | 3 | 75 | 1 | 25 | |||||
| Mikrogen | 16 | 3 | 12 | 75 | 4 | 25 | |||||
| Viramed Biotech | 8 | 1 | 8 | 100 | |||||||
| value of correctness [average %] | 79.45 | ||||||||||
| (b) | |||||||||||
| Task | n | % | Manufacturer | [n] | [%] | Correct [n] | [%] | Borderline [n] | [%] | Incorrect [n] | [%] |
| Anti-S-SARS-CoV-2 IgG | 447 | 35 | Bio-Rad | 4 | 1 | 4 | 100 | ||||
| Abbott | 56 | 13 | 53 | 95 | 3 | 5 | |||||
| Euroimmun | 76 | 17 | 72 | 95 | 4 | 5 | |||||
| bioMerieux | 4 | 1 | 4 | 100 | |||||||
| Roche | 175 | 39 | 169 | 97 | 6 | 3 | |||||
| Siemens Healthineers | 8 | 2 | 8 | 100 | |||||||
| IBL | 4 | 1 | 4 | 100 | |||||||
| Siemens Healthineers-Atellica | 20 | 4 | 20 | 100 | |||||||
| SERAMUN Diagnostica | 4 | 1 | 4 | 100 | |||||||
| Mediagnost | 8 | 2 | 6 | 75 | 2 | 25 | |||||
| DiaSorin | 36 | 8 | 36 | 100 | |||||||
| others | 16 | 4 | 11 | 69 | 5 | 31 | |||||
| AESKI.Diagnostics | 4 | 1 | 3 | 75 | 1 | 25 | |||||
| Mikrogen | 8 | 2 | 8 | 100 | |||||||
| Novatec | 4 | 1 | 4 | 100 | |||||||
| Bühlmann | 4 | 1 | 4 | 100 | |||||||
| Viramed Biotech | 4 | 1 | 4 | 100 | |||||||
| Virion/Serion | 4 | 1 | 4 | 100 | |||||||
| Snibe | 8 | 2 | 8 | 100 | |||||||
| value of correctness [average %] | 95.02 | ||||||||||
| (c) | |||||||||||
| Task | n | % | Manufacturer | [n] | [%] | Correct [n] | [%] | Borderline [n] | [%] | Incorrect [n] | [%] |
| Anti-N-SARS-CoV-2 IgG | 204 | 16 | Bio-Rad | 4 | 2 | 4 | 100 | ||||
| Abbott | 44 | 22 | 10 | 23 | 1 | 2 | 33 | 75 | |||
| Euroimmun | 20 | 10 | 4 | 20 | 1 | 5 | 15 | 75 | |||
| Roche | 104 | 51 | 100 | 96 | 4 | 4 | |||||
| SERAMUN Diagnostica | 4 | 2 | 4 | 100 | |||||||
| others | 8 | 4 | 7 | 88 | 1 | 12 | |||||
| AESKI.Diagnostics | 4 | 2 | 3 | 75 | 1 | 25 | |||||
| Mikrogen | 12 | 6 | 12 | 100 | |||||||
| Viramed Biotech | 4 | 2 | 4 | 100 | |||||||
| value of correctness [average %] | 78 | ||||||||||
| (a) | ||||
| Task | Manufacturer | Reported Results [n] | Diagnostic Sensitivity [%] | Diagnostic Specificity [%] |
| Anti-SARS-CoV-2 IgG total | Abbott | 52 | 72 | 100 |
| AESKI.Diagnostics | 4 | 100 | 100 | |
| Beckmann Coulter | 16 | 75 | 100 | |
| Bio Rad | 4 | 100 | 100 | |
| bioMeriéux | 4 | 100 | 100 | |
| DiaSorin | 104 | 96 | 88 | |
| DiaSys | 8 | 100 | 100 | |
| lab developed assay | 4 | 33 | 100 | |
| Euroimmun | 96 | 92 | 92 | |
| IDS S.A. | 4 | 33 | 100 | |
| MöLAB | 4 | 66 | 100 | |
| nal von Minden | 16 | 59 | 100 | |
| Roche | 212 | 54 | 98 | |
| SERAMUN Diagnostica | 4 | 100 | 100 | |
| Siemens Healthineers | 24 | 100 | 100 | |
| Siemens Healthineers Atellica | 16 | 100 | 100 | |
| Viramed Biotech | 8 | 100 | 100 | |
| Virotech Diagnostics | 4 | 33 | 100 | |
| others | 24 | 56 | 100 | |
| Results: average [median] | 77.32 [92] | 98.84 [100] | ||
| (b) | ||||
| Task | Manufacturer | Reported Results [n] | Diagnostic Sensitivity [%] | Diagnostic Specificity [%] |
| Anti-S-SARS-CoV-2 IgG | Abbott | 56 | 93 | 100 |
| AESKI.Diagnostics | 4 | 100 | 100 | |
| Bio Rad | 4 | 100 | 100 | |
| bioMeriéux | 4 | 100 | 100 | |
| Bühlmann | 4 | 100 | 100 | |
| DiaSorin | 36 | 100 | 100 | |
| Euroimmun | 76 | 95 | 95 | |
| IBL | 4 | 100 | 100 | |
| Mediagnost | 8 | 100 | 100 | |
| Mikrogen | 8 | 100 | 100 | |
| Novatec | 4 | 100 | 100 | |
| Roche | 175 | 95 | 100 | |
| SERAMUN Diagnostica | 4 | 100 | 100 | |
| Siemens Healthineers | 8 | 100 | 100 | |
| Siemens Healthineers Atellica | 20 | 100 | 100 | |
| Snibe | 8 | 100 | 100 | |
| Viramed Biotech | 4 | 100 | 100 | |
| Virion/Serion | 4 | 100 | 100 | |
| others | 16 | 67 | 75 | |
| Results: average [median] | 97.37 [100] | 98.42 [100] | ||
| (c) | ||||
| Task | Manufacturer | Reported Results [n] | Diagnostic Sensitivity [%] | Diagnostic Specificity [%] |
| Anti-N-SARS-CoV- IgG * | Abbott | 44 | n.a. | 100 |
| AESKI.Diagnostics | 4 | n.a. | 100 | |
| Bio Rad | 4 | n.a. | 100 | |
| Euroimmun | 20 | n.a. | 100 | |
| Mikrogen | 12 | n.a. | 100 | |
| Roche | 104 | n.a. | 95 | |
| SERAMUN Diagnostica | 4 | n.a. | 100 | |
| Viramed Biotech | 4 | n.a. | 100 | |
| others | 8 | n.a. | 100 | |
| Results: average [median] | n.a. | 99.44 [100] | ||
| Task | Participants [n] | Success/Passing Rate [%] | False Positive [%] | False Negative [%] |
|---|---|---|---|---|
| Anti-SARS-CoV-2 IgG total | 129 | 64 | 3.7 | 20.2 |
| Anti-S-SARS-CoV-2 IgG | 100 | 96 | 1.8 | 0.9 |
| Anti-N-SARS-CoV-2 IgG | 47 | 90 | n.a. | 3.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kittel, M.; Eichner, R.; Aida, S.; Bode, A.; Ast, V.; Kessler, A.; Neumaier, M.; Wölfel, R.; Haselmann, V. Results of a European-Wide External Quality Assessment (EQA) Scheme for Serological Detection of Anti-SARS-CoV-2 (CoVimm)—Pitfalls of Routine Application. Viruses 2022, 14, 1662. https://doi.org/10.3390/v14081662
Kittel M, Eichner R, Aida S, Bode A, Ast V, Kessler A, Neumaier M, Wölfel R, Haselmann V. Results of a European-Wide External Quality Assessment (EQA) Scheme for Serological Detection of Anti-SARS-CoV-2 (CoVimm)—Pitfalls of Routine Application. Viruses. 2022; 14(8):1662. https://doi.org/10.3390/v14081662
Chicago/Turabian StyleKittel, Maximilian, Romy Eichner, Sihem Aida, Anna Bode, Volker Ast, Anja Kessler, Michael Neumaier, Roman Wölfel, and Verena Haselmann. 2022. "Results of a European-Wide External Quality Assessment (EQA) Scheme for Serological Detection of Anti-SARS-CoV-2 (CoVimm)—Pitfalls of Routine Application" Viruses 14, no. 8: 1662. https://doi.org/10.3390/v14081662
APA StyleKittel, M., Eichner, R., Aida, S., Bode, A., Ast, V., Kessler, A., Neumaier, M., Wölfel, R., & Haselmann, V. (2022). Results of a European-Wide External Quality Assessment (EQA) Scheme for Serological Detection of Anti-SARS-CoV-2 (CoVimm)—Pitfalls of Routine Application. Viruses, 14(8), 1662. https://doi.org/10.3390/v14081662