
Differences in Clinical Presentations of Omicron Infections with the Lineages BA.2 and BA.5 in Mecklenburg-Western Pomerania, Germany, between April and July 2022

 ,
,
Abstract
:1. Introduction
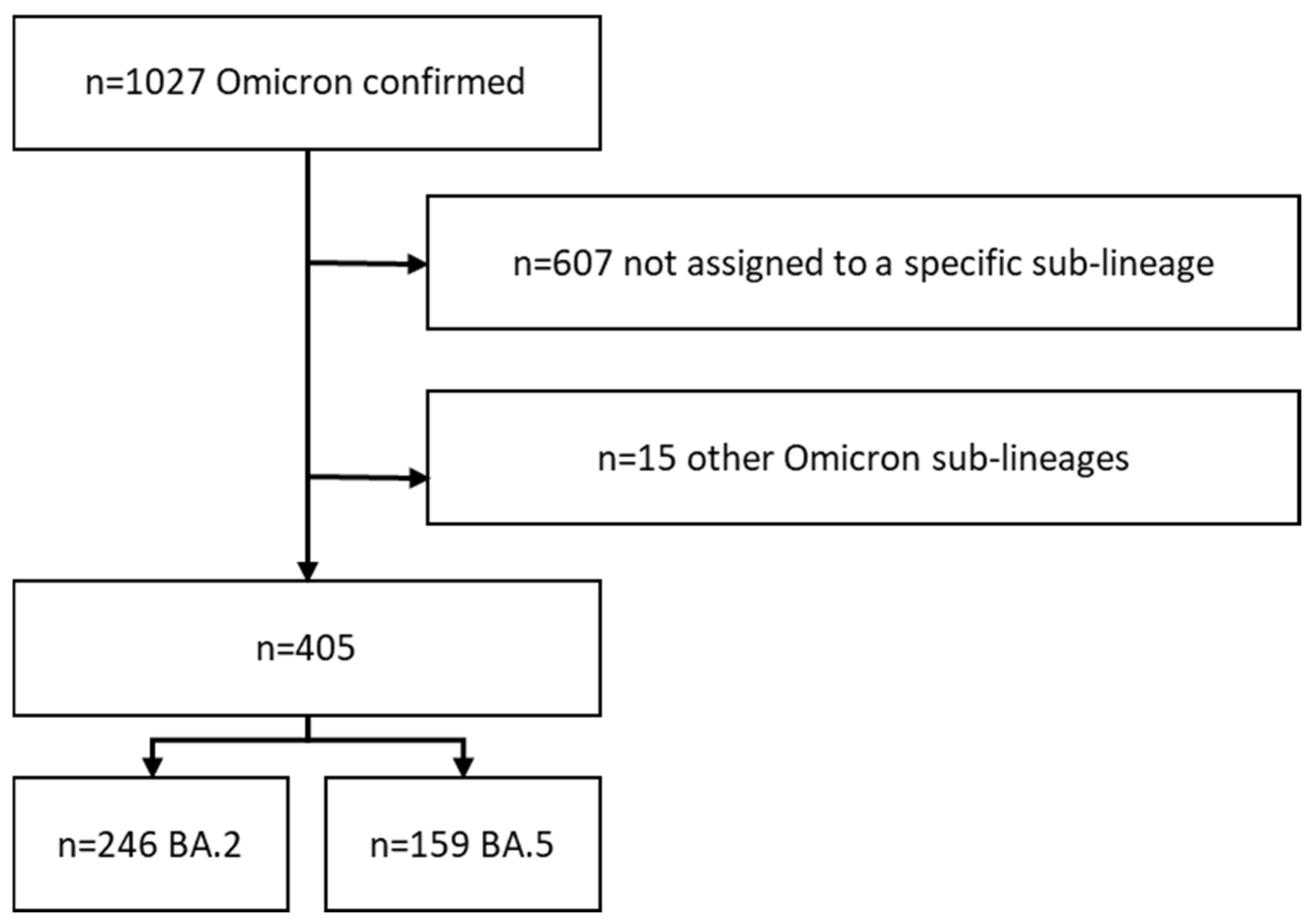
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robert Koch Institut (RKI). Wöchentlicher Lagebericht des RKI zur Coronavirus-Krankheit-2019 (COVID-19). Available online: http://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/VOC_VOI_Tabelle.html (accessed on 7 July 2022).
- Sievers, C.; Zacher, B.; Ullrich, A.; Huska, M.; Fuchs, S.; Buda, S.; Haas, W.; Diercke, M.; an der Heiden, M.; Kröger, S. SARS-CoV-2 Omicron variants BA.1 and BA.2 both show similarly reduced disease severity of COVID-19 compared to Delta, Germany, 2021 to 2022. Eurosurveillance 2022, 27, 2200396. [Google Scholar] [CrossRef] [PubMed]
- Tegally, H.; Moir, M.; Everatt, J.; Giovanetti, M.; Scheepers, C.; Wilkinson, E.; Subramoney, K.; Makatini, Z.; Moyo, S.; Amoako, D.G.; et al. Emergence of SARS-CoV-2 Omicron lineages BA.4 and BA.5 in South Africa. Nat. Med. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Viana, R.; Moyo, S.; Amoako, D.G.; Tegally, H.; Scheepers, C.; Althaus, C.L.; Anyaneji, U.J.; Bester, P.A.; Boni, M.F.; Chand, M.; et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in southern Africa. Nature 2022, 603, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Kimura, I.; Yamasoba, D.; Tamura, T.; Nao, N.; Oda, Y.; Mitoma, S.; Ito, J.; Nasser, H.; Zahradnik, J.; Uriu, K.; et al. Virological characteristics of the novel SARS-CoV-2 Omicron variants including BA.2.12.1, BA.4 and BA.5. bioRxiv 2022. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Jian, F.; Song, W.; Xiao, T.; Wang, L.; Du, S.; Wang, J.; Li, Q.; Chen, X.; et al. BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Nature 2022, 608, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Tom-Aba, D.; Silenou, B.C.; Doerrbecker, J.; Fourie, C.; Leitner, C.; Wahnschaffe, M.; Strysewske, M.; Arinze, C.C.; Krause, G. The Surveillance Outbreak Response Management and Analysis System (SORMAS): Digital Health Global Goods Maturity Assessment. JMIR Public Health Surveill. 2020, 6, e15860. [Google Scholar] [CrossRef] [PubMed]
- Sass, J.; Bartschke, A.; Lehne, M.; Essenwanger, A.; Rinaldi, E.; Rudolph, S.; Heitmann, K.U.; Vehreschild, J.J.; von Kalle, C.; Thun, S. The German Corona Consensus Dataset (GECCO): A standardized dataset for COVID-19 research in university medicine and beyond. BMC Med. Inform. Decis. Mak. 2020, 20, 341. [Google Scholar] [CrossRef] [PubMed]
- The ZOE Health Study. Omicron Symptoms: What Are They and How Long Do They Last? Available online: www.joinzoe.com/learn/omicron-symptoms (accessed on 8 July 2022).
- Dixon, B.E.; Wools-Kaloustian, K.; Fadel, W.F.; Duszynski, T.J.; Yiannoutsos, C.; Halverson, P.K.; Menachemi, N. Symptoms and symptom clusters associated with SARS-CoV-2 infection in community-based populations: Results from a statewide epidemiological study. PLoS ONE 2021, 16, e0241875. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Meo, S.A.; Meo, A.S.; Al-Jassir, F.F.; Klonoff, D.C. Omicron SARS-CoV-2 new variant: Global prevalence and biological and clinical characteristics. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 8012–8018. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/COVID-19/variants-concern (accessed on 18 July 2022).



{kind=link}
{kind=link}
| Characteristics | BA.2 | BA.5 | p Value 1 | ||||
|---|---|---|---|---|---|---|---|
| n | [%] | n | [%] | ||||
| Sex | Female | 126 | 51.2 | 96 | 60.4 | 0.135 | |
| Male | 118 | 48.0 | 61 | 38.4 | |||
| Unknown | 2 | 0.8 | 2 | 1.3 | |||
| Age groups | 0–19 | 25 | 10.2 | 13 | 8.2 | 0.759 | |
| 20–39 | 76 | 30.9 | 48 | 30.2 | |||
| 40–59 | 94 | 38.2 | 70 | 44.0 | |||
| 60–79 | 43 | 17.5 | 24 | 15.1 | |||
| 80+ | 7 | 2.8 | 3 | 1.9 | |||
| Unknown | 1 | 0.4 | 1 | 0.6 | |||
| Symptoms | Yes | 124 | 50.1 | 69 | 43.4 | 0.186 | |
| No | 122 | 49.9 | 90 | 56.6 | |||
| Vaccination 2 | Yes | 75 | 57.7 | 60 | 49.2 | 0.124 | |
| No | 42 | 32.3 | 54 | 44.3 | |||
| Unknown | 13 | 10 | 8 | 6.6 | |||
| Symptom | Status | BA.2 | BA.5 | p-Value 1 | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | CI 95 [%] | n | % | CI 95 [%] | |||
| Breathing difficulties/dyspnoea | Positive | 18 | 14.5 | [9.2–21.5] | 4 | 5.8 | [2.0–13.2] | 0.097 |
| n.r. | 106 | 85.5 | [78.5–90.8] | 65 | 94.2 | [86.8–98.0] | ||
| Chills or sweating | Positive | 22 | 17.7 | [11.8–25.2] | 3 | 4.3 | [1.2–11.1] | 0.012 |
| n.r. | 102 | 82.3 | [74.8–88.2] | 66 | 95.7 | [88.9–98.8] | ||
| Cough | Positive | 105 | 84.7 | [77.6–90.2] | 52 | 75.4 | [64.3–84.3] | 0.125 |
| n.r. | 19 | 15.3 | [9.8–22.4] | 17 | 24.6 | [15.7–35.7] | ||
| Diarrhea | Positive | 12 | 9.7 | [5.4–15.8] | 9 | 13 | [6.7–22.5] | 0.631 |
| n.r. | 112 | 90.3 | [84.2–94.6] | 60 | 87 | [77.5–93.3] | ||
| Fever | Positive | 43 | 34.7 | [26.7–43.3] | 34 | 49.3 | [37.7–60.9] | 0.065 |
| n.r. | 81 | 65.3 | [56.7–73.3] | 35 | 50.7 | [39.1–62.3] | ||
| Freeze | Positive | 29 | 23.4 | [16.6–31.4] | 6 | 8.7 | [3.7–17.0] | 0.011 |
| n.r. | 95 | 76.6 | [68.6–83.4] | 63 | 91.3 | [83.0–96.3] | ||
| Headache | Positive | 68 | 54.8 | [46.1–63.4] | 37 | 53.6 | [41.9–65.0] | 0.881 |
| n.r. | 56 | 45.2 | [36.6–53.9] | 32 | 46.4 | [35.0–58.1] | ||
| Increased heart rate/tachycardia | Positive | 12 | 9.7 | [5.4–15.8] | 3 | 4.3 | [1.2–11.1] | 0.264 |
| n.r. | 112 | 90.3 | [84.2–94.6] | 66 | 95.7 | [88.9–98.8] | ||
| Loss of smell | Positive | 15 | 12.1 | [7.2–18.7] | 15 | 21.7 | [13.3–32.5] | 0.097 |
| n.r. | 109 | 87.9 | [81.3–92.8] | 54 | 78.3 | [67.5–86.7] | ||
| Loss of taste | Positive | 25 | 20.2 | [13.8–27.9] | 17 | 24.6 | [15.7–35.7] | 0.585 |
| n.r. | 99 | 79.8 | [72.1–86.2] | 52 | 75.4 | [64.3–84.3] | ||
| Muscle or body aches | Positive | 40 | 32.3 | [24.5–40.8] | 28 | 40.6 | [29.6–52.4] | 0.273 |
| n.r. | 84 | 67.7 | [59.2–75.5] | 41 | 59.4 | [47.6–70.4] | ||
| Nausea | Positive | 8 | 6.5 | [3.1–11.8] | 6 | 8.7 | [3.7–17.0] | 0.774 |
| n.r. | 116 | 93.5 | [88.2–96.9] | 63 | 91.3 | [83.0–96.3] | ||
| Other symptoms 2 | Positive | 39 | 31.5 | [23.8–40.0] | 40 | 58.0 | [46.2–69.1] | <0.001 |
| n.r. | 85 | 68.5 | [60.0–76.2] | 29 | 42.0 | [30.9–53.8] | ||
| Pneumonia | Positive | 2 | 1.6 | [0.3–5.1] | 0 | 0 | [–] | 0.289 |
| n.r. | 122 | 98.4 | [94.9–99.7] | 69 | 100 | [–] | ||
| Rapid breathing/tachypnea | Positive | 2 | 1.6 | [0.3–5.1] | 2 | 2.9 | [0.6–9.0] | 0.618 |
| n.r. | 122 | 98.4 | [94.9–99.7] | 67 | 97.1 | [91.0–99.4] | ||
| Runny nose | Positive | 110 | 88.7 | [82.3–93.4] | 52 | 75.4 | [64.3–84.3] | 0.023 |
| n.r. | 14 | 11.3 | [6.6–17.7] | 17 | 24.6 | [15.7–35.7] | ||
| Severe feeling of sickness | Positive | 40 | 32.3 | [24.5–40.8] | 30 | 43.5 | [32.2–55.2] | 0.159 |
| n.r. | 84 | 67.7 | [59.2–75.5] | 39 | 56.5 | [44.8–67.8] | ||
| Sore throat/pharyngitis | Positive | 77 | 62.1 | [53.4–70.3] | 37 | 53.6 | [41.9–65.0] | 0.538 |
| n.r. | 47 | 37.9 | [29.7–46.6] | 32 | 46.4 | [35.0–58.1] | ||
| Symptoms | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chills or Sweating | Cough | Diarrhea | Breathing Difficulties/Dyspnea | Fever | Headache | Muscle or Body Aches | Rapid Breathing/Tachypnea | Runny Nose | Sore Throat/Pharyngitis | Loss of Taste | Loss of Smell | Freeze | |
| Chills or sweating | 1.000 | ||||||||||||
| Cough | 0.026 | 1.000 | |||||||||||
| Diarrhea | 0.063 | 0.082 | 1.000 | ||||||||||
| Breathing difficulties/dyspnea | 0.299 2 | 0.046 | 0.136 | 1.000 | |||||||||
| Fever | 0.095 | 0.064 | 0.191 2 | 0.107 | 1.000 | ||||||||
| Headache | 0.198 2 | 0.096 | 0.019 | 0.230 2 | 0.278 2 | 1.000 | |||||||
| Muscle or body aches | 0.232 2 | 0.047 | 0.125 | 0.179 1 | 0.174 1 | 0.414 2 | 1.000 | ||||||
| Rapid breathing/tachypnea | 0.161 1 | 0.07 | 0.066 | 0.291 2 | 0.179 1 | 0.133 | 0.121 | 1.000 | |||||
| Runny nose | 0.169 1 | 0.334 2 | 0.108 | 0.113 | −0.105 | 0.053 | −0.002 | 0.064 | 1.000 | ||||
| Sore throat/pharyngitis | 0.07 | 0.169 1 | 0.122 | 0.1 | 0.205 2 | 0.190 2 | 0.217 2 | −0.027 | 0.181 1 | 1.000 | |||
| Loss of taste | 0.096 | 0.059 | 0.219 2 | 0.127 | 0.109 | 0.079 | 0.242 2 | 0.188 2 | 0.094 | 0.107 | 1.000 | ||
| Loss of smell | 0.133 | 0.022 | 0.263 2 | 0.251 2 | 0.147 1 | 0.163 1 | 0.192 2 | 0.239 2 | 0.149 1 | 0.124 | 0.5712 | 1.000 | |
| Freeze | 0.5792 | 0.122 | 0.181 1 | 0.254 2 | 0.111 | 0.269 2 | 0.3282 | 0.12 | 0.206 2 | 0.009 | 0.045 | 0.021 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goller, K.V.; Moritz, J.; Ziemann, J.; Kohler, C.; Becker, K.; Hübner, N.-O.; the CoMV-Gen Study Group. Differences in Clinical Presentations of Omicron Infections with the Lineages BA.2 and BA.5 in Mecklenburg-Western Pomerania, Germany, between April and July 2022. Viruses 2022, 14, 2033. https://doi.org/10.3390/v14092033
Goller KV, Moritz J, Ziemann J, Kohler C, Becker K, Hübner N-O, the CoMV-Gen Study Group. Differences in Clinical Presentations of Omicron Infections with the Lineages BA.2 and BA.5 in Mecklenburg-Western Pomerania, Germany, between April and July 2022. Viruses. 2022; 14(9):2033. https://doi.org/10.3390/v14092033
Chicago/Turabian StyleGoller, Katja Verena, Juliane Moritz, Janine Ziemann, Christian Kohler, Karsten Becker, Nils-Olaf Hübner, and the CoMV-Gen Study Group. 2022. "Differences in Clinical Presentations of Omicron Infections with the Lineages BA.2 and BA.5 in Mecklenburg-Western Pomerania, Germany, between April and July 2022" Viruses 14, no. 9: 2033. https://doi.org/10.3390/v14092033
APA StyleGoller, K. V., Moritz, J., Ziemann, J., Kohler, C., Becker, K., Hübner, N. -O., & the CoMV-Gen Study Group. (2022). Differences in Clinical Presentations of Omicron Infections with the Lineages BA.2 and BA.5 in Mecklenburg-Western Pomerania, Germany, between April and July 2022. Viruses, 14(9), 2033. https://doi.org/10.3390/v14092033