
Secular Trends of Clinical Characteristics and Survival of Hepatocellular Carcinoma in Taiwan from 2011 to 2019

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Methods
2.2. Statistical Analysis
3. Results
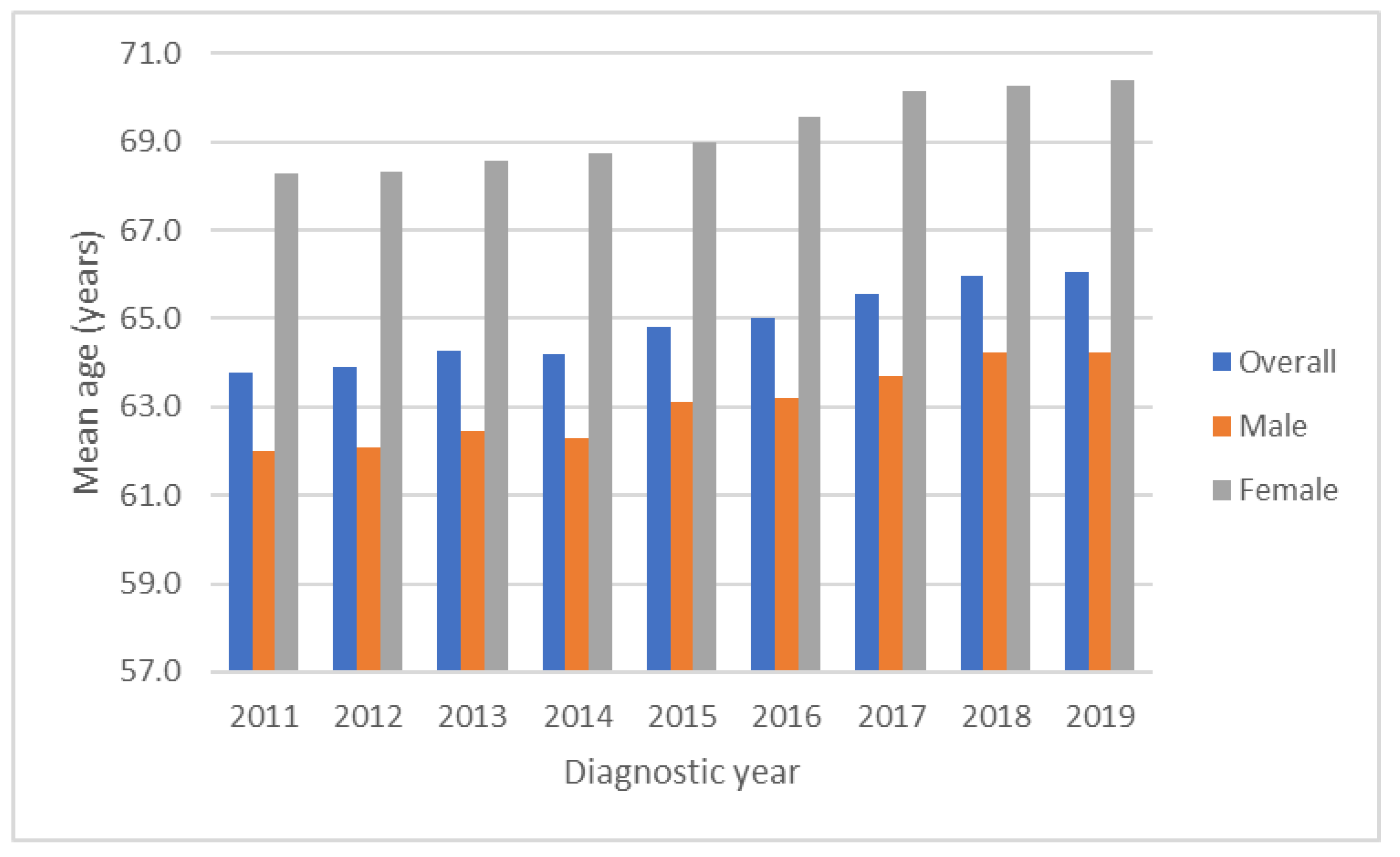
3.1. Secular Trends of Sex Ratio and Age
3.2. Secular Trends of Child–Pugh Classification
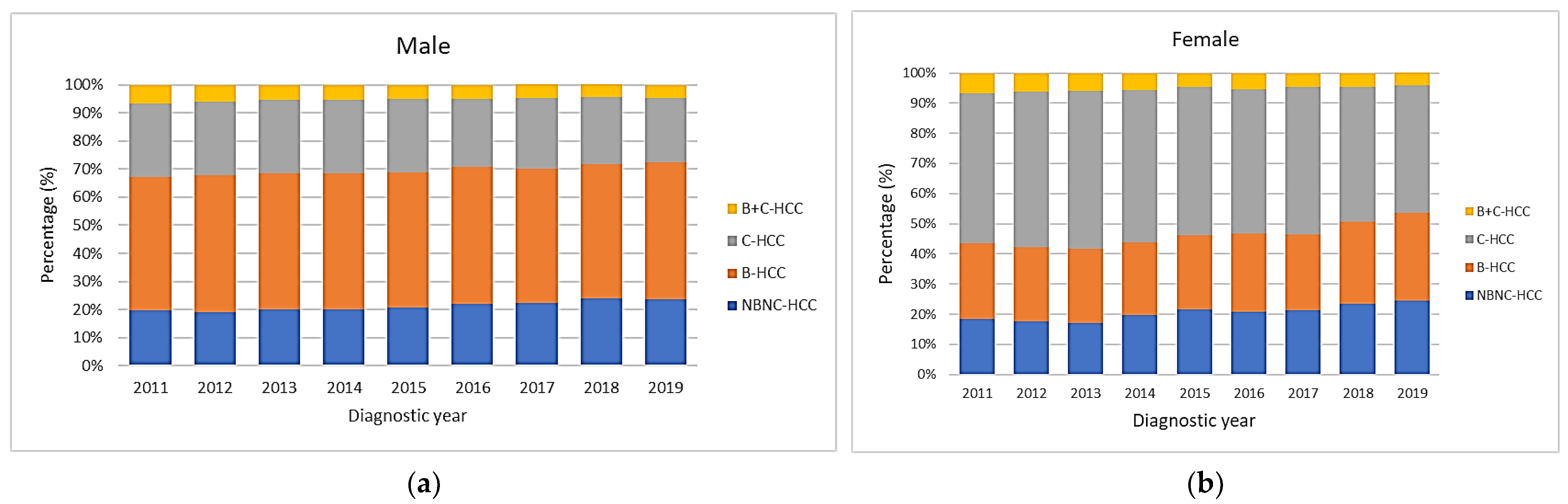
3.3. Secular Trends of Viral Etiology Based on Gender
3.4. Secular Trends of Age Based on Viral Etiology and Gender
3.5. Secular Trends of Male-to-Female Ratio Based on Viral Etiology
3.6. Secular Trends of BCLC Stages
3.7. Overall Survival and Associated Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, R.; Uchino, K.; Fujiwara, N.; Takehara, T.; Okanoue, T.; Seike, M.; Yoshiji, H.; Yatsuhashi, H.; Shimizu, M.; Torimura, T.; et al. A nationwide survey on non-B, non-C hepatocellular carcinoma in Japan: 2011-2015 update. J. Gastroenterol. 2019, 54, 367–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taiwan Cancer Registry Center. Cancer Stastistics. Available online: https://twcr.tw/?page_id=1855&lang=en (accessed on 6 October 2022).
- Beasley, R.P.; Hwang, L.Y.; Lin, C.C.; Chien, C.S. Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22 707 men in Taiwan. Lancet 1981, 2, 1129–1133. [Google Scholar] [CrossRef]
- Bennett, H.; Waser, N.; Johnston, K.M.; Kao, J.-H.; Lim, Y.-S.; Duan, Z.-P.; Lee, Y.-J.; Wei, L.; Chen, C.-J.; Sievert, W.; et al. A review of the burden of hepatitis C virus infection in China, Japan, South Korea and Taiwan. Hepatol. Int. 2015, 9, 378–390. [Google Scholar] [CrossRef]
- Chen, C.-H.; Yang, P.-M.; Huang, G.-T.; Lee, H.-S.; Sung, J.-L.; Sheu, J.-C. Estimation of Seroprevalence of Hepatitis B Virus and Hepatitis C Virus in Taiwan from a Large-scale Survey of Free Hepatitis Screening Participants. J. Formos. Med. Assoc. 2007, 106, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Chen, C.; Chen, J.; Hsu, N.; Wei, S.; Hou, S.; Lu, S.; Chen, P. Secular Trends and Geographic Maps of Hepatitis C Virus Infection among 4 Million Blood Donors in Taiwan from 1999 to 2017. Hepatol. Commun. 2020, 4, 1193–1205. [Google Scholar] [CrossRef]
- Lu, S.-N.; Su, W.-W.; Yang, S.-S.; Chang, T.-T.; Cheng, K.-S.; Wu, J.-C.; Lin, H.H.; Wu, S.-S.; Lee, C.-M.; Changchien, C.-S.; et al. Secular trends and geographic variations of hepatitis B virus and hepatitis C virus-associated hepatocellular carcinoma in Taiwan. Int. J. Cancer 2006, 119, 1946–1952. [Google Scholar] [CrossRef]
- Liu, W.-C.; Liu, Q.-Y. Molecular mechanisms of gender disparity in hepatitis B virus-associated hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 6252–6261. [Google Scholar] [CrossRef]
- Petrick, J.L.; Florio, A.A.; Znaor, A.; Ruggieri, D.; Laversanne, M.; Alvarez, C.S.; Ferlay, J.; Valery, P.C.; Bray, F.; McGlynn, K.A. International trends in hepatocellular carcinoma incidence, 1978–2012. Int. J. Cancer 2019, 147, 317–330. [Google Scholar] [CrossRef]
- Chiang, C.J.; Wang, Y.W.; Lee, W.C. Taiwan’s Nationwide Cancer Registry System of 40 years: Past, present, and future. J. Formos. Med. Assoc. 2019, 118, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.-W.; Chiang, C.-J.; Lin, L.-J.; Huang, C.-W.; Lee, W.-C.; Lee, M.-Y.; Cheng-Yi, S.; Lin, H.-L.; Lin, M.-M.; Wang, Y.-P.; et al. Accuracy of long-form data in the Taiwan cancer registry. J. Formos. Med. Assoc. 2021, 120, 2037–2041. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Chiang, C.-J.; You, S.-L.; Chen, C.-J.; Yang, Y.-W.; Lo, W.-C.; Lai, M.-S. Quality assessment and improvement of nationwide cancer registration system in Taiwan: A review. Jpn. J. Clin. Oncol. 2015, 45, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.-H.; You, S.-L.; Chen, C.-J.; Liu, C.-J.; Lai, M.-W.; Wu, T.-C.; Wu, S.-F.; Lee, C.-M.; Yang, S.-S.; Chu, H.-C.; et al. Long-term Effects of Hepatitis B Immunization of Infants in Preventing Liver Cancer. Gastroenterology 2016, 151, 472–480.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-Y.; Lin, J.-T.; Ho, H.J.; Su, C.-W.; Lee, T.-Y.; Wang, S.-Y.; Wu, C.; Wu, J.-C. Association of Nucleos(t)ide Analogue Therapy With Reduced Risk of Hepatocellular Carcinoma in Patients With Chronic Hepatitis B—A Nationwide Cohort Study. Gastroenterology 2014, 147, 143–151.e5. [Google Scholar] [CrossRef] [Green Version]
- Singal, A.K.; Singh, A.; Jaganmohan, S.; Guturu, P.; Mummadi, R.; Kuo, Y.; Sood, G.K. Antiviral Therapy Reduces Risk of Hepatocellular Carcinoma in Patients With Hepatitis C Virus–Related Cirrhosis. Clin. Gastroenterol. Hepatol. 2010, 8, 192–199. [Google Scholar] [CrossRef]
- Yu, M.L.; Lin, S.M.; Chuang, W.L.; Dai, C.Y.; Wang, J.H.; Lu, S.N.; Sheen, I.S.; Chang, W.Y.; Lee, C.M.; Liaw, Y.F. A sustained virological response to interferon or interferon/ribavirin reduces hepatocellular carcinoma and improves survival in chronic hepatitis C: A nationwide, multicentre study in Taiwan. Antivir. Ther. 2006, 11, 985–994. [Google Scholar] [CrossRef]
- Taiwan Hepatitis C Policy Guideline 2018–2025; Ministry of Health and Welfare, Executive Yuan ROC: Tapei City, Taiwan, 2019.
- Nagaoki, Y.; Hyogo, H.; Aikata, H.; Tanaka, M.; Naeshiro, N.; Nakahara, T.; Honda, Y.; Miyaki, D.; Kawaoka, T.; Takaki, S.; et al. Recent trend of clinical features in patients with hepatocellular carcinoma. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2012, 42, 368–375. [Google Scholar] [CrossRef]
- Chang, T.-S.; Hsu, N.-T.; Chen, S.-C.; Hsu, I.-L.; Lee, M.-H.; Lu, S.-N. Non-B, Non-C Hepatocellular Carcinoma in an HBV- and HCV-Endemic Area: A Community-Based Prospective Longitudinal Study. Viruses 2022, 14, 984. [Google Scholar] [CrossRef]
- Kaur, S.P.; Talat, A.; Karimi-Sari, H.; Grees, A.; Chen, H.W.; Lau, D.T.Y.; Catana, A.M. Hepatocellular Carcinoma in Hepatitis B Virus-Infected Patients and the Role of Hepatitis B Surface Antigen (HBsAg). J. Clin. Med. 2022, 11, 1126. [Google Scholar] [CrossRef] [PubMed]
- Sou, F.-M.; Wu, C.-K.; Chang, K.-C.; Lu, S.-N.; Wang, J.-H.; Hung, C.-H.; Chen, C.-H.; Kee, K.-M.; Yen, Y.-H.; Lin, M.-T.; et al. Clinical characteristics and prognosis of HCC occurrence after antiviral therapy for HCV patients between sustained and non-sustained responders. J. Formos. Med. Assoc. 2018, 118 Pt 3, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Su, T.-H.; Hu, T.-H.; Chen, C.-Y.; Huang, Y.-H.; Chuang, W.-L.; Lin, C.-C.; Wang, C.-C.; Su, W.-W.; Chen, M.-Y.; Peng, C.-Y.; et al. Four-year entecavir therapy reduces hepatocellular carcinoma, cirrhotic events and mortality in chronic hepatitis B patients. Liver Int. 2016, 36, 1755–1764. [Google Scholar] [CrossRef] [PubMed]
- Naugler, W.E.; Sakurai, T.; Kim, S.; Maeda, S.; Kim, K.; Elsharkawy, A.M.; Karin, M. Gender Disparity in Liver Cancer Due to Sex Differences in MyD88-Dependent IL-6 Production. Science 2007, 317, 121–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-H.; Lin, R.-C.; Hsu, H.-Y.; Tseng, Y.-T. Hormone replacement therapy is associated with reduced hepatocellular carcinoma risk and improved survival in postmenopausal women with hepatitis B: A nationwide long-term population-based cohort study. PLoS ONE 2022, 17, e0271790. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Steele, R.; Ray, R.; Ray, R.B. Hepatitis C virus core protein augments androgen receptor-mediated signaling. J. Virol. 2008, 82, 11066–11072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Kuo, C.-F.; Chen, W.-L.; Ou, J.-H.J. Enhancement of Hepatitis B Virus Replication by Androgen and Its Receptor in Mice. J. Virol. 2012, 86, 1904–1910. [Google Scholar] [CrossRef] [Green Version]
- White, D.L.; Liu, Y.; Garcia, J.; El-Serag, H.B.; Jiao, L.; Tsavachidis, S.; Franco, L.M.; Lee, J.-S.; Tavakoli-Tabasi, S.; Moore, D.; et al. Sex hormone pathway gene polymorphisms are associated with risk of advanced hepatitis C-related liver disease in males. Int. J. Mol. Epidemiol. Genet. 2014, 5, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Qi, W.; Wang, X.; Zhang, Y.; Han, L.; Shi, J.; Wang, G.; Liu, J.; Duan, H.; Cong, X.; et al. Signal transducer and activator of transcription 3 cooperates with androgen receptor/cell cycle-related kinase signalling pathway in the progression of hepatitis B virus infection and gender differences. J. Viral Hepat. 2022, 29, 569–578. [Google Scholar] [CrossRef]
- Yeh, S.-H.; Chiu, C.-M.; Chen, C.-L.; Lu, S.-F.; Hsu, H.-C.; Chen, D.-S.; Chen, P.-J. Somatic mutations at the trinucleotide repeats of androgen receptor gene in male hepatocellular carcinoma. Int. J. Cancer 2007, 120, 1610–1617. [Google Scholar] [CrossRef]
- Zheng, Y.; Chen, W.-L.; Ma, W.-L.M.; Chang, C.; Ou, J.-H.J. Enhancement of gene transactivation activity of androgen receptor by hepatitis B virus X protein. Virology 2007, 363, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.-H.; Changchien, C.-S.; Hu, T.-H.; Lee, C.-M.; Kee, K.-M.; Lin, C.-Y.; Chen, C.-L.; Chen, T.-Y.; Huang, Y.-J.; Lu, S.-N. The efficacy of treatment schedules according to Barcelona Clinic Liver Cancer staging for hepatocellular carcinoma—Survival analysis of 3892 patients. Eur. J. Cancer 2008, 44, 1000–1006. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.-H.; Lu, S.-N.; Chen, C.-L.; Cheng, Y.-F.; Lin, C.-Y.; Hung, C.-H.; Chen, C.-H.; Changchien, C.-S.; Hsu, H.-C.; Hu, T.-H.; et al. Hepatocellular carcinoma surveillance and appropriate treatment options improve survival for patients with liver cirrhosis. Eur. J. Cancer 2010, 46, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Hsu, Y.C.; Ho, H.J.; Chen, Y.J.; Lee, T.Y.; Lin, J.T. Association between ultrasonography screening and mortality in patients with hepatocellular carcinoma: A nationwide cohort study. Gut 2016, 65, 693–701. [Google Scholar] [CrossRef]
- Chien, R.-N.; Liaw, Y.-F. Current Trend in Antiviral Therapy for Chronic Hepatitis B. Viruses 2022, 14, 434. [Google Scholar] [CrossRef]
- Hsu, W.; Tsai, P.; Chen, C.; Tseng, K.; Lai, H.; Kuo, H.; Hung, C.; Tung, S.; Wang, J.; Chen, J.; et al. Hepatitis C virus eradication decreases the risks of liver cirrhosis and cirrhosis-related complications (Taiwanese chronic hepatitis C cohort). J. Gastroenterol. Hepatol. 2021, 36, 2884–2892. [Google Scholar] [CrossRef]
- Park, J.; Chen, M.; Colombo, M.; Roberts, L.; Schwartz, M.; Chen, P.-J.; Kudo, M.; Johnson, P.; Wagner, S.; Orsini, L.S.; et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: The BRIDGE Study. Liver Int. 2015, 35, 2155–2166. [Google Scholar] [CrossRef] [Green Version]
- Ho, M.-C.; Hasegawa, K.; Chen, X.-P.; Nagano, H.; Lee, Y.-J.; Chau, G.-Y.; Zhou, J.; Wang, C.-C.; Choi, Y.R.; Poon, R.T.-P.; et al. Surgery for Intermediate and Advanced Hepatocellular Carcinoma: A Consensus Report from the 5th Asia-Pacific Primary Liver Cancer Expert Meeting (APPLE 2014). Liver Cancer 2016, 5, 245–256. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation Barcelona Clinic Liver Cancer (BCLC) staging system: The 2022 update. J. Hepatol. 2021, 76, 681–693. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kee, K.-M.; Lu, S.-N. Hospital- and Community-Based Screenings for Hepatocellular Carcinoma in Taiwan. Oncology 2011, 81, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-H.; Lin, C.-Y.; Hsu, N.-T.; Yen, Y.-H.; Kee, K.-M.; Wang, J.-H.; Hu, T.-H.; Chen, C.-H.; Hung, C.-H.; Hu, J.-T.; et al. Reappraisal of the roles of alpha-fetoprotein in hepatocellular carcinoma surveillance using large-scale nationwide database and hospital-based information. J. Formos. Med. Assoc. 2022, 121, 2085–2092. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.X.; Mehta, N. Does Hepatocellular Carcinoma Surveillance Increase Survival in At-Risk Populations? Patient Selection, Biomarkers, and Barriers. Am. J. Dig. Dis. 2020, 65, 3456–3462. [Google Scholar] [CrossRef]
- Best, J.; Bilgi, H.; Heider, D.; Schotten, C.; Manka, P.; Bedreli, S.; Gorray, M.; Ertle, J.; van Grunsven, L.A.; Dechêne, A. The GALAD scoring algorithm based on AFP, AFP-L3, and DCP significantly improves detection of BCLC early stage hepatocellular carcinoma. Z. Gastroenterol. 2016, 54, 1296–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, J.; Bechmann, L.P.; Sowa, J.P.; Sydor, S.; Dechêne, A.; Pflanz, K.; Bedreli, S.; Schotten, C.; Geier, A.; Berg, T.; et al. GALAD Score Detects Early Hepatocellular Carcinoma in an International Cohort of Patients With Nonalcoholic Steatohepatitis. Clin. Gastroenterol. Hepatol. 2020, 18, 728–735.e4. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Univariate | Multivariate | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | ||||
| Sex | Male | 1 | 1 | ||||||
| Female | 0.901 | 0.882 | 0.919 | <0.001 | 0.916 | 0.894 | 0.938 | <0.001 | |
| Age (years) | <56 | 1 | 1 | ||||||
| 56–65 | 0.947 | 0.921 | 0.972 | <0.001 | 1.127 | 1.096 | 1.158 | <0.001 | |
| 66–75 | 1.075 | 1.046 | 1.104 | <0.001 | 1.342 | 1.304 | 1.38 | <0.001 | |
| >75 | 1.629 | 1.585 | 1.674 | <0.001 | 1.698 | 1.648 | 1.749 | <0.001 | |
| Diagnostic year | 2011 | 1 | 1 | ||||||
| 2012 | 0.954 | 0.921 | 0.988 | 0.0090 | 1.004 | 0.969 | 1.04 | 0.831 | |
| 2013 | 0.948 | 0.915 | 0.982 | 0.0030 | 0.999 | 0.964 | 1.036 | 0.961 | |
| 2014 | 0.912 | 0.88 | 0.946 | <0.001 | 0.969 | 0.934 | 1.005 | 0.092 | |
| 2015 | 0.925 | 0.892 | 0.96 | <0.001 | 0.953 | 0.918 | 0.989 | 0.012 | |
| 2016 | 0.867 | 0.835 | 0.901 | <0.001 | 0.9 | 0.865 | 0.935 | <0.001 | |
| 2017 | 0.842 | 0.81 | 0.876 | <0.001 | 0.852 | 0.819 | 0.887 | <0.001 | |
| 2018 | 0.828 | 0.794 | 0.862 | <0.001 | 0.842 | 0.807 | 0.878 | <0.001 | |
| 2019 | 0.768 | 0.734 | 0.804 | <0.001 | 0.839 | 0.8 | 0.879 | <0.001 | |
| BCLC stages | 0 | 1 | 1 | ||||||
| A | 1.472 | 1.402 | 1.545 | <0.001 | 1.288 | 1.226 | 1.352 | <0.001 | |
| B | 2.962 | 2.821 | 3.11 | <0.001 | 2.296 | 2.185 | 2.412 | <0.001 | |
| C | 7.458 | 7.113 | 7.82 | <0.001 | 4.882 | 4.65 | 5.125 | <0.001 | |
| D | 16.235 | 15.408 | 17.106 | <0.001 | 7.575 | 7.124 | 8.056 | <0.001 | |
| Hospital level, n (%) | Medical center | 1 | 1 | ||||||
| Regional hospital | 1.268 | 1.245 | 1.292 | <0.001 | 1.209 | 1.186 | 1.232 | <0.001 | |
| Body mass index (kg/m2) | Normal (18.5~24) | 1 | 1 | ||||||
| Underweight (<18.5) | 1.534 | 1.47 | 1.6 | <0.001 | 1.176 | 1.127 | 1.227 | <0.001 | |
| Overweight (>24) | 0.794 | 0.779 | 0.81 | <0.001 | 0.895 | 0.877 | 0.913 | <0.001 | |
| Unknown | 2.011 | 1.94 | 2.085 | <0.001 | 1.177 | 1.134 | 1.223 | <0.001 | |
| Smoking status | Non-smoker | 1 | 1 | ||||||
| Smoker | 1.262 | 1.238 | 1.285 | <0.001 | 1.18 | 1.155 | 1.206 | <0.001 | |
| Unknown | 2.246 | 2.081 | 2.424 | <0.001 | 1.162 | 1.074 | 1.257 | <0.001 | |
| Alcohol consumption | No | 1 | 1 | ||||||
| Yes | 1.056 | 1.035 | 1.078 | <0.001 | 1.029 | 1.008 | 1.051 | 0.007 | |
| Unknown | 1.038 | 0.948 | 1.137 | 0.4200 | 1.125 | 1.027 | 1.233 | 0.011 | |
| Alpha Fetoprotein (ng/mL) | <20 | 1 | 1 | ||||||
| 20–399 | 1.448 | 1.414 | 1.483 | <0.001 | 1.401 | 1.367 | 1.435 | <0.001 | |
| 400–5999 | 2.284 | 2.223 | 2.347 | <0.001 | 1.774 | 1.726 | 1.824 | <0.001 | |
| ≥6000 | 3.383 | 3.298 | 3.469 | <0.001 | 2.195 | 2.137 | 2.254 | <0.001 | |
| Child–Pugh class | A | 1 | 1 | ||||||
| B and C | 3.574 | 3.501 | 3.648 | <0.001 | 2.022 | 1.924 | 2.124 | <0.001 | |
| Unknown | 1.677 | 1.617 | 1.739 | <0.001 | 1.33 | 1.278 | 1.384 | <0.001 | |
| HBV and HCV status | Non-B–Non-C | 1 | 1 | ||||||
| Only HBV | 0.723 | 0.705 | 0.74 | <0.001 | 0.901 | 0.879 | 0.924 | <0.001 | |
| Only HCV | 0.764 | 0.745 | 0.783 | <0.001 | 0.897 | 0.874 | 0.921 | <0.001 | |
| HBV+HCV | 0.806 | 0.771 | 0.842 | <0.001 | 0.951 | 0.91 | 0.994 | 0.027 | |
| Unknown | 0.947 | 0.883 | 1.016 | 0.1300 | 0.742 | 0.687 | 0.802 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kee, K.-M.; Chen, C.-H.; Hu, J.-T.; Huang, Y.-H.; Wang, T.-E.; Chau, G.-Y.; Chen, K.-H.; Chen, Y.-L.; Lin, C.-C.; Hung, C.-F.; et al. Secular Trends of Clinical Characteristics and Survival of Hepatocellular Carcinoma in Taiwan from 2011 to 2019. Viruses 2023, 15, 126. https://doi.org/10.3390/v15010126
Kee K-M, Chen C-H, Hu J-T, Huang Y-H, Wang T-E, Chau G-Y, Chen K-H, Chen Y-L, Lin C-C, Hung C-F, et al. Secular Trends of Clinical Characteristics and Survival of Hepatocellular Carcinoma in Taiwan from 2011 to 2019. Viruses. 2023; 15(1):126. https://doi.org/10.3390/v15010126
Chicago/Turabian StyleKee, Kwong-Ming, Chien-Hung Chen, Jui-Ting Hu, Yi-Hsiang Huang, Tsang-En Wang, Gar-Yang Chau, Kuo-Hsin Chen, Yao-Li Chen, Chih-Che Lin, Chien-Fu Hung, and et al. 2023. "Secular Trends of Clinical Characteristics and Survival of Hepatocellular Carcinoma in Taiwan from 2011 to 2019" Viruses 15, no. 1: 126. https://doi.org/10.3390/v15010126
APA StyleKee, K. -M., Chen, C. -H., Hu, J. -T., Huang, Y. -H., Wang, T. -E., Chau, G. -Y., Chen, K. -H., Chen, Y. -L., Lin, C. -C., Hung, C. -F., Huang, S. -F., Liu, T. -W., Ku, H. -Y., Huang, B. -S., Wang, Y. -P., Tseng, H. -P., Chiang, C. -J., & Lu, S. -N. (2023). Secular Trends of Clinical Characteristics and Survival of Hepatocellular Carcinoma in Taiwan from 2011 to 2019. Viruses, 15(1), 126. https://doi.org/10.3390/v15010126