1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel strain of the long-known coronaviridae, which causes a complex of symptoms that are initially and predominantly respiratory in nature [
1]. SARS-CoV-2 has been categorized as a positive sense single-strand RNA virus that is highly contagious. The SARS-CoV-2 was first identified in Wuhan, China, in 2019, forcing the World Health Organization (WHO) to declare an outbreak of crucial public health emergency and concern in January 2020 and a pandemic by March 2020 [
2]. After its initial outbreak in Wuhan, WHO recommended the name 2019 novel coronavirus as a provisional name, however, by February, the international committee on taxonomy of virus officially recommended the name severe acute respiratory syndrome coronavirus 2 [
3].
After identifying the first case of COVID-19 in China in 2019, the disease started to spread at a very high rate among humans in various parts of the globe, mainly through tiny droplets in the air that occur as a result of sneezing and coughing [
4]. Some key symptoms that the COVID-19 patients recorded include fatigue, fever, loss of sense of smell, and dry cough.
The COVID-19 cases in Central Europe, France were first reported in January 2020, where three cases were detected, and the first death was also reported in the same location in February 2020 [
5]. Later on, COVID-19 cases spread to other parts of Europe, causing numerous deaths that resulted in the creation and implementation of COVID-19 mitigation guidelines to contain the disease in Central Europe and other parts of the globe [
6], as well as unprecedented efforts to understand the pathogenicity of SARS-CoV-2 [
7].
There are numerous COVID-19 vaccines available and administered in various parts of the globe [
8]. However, the vital COVID-19 vaccines available in Germany include, first, the vector-based ChAdOx-1 nCOV-19 vaccine (
Vaxzevria, Oxford/AstraZeneca, UK) hereinafter referred to as
AZE, which was recommended for people above 60 years of age and at high risk of contracting the disease because of its age-dependent safety profile [
9]. Due to rare but severe thrombotic complications, this vaccine is no longer recommended [
10]. Secondly, the BNT162b2 vaccine (Comirnaty, BioNTech/Pfizer, Mainz, Germany), hereinafter referred to as
BNT, is administered to people 5 years of age and above. Both mRNA-1273 and BNT162b2 are mRNA-based vaccines. Thirdly, the mRNA-1273 (Spikevax, Moderna, Cambridge, MA, USA) vaccine, hereinafter referred to as
MOD, which is considered effective and safe, particularly for people 30 years of age and above [
11]. The vaccine is also be given to individuals who had previously contracted the coronavirus. For a complete immunization, two repeated doses of the same vaccine are necessary. However, due to vaccine availability, a combination of different vaccines has been also accepted as a full immunization. Since antibody titers are reduced with time, a booster vaccination 6 months after a full vaccination is deemed to be necessary for continued protection [
12].
The COVID-19 vaccine administered triggers numerous side effects (SE) and reactions [
13,
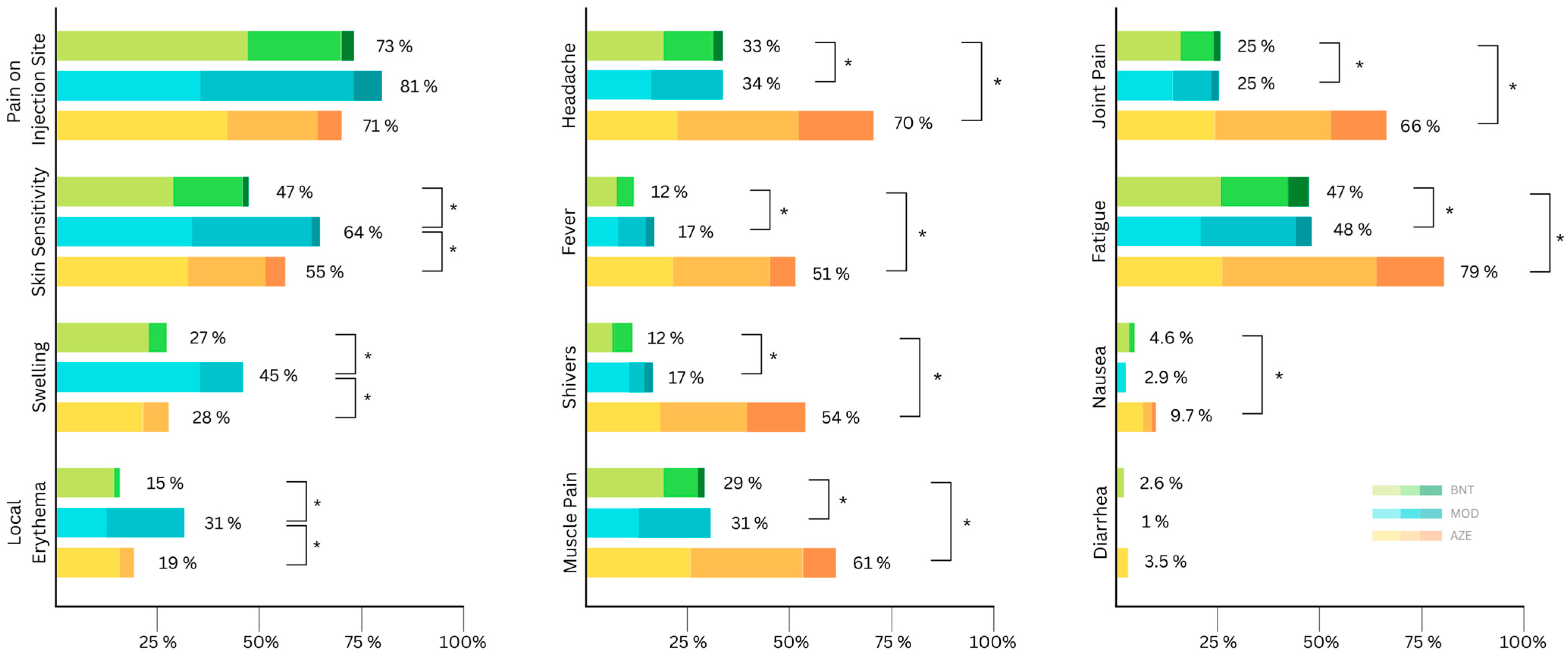
14]. Acute side effects after a COVID-19 vaccine can be classified into two groups: local and systemic side effects. Local side effects include swelling, redness, pain on the injection site, and skin sensitivity. Systemic side effects include fatigue, diarrhea, nausea, muscle pain, joint pain, headache, shivering, and fever [
15]. Most of the reported side effects usually diminish in a few days, however, on rare occasions, severe side effects such as anaphylaxis [
16] and thrombotic events were reported [
17,
18].
Vaccine side effects are one of the reasons for reluctance to vaccinate [
19]. In this study, we systematically investigated self-reported vaccine side effects after the first, second, and booster vaccinations.
2. Materials and Methods
The data were collected during the TüSeRe:exact Study (Tübinger Monitoring Studie zur exakten Analyse der Immunantwort nach Vakzinierung). TüSeRe:exact study aims to investigate the longitudinal changes in antibody levels after COVID-19 vaccines. Employees from the University Hospital Tübingen, the Center for Clinical Transfusion Medicine and Natural and Medical Sciences Institute Reutlingen were invited via e-mail to participate in the study.
Study participants were asked to fill out an online questionnaire and report side effects after receiving first, second, and booster vaccinations [
20]. Regarding local side effects at the injection site, the probands were asked about were pain, skin sensitivity, swelling, and redness (i.e., erythema). The systemic side effects we asked about were headache, fever, shivers, generalized muscle pain, joint pain, fatigue, nausea, and diarrhea. These were acquired on an ordinal scale as follows: none, mild, moderate, severe.
Data are expressed as % (
n) or as mean ± standard deviation (SD). The Mann–Whitney U test was used to test continuous variables. The frequency of adverse events was compared between vaccines using the Fisher’s exact test with Bonferroni correction. The severity of side effects was compared using the Kruskal–Wallis test with Dunn–Bonferroni correction between the different vaccines. A
p < 0.05 is considered statistically significant. We used DATAtab: Online Statistics Calculator for statistical analysis (DATAtab e.U. Graz, Austria,
https://datatab.net (accessed on 15 October 2022)). Multivariate analysis with a generalized linear model (GLM) and an adjustment for dependencies of observation between different vaccinations in the same subject (GEE, Generalized Estimating Equations) was performed using SPSS Version 29 (IBM Inc, Armonk, NY, USA). The presence of local and systemic side effects was included as a dependent parameter in the model. Variables were included in the models according to their statistical significance in univariate logistic regression analysis (
p ≤ 0.1). Odds ratios (OR) with 95% confidence intervals (95%CI) were calculated.
4. Discussion
Dominating not only the scientific efforts of the last two and a half years globally but also the mainstream media, the topic of COVID-19 has caused an unprecedented social division in ethical, medical, scientific, and socio-political standpoints. Misinformation has reached a new peak. By continuing the effort of monitoring both the subjective position of the population receiving vaccines as well as collecting quantifiable and absolute data on the immune response, we are able to enhance trust in scientific research, can prove the effectiveness of vaccines, or raise concern by monitoring vaccine breakthroughs. As of today, the COVID-19 pandemic is continuing, thus the scientific effort around the multi-faceted subject matter of COVID-19 should continue.
In the current study, we investigated self-reported acute side effects after first, second and third vaccinations. After the first vaccination, although local side effects were more common after mRNA vaccines, systemic side effects were more common and severe after AZE. Similarly, Briggs et al. reported a higher side effect rate after receiving AZE compared to BNT after the first dose [
21]. Furthermore, Klugar et al. compared mRNA-based and viral vector based COVID-19 vaccines among healthcare workers after receiving the first vaccination [
22]. Similar to our findings, while local side effects were more common after receiving mRNA-based vaccines compared to viral vector-based vaccines (78.3% vs 70.4%), systemic side effects were more frequent after viral vector-based vaccines (62% vs 87%) [
22]. The fact that a vector vaccine carries both the antigen and the viral vector, and both can elicit an immune response, it may explain the higher reactogenicity of vector vaccines [
23]. Furthermore, high prevalence of adenoviral diseases in the community and the consecutive pre-existing immune mechanisms might also contribute to these findings [
24,
25].
In further analysis of our data, we observed that local side effects were more common after MOD compared to BNT, however, only some systemic symptoms were significantly different between BNT and MOD. Previous studies reported a higher side effect rate after MOD compared to BNT [
26]. Both vaccines are mRNA-based and are packed in lipid particles and contain no adjuvants. However, potentially explaining the difference, is the dose per injection, which is significantly higher in MOD (100 µg) compared to BNT (30 µg).
After the second dose, the frequency of side effects reduced if AZE was administered. Kaur et al. investigated local and systemic side effects after vaccination with AZE in health care workers [
13]. Similar to our findings, they found that side effects are more common after the first dose compared to the second dose [
13]. This effect may be in part explained by the adjustment of the German vaccination recommendations. AZE recipients were significantly older. As Ramasamy et al. have shown, the tolerance of AZE is higher in older adults [
27]. On the other hand, we found that compared to the first dose, the number of individuals reporting systemic side effects increased among those receiving an mRNA vaccine as a second dose. This finding is in accordance with the literature. El-Shitany et al. also reported an increased side effect rate after a second dose of BNT compared to the first vaccine dose [
15]. It can be explained through a two-fold mechanism: the build-up of long-lasting memory T-cells and B-cells facilitates a faster and more intense immune response. And as discussed by Yao et al., a more recent finding suggests an additional role of the cells of the innate immune system in contributing to a well-prepared immune response upon a second encounter with an immunogen. This phenomenon is referred to as trained immunity [
28].
For primary vaccination, a second vaccine dose with the same vaccine is recommended. However, due to limited vaccine availability, heterologous vaccine regimes were also approved by regulatory agencies [
29]. Furthermore, heterologous vaccination provides a better immunogenicity compared to homologous vaccination [
30]. We further investigated whether heterologous vaccination influenced the side effect frequency. Both local and systemic side effects were more common in individuals receiving MOD or BNT after AZE compared to those who received two doses of AZE. Hillus et al. recently found systemic reactions in 49% of vaccinations after heterologous AZE–BNT vaccination, and in 39% after homologous AZE–AZE [
31]. Baldolli et al. investigated the side effect rate after heterologous vaccination in health care workers [
32]. In accordance with our findings, individuals receiving the mRNA-1273 vaccine reported more local and systemic symptoms compared with those receiving the BNT162b2 vaccine after AZE [
32].
Due to declining antibody titers, booster vaccination was recommended to prolong protection against COVID-19. Furthermore, it has been shown that the antibodies that are developed after vaccines using the spike protein of a wild-type virus have a limited neutralization ability against new variants of the virus [
33]. A third vaccination improves the antibody binding to the omicron variant [
33]. Most of the participants in our study received BNT as a booster. Local side effects were more common after MOD compared to BNT in booster vaccination.
Age and gender might affect the reactogenicity to COVID-19 vaccination [
14,
15,
34]. Using multivariate analyses, we investigated possible confounders. Differences between vaccines remained significant after adjustment. In agreement with previous studies [
15,
35], multivariate analyses in our study revealed a tendency to local and systemic SE in participants older than 45 years of age. Furthermore, females reported more side effects compared to males in our cohort. These results indicated that age and sex were associated with vaccine side effects and that these effects should be considered when interpreting the results of similar studies investigating reactogenicity after COVID-19 vaccination.
We also found that people with skin diseases had a higher odds ratio for local SE but not for systemic SE. Similarly, cardiovascular diseases were associated with higher systemic SE. These findings might be important in pre-vaccination information. However, further studies are needed to better understand this phenomenon. However, these results should be interpreted cautiously because the number of persons with investigated comorbidities was small.
Prior COVID-19 infection might be associated with more frequent and severe SE after COVID-19 vaccination [
35]. However, in the current study, previous COVID-19 infection was not found to be associated with SE. We believe the low number of participants with prior COVID-19 infection (3%) precludes any certain association.
The strengths of our study are the collection of real-world data in a special population after different vaccine schemes and high study adherence after the 1st, 2nd, and booster vaccinations.
Still, our study has limitations. First, the number of participants was relatively small compared to other population-based side effect studies supported by government agencies. However, this study targeted a specific occupational group and included around 1000 participants. In addition, the continuous follow-up of study participants allowed the collection of data on adverse events after the 1st, 2nd, and 3rd vaccinations, and to study the effect of different vaccination regimens. Second, the study population consisted mainly of women. In Germany, approximately 75% of health care workers are female [
36]. Therefore, the gender distribution reflects the population under study. Third, side effects were collected using a pre-formed online questionnaire, which might cause the underreporting of rare side effects. Online questionnaires and applications have recently been increasingly used to collect information for medical studies when face-to-face interviews are not possible because of contact limitations. On the other hand, the studied population consisted of health professionals who can be assumed to have the necessary health literacy to understand and answer the health-related questions.


 ,
, 





{kind=link}
{kind=link}
{kind=link}