
Optimizing Antiretroviral Therapy in Heavily ART-Experienced Patients with Multi-Class Resistant HIV-1 Using Proviral DNA Genotypic Resistance Testing
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
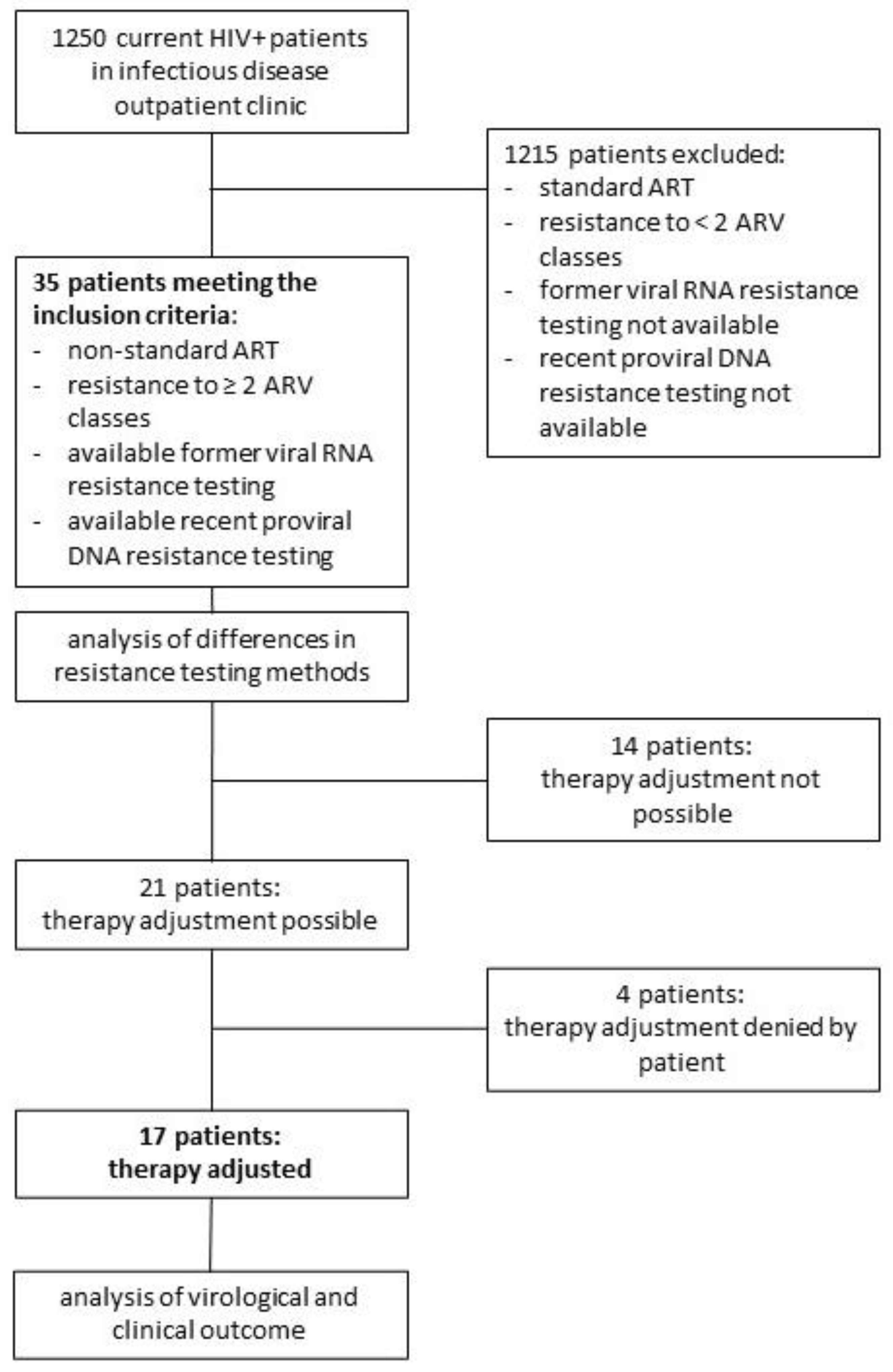
2.1. Study Design and Population
2.2. Resistance Analysis
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Characteristics of the Patient Group
3.2. Analysis and Comparison of Detected Resistance Mutations in Viral RNA and Proviral DNA
3.2.1. NRTI-Associated Resistance Mutations
3.2.2. PI associated Resistance Mutations
3.2.3. NNRTI-Associated Resistance Mutations
3.2.4. INI-Resistance-Associated Resistance Mutations
3.2.5. Comparison of Resistance Mutations between Viral RNA and Proviral DNA—Higher Frequency of Resistance Mutations in Viral RNA
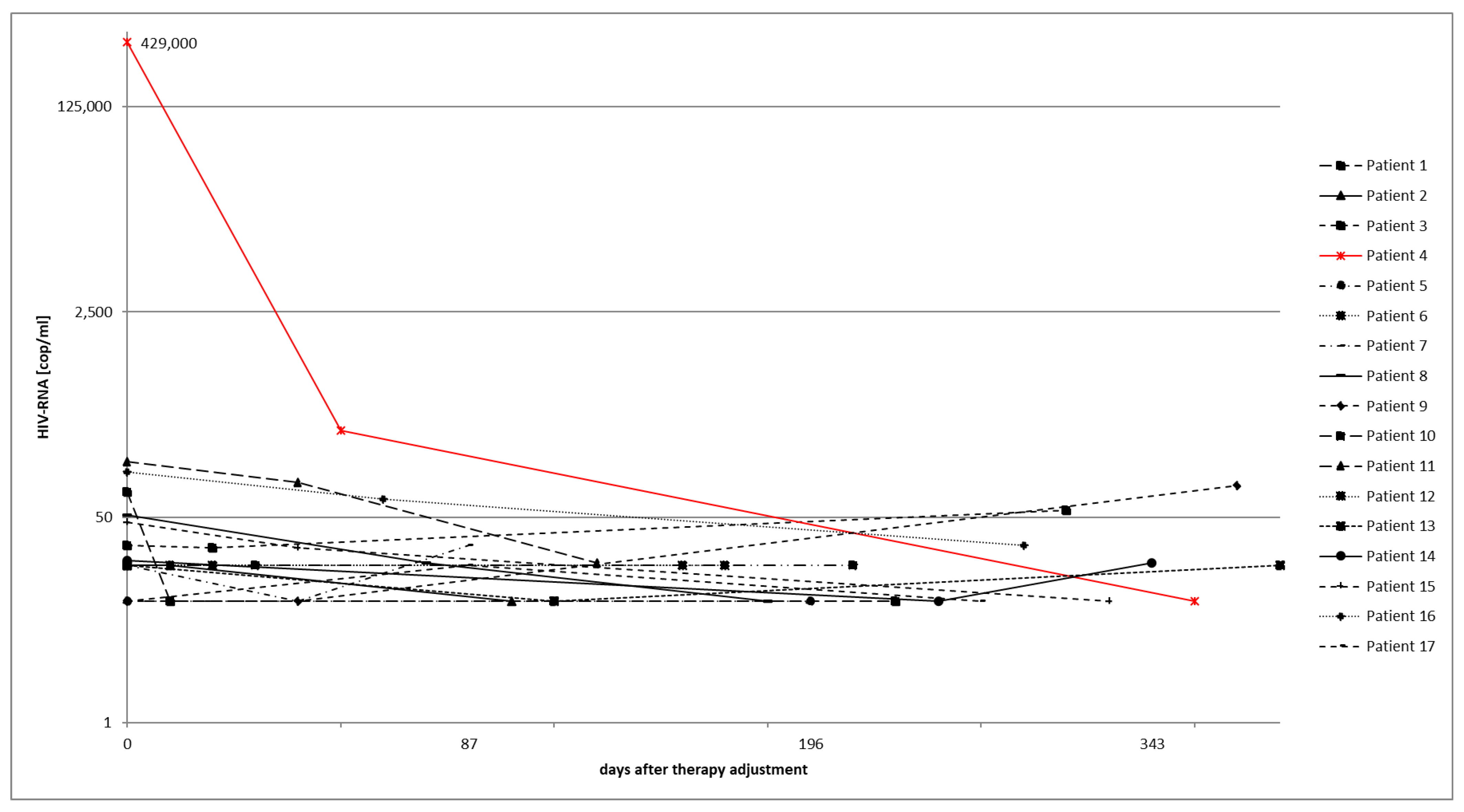
3.3. Virological Course after Therapy Adjustment
3.4. Reduction in Daily Pill Intake and Number of Drug Classes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marcus, J.L.; Leyden, W.A.; Alexeeff, S.E.; Anderson, A.N.; Hechter, R.C.; Hu, H.; Lam, J.O.; Towner, W.J.; Yuan, Q.; Horberg, M.A.; et al. Comparison of Overall and Comorbidity-Free Life Expectancy Between Insured Adults with and without HIV Infection, 2000–2016. JAMA Netw. Open 2020, 3, e207954. [Google Scholar] [CrossRef] [PubMed]
- Mauskopf, J.; Fernandez, M.M.; Ghosn, J.; Sax, P.; Priest, J.; Garris, C.; Clark, A. 2510 Systematic Literature Review of Multiclass Resistance in Heavily Treatment Experienced Persons with, H.I.V. Open Forum Infect. Dis. 2019, 6 (Suppl. 2), S871. [Google Scholar] [CrossRef]
- Miranda, M.N.S.; Pingarilho, M.; Pimentel, V.; Martins, M.d.R.O.; Kaiser, R.; Seguin-Devaux, C.; Paredes, R.; Zazzi, M.; Incardona, F.; Abecasis, A.B. Trends of Transmitted and Acquired Drug Resistance in Europe From 1981 to 2019: A Comparison Between the Populations of Late Presenters and Non-late Presenters. Front. Microbiol. 2022, 13, 846943. [Google Scholar] [CrossRef] [PubMed]
- Eaton, E.F.; McDavid, C.; Banasiewicz, M.K.; Mugavero, M.J.; Knight, S.J. Patient preferences for antiretroviral therapy: Effectiveness, quality of life, access and novel delivery methods. Patient Prefer. Adherence 2017, 11, 1585–1590. [Google Scholar] [CrossRef] [Green Version]
- Onoya, D.; Hirasen, K.; van den Berg, L.; Miot, J.; Long, L.C.; Fox, M.P. Adverse Drug Reactions Among Patients Initiating Second-Line Antiretroviral Therapy in South Africa. Drug. Saf. 2018, 41, 1343–1353. [Google Scholar] [CrossRef] [Green Version]
- Burgoyne, R.W.; Tan, D.H.S. Prolongation and quality of life for HIV-infected adults treated with highly active antiretroviral therapy (HAART): A balancing act. J. Antimicrob. Chemother. 2008, 61, 469–473. [Google Scholar] [CrossRef] [Green Version]
- What’s New in the Guidelines?|NIH [Internet]. Available online: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv/whats-new-guidelines (accessed on 25 February 2022).
- Lübke, N.; Di Cristanziano, V.; Sierra, S.; Knops, E.; Schülter, E.; Jensen, B.; Oette, M.; Lengauer, T.; Kaiser, R. Proviral DNA as a Target for HIV-1 Resistance Analysis. Intervirology 2015, 58, 184–189. [Google Scholar] [CrossRef]
- Caetano, D.G.; Côrtes, F.H.; Bello, G.; Teixeira, S.L.M.; Hoagland, B.; Grinsztejn, B.; Gonçalves Veloso, V.; Lindenmeyer Guimarães, M.; Gonçalves Morgado, M. Next-generation sequencing analyses of the emergence and maintenance of mutations in CTL epitopes in HIV controllers with differential viremia control. Retrovirology 2018, 15, 62. [Google Scholar] [CrossRef]
- Chun, T.W.; Stuyver, L.; Mizell, S.B.; Ehler, L.A.; Mican, J.A.; Baseler, M.; Lloyd, A.L.; Nowak, M.A.; Fauci, A.S. Presence of an inducible HIV-1 latent reservoir during highly active antiretroviral therapy. Proc. Natl. Acad. Sci. USA 1997, 94, 13193–13197. [Google Scholar] [CrossRef] [Green Version]
- Chew, C.B.; Potter, S.J.; Wang, B.; Wang, Y.M.; Shaw, C.O.; Dwyer, D.E.; Saksena, N.K. Assessment of drug resistance mutations in plasma and peripheral blood mononuclear cells at different plasma viral loads in patients receiving HAART. J. Clin. Virol. Off. Publ. Pan. Am. Soc. Clin. Virol. 2005, 33, 206–216. [Google Scholar] [CrossRef]
- Trémeaux, P.; Lenfant, T.; Boufassa, F.; Essat, A.; Mélard, A.; Gousset, M.; Delelis, O.; Viard, J.P.; Bary, M.; Goujard, C.; et al. Increasing contribution of integrated forms to total HIV DNA in blood during HIV disease progression from primary infection. EBioMedicine 2019, 41, 455–464. [Google Scholar] [CrossRef] [Green Version]
- Jain, V.; Hartogensis, W.; Bacchetti, P.; Hunt, P.W.; Hatano, H.; Sinclair, E.; Epplin, L.; Lee, T.-H.; Busch, M.P.; McCune, J.M.; et al. Antiretroviral therapy initiated within 6 months of HIV infection is associated with lower T-cell activation and smaller HIV reservoir size. J. Infect. Dis. 2013, 208, 1202–1211. [Google Scholar] [CrossRef] [Green Version]
- Abrahams, M.R.; Joseph, S.B.; Garrett, N.; Tyers, L.; Moeser, M.; Archin, N.; Council, O.D.; Matten, D.; Zhou, S.; Doolabh, D.; et al. The replication-competent HIV-1 latent reservoir is primarily established near the time of therapy initiation. Sci. Transl. Med. 2019, 11, eaaw5589. [Google Scholar] [CrossRef]
- Brooks, K.; Jones, B.R.; Dilernia, D.A.; Wilkins, D.J.; Claiborne, D.T.; McInally, S.; Gilmour, J.; Kilembe, W.; Joy, J.B.; Allen, S.A.; et al. HIV-1 variants are archived throughout infection and persist in the reservoir. PLoS Pathog. 2020, 16, e1008378. [Google Scholar] [CrossRef]
- Wagner, T.A.; McKernan, J.L.; Tobin, N.H.; Tapia, K.A.; Mullins, J.I.; Frenkel, L.M. An increasing proportion of monotypic HIV-1 DNA sequences during antiretroviral treatment suggests proliferation of HIV-infected cells. J. Virol. 2013, 87, 1770–1778. [Google Scholar] [CrossRef] [Green Version]
- Ellis, K.E.; Nawas, G.T.; Chan, C.; York, L.; Fisher, J.; Connick, E.; Zangeneh, T.T. Clinical Outcomes Following the Use of Archived Proviral HIV-1 DNA Genotype to Guide Antiretroviral Therapy Adjustment. Open Forum Infect. Dis. 2020, 7, ofz533. [Google Scholar] [CrossRef]
- Meybeck, A.; Alidjinou, E.K.; Huleux, T.; Boucher, A.; Tetart, M.; Choisy, P.; Bocket, L.; Ajana, F.; Robineau, O. Virological Outcome After Choice of Antiretroviral Regimen Guided by Proviral HIV-1 DNA Genotyping in a Real-Life Cohort of HIV-Infected Patients. AIDS Patient Care STDs 2020, 34, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Update of Recommendations on First- and Second-Line Antiretroviral Regimens; World Health Organization: Geneva, Switzerland, 2019; (WHO/CDS/HIV/19.15). Licence: CC BY-NC-SA 3.0 IGO [Internet]. Available online: https://apps.who.int/iris/bitstream/handle/10665/325892/WHO-CDS-HIV-19.15-eng.pdf (accessed on 30 May 2023).
- Marlowe, N.; Dileanis, J.; Elbeik, T. Evaluation of Applied Biosystems ViroSeqTM HIV-1 Genotyping System Version 2 for the Detection of Drug Resistance Mutations in Research Clinical Plasma Samples. In Durban, South Africa. 2000. Available online: https://tools.thermofisher.com/content/sfs/brochures/cms_039715.pdf (accessed on 13 June 2023).
- Lapointe, H.R.; Dong, W.; Lee, G.Q.; Bangsberg, D.R.; Martin, J.N.; Mocello, A.R.; Boum, Y.; Karakas, A.; Kirkby, D.; Poon, A.F.Y.; et al. HIV Drug Resistance Testing by High-Multiplex “Wide” Sequencing on the MiSeq Instrument. Antimicrob. Agents Chemother. 2015, 59, 6824–6833. [Google Scholar] [CrossRef] [Green Version]
- Rhee, S.Y.; Gonzales, M.J.; Kantor, R.; Betts, B.J.; Ravela, J.; Shafer, R.W. Human immunodeficiency virus reverse transcriptase and protease sequence database. Nucleic Acids Res. 2003, 31, 298–303. [Google Scholar] [CrossRef] [Green Version]
- Krentz, H.B.; John Gill, M. Long-term HIV/AIDS survivors: Patients living with HIV infection retained in care for over 20 years. What have we learned? Int. J. STD AIDS 2018, 29, 1098–1105. [Google Scholar] [CrossRef]
- Clutter, D.S.; Jordan, M.R.; Bertagnolio, S.; Shafer, R.W. HIV-1 drug resistance and resistance testing. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2016, 46, 292–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaugerre, C.; Braun, J.; Charreau, I.; Delarue, S.; Nere, M.L.; de Castro, N.; May, T.; Marchou, B.; Simon, F.; Molina, J.M.; et al. Comparison of resistance mutation patterns in historical plasma HIV RNA genotypes with those in current proviral HIV DNA genotypes among extensively treated patients with suppressed replication. HIV Med. 2012, 13, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Derache, A.; Shin, H.S.; Balamane, M.; White, E.; Israelski, D.; Klausner, J.D.; Freeman, A.H.; Katzenstein, D. HIV drug resistance mutations in proviral DNA from a community treatment program. PLoS ONE 2015, 10, e0117430. [Google Scholar] [CrossRef] [Green Version]
- Geretti, A.M.; Conibear, T.; Hill, A.; Johnson, J.A.; Tambuyzer, L.; Thys, K.; Vingerhoets, J.; Van Delft, Y. Sensitive testing of plasma HIV-1 RNA and Sanger sequencing of cellular HIV-1 DNA for the detection of drug resistance prior to starting first-line antiretroviral therapy with etravirine or efavirenz. J. Antimicrob. Chemother. 2014, 69, 1090–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wirden, M.; Soulie, C.; Valantin, M.A.; Fourati, S.; Simon, A.; Lambert-Niclot, S.; Bonmarchand, M.; Clavel-Osorio, C.; Marcelin, A.-G.; Katlama, C.; et al. Historical HIV-RNA resistance test results are more informative than proviral DNA genotyping in cases of suppressed or residual viraemia. J. Antimicrob. Chemother. 2011, 66, 709–712. [Google Scholar] [CrossRef] [Green Version]
- Verhofstede, C.; Noë, A.; Demecheleer, E.; De Cabooter, N.; Van Wanzeele, F.; Van Der Gucht, B.; Vogelaers, D.; Plum, J. Drug-resistant variants that evolve during nonsuppressive therapy persist in HIV-1-infected peripheral blood mononuclear cells after long-term highly active antiretroviral therapy. J. Acquir. Immune Defic. Syndr. 2004, 35, 473–483. [Google Scholar] [CrossRef]
- Falasca, F.; Montagna, C.; Maida, P.; Bucci, M.; Fantauzzi, A.; Mezzaroma, I.; Turriziani, O. Analysis of intracellular human immunodeficiency virus (HIV)-1 drug resistance mutations in multi-failed HIV-1-infected patients treated with a salvage regimen: 72-week follow-up. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2013, 19, E318–E321. [Google Scholar] [CrossRef] [Green Version]
- Gantner, P.; Morand-Joubert, L.; Sueur, C.; Raffi, F.; Fagard, C.; Lascoux-Combe, C.; Salmon, D.; Amiel, C.; Lambert-Niclot, S.; Fofana, D.B.; et al. Drug resistance and tropism as markers of the dynamics of HIV-1 DNA quasispecies in blood cells of heavily pretreated patients who achieved sustained virological suppression. J. Antimicrob. Chemother. 2016, 71, 751–761. [Google Scholar] [CrossRef] [Green Version]
- Boukli, N.; Boyd, A.; Collot, M.; Meynard, J.L.; Girard, P.M.; Morand-Joubert, L. Utility of HIV-1 DNA genotype in determining antiretroviral resistance in patients with low or undetectable HIV RNA viral loads. J. Antimicrob. Chemother. 2018, 73, 3129–3136. [Google Scholar] [CrossRef]
- Zaccarelli, M.; Santoro, M.M.; Armenia, D.; Borghi, V.; Gennari, W.; Gori, C.; Forbici, F.; Bertoli, A.; Fabeni, L.; Giannetti, A. Genotypic resistance test in proviral DNA can identify resistance mutations never detected in historical genotypic test in patients with low level or undetectable, HIV-RNA. J. Clin. Virol. Off. Publ. Pan. Am. Soc. Clin. Virol. 2016, 82, 94–100. [Google Scholar] [CrossRef]
- Diallo, K.; Murillo, W.E.; de Rivera, I.L.; Albert, J.; Zhou, Z.; Nkengasong, J.; Zhang, G.; Sabatier, J.F.; Yang, C. Comparison of HIV-1 resistance profiles in plasma RNA versus PBMC DNA in heavily treated patients in Honduras, a resource-limited country. Int. J. Mol. Epidemiol. Genet. 2012, 3, 56–65. [Google Scholar]
- Geretti, A.M.; Blanco, J.L.; Marcelin, A.G.; Perno, C.F.; Stellbrink, H.J.; Turner, D.; Zengin, T. HIV DNA Sequencing to Detect Archived Antiretroviral Drug Resistance. Infect. Dis. Ther. 2022, 11, 1793–1803. [Google Scholar] [CrossRef]
- Ma, R.; Jung, T.H.; Peduzzi, P.N.; Brown, S.T.; Kyriakides, T.C. Analysis of the Impact of Antiretroviral Drug Changes on Survival of Patients with Advanced-Stage AIDS with Multidrug-Resistant HIV Infection. J. Int. Assoc. Provid. AIDS Care 2019, 18, 2325958219849101. [Google Scholar] [CrossRef] [Green Version]
- Krentz, H.B.; Cosman, I.; Lee, K.; Ming, J.M.; Gill, M.J. Pill burden in HIV infection: 20 years of experience. Antivir. Ther. 2012, 17, 833–840. [Google Scholar] [CrossRef] [Green Version]
- Doctor, J. Anticholinergic Medications Associated with Falls and Frailty in People Ageing with HIV [Internet]. 2022. Virtual. Available online: https://www.croiconference.org/abstract/anticholinergic-medications-associated-with-falls-and-frailty-in-people-with-hiv/ (accessed on 29 May 2022).
- Schoen, J.C.; Erlandson, K.M.; Anderson, P.L. Clinical pharmacokinetics of antiretroviral drugs in older persons. Expert. Opin. Drug. Metab. Toxicol. 2013, 9, 573–588. [Google Scholar] [CrossRef] [Green Version]
- Nachega, J.B.; Parienti, J.J.; Uthman, O.A.; Gross, R.; Dowdy, D.W.; Sax, P.E.; Gallant, J.E.; Mugavero, M.J.; Mills, E.J.; Giordano, T.P. Lower pill burden and once-daily antiretroviral treatment regimens for HIV infection: A meta-analysis of randomized controlled trials. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2014, 58, 1297–1307. [Google Scholar] [CrossRef] [Green Version]
- Martin, M.; Del Cacho, E.; Codina, C.; Tuset, M.; De Lazzari, E.; Mallolas, J.; Miró, J.-M.; Gatell, J.M.; Ribas, J. Relationship between adherence level, type of the antiretroviral regimen, and plasma HIV type 1 RNA viral load: A prospective cohort study. AIDS Res. Hum. Retrovir. 2008, 24, 1263–1268. [Google Scholar] [CrossRef] [Green Version]
- Airoldi, M.; Zaccarelli, M.; Bisi, L.; Bini, T.; Antinori, A.; Mussini, C.; Bai, F.; Orofino, G.; Sighinolfi, L.; Gori, A.; et al. One-pill once-a-day HAART: A simplification strategy that improves adherence and quality of life of HIV-infected subjects. Patient Prefer. Adherence 2010, 4, 115–125. [Google Scholar]
- Mannheimer, S.B.; Matts, J.; Telzak, E.; Chesney, M.; Child, C.; Wu, A.W.; Friedland, G. Quality of life in HIV-infected individuals receiving antiretroviral therapy is related to adherence. AIDS Care 2005, 17, 10–22. [Google Scholar] [CrossRef]
- Chounta, V.; Overton, E.T.; Mills, A.; Swindells, S.; Benn, P.D.; Vanveggel, S.; van Solingen-Ristea, R.; Wang, Y.; Hudson, K.J.; Shaefer, M.S.; et al. Patient-Reported Outcomes Through 1 Year of an HIV-1 Clinical Trial Evaluating Long-Acting Cabotegravir and Rilpivirine Administered Every 4 or 8 Weeks (ATLAS-2M). Patient 2021, 14, 849–862. [Google Scholar] [CrossRef]
- Varghese, V.; Wang, E.; Babrzadeh, F.; Bachmann, M.H.; Shahriar, R.; Liu, T.; Mappala, S.J.M.; Gharizadeh, B.; Fessel, W.J.; Katzenstein, D.; et al. Nucleic acid template and the risk of a PCR-Induced HIV-1 drug resistance mutation. PLoS ONE 2010, 5, e10992. [Google Scholar] [CrossRef] [PubMed]
- Goodman, D.D.; Zhou, Y.; Margot, N.A.; McColl, D.J.; Zhong, L.; Borroto-Esoda, K.; Miller, M.D.; Svarovskaia, E.S. Low level of the K103N HIV-1 above a threshold is associated with virological failure in treatment-naive individuals undergoing efavirenz-containing therapy. AIDS 2011, 25, 325. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.T.; Bedimo, R.; Hoy, J.F.; Landovitz, R.J.; Smith, D.M.; Eaton, E.F.; Lehmann, C.; Springer, S.A.; Sax, P.E.; Thompson, M.A.; et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2022 Recommendations of the International Antiviral Society–USA Panel. JAMA 2023, 329, 63–84. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 35) | Results |
|---|---|
| demographics | |
| age, years, median (range) | 60 (26–79) |
| female gender, % | 26 |
| ethnicity, caucasian, % | 82 |
| comorbidity | |
| coinfection with hepatitis virus (HBV, HCV), % | 40 |
| chronic kidney disease, % | 9 |
| atherosclerotic vascular diesases, % | 26 |
| arterial hypertension, % | 40 |
| diabetes mellitus, % | 11 |
| psychiatric diagnosis, % | 29 |
| HIV parameters | |
| years of HIV infection, median (range) | 27 (5–35) |
| CDC stage 3, % | 69 |
| HIV subtype B, % | 69 |
| R5 tropism, % | 45 |
| current CD4 count, cells/µL, median (range) | 500 (100–1370) |
| current CD4 count, %, median (range) | 23.55 (9–48) |
| Nadir CD4 count, cells/µL, median (range) | 110 (0–440) |
| maximum viral load, cop/mL, median (range) | 308,956 (13,500–6,822,000) |
| antiretroviral therapy data | |
| duration of ART, years, median (range) | 22 (5–26) |
| history of mono/dual therapy, % | 49 |
| number of ART regimens, mean (range) | 10 (2–18) |
| 5 ARV classes in history, % | 46 |
| number of ARV classes in current regime, mean (range) | 3 (1–4) |
| years of viral suppression, median (range) | 8 (0–16) |
| Characteristics (n = 35) | Results |
|---|---|
| resistance situation | |
| number of RNA GT, median (range) | 6 (2–19) |
| number of DNA GT, median (range) | 1 (1–3) |
| historical INI GT, % | 55 |
| resistance ≥ 2 ARV classes, % | 100 |
| resistance ≥ 3 ARV classes, % | 88, 57 |
| years between last RNA GT and current DNA GT, median (range) | 7 (0–17) |
| Patient | NRTI-Associated Resistance Mutation (RNA) | NNRTI-Associated Resistance Mutation (RNA) | PI-Associated Resistance Mutation (RNA) | INI-Associated Resistance Mutation (RNA) | Old ART Regimen | NRTI-Associated Resistance Mutation (DNA) | NNRTI-Associated Resistance Mutation (DNA) | PI-Associated Resistance Mutation (DNA) | INI-Associated Resistance Mutation (DNA) | New ART Regimen |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | L74V, M184V, T215Y, M41L, L210W, K219E/N, D67N, | G190S, K101E, Y181C, | V82T, I54V, L24I, M46I, G73S, Q58E | na | FPV + rtv + AZT + TDF + MVC | L74V, M184V, T215Y, M41L, L210W, K219N | Y181C, G190S, K101H/Q | V82S/T, I54V, L24I, M46I, G73S, L33F | - | TAF/FTC/EVG/cob + DRV Due to adverse drug effects switched to: DRV + rtv + DTG + MVC |
| 2 | M184V, T215F, M41L | K103N | I54V, V82A | na | TAF/FTC + DRV + rtv + MVC | - | - | - | - | TAF/FTC/DRV/cob |
| 3 | M184V, T215Y, M41L, L210W | H221Y, K103N | V82L | na | LPV/rtv + RAL | M184V, T215N/S/Y, L74V, M184I/V, T215N/S/Y, M41I/L, L210W M41L | K103N | V82L | - | BIC/TAF/FTC + MVC |
| 4 | M184V, L74I | V106I, Y181C, E138A/P/Q | T74P, K20T, L33F, I84V, V82I/M, | - | TDF + ETR + RAL + DRV + rtv | M184V, K219N | Y181C E138K | - | - | DRV+ rtv + DTG |
| 5 | L74V/I, M184I/V, T215C/Y, M41L, D67G, K70R, K219E, V75A | Y188F/H, L100V, V106I, K103N, A98G, V108I, H221Y, Y318F | V82T, L90M, I54V, G73S, G48A/M/T/V, F53L | - | RAL + MVC + rtv + DRV + 3TC/ABC | L74I, M184V, T215Y, M41L, D67G/N/S, K70R, K219E | Y188F/H/L, A98G, V108I, H221Y, L100V, V106I | V82T, L90M, I54V, G73S | - | DRV + rtv + RAL |
| 6 | L74V, K70R/N, T215N/S/Y, M41L, L210W, K219R, T69D | L100I, K103N, K238T | I84V, L90M, M46I, G73S/T | na | DRV + rtv + RAL + ETR | L74V, M184V, T215Y, M41L, L210W, K219R, T69D | L100I, K103N | I84V, L90M, I54V, M46I, G73T, L10F | - | TAF/FTC/DRV/cob + DTG |
| 7 | T215F, K219E, M184V, D67N, K70R, M41L, | K103N, Y181C, V108I | L90M, V32I, I54V, V82A, M46I, I47V, F53L, L33F | na | DRV + rtv DDI + RAL | M184V, T215F, M41L, D67N, K70R, K219E | K103N, Y181C | L90M, V32I, I54L/V, V82A, M46I, I47V, F53L, L33F | - | MVC + DTG/3TC |
| 8 | L74V, M184V, T215F/I/S, D67N, K70G/R/S, M41L, K219H/Q, V75M, F77L | K103N, Y181C, V108I, H221Y, K101H | I84V, L24I, M46I, V32I, I54L, T74P, L89M/V, K20T, L33F, K43T | - | RAL + DOR + DRV + rtv | M184V, T215F/I/S, M41I/L, D67N, K70R, V75I/M, F77L, K219Q | K103N, K101H/N/Q | I84V, L24I, M46I | - | RAL + DRV+ rtv |
| 9 | M184V | K103N | - | na | 3TC/ABC + DRV + rtv + MVC | - | E138A | - | - | TAF/FTC/DRV/cob |
| 10 | M184V, D67N, K70R, K219E | Y181C | I54V, V82A, L24I, M46L, F53L, L33F | - | DRV + rtv + RAL + ETR | K65R, M184V, D67N | Y181C | I54V, V82A, L24I, M46L, F53L, L33F, G73S | - | TAF/FTC/DRV/cob + DTG + ETR |
| 11 | L74V, T215Y, M41L, M184V | K103N, G190A, Y181C, H221Y, K101H | I54V/M, V82A, M46I, I84V, Q58E, L33F | na | DRV + rtv + TDF/FTC + MVC | - | - | - | - | BIC/TAF/FTC |
| 12 | L74V, M184V, T215Y, M41L, D67N, L210W, V75M, E44D | K103N, G190A, Y181C | I84V, L90M, M46I, L24F, L33F, G73S, I54L, L10F | - | DRV + rtv + RAL + MVC | M184V, T215N/S/Y, M41L, D67N, K70R, L210W | - | - | - | DRV + rtv + DTG |
| 13 | M184I/V | K103N, P225H | - | N155H | DRV + rtv + ETR + DTG | M184I | - | - | - | BIC/TAF/FTC |
| 14 | K65R, M184V | G190S, Y181C, K101E, A98G, E138A | L89M/V | - | DTG + DRV + rtv | M184V | G190S, K101E | - | - | TAF/FTC/DRV/cob + DTG |
| 15 | L74V, M41L, D67N, L210W, T215D, L74V, M41L, D67N, L210W, T215D, V75M | K103N, G190A, Y181C | I84V, L90M, I54L, M46I, L33F, L10F | - | 3TC + RAL + DRV + rtv + ETR + MVC | L74V, M41L, D67N, L210W, T215D, V75M | K103N, G190A, Y181C | I84V, L90M, I54L, M46I, G73S, L33F, L10F | - | TAF/FTC/DRV/cob + DTG |
| 16 | D67N, T215E, K219Q | Y188L | I54L | - | DRV + rtv + RAL + 3TC | D67N, T215E, K219Q | Y188L | I54L | - | BIC/TAF/FTC |
| 17 | K70E/G/R | K101E | M46L | na | RAL + DRV + rtv | K70G | M46L | - | - | BIC/TAF/FTC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rauschning, D.; Ehren, I.; Heger, E.; Knops, E.; Fätkenheuer, G.; Suárez, I.; Lehmann, C. Optimizing Antiretroviral Therapy in Heavily ART-Experienced Patients with Multi-Class Resistant HIV-1 Using Proviral DNA Genotypic Resistance Testing. Viruses 2023, 15, 1444. https://doi.org/10.3390/v15071444
Rauschning D, Ehren I, Heger E, Knops E, Fätkenheuer G, Suárez I, Lehmann C. Optimizing Antiretroviral Therapy in Heavily ART-Experienced Patients with Multi-Class Resistant HIV-1 Using Proviral DNA Genotypic Resistance Testing. Viruses. 2023; 15(7):1444. https://doi.org/10.3390/v15071444
Chicago/Turabian StyleRauschning, Dominic, Ira Ehren, Eva Heger, Elena Knops, Gerd Fätkenheuer, Isabelle Suárez, and Clara Lehmann. 2023. "Optimizing Antiretroviral Therapy in Heavily ART-Experienced Patients with Multi-Class Resistant HIV-1 Using Proviral DNA Genotypic Resistance Testing" Viruses 15, no. 7: 1444. https://doi.org/10.3390/v15071444
APA StyleRauschning, D., Ehren, I., Heger, E., Knops, E., Fätkenheuer, G., Suárez, I., & Lehmann, C. (2023). Optimizing Antiretroviral Therapy in Heavily ART-Experienced Patients with Multi-Class Resistant HIV-1 Using Proviral DNA Genotypic Resistance Testing. Viruses, 15(7), 1444. https://doi.org/10.3390/v15071444