


Spatio-Temporal Cluster Detection of Dengue, Chikungunya, and Zika Viruses’ Infection in Rio de Janeiro State from 2010 to 2019
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
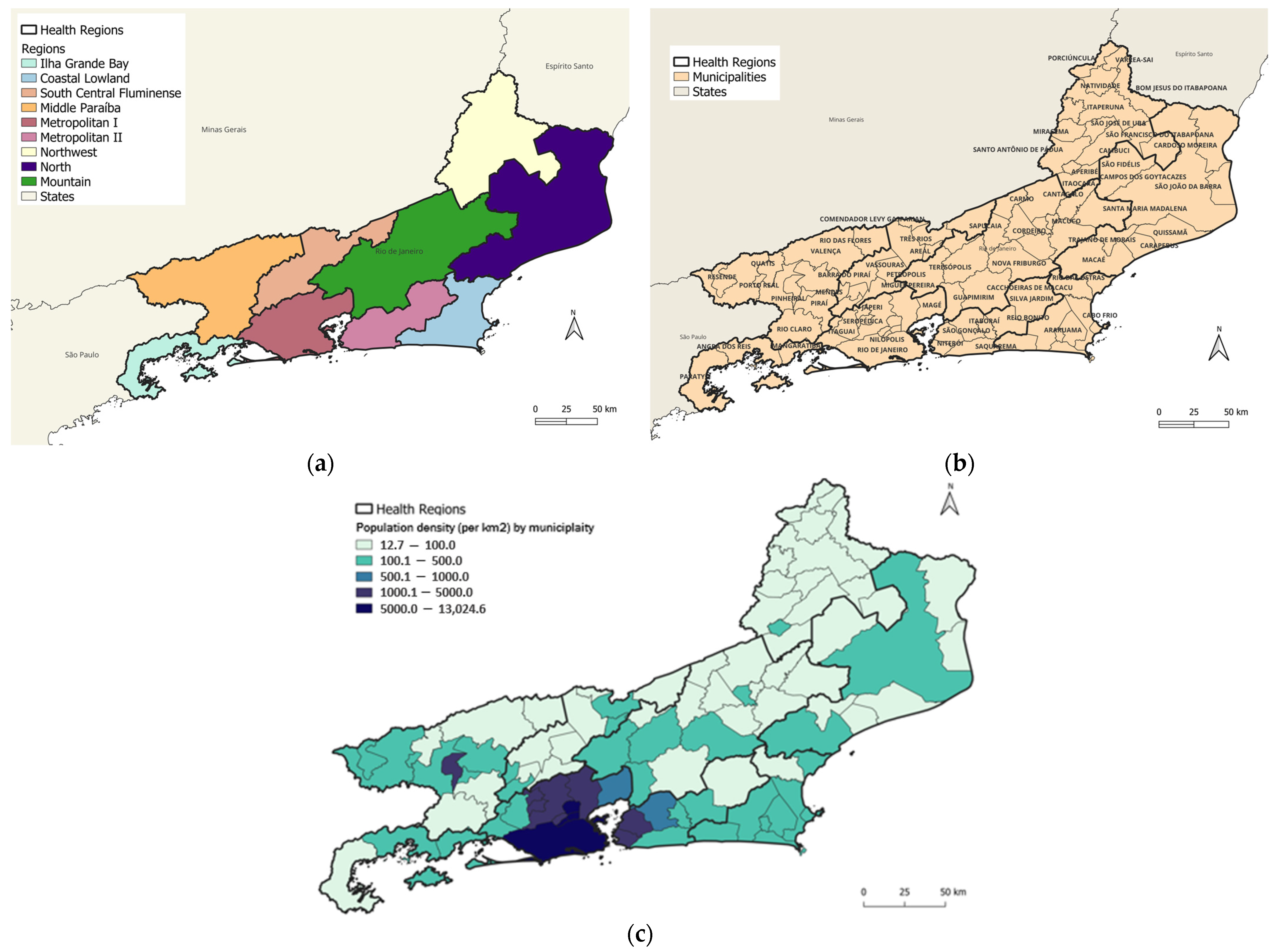
2.1. Study Site
2.2. Study Design and Data Source
2.3. Spatio-Temporal Analyses
3. Results
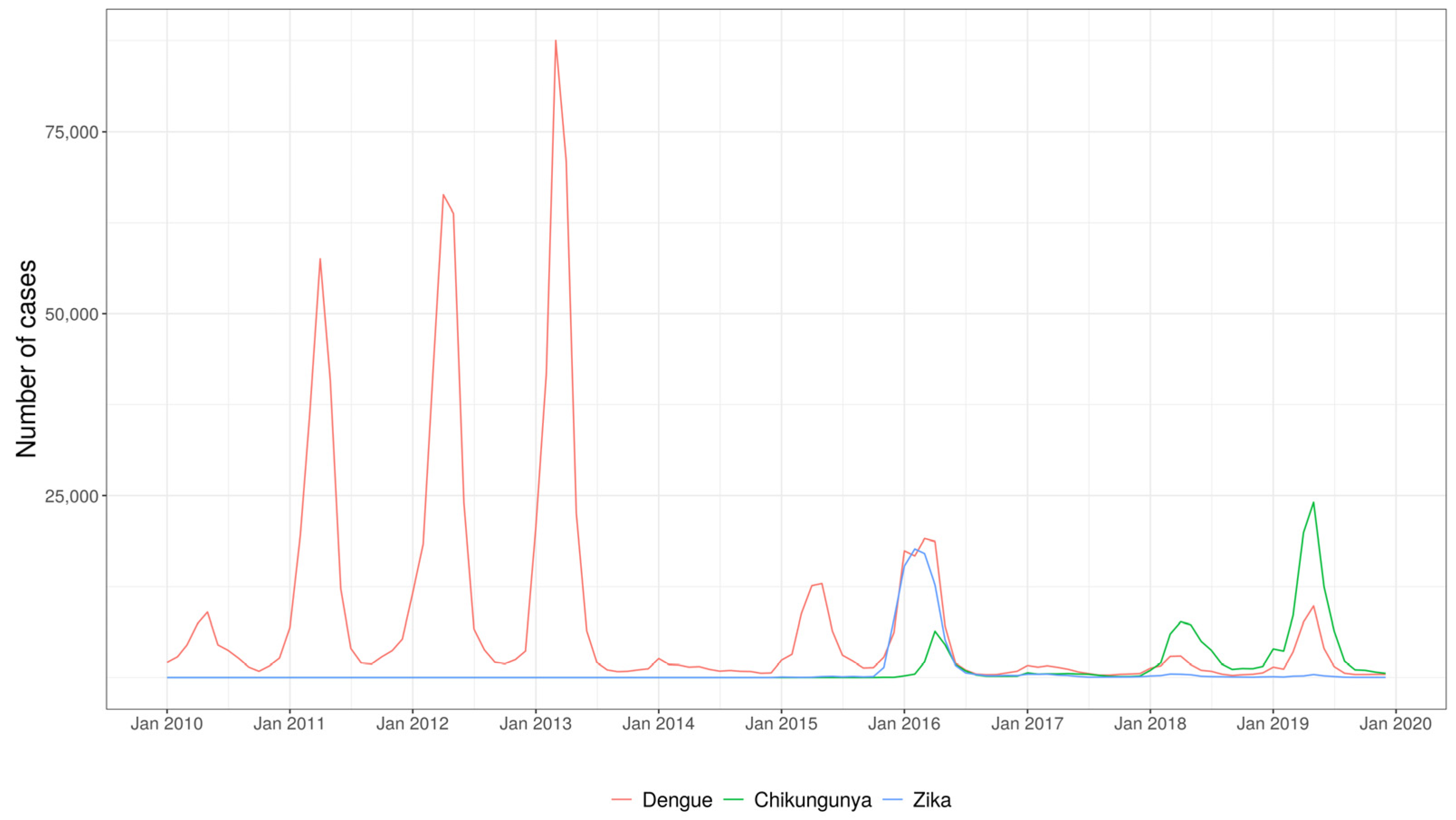
3.1. Exploratory Analysis
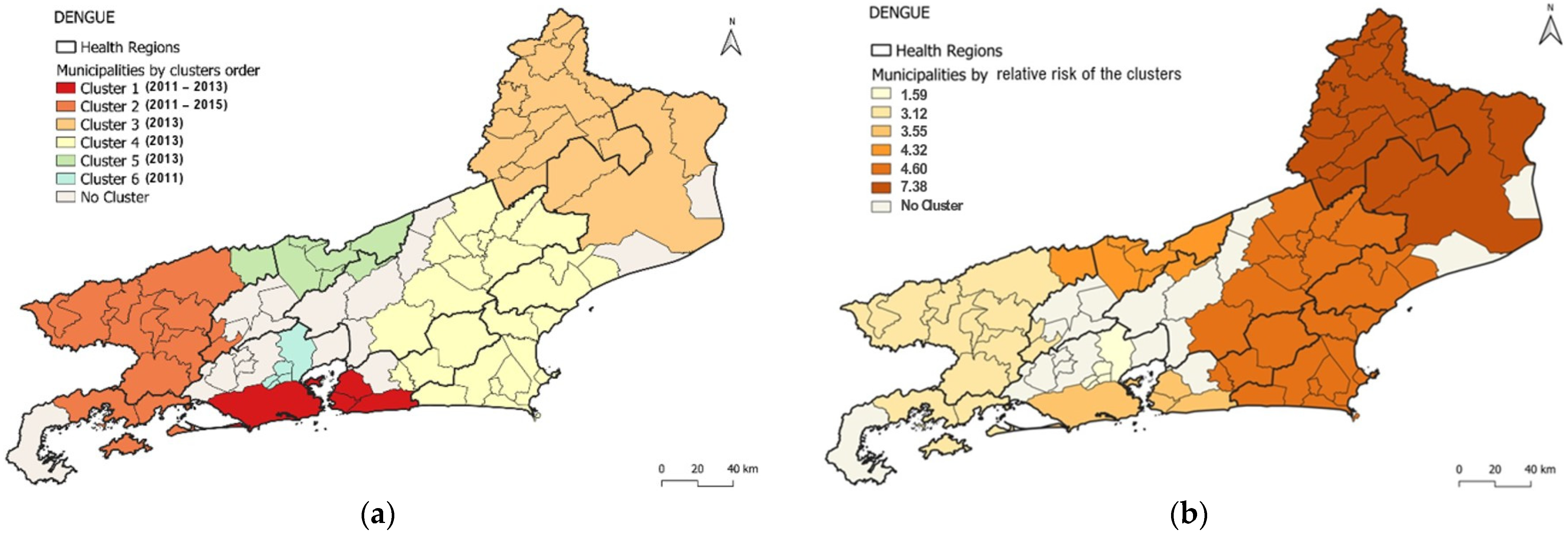
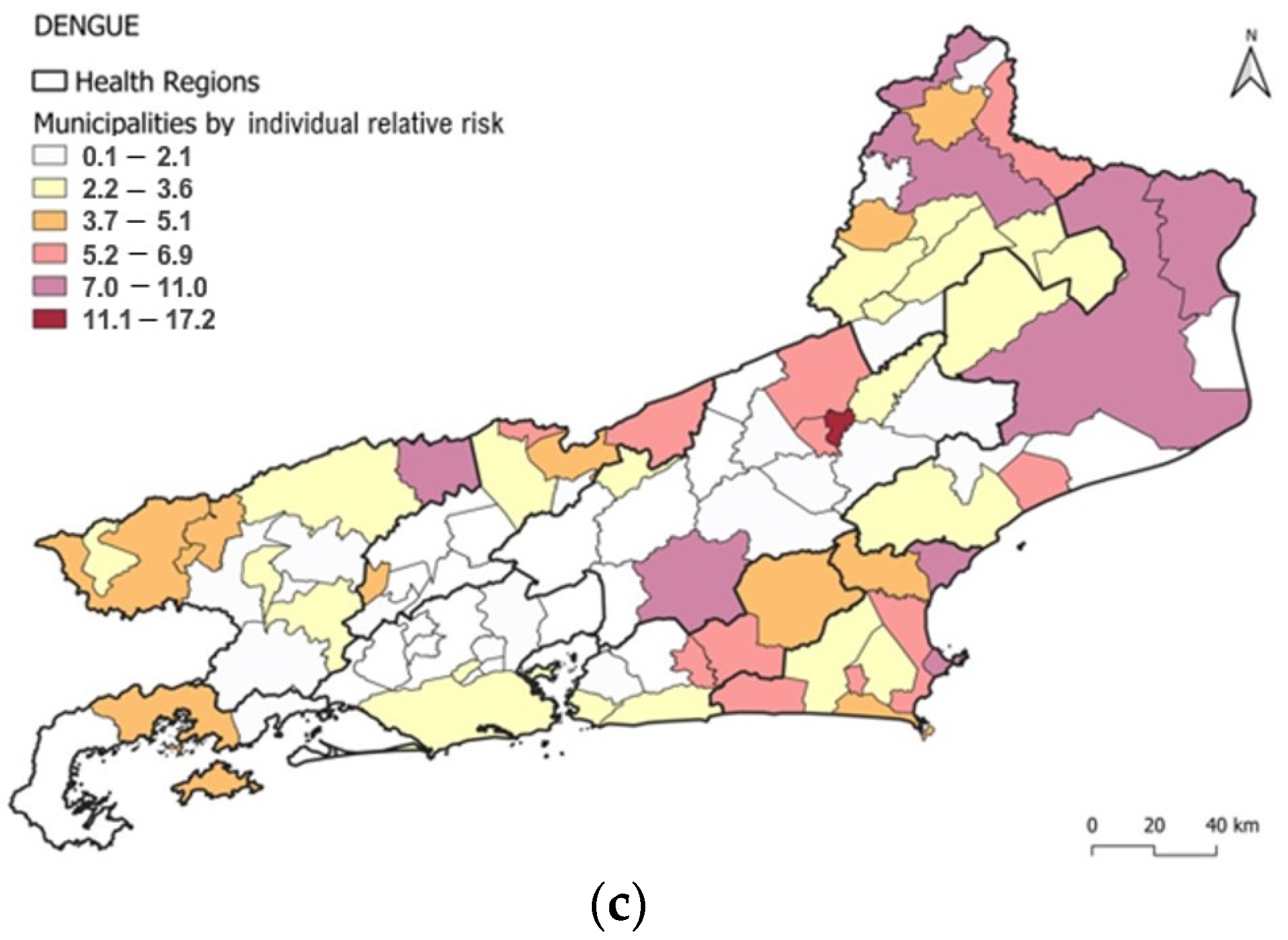
3.2. Spatio-Temporal Cluster Analysis of Dengue
3.3. Spatio-Temporal Cluster Analysis of Chikungunya
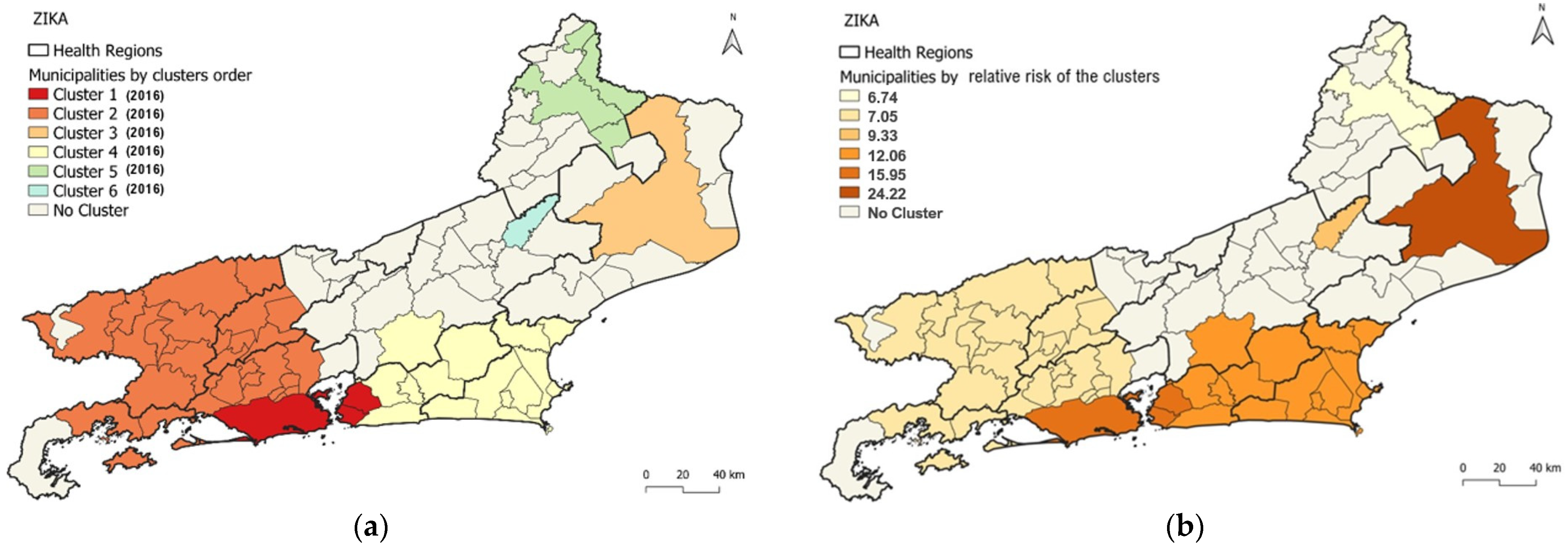
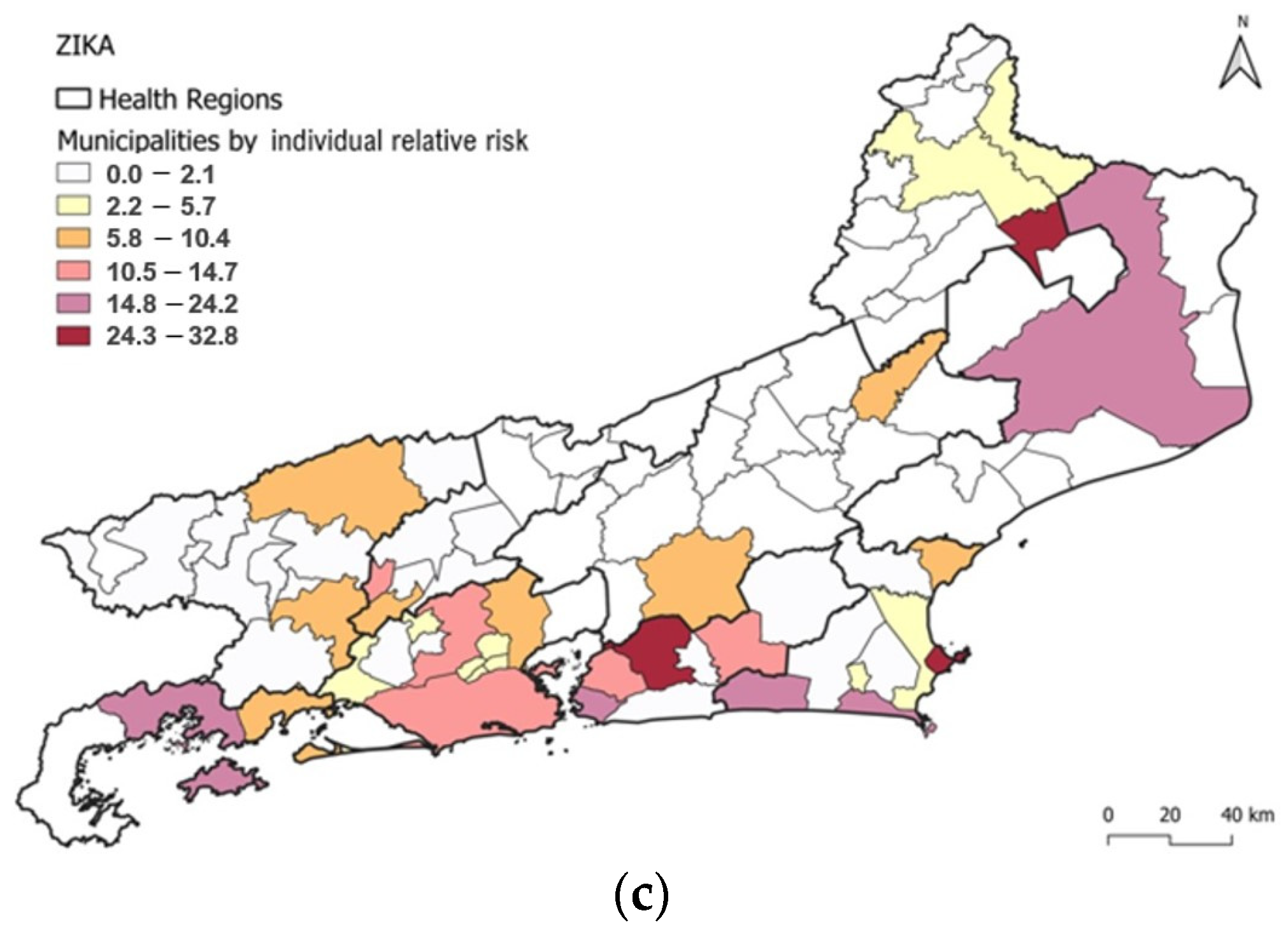
3.4. Spatio-Temporal Cluster Analysis of Zika
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schatzmayr, H.G.; Nogueira, R.M.R.; da Rosa, A.P.A.T. An outbreak of dengue virus at Rio de Janeiro-1986. Mem. Inst. Oswaldo Cruz 1986, 81, 245–246. [Google Scholar] [CrossRef] [Green Version]
- Marzochi, K.B.F. Dengue in Brazil—Situation, transmission and control: A proposal for ecological control. Mem. Inst. Oswaldo Cruz 1994, 89, 235–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nogueira, R.M.R.; De Araújo, J.M.G.; Schatzmayr, H.G. Dengue viruses in Brazil, 1986–2006. Rev. Panam. Salud Publica 2007, 22, 358–363. [Google Scholar] [CrossRef] [Green Version]
- Nogueira, M.R.; Eppinghaus, L.F. Dengue virus type 4 arrives in the state of Rio de Janeiro: A challenge for epidemiological surveillance and control. Mem. Inst. Oswaldo Cruz 2011, 106, 255–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, P.C.G.; Daumas, R.P.; Sánchez-Arcila, J.C.; Nogueira, R.M.R.; Horta, M.A.P.; Dos Santos, F.B. 30 years of fatal dengue cases in Brazil: A review. BMC Public Health 2019, 19, 329. [Google Scholar] [CrossRef]
- de Almeida, P.M.P.; Nobre, A.A.; Câmara, D.C.P.; Costa, L.M.M.; dos Reis, I.C.; Ribeiro, M.S.; Dias, C.M.G.; Ayllón, T.; Honório, N.A. Dengue, Chikungunya, and Zika: Spatial and Temporal Distribution in Rio de Janeiro State, 2015–2019. Trop. Med. Infect. Dis. 2022, 7, 141. [Google Scholar] [CrossRef]
- Dantés, H.G.; Manrique-Saide, P.; Vazquez-Prokopec, G.; Morales, F.C.; Junior, J.B.S.; Pimenta, F.; Coelho, G.; Bezerra, H. Prevention and control of Aedes transmitted infections in the post-pandemic scenario of COVID-19: Challenges and opportunities for the region of the Americas. Mem. Inst. Oswaldo Cruz 2020, 115, e200284. [Google Scholar] [CrossRef] [PubMed]
- Gubler, D.J. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21st Century. Trop. Med. Health 2011, 39 (Suppl. S4), S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Honório, N.A.; Câmara, D.; Calvet, G.A.; Brasil, P. Chikungunya: Uma arbovirose em estabelecimento e expansão no Brasil. Cad. Saúde Pública 2015, 31, 906–908. [Google Scholar] [CrossRef] [Green Version]
- Martelli, C.M.T.; Siqueira, J.B.; Parente, M.P.P.D.; de Zara, A.L.S.A.; Oliveira, C.S.; Braga, C.; Pimenta, F.G.; Cortes, F.; Lopez, J.G.; Bahia, L.R.; et al. Economic Impact of Dengue: Multicenter Study across Four Brazilian Regions. PLoS Negl. Trop. Dis. 2015, 9, e0004042. [Google Scholar] [CrossRef] [Green Version]
- Fuller, T.L.; Calvet, G.; Estevam, G.C.; Angelo, J.R.; Abiodun, G.J.; Halai, U.-A.; Santis, B.; Sequeira, P.C.; Araújo, E.M.; Sampaio, S.A.; et al. Behavioral, climatic, and environmental risk factors for Zika and Chikungunya virus infections in Rio de Janeiro, Brazil, 2015–16. PLoS ONE 2017, 12, e0188002. [Google Scholar] [CrossRef] [Green Version]
- Donalisio, M.R.; Freitas, A.R.R.; Von Zuben, A.P.B. Arboviruses emerging in Brazil: Challenges for clinic and implications for public health. Rev. Saude Publica 2017, 51, 30. [Google Scholar] [CrossRef]
- Freitas, L.P.; Cruz, O.G.; Lowe, R.; Carvalho, M.S. Space–time dynamics of a triple epidemic: Dengue, chikungunya and Zika clusters in the city of Rio de Janeiro. Proc. R. Soc. B Boil. Sci. 2019, 286, 20191867. [Google Scholar] [CrossRef] [Green Version]
- Lowe, R.; Barcellos, C.; Brasil, P.; Cruz, O.G.; Honório, N.A.; Kuper, H.; Carvalho, M.S. The Zika Virus Epidemic in Brazil: From Discovery to Future Implications. Int. J. Environ. Res. Public Health 2018, 15, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, J.P.C.; Honório, N.A.; Nobre, A.A. Definition of persistent areas with increased dengue risk by detecting clusters in populations with differing mobility and immunity in Rio de Janeiro, Brazil. Cad. Saúde Pública 2019, 35, e00248118. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.D.; Mahabir, R.S.; Curtin, K.M.; Sutherland, J.M.; Agard, J.B.; Chadee, D.D. Exploratory space-time analysis of dengue incidence in Trinidad: A retrospective study using travel hubs as dispersal points, 1998–2004. Parasites Vectors 2014, 7, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desjardins, M.; Whiteman, A.; Casas, I.; Delmelle, E. Space-time clusters and co-occurrence of chikungunya and dengue fever in Colombia from 2015 to 2016. Acta Trop. 2018, 185, 77–85. [Google Scholar] [CrossRef]
- Xu, Z.; Bambrick, H.; Yakob, L.; Devine, G.; Lu, J.; Frentiu, F.D.; Yang, W.; Williams, G.; Hu, W. Spatiotemporal patterns and climatic drivers of severe dengue in Thailand. Sci. Total Environ. 2018, 656, 889–901. [Google Scholar] [CrossRef] [Green Version]
- Freitas, L.P.; Carabali, M.; Yuan, M.; Jaramillo-Ramirez, G.I.; Balaguera, C.G.; Restrepo, B.N.; Zinszer, K. Spatio-temporal clusters and patterns of spread of dengue, chikungunya, and Zika in Colombia. PLoS Neglected Trop. Dis. 2022, 16, e0010334. [Google Scholar] [CrossRef]
- Organização Pan-Americana da Saúde (OPAS). Documento Técnico para a Implementação de Intervenções Baseado em Cenários Operacionais Genéricos Para o Controle do Aedes aegypti; OPAS: Washington, DC, USA, 2019; Available online: https://iris.paho.org/bitstream/handle/10665.2/51653/9789275721100_por.pdf?sequence=1&isAllowed=y (accessed on 23 June 2023).
- dos Santos, J.P.C.; Albuquerque, H.G.; Siqueira, A.S.P.; Praça, H.L.F.; Pereira, L.V.; Tavares, A.D.M.; Gusmão, E.V.V.; Bruno, P.R.D.A.; Barcellos, C.; Carvalho, M.D.S.; et al. ARBOALVO: Estratificação territorial para definição de áreas de pronta resposta para vigilância e controle de arboviroses urbanas em tempo oportuno [ARBOALVO: Territorial stratification for definition of areas for prompt response by surveillance and timely control of urban arbovirus infections]. Cad. Saude Publica 2022, 38, e00110121. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Available online: https://www.ibge.gov.br (accessed on 19 April 2022).
- Estado do Rio de Janeiro. Secretaria de Estado de Saúde do Rio de Janeiro (SES/RJ). Atualização do Plano Diretor de Regionalização, SES/RJ, anos 2012/2013. Available online: https://www.saude.rj.gov.br/comum/code/MostrarArquivo.php?C=MzA0OQ%2C%2C (accessed on 19 December 2022).
- Estado do Rio de Janeiro. Secretaria de Estado de Saúde do Rio de Janeiro (SES/RJ). Plano Estadual de Saúde do Rio de Janeiro 2020–2023. Available online: https://www.saude.rj.gov.br/comum/code/MostrarArquivo.php?C=Mjk2Nzk%2C (accessed on 3 May 2023).
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Kulldorff, M. 2018 SaTScan™ User Guide for Version 9.6. Available online: https://www.satscan.org/cgi-bin/satscan/register.pl/SaTScan_Users_Guide.pdf?todo=process_userguide_download (accessed on 22 August 2022).
- Escosteguy, C.C.; Pereira, A.G.L.; Marques, M.R.V.E.; Lima, T.R.D.A.; Galliez, R.M.; Medronho, R.D.A. Yellow fever: Profile of cases and factors associated with death in a hospital in the State of Rio de Janeiro, 2017–2018. Rev. Saude Publica 2019, 53, 89. [Google Scholar] [CrossRef] [Green Version]
- Salles, T.S.; Sá-Guimarães, T.D.E.; De Alvarenga, E.S.L.; Guimarães-Ribeiro, V.; De Meneses, M.D.F.; De Castro-Salles, P.F.; Dos Santos, C.R.; Melo, A.C.D.A.; Soares, M.R.; Ferreira, D.F.; et al. History, epidemiology and diagnostics of dengue in the American and Brazilian contexts: A review. Parasites Vectors 2018, 11, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estado do Rio de Janeiro 2022. Secretaria de Estado de Saúde do Rio de Janeiro (SES/RJ). Plano de Contigência Para Enfrentamento às Arboviroses Urbanas Causadas pelo Aedes aegypti—2022 a 2024. Secretaria de Estado do Saúde do Rio de janeiro. Available online: https://drive.google.com/file/d/17H3cz1awHcTOfhsKbSI3LllKU6gfnidR/view (accessed on 5 May 2023).
- Ximenes, R.; Amaku, M.; Lopez, L.F.; Coutinho, F.A.B.; Burattini, M.N.; Greenhalgh, D.; Wilder-Smith, A.; Struchiner, C.J.; Massad, E. The risk of dengue for non-immune foreign visitors to the 2016 summer olympic games in Rio de Janeiro, Brazil. BMC Infect. Dis. 2016, 16, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Almeida, I.F.; Lana, R.M.; Codeço, C.T. How heterogeneous is the dengue transmission profile in Brazil? A study in six Brazilian states. PLoS Negl. Trop. Dis. 2022, 16, e0010746. [Google Scholar] [CrossRef] [PubMed]
- Coleman, M.; Coleman, M.; Mabuza, A.M.; Kok, G.; Coetzee, M.; Durrheim, D.N. Using the SaTScan method to detect local malaria clusters for guiding malaria control programmes. Malar. J. 2009, 8, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brasil. Ministério da Saúde, Nota Técnica nº1/2023-CGARB/DEIDT/SVS/MS, Ministério da Saúde, 2023. Available online: https://drive.google.com/file/d/1e81yJUi7LGOwBxUJr2Wc6t_AE6B4yCxS/view (accessed on 19 December 2022).
- Estado do Rio de Janeiro 2023. Secretaria de Estado de Saúde do Rio de Janeiro (SES/RJ). Painel de Arboviroses–DENGUE. Available online: https://www.saude.rj.gov.br/ (accessed on 22 January 2023).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cluster | No. of Locations | Period | No. of Cases | Population | Annual Incidence Rate a | Relative Risk | LLR | P |
|---|---|---|---|---|---|---|---|---|
| 1 | 4 | 2011–2013 | 395,331 | 8,165,684 | 1639.5 | 3.55 | 169,431.528 | <0.001 |
| 2 | 15 | 2011–2015 | 105,720 | 1,165,671 | 1841.1 | 3.12 | 45,829.719 | <0.001 |
| 3 | 17 | 2013 | 40,285 | 900,056 | 4525.3 | 7.38 | 45,121.201 | <0.001 |
| 4 | 25 | 2013 | 41,183 | 1,495,223 | 2824.7 | 4.6 | 30,093.344 | <0.001 |
| 5 | 7 | 2013 | 5,114 | 189,491 | 2725.7 | 4.32 | 3541.912 | <0.001 |
| 6 | 5 | 2011 | 21,211 | 2,162,210 | 1001.5 | 1.59 | 1945.04 | <0.001 |
| Cluster | No. of Locations | Period | No. of Cases | Population | Annual Incidence Rate a | Relative Risk | LLR | P |
|---|---|---|---|---|---|---|---|---|
| 1 | 16 | 2018–2019 | 30,728 | 906,082 | 1637.6 | 19.71 | 59,534.31 | <0.001 |
| 2 | 4 | 2018–2019 | 64,933 | 8,165,684 | 384.7 | 5.62 | 47,743.47 | <0.001 |
| 3 | 28 | 2019 | 20,022 | 4,668,653 | 414.7 | 4.54 | 13,908.13 | <0.001 |
| 4 | 11 | 2019 | 7336 | 1,013,163 | 657.9 | 6.79 | 7672.22 | <0.001 |
| 5 | 2 | 2019 | 1348 | 226,745 | 547.3 | 5.47 | 1185.31 | <0.001 |
| Cluster | No. of Locations | Period | No. of Cases | Population | Annual Incidence Rate a | Relative Risk | LLR | P |
|---|---|---|---|---|---|---|---|---|
| 1 | 3 | 2016 | 44,718 | 8,021,163 | 555 | 15.95 | 69,429.54 | <0.001 |
| 2 | 29 | 2016 | 16,940 | 4,656,627 | 361.8 | 7.05 | 17,363.67 | <0.001 |
| 3 | 1 | 2016 | 6652 | 483,435 | 1362.6 | 24.22 | 14,608.92 | <0.001 |
| 4 | 15 | 2016 | 8895 | 1,300,690 | 665.6 | 12.06 | 13,635.88 | <0.001 |
| 5 | 4 | 2016 | 649 | 159,871 | 403.1 | 6.74 | 684.2 | <0.001 |
| 6 | 1 | 2016 | 51 | 9076 | 560.8 | 9.33 | 68.36 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, P.M.P.d.; Câmara, D.C.P.; Nobre, A.A.; Ayllón, T.; Ribeiro, M.S.; Dias, C.M.G.; Peixoto, E.M.; Rocha, M.M.d.; Carvalho, S.; Honório, N.A. Spatio-Temporal Cluster Detection of Dengue, Chikungunya, and Zika Viruses’ Infection in Rio de Janeiro State from 2010 to 2019. Viruses 2023, 15, 1496. https://doi.org/10.3390/v15071496
Almeida PMPd, Câmara DCP, Nobre AA, Ayllón T, Ribeiro MS, Dias CMG, Peixoto EM, Rocha MMd, Carvalho S, Honório NA. Spatio-Temporal Cluster Detection of Dengue, Chikungunya, and Zika Viruses’ Infection in Rio de Janeiro State from 2010 to 2019. Viruses. 2023; 15(7):1496. https://doi.org/10.3390/v15071496
Chicago/Turabian StyleAlmeida, Paula Maria Pereira de, Daniel Cardoso Portela Câmara, Aline Araújo Nobre, Tania Ayllón, Mário Sérgio Ribeiro, Cristina Maria Giordano Dias, Eduardo Mesquita Peixoto, Maíra Mendonça da Rocha, Silvia Carvalho, and Nildimar Alves Honório. 2023. "Spatio-Temporal Cluster Detection of Dengue, Chikungunya, and Zika Viruses’ Infection in Rio de Janeiro State from 2010 to 2019" Viruses 15, no. 7: 1496. https://doi.org/10.3390/v15071496
APA StyleAlmeida, P. M. P. d., Câmara, D. C. P., Nobre, A. A., Ayllón, T., Ribeiro, M. S., Dias, C. M. G., Peixoto, E. M., Rocha, M. M. d., Carvalho, S., & Honório, N. A. (2023). Spatio-Temporal Cluster Detection of Dengue, Chikungunya, and Zika Viruses’ Infection in Rio de Janeiro State from 2010 to 2019. Viruses, 15(7), 1496. https://doi.org/10.3390/v15071496