
Kinetics and Value of Hepatitis B Core-Related Antigen in Patients with Chronic Hepatitis B Virus Infection during Antiviral Treatment

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Laboratory Assays
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Kinetics of HBV DNA, HBsAg and HBcrAg after Initiation of NA Treatment
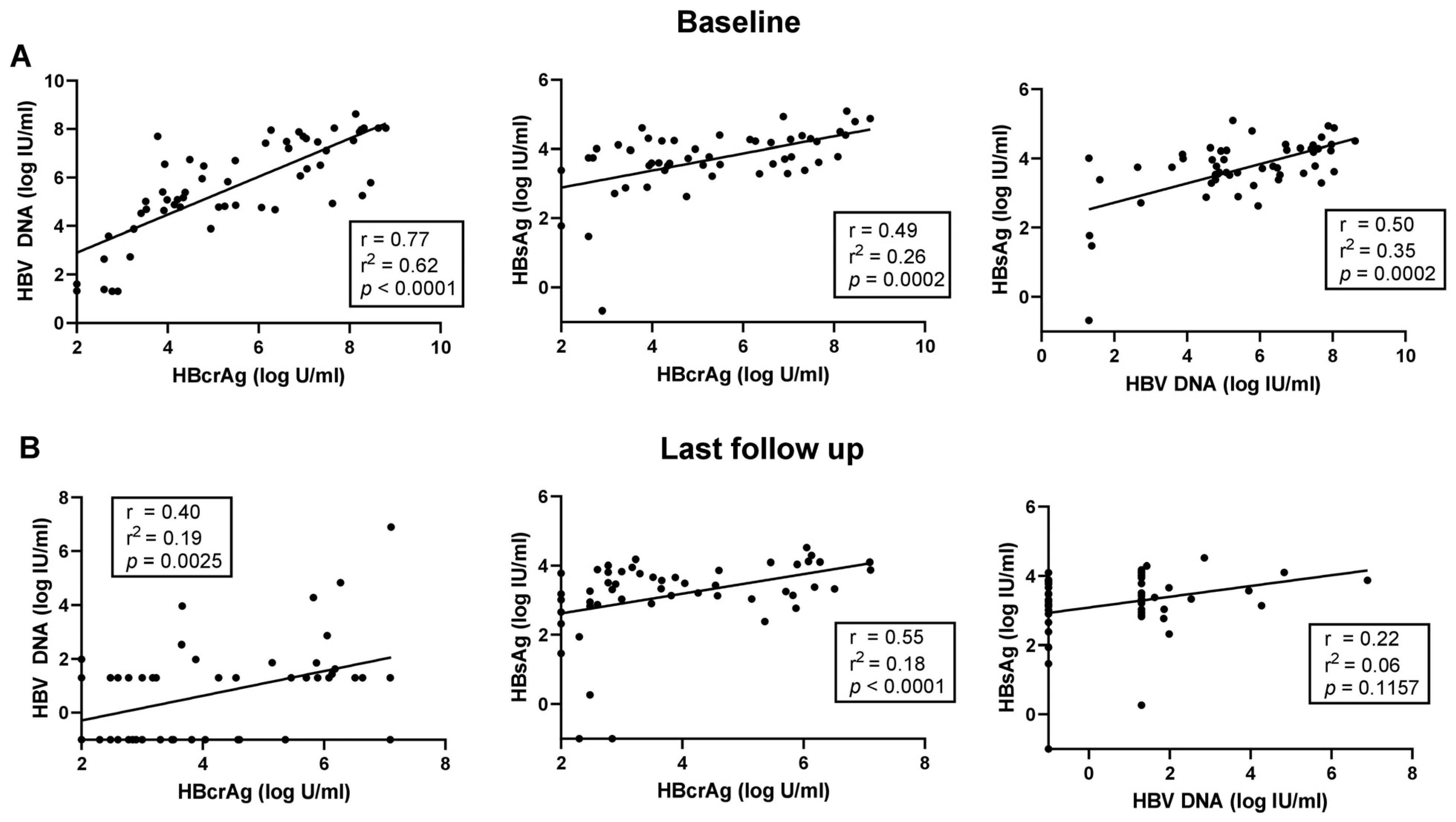
3.2. Correlation of HBV DNA, HBcrAg and HBsAg during NA Treatment
3.3. Predictive Value of Baseline HBcrAg Levels for HBeAg Seroconversion during NA Treatment
3.4. Predictive Value of Baseline HBcrAg Levels for HBsAg Loss or Decline during NA Treatment
3.5. Correlation of HBV DNA and HBcrAg after NA Cessation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Association for the Study of the Liver (EASL) 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [CrossRef]
- Terrault, N.A.; Bzowej, N.H.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H. AASLD guidelines for treatment of chronic hepatitis B. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef]
- Chevaliez, S.; Hézode, C.; Bahrami, S.; Grare, M.; Pawlotsky, J.-M.M. Long-term hepatitis B surface antigen (HBsAg) kinetics during nucleoside/nucleotide analogue therapy: Finite treatment duration unlikely. J. Hepatol. 2013, 58, 676–683. [Google Scholar] [CrossRef]
- van Bommel, F.; Stein, K.; Heyne, R.; Petersen, J.; Buggisch, P.; Berg, C.; Zeuzem, S.; Stallmach, A.; Sprinzl, M.; Schott, E.; et al. A multicenter randomized-controlled trial of nucleos(t)ide analogue cessation in HBeAg-negative chronic hepatitis B. J. Hepatol. 2023, 78, 926–936. [Google Scholar] [CrossRef]
- Agarwal, K.; Lok, J.; Carey, I.; Shivkar, Y.; Biermer, M.; Berg, T.; Lonjon-Domanec, I. A case of HBV-induced liver failure in the REEF-2 phase II trial: Implications for finite treatment strategies in HBV ‘cure’. J. Hepatol. 2022, 77, 245–248. [Google Scholar] [CrossRef]
- Suzuki, F.; Miyakoshi, H.; Kobayashi, M.; Kumada, H. Correlation between serum hepatitis B virus core-related antigen and intrahepatic covalently closed circular DNA in chronic hepatitis B patients. J. Med. Virol. 2009, 81, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Maasoumy, B.; Wiegand, S.B.; Jaroszewicz, J.; Bremer, B.; Lehmann, P.; Deterding, K.; Taranta, A.; Manns, M.P.; Wedemeyer, H.; Glebe, D.; et al. Hepatitis B core-related antigen (HBcrAg) levels in the natural history of hepatitis B virus infection in a large European cohort predominantly infected with genotypes A and D. Clin. Microbiol. Infect. 2015, 21, 606.e1–606.e10. [Google Scholar] [CrossRef] [PubMed]
- Riveiro-Barciela, M.; Bes, M.; Rodríguez-Frías, F.; Tabernero, D.; Ruiz, A.; Casillas, R.; Vidal-González, J.; Homs, M.; Nieto, L.; Sauleda, S.; et al. Serum hepatitis B core-related antigen is more accurate than hepatitis B surface antigen to identify inactive carriers, regardless of hepatitis B virus genotype. Clin. Microbiol. Infect. 2017, 23, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Carey, I.; Gersch, J.; Wang, B.; Moigboi, C.; Kuhns, M.; Cloherty, G.; Dusheiko, G.; Agarwal, K. Pre-genomic HBV RNA and HBcrAg predict outcomes in HBeAg negative chronic hepatitis B patients suppressed on nucleos(t)ide analogue therapy. Hepatology 2020, 72, 42–57. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, M.J.; Park, J.Y.; Kaewdech, A.; Seto, W.-K.; Tanaka, Y.; Carey, I.; Papatheodoridi, M.; van Bömmel, F.; Berg, T.; Zoulim, F.; et al. Prediction of Sustained Response After Nucleo(s)tide Analogue Cessation Using HBsAg and HBcrAg Levels: A Multicenter Study (CREATE). Clin. Gastroenterol. Hepatol. 2022, 20, e784–e793. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Hepatitis B and C Testing; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Singal, A.K.; Salameh, H.; Kuo, Y.F.; Fontana, R.J. Meta-analysis: The impact of oral anti-viral agents on the incidence of hepatocellular carcinoma in chronic hepatitis B. Aliment. Pharmacol. Ther. 2013, 38, 98–106. [Google Scholar] [CrossRef]
- Lok, A.S.; McMahon, B.J.; Brown, R.S., Jr.; Wong, J.B.; Ahmed, A.T.; Farah, W.; Almasri, J.; Alahdab, F.; Benkhadra, K.; Mouchli, M.A.; et al. Antiviral therapy for chronic hepatitis B viral infection in adults: A systematic review and meta-analysis. Hepatology 2016, 63, 284–306. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Chan, H.L.; Hansen, B.E.; Janssen, H.L.; Lampertico, P. Risk of hepatocellular carcinoma in chronic hepatitis B: Assessment and modification with current antiviral therapy. J. Hepatol. 2015, 62, 956–967. [Google Scholar] [CrossRef] [PubMed]
- Marcellin, P.; Gane, E.; Buti, M.; Afdhal, N.; Sievert, W.; Jacobson, I.M.; Washington, M.K.; Germanidis, G.; Flaherty, J.F.; Aguilar Schall, R.; et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: A 5-year open-label follow-up study. Lancet 2013, 381, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.Q.; Feng, S.; Wang, M.L.; Liang, L.B.; Zhou, L.Y.; Du, L.Y.; Yan, L.B.; Tao, C.M.; Tang, H. Serum hepatitis B core-related antigen is a satisfactory surrogate marker of intrahepatic covalently closed circular DNA in chronic hepatitis B. Sci. Rep. 2017, 7, 173. [Google Scholar] [CrossRef] [PubMed]
- Testoni, B.; Lebossé, F.; Scholtes, C.; Berby, F.; Miaglia, C.; Subic, M.; Loglio, A.; Facchetti, F.; Lampertico, P.; Levrero, M.; et al. Serum hepatitis B core-related antigen (HBcrAg) correlates with covalently closed circular DNA transcriptional activity in chronic hepatitis B patients. J. Hepatol. 2019, 70, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Honda, M.; Shirasaki, T.; Terashima, T.; Kawaguchi, K.; Nakamura, M.; Oishi, N.; Wang, X.; Shimakami, T.; Okada, H.; Arai, K.; et al. Hepatitis B Virus (HBV) Core-Related Antigen During Nucleos(t)ide Analog Therapy Is Related to Intra-hepatic HBV Replication and Development of Hepatocellular Carcinoma. J. Infect. Dis. 2016, 213, 1096–1106. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Ndow, G.; Njie, R.; Njai, H.F.; Takahashi, K.; Akbar, S.M.F.; Cohen, D.; Nayagam, S.; Jeng, A.; Ceesay, A.; et al. Hepatitis B Core-related Antigen: An Alternative to Hepatitis B Virus DNA to Assess Treatment Eligibility in Africa. Clin. Infect. Dis. 2020, 70, 1442–1452. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.C.; Lin, M.T.; Wang, J.H.; Hung, C.H.; Chen, C.H.; Chiu, S.Y.; Hu, T.H. HBcrAg Predicts Hepatocellular Carcinoma Development in Chronic B Hepatitis Related Liver Cirrhosis Patients Undergoing Long-Term Effective Anti-Viral. Viruses 2022, 14, 2671. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Toyoda, H.; Kiriyama, S.; Tanikawa, M.; Hisanaga, Y.; Kanamori, A.; Kitabatake, S.; Yama, T.; Tanaka, J. HBcrAg predicts hepatocellular carcinoma development: An analysis using time-dependent receiver operating characteristics. J. Hepatol. 2016, 65, 48–56. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Toyoda, H.; Kobayashi, N.; Akita, T.; Tanaka, J. Hepatitis B virus core-related antigen levels predict progression to liver cirrhosis in hepatitis B carriers. J. Gastroenterol. Hepatol. 2018, 33, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Shimakawa, Y.; Ndow, G.; Kaneko, A.; Aoyagi, K.; Lemoine, M.; Tanaka, Y. Rapid Point-of-Care Test for Hepatitis B Core-Related Antigen to Diagnose High Viral Load in Resource-Limited Settings. Clin. Gastroenterol. Hepatol. 2023, 21, 1943–1946.e2. [Google Scholar] [CrossRef]
- Adraneda, C.; Tan, Y.C.; Yeo, E.J.; Kew, G.S.; Khakpoor, A.; Lim, S.G. A critique and systematic review of the clinical utility of hepatitis B core-related antigen. J. Hepatol. 2023, 78, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Watanabe, T.; Tanaka, Y. Hepatitis B core-related antigen: A novel and promising surrogate biomarker to guide anti-hepatitis B virus therapy. Clin. Mol. Hepatol. 2023, 29, 851–868. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Carey, I.; Bruce, M.; Montague, S.; Dusheiko, G.; Agarwal, K. HBsAg and HBcrAg as predictors of HBeAg seroconversion in HBeAg-positive patients treated with nucleos(t)ide analogues. J. Viral Hepat. 2018, 25, 886–893. [Google Scholar] [CrossRef]
- Tseng, T.C.; Liu, C.J.; Su, T.H.; Wang, C.C.; Chen, C.L.; Chen, P.J.; Chen, D.S.; Kao, J.H. Serum hepatitis B surface antigen levels predict surface antigen loss in hepatitis B e antigen seroconverters. Gastroenterology 2011, 141, 517–525.e2. [Google Scholar] [CrossRef]
- Ghany, M.G.; Buti, M.; Lampertico, P.; Lee, H.M. Guidance on Treatment Endpoints and Study Design for Clinical Trials Aiming to Achieve Cure in, Chronic Hepatitis B and D-Report from the 2022 AASLD-EASL HBV/HDV Treatment Endpoints Conference. J. Hepatol. 2023, 79, 1254–1269. [Google Scholar] [CrossRef]
- Ghany, M.G.; King, W.C.; Hinerman, A.S.; Lok, A.S.; Lisker-Melman, M.; Chung, R.T.; Terrault, N.; Janssen, H.L.A.; Khalili, M.; Lee, W.M.; et al. Use of HBV RNA and to predict change in serological status and disease activity in CHB. Hepatology 2023, 78, 1542–1557. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient number, n | 56 |
| Age (years; mean ± SD) | 43 (32–49) |
| Male/female, n (%) | 41 (73)/15 (27) |
| HBeAg status (pos/neg/n.a.), n (%) | 18 (32)/29 (52)/9 (16) |
| Creatinine (µmol/L) | 78 (67–88) |
| AST (U/L) | 57 (39–92) |
| ALT (U/L) | 89 (52–158) |
| GGT (U/L) | 43 (21–94) |
| Total bilirubin (µmol/L) | 12 (7–19) |
| Albumin (g/L) | 40 (38–42) |
| Leucocytes (×103/µL) | 5.2 (4.5–6.5) |
| Platelets (×103/µL) | 204 (159–240) |
| INR | 1.06 (1.02–1.13) |
| Antiviral treatment | |
| Tenofovir, n (%) | 12 (21) |
| Entecavir, n (%) | 24 (43) |
| Telbivudin, n (%) | 2 (4) |
| Adefovir, n (%) | 3 (5) |
| Lamivudine, n (%) | 10 (18) |
| Combination #, n (%) | 6 (11) |
| Follow up (months) | 60 (37–72) |
| HBV DNA (log IU/mL) | 5.60 (4.71–7.47) |
| HBsAg (log IU/mL) | 3.76 (3.42–4.26) |
| HBcrAg (log U/mL; median, IQR) | 5.29 (3.90–7.24) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandmann, L.; Bremer, B.; Ohlendorf, V.; Jaroszewicz, J.; Wedemeyer, H.; Cornberg, M.; Maasoumy, B. Kinetics and Value of Hepatitis B Core-Related Antigen in Patients with Chronic Hepatitis B Virus Infection during Antiviral Treatment. Viruses 2024, 16, 255. https://doi.org/10.3390/v16020255
Sandmann L, Bremer B, Ohlendorf V, Jaroszewicz J, Wedemeyer H, Cornberg M, Maasoumy B. Kinetics and Value of Hepatitis B Core-Related Antigen in Patients with Chronic Hepatitis B Virus Infection during Antiviral Treatment. Viruses. 2024; 16(2):255. https://doi.org/10.3390/v16020255
Chicago/Turabian StyleSandmann, Lisa, Birgit Bremer, Valerie Ohlendorf, Jerzy Jaroszewicz, Heiner Wedemeyer, Markus Cornberg, and Benjamin Maasoumy. 2024. "Kinetics and Value of Hepatitis B Core-Related Antigen in Patients with Chronic Hepatitis B Virus Infection during Antiviral Treatment" Viruses 16, no. 2: 255. https://doi.org/10.3390/v16020255
APA StyleSandmann, L., Bremer, B., Ohlendorf, V., Jaroszewicz, J., Wedemeyer, H., Cornberg, M., & Maasoumy, B. (2024). Kinetics and Value of Hepatitis B Core-Related Antigen in Patients with Chronic Hepatitis B Virus Infection during Antiviral Treatment. Viruses, 16(2), 255. https://doi.org/10.3390/v16020255