
Comparative Analysis of Cytomegalovirus Gastrointestinal Disease in Immunocompetent and Immunocompromised Patients
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Patient
2.3. Definition of Immune Status
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Clinical Manifestations
3.2. Prognostic Factors
3.3. Survival Curve Analysis and Efficacy of Antiviral Treatments
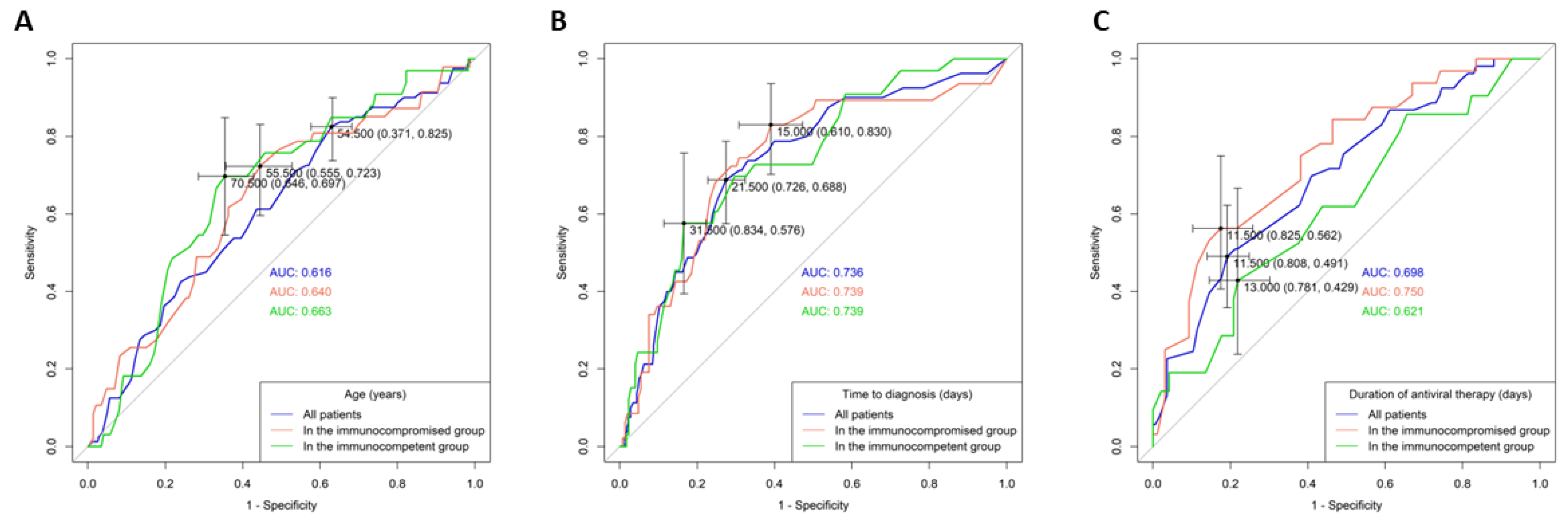
3.4. AUROC Analysis of Continuous Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Griffiths, P.; Reeves, M. Pathogenesis of human cytomegalovirus in the immunocompromised host. Nat. Rev. Microbiol. 2021, 19, 759–773. [Google Scholar] [CrossRef]
- Fowler, K.; Mucha, J.; Neumann, M.; Lewandowski, W.; Kaczanowska, M.; Grys, M.; Schmidt, E.; Natenshon, A.; Talarico, C.; Buck, P.O. A systematic literature review of the global seroprevalence of cytomegalovirus: Possible implications for treatment, screening, and vaccine development. BMC Public. Health 2022, 22, 1659. [Google Scholar] [CrossRef]
- Mourad, F.H.; Hashash, J.G.; Kariyawasam, V.C.; Leong, R.W. Ulcerative Colitis and Cytomegalovirus Infection: From A to Z. J. Crohn’s Colitis 2020, 14, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Kotton, C.N.; Kamar, N. New Insights on CMV Management in Solid Organ Transplant Patients: Prevention, Treatment, and Management of Resistant/Refractory Disease. Infect. Dis. Ther. 2023, 12, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Allaw, F.; Haddad, S.F.; Zakhour, J.; Kanj, S.S. Management of cytomegalovirus infection in allogeneic hematopoietic stem cell transplants. Int. J. Antimicrob. Agents 2023, 62, 106860. [Google Scholar] [CrossRef] [PubMed]
- You, D.M.; Johnson, M.D. Cytomegalovirus infection and the gastrointestinal tract. Curr. Gastroenterol. Rep. 2012, 14, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Yeh, P.J.; Wu, R.C.; Chiu, C.T.; Lai, M.W.; Chen, C.M.; Pan, Y.B.; Su, M.Y.; Kuo, C.J.; Lin, W.R.; Le, P.H. Cytomegalovirus Diseases of the Gastrointestinal Tract. Viruses 2022, 14, 352. [Google Scholar] [CrossRef] [PubMed]
- Wetwittayakhlang, P.; Rujeerapaiboon, N.; Wetwittayakhlung, P.; Sripongpun, P.; Pruphetkaew, N.; Jandee, S.; Chamroonkul, N.; Piratvisuth, T. Clinical Features, Endoscopic Findings, and Predictive Factors for Mortality in Tissue-Invasive Gastrointestinal Cytomegalovirus Disease between Immunocompetent and Immunocompromised Patients. Gastroenterol. Res. Pract. 2021, 2021, 8886525. [Google Scholar] [CrossRef] [PubMed]
- Chaemsupaphan, T.; Limsrivilai, J.; Thongdee, C.; Sudcharoen, A.; Pongpaibul, A.; Pausawasdi, N.; Charatcharoenwitthaya, P. Patient characteristics, clinical manifestations, prognosis, and factors associated with gastrointestinal cytomegalovirus infection in immunocompetent patients. BMC Gastroenterol. 2020, 20, 22. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.; Lee, J.; Kim, D.S.; Lee, J.W.; Hong, S.W.; Hwang, H.W.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Ye, B.D.; et al. Endoscopic features and clinical outcomes of cytomegalovirus gastroenterocolitis in immunocompetent patients. Sci. Rep. 2021, 11, 6284. [Google Scholar] [CrossRef] [PubMed]
- Kovaiou, R.D.; Weinberger, B.; Grubeck-Loebenstein, B. 33—Aging and the immune system. In Clinical Immunology, 3rd ed.; Rich, R.R., Fleisher, T.A., Shearer, W.T., Schroeder, H.W., Frew, A.J., Weyand, C.M., Eds.; Mosby: Edinburgh, Scotland, 2008; pp. 503–511. [Google Scholar]
- Azevedo, L.S.; Pierrotti, L.C.; Abdala, E.; Costa, S.F.; Strabelli, T.M.; Campos, S.V.; Ramos, J.F.; Latif, A.Z.; Litvinov, N.; Maluf, N.Z.; et al. Cytomegalovirus infection in transplant recipients. Clinics 2015, 70, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Razonable, R.R.; Humar, A. Cytomegalovirus in solid organ transplant recipients—Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13512. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Ar, M.C.; Machado, C.M.; Wu, D.; Singh, I.; Sandhu, A.; Demuth, D.; Slavin, M. Epidemiology, treatment patterns, and disease burden of cytomegalovirus in hematopoietic cell transplant recipients in selected countries outside of Europe and North America: A systematic review. Transpl. Infect. Dis. 2023, 25, e14083. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, F.; Spallone, A.; Kotton, C.N.; Chemaly, R.F. Cytomegalovirus infection in transplant recipients: Newly approved additions to our armamentarium. Clin. Microbiol. Infect. 2023, 29, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, D.; Sutherland, R.; Raffe, S.; Pool, E.; Beadsworth, M. British HIV Association guidelines on the management of opportunistic infection in people living with HIV: The clinical management of gastrointestinal opportunistic infections 2020. HIV Med. 2020, 21, 1–19. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Immunocompromised (N = 193) | Immunocompetent (N = 208) | Total (N = 401) | p-Value | |
|---|---|---|---|---|
| General data | ||||
| Age (year) (mean ± SD) | 54.6 ± 17.9 | 65.4 ± 17.3 | 60.2 ± 18.4 | <0.001 * |
| Gender (male/female) | 129/64 | 125/83 | 254/147 | 0.161 |
| Outpatient/inpatient | 38/155 | 51/157 | 89/312 | 0.245 |
| Critical illness (N (%)) | ||||
| Shock | 37 (19.2) | 50 (24) | 87 (21.7) | 0.237 |
| Pneumonia | 60 (31.1) | 44 (21.2) | 104 (25.9) | 0.023 * |
| Intubation | 26 (13.5) | 49 (23.6) | 75 (18.7) | 0.010 * |
| Intensive care unit | 36 (18.7) | 60 (28.8) | 96 (23.9) | 0.017 * |
| AKI | 30 (15.5) | 50 (24) | 80 (20) | 0.033 * |
| Underlying diseases (N (%)) | ||||
| Diabetes mellitus | 31 (16.1) | 85 (40.9) | 116 (28.9) | <0.001 * |
| Hypertension | 71 (36.8) | 110 (52.9) | 181 (45.1) | 0.001 * |
| Old CVA | 11 (5.7) | 36 (17.3) | 47 (11.7) | <0.001 * |
| COPD | 9 (4.7) | 9 (4.3) | 18 (4.5) | 0.871 |
| CAD | 17 (8.8) | 33 (15.9) | 50 (12.5) | 0.033 * |
| Liver cirrhosis | 7 (3.6) | 10 (4.8) | 17 (4.2) | 0.558 |
| ESRD | 19 (9.8) | 29 (13.9) | 48 (12) | 0.207 |
| CKD | 40 (20.7) | 51 (24.5) | 91 (22.7) | 0.365 |
| Hematology diseases | 12 (6.2) | 2 (1) | 14 (3.5) | 0.004 * |
| Crohn’s disease | 5 (2.6) | 7 (3.4) | 12 (3) | 0.773 |
| Ulcerative colitis | 14 (7.3) | 28 (13.5) | 42 (10.5) | 0.043 * |
| HBV | 22 (11.4) | 16 (7.7) | 38 (9.5) | 0.205 |
| HCV | 10 (5.2) | 7 (3.4) | 17 (4.2) | 0.367 |
| Laboratory tests | ||||
| WBC (/uL) | 7129.9 ± 4930.9 | 8696 ± 3835.6 | 7923.5 ± 4473.3 | 0.001 * |
| Segment (%) | 75.1 ± 15.2 | 71.2 ± 13.9 | 73.1 ± 14.6 | 0.011 * |
| Lymphocyte (%) | 14.5 ± 12.7 | 18.9 ± 12.2 | 16.7 ± 12.6 | 0.001 * |
| Hemoglobin (g/dL) | 9.9 ± 2 | 10.6 ± 2.7 | 10.3 ± 2.4 | 0.005 * |
| Platelet (1000/uL) | 193 ± 110.9 | 246.4 ± 119.9 | 220.1 ± 118.5 | <0.001 * |
| Bilirubin (mg/dL) | 1.5 ± 5.2 | 0.8 ± 1.1 | 1.2 ± 3.9 | 0.129 |
| ALT (IU/L) | 51.9 ± 144.1 | 25.4 ± 27.8 | 38.9 ± 105.4 | 0.016 * |
| Creatinine (mg/dL) | 1.5 ± 2.6 | 1.9 ± 2.2 | 1.7 ± 2.4 | 0.068 |
| Albumin (g/dL) | 2.8 ± 0.7 | 3.1 ± 4 | 2.9 ± 2.8 | 0.306 |
| CRP (mg/L) | 66.2 ± 77.4 | 55.3 ± 61.7 | 60.5 ± 69.7 | 0.177 |
| Virology tests (N-positive/N-tested (%)) | ||||
| CMV-IgM | 17/84 (20.2) | 17/94 (18.1) | 34/178 (19.1) | 0.884 |
| CMV-IgG | 77/79 (97.5) | 86/88 (97.7) | 163/167 (97.6) | 0.956 |
| CMV-antigenemia | 44/68 (64.7) | 24/56 (42.9) | 68/124 (54.8) | 0.011 * |
| CMV-viremia | 57/74 (77) | 39/56 (69.6) | 96/130 (73.8) | 0.033 * |
| C. diff (colon) | 7 (8.1) | 17 (11.5) | 24 (10.3) | 0.416 |
| CI (colon) | 0 (0) | 4 (2.7) | 4 (1.7) | 0.299 |
| Symptoms (N (%)) | ||||
| Fever | 65 (33.7) | 57 (27.4) | 122 (30.4) | 0.172 |
| Abdominal pain | 65 (33.7) | 69 (33.2) | 134 (33.4) | 0.915 |
| GI bleeding | 75 (38.9) | 108 (51.9) | 183 (45.6) | 0.009 * |
| Endoscopic findings (N (%)) | ||||
| Polypoid mass | 21 (10.9) | 23 (11.1) | 44 (11) | 0.955 |
| Inflammation | 17 (8.8) | 22 (10.6) | 39 (9.7) | 0.550 |
| Ulcer | 169 (87.6) | 171 (82.2) | 340 (84.8) | 0.136 |
| Treatment (N (%)) | ||||
| Operation | 14 (7.3) | 11 (5.3) | 25 (6.2) | 0.416 |
| Antiviral therapy | ||||
| IV and PO | 37 (19.2) | 32 (15.4) | 69 (17.2) | 0.316 |
| IV or PO | 128 (66.3) | 119 (57.2) | 247 (61.6) | 0.061 |
| IV duration (day) | 14 (8, 18) | 14 (7.25, 15) | 14 (8, 16.5) | 0.096 |
| PO duration (day) | 16 (10, 28) | 15.5 (10, 22) | 16 (10, 27.3) | 0.063 |
| Total duration (day) | 17 (11, 34.5) | 17 (12, 28) | 17 (11, 28) | 0.035 * |
| Total duration ≥ 14 days | 90 (46.6) | 87 (41.8) | 177 (44.1) | 0.333 |
| Outcomes (N (%)) | ||||
| Time to diagnosis (day) | 19.2 ± 16.5 | 19.9 ± 21.3 | 19.6 ± 19.1 | 0.726 |
| Admission time (day) | 37.1 ± 27.3 | 44.7 ± 36.8 | 40.8 ± 32.6 | 0.039 * |
| Follow-up time (day) | 855.9 ± 1346.4 | 905.2 ± 1343.7 | 881.5–1343.5 | 0.714 |
| Perforation | 6 (3.1) | 5 (2.4) | 11 (2.7) | 0.666 |
| Recurrence | 10 (5.2) | 10 (4.8) | 20 (5) | 0.573 |
| In-hospital mortality | 47 (24.4) | 33 (15.9) | 80 (20) | 0.034 * |
| Overall mortality | 92 (47.7) | 63 (30.3) | 155 (38.7) | <0.001 * |
| Immunocompromised | Immunocompetent | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age | 1.029 | 1.008–1.050 | 0.007 * | 1.036 | 1.008–1.066 | 0.012 * | 1.08 | 1.006–1.159 | 0.032 * | |||
| Gender (male) | 1.349 | 0.681–2.674 | 0.391 | 1.311 | 0.620–2.775 | 0.479 | ||||||
| Outpatient | 0.064 | 0.009–0.481 | 0.008 * | 0 | 0– | 0.997 | ||||||
| Shock | 10.676 | 4.763–23.929 | <0.001 * | 3.333 | 1.530–7.264 | 0.002 * | ||||||
| Pneumonia | 3.604 | 1.812–7.167 | <0.001 * | 6.877 | 3.084–15.334 | <0.001 * | ||||||
| Intubation | 5.753 | 2.414–13.707 | <0.001 * | 5.574 | 2.536–12.251 | <0.001 * | ||||||
| Intensive care unit | 7.054 | 3.218–15.464 | <0.001 * | 12.5 | 5.195–30.079 | <0.001 * | ||||||
| Diabetes mellitus | 0.41 | 0.136–1.240 | 0.114 | 1.934 | 0.914–4.095 | 0.085 | ||||||
| Hypertension | 1.742 | 0.893–3.398 | 0.103 | 1.691 | 0.784–3.647 | 0.180 | ||||||
| Old CVA | 1.847 | 0.516–6.612 | 0.346 | 2.056 | 0.862–4.901 | 0.104 | ||||||
| COPD | 1.591 | 0.382–6.626 | 0.524 | 0 | 0– | 0.999 | ||||||
| CAD | 2.38 | 0.851–6.655 | 0.098 | 2.359 | 0.980–5.682 | 0.056 | ||||||
| Liver cirrhosis | 0.507 | 0.059–4.324 | 0.535 | 0.576 | 0.071–4.759 | 0.607 | ||||||
| ESRD | 0.554 | 0.154–1.992 | 0.366 | 1.872 | 0.727–4.825 | 0.194 | ||||||
| CKD | 1.685 | 0.785–3.616 | 0.180 | 0.802 | 0.325–1.975 | 0.631 | ||||||
| AKI | 2.901 | 1.284–6.555 | 0.010 * | 2.845 | 1.302–6.216 | 0.009 * | ||||||
| Malignancy | 2.666 | 1.355–5.244 | 0.005 * | 0.775 | 0.217–2.773 | 0.695 | ||||||
| Chemotherapy | 1.717 | 0.872–3.382 | 0.118 | na | na | na | ||||||
| Radiotherapy | 2.211 | 1.091–4.483 | 0.028 * | na | na | na | ||||||
| Transplant | 0.706 | 0.225–2.213 | 0.550 | 0 | 0– | 1 | ||||||
| Hematology disease | 1.605 | 0.461–5.59 | 0.458 | 5.437 | 0.332–89.179 | 0.235 | ||||||
| Autoimmune/PID | 0.75 | 0.265–2.123 | 0.588 | 5.581 | 0.758–41.108 | 0.092 | ||||||
| Crohn’s disease | 0 | 0– | 0.999 | 0 | 0– | 0.999 | ||||||
| Ulcerative colitis | 0.496 | 0.107–2.302 | 0.371 | 0.171 | 0.022–1.307 | 0.089 | ||||||
| HIV | 0.216 | 0.063–0.74 | 0.015 * | na | na | na | ||||||
| HBV | 0.456 | 0.129–1.615 | 0.223 | 1.246 | 0.335–4.639 | 0.743 | ||||||
| HCV | 0.331 | 0.041–2.683 | 0.300 | 0.88 | 0.102–7.56 | 0.907 | ||||||
| Corticosteroids | 2.484 | 1.173–5.261 | 0.017 * | 1.398 | 0.523–3.74 | 0.504 | ||||||
| Immunosuppressant | 0.448 | 0.186–1.081 | 0.074 | 0 | 0– | 1 | ||||||
| NLR | 1.042 | 1.022–1.063 | <0.001 * | 1.08 | 1.044–1.118 | <0.001 * | ||||||
| Hemoglobin | 0.775 | 0.651–0.924 | 0.004 * | 0.809 | 0.664–0.986 | 0.036 * | ||||||
| Platelet | 0.993 | 0.989–0.997 | <0.001 * | 0.992 | 0.988–0.996 | <0.001 * | ||||||
| Bilirubin | 1.05 | 0.97–1.137 | 0.226 | 1.046 | 0.715–1.528 | 0.818 | ||||||
| ALT | 1.007 | 1.001–1.013 | 0.023 * | 1.005 | 0.992–1.017 | 0.458 | ||||||
| Creatinine | 1.108 | 0.961–1.278 | 0.159 | 1 | 0.837–1.195 | 1 | ||||||
| Albumin | 0.31 | 0.168–0.572 | <0.001 * | 0.217 | 0.089–0.531 | 0.001 * | ||||||
| CRP | 1.009 | 1.004–1.014 | <0.001 * | 1.01 | 1.004–1.016 | 0.001 * | ||||||
| Fever | 1.663 | 0.845–3.27 | 0.141 | 3.076 | 1.428–6.624 | 0.004 * | ||||||
| Abdominal pain | 1.022 | 0.51–2.046 | 0.952 | 0.719 | 0.314–1.644 | 0.434 | ||||||
| GI bleeding | 4.491 | 2.232–9.038 | <0.001 * | 5.782 | 1.257–26.599 | 0.024 * | 6.65 | 2.454–18.022 | <0.001 * | 10.036 | 1.183–85.133 | 0.035 * |
| Lesion—polypoid | 0.485 | 0.136–1.725 | 0.264 | 0 | 0– | 0.998 | ||||||
| Lesion—inflammation | 0.388 | 0.085–1.764 | 0.220 | 1.203 | 0.38–3.813 | 0.753 | ||||||
| Lesion—ulcer | 3.992 | 0.902–17.663 | 0.068 | 1.685 | 0.554–5.122 | 0.358 | ||||||
| Operation | 2.524 | 0.828–7.694 | 0.103 | 3.31 | 0.911–12.028 | 0.069 | ||||||
| Any antiviral therapy | 0.979 | 0.489–1.96 | 0.952 | 1.375 | 0.637–2.968 | 0.417 | ||||||
| Therapy duration ≥ 14 days | 0.391 | 0.193–0.790 | 0.009 * | 0.232 | 0.059–0.911 | 0.036 * | 0.762 | 0.353–1.645 | 0.489 | |||
| Time-to-diagnosis period | 1.044 | 1.021–1.068 | <0.001 * | 1.023 | 1.003–1.043 | 0.021 * | 1.029 | 1.004–1.055 | 0.021 * | |||
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age | 1.036 | 1.008–1.066 | 0.012 * | 1.08 | 1.006–1.159 | 0.032 * |
| Gender (male) | 1.311 | 0.620–2.775 | 0.479 | |||
| Outpatient | 0 | 0- | 0.997 | |||
| Shock | 3.333 | 1.530–7.264 | 0.002 * | |||
| Pneumonia | 6.877 | 3.084–15.334 | <0.001 * | |||
| Intubation | 5.574 | 2.536–12.251 | <0.001 * | |||
| ICU | 12.5 | 5.195–30.079 | <0.001 * | |||
| DM | 1.934 | 0.914–4.095 | 0.085 | |||
| HTN | 1.691 | 0.784–3.647 | 0.180 | |||
| Old CVA | 2.056 | 0.862–4.901 | 0.104 | |||
| COPD | 0 | 0- | 0.999 | |||
| CAD | 2.359 | 0.980–5.682 | 0.056 | |||
| LC | 0.576 | 0.071–4.759 | 0.607 | |||
| ESRD | 1.872 | 0.727–4.825 | 0.194 | |||
| CKD | 0.802 | 0.325–1.975 | 0.631 | |||
| AKI | 2.845 | 1.302–6.216 | 0.009 * | |||
| Malignancy | 0.775 | 0.217–2.773 | 0.695 | |||
| Chemotherapy | na | na | na | |||
| Radiotherapy | na | na | na | |||
| Transplant | 0 | 0- | 1 | |||
| Hematology disease | 5.437 | 0.332–89.179 | 0.235 | |||
| Autoimmune/PID | 5.581 | 0.758–41.108 | 0.092 | |||
| Crohn’s disease | 0 | 0- | 0.999 | |||
| Ulcerative colitis | 0.171 | 0.022–1.307 | 0.089 | |||
| HIV | na | na | na | |||
| HBV | 1.246 | 0.335–4.639 | 0.743 | |||
| HCV | 0.88 | 0.102–7.56 | 0.907 | |||
| Corticosteroids | 1.398 | 0.523–3.74 | 0.504 | |||
| Immunosuppressant | 0 | 0- | 1 | |||
| NLR | 1.08 | 1.044–1.118 | <0.001 * | |||
| Hemoglobin | 0.809 | 0.664–0.986 | 0.036 * | |||
| Platelet | 0.992 | 0.988–0.996 | <0.001 * | |||
| Bilirubin | 1.046 | 0.715–1.528 | 0.818 | |||
| ALT | 1.005 | 0.992–1.017 | 0.458 | |||
| Creatinine | 1 | 0.837–1.195 | 1 | |||
| Albumin | 0.217 | 0.089–0.531 | 0.001 * | |||
| CRP | 1.01 | 1.004–1.016 | 0.001 * | |||
| Fever | 3.076 | 1.428–6.624 | 0.004 * | |||
| Abdominal pain | 0.719 | 0.314–1.644 | 0.434 | |||
| GI bleeding | 6.65 | 2.454–18.022 | <0.001 * | 10.036 | 1.183–85.133 | 0.035 * |
| Lesion—polypoid | 0 | 0- | 0.998 | |||
| Lesion—inflammation | 1.203 | 0.38–3.813 | 0.753 | |||
| Lesion—ulcer | 1.685 | 0.554–5.122 | 0.358 | |||
| Operation | 3.31 | 0.911–12.028 | 0.069 | |||
| Any antiviral therapy | 1.375 | 0.637–2.968 | 0.417 | |||
| Therapy duration ≥ 14 days | 0.762 | 0.353–1.645 | 0.489 | |||
| Time-to-diagnosis period | 1.023 | 1.003–1.043 | 0.021 * | 1.029 | 1.004–1.055 | 0.021 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, P.-J.; Wu, R.-C.; Tsou, Y.-K.; Chen, C.-M.; Chiu, C.-T.; Chen, C.-C.; Lai, M.-W.; Pan, Y.-B.; Le, P.-H. Comparative Analysis of Cytomegalovirus Gastrointestinal Disease in Immunocompetent and Immunocompromised Patients. Viruses 2024, 16, 452. https://doi.org/10.3390/v16030452
Yeh P-J, Wu R-C, Tsou Y-K, Chen C-M, Chiu C-T, Chen C-C, Lai M-W, Pan Y-B, Le P-H. Comparative Analysis of Cytomegalovirus Gastrointestinal Disease in Immunocompetent and Immunocompromised Patients. Viruses. 2024; 16(3):452. https://doi.org/10.3390/v16030452
Chicago/Turabian StyleYeh, Pai-Jui, Ren-Chin Wu, Yung-Kuan Tsou, Chien-Ming Chen, Cheng-Tang Chiu, Chien-Chang Chen, Ming-Wei Lai, Yu-Bin Pan, and Puo-Hsien Le. 2024. "Comparative Analysis of Cytomegalovirus Gastrointestinal Disease in Immunocompetent and Immunocompromised Patients" Viruses 16, no. 3: 452. https://doi.org/10.3390/v16030452
APA StyleYeh, P.-J., Wu, R.-C., Tsou, Y.-K., Chen, C.-M., Chiu, C.-T., Chen, C.-C., Lai, M.-W., Pan, Y.-B., & Le, P.-H. (2024). Comparative Analysis of Cytomegalovirus Gastrointestinal Disease in Immunocompetent and Immunocompromised Patients. Viruses, 16(3), 452. https://doi.org/10.3390/v16030452