Analysis of an Outbreak of Hemorrhagic Fever with Renal Syndrome in College Students in Xi’an, China

 ,
,
Abstract
:1. Introduction
2. Experimental
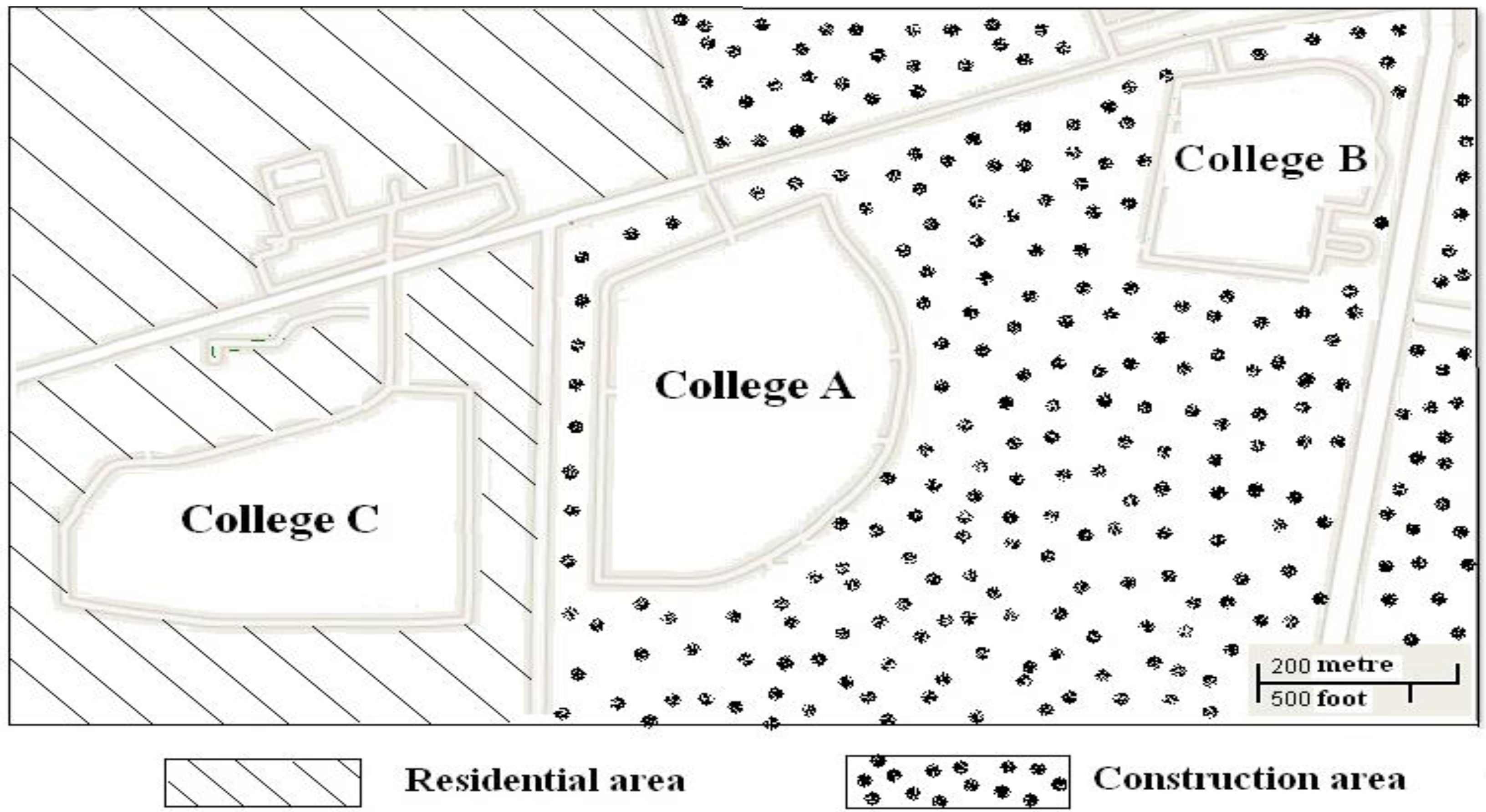
2.1. Rodent Population Density Survey and Sample Collection

2.2. Detection of Antibody against HV in the Sera
2.3. Reverse Transcriptase-PCR for the Detection of HV RNA
2.4. Amplification and Sequencing of the S Segments and Phylogenetic Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical Manifestations

{kind=link}
{kind=link}
| Clinical Data | Patient No. | |||||
|---|---|---|---|---|---|---|
| 1 * | 2 * | 3 | 4 | 5 | 6 | |
| Sex | F | M | F | F | M | M |
| Age(Year) | 23.3 | 19.6 | 22.4 | 19.1 | 20.6 | 22.8 |
| Signs and symptoms | ||||||
| Fever (days) | 7 | 9 | 4 | 4 | 3 | 5 |
| Peak temperature (°C) | 39.4 | 39.8 | 39.6 | 40.2 | 39.2 | 40.7 |
| Chills | Y | Y | N | N | N | N |
| Malaise | Y | Y | Y | Y | Y | Y |
| Fatigue | Y | Y | Y | Y | Y | Y |
| Myalgia | Y | N | N | N | N | N |
| Abdominal pain | Y | Y | N | N | N | N |
| Nausea | Y | Y | Y | Y | Y | Y |
| Vomiting | Y | Y | N | N | N | N |
| Backache | Y | Y | Y | Y | Y | Y |
| Chest pain | Y | Y | Y | Y | Y | Y |
| Eyeball pain | Y | Y | Y | Y | Y | Y |
| Diffuse reddening | Y | Y | Y | Y | Y | Y |
| Bradycardia | N | N | Y | N | Y | N |
| Photophobia | N | N | Y | N | N | N |
| Pharynx enanthema | N | N | N | N | N | Y |
| Petechia | Y | Y | Y | Y | Y | Y |
| Conjunctival hemorrhages | Y | Y | Y | Y | Y | Y |
| Thrombocytopenia | Y | Y | Y | Y | Y | Y |
| Acute tubulointerstitial nephritis | Y | Y | Y | Y | Y | Y |
| Proteinuria | Y | Y | Y | Y | Y | Y |
| Shock | Y | Y | N | N | N | N |
| Hypotension | Y | Y | N | N | N | N |
| Necrotizing glomerulonephritis | Y | Y | N | N | N | N |
| Multi-organ hypoperfusion | Y | Y | N | N | N | N |
| Multi-organ dysfunction | Y | Y | N | N | N | N |
| Multi-organ failure | Y | Y | N | N | N | N |
3.2. Rodent Population Density Survey
| Campus | Rn | Mm | Aa | |||
|---|---|---|---|---|---|---|
| number | IgG Positive | number | IgG Positive | number | IgG Positive | |
| College A | 10 | 2 | 7 | 2 | 1 | 0 |
| College B | 8 | 2 | 6 | 1 | 0 | 0 |
| College C | 3 | 0 | 1 | 0 | 0 | 0 |
| Total | 21 | 4 | 14 | 3 | 1 | 0 |
3.3. Detection of Anti-HV Antibody
| Patients | IgM (Positive days after onset) | IgG | HV RNA genotyping (Positive days after onset) | S segment |
|---|---|---|---|---|
| 1 * | +(6) | - | - | / |
| 2 * | +(7) | + | - | / |
| 3 | +(5) | - | HTNV(0) | + |
| 4 | +(4) | + | HTNV (1) | / |
| 5 | +(4) | + | - | / |
| 6 | +(5) | + | HTNV (1) | + |
3.4. HV RNA Detection and Sequencing of S Segments from Samples
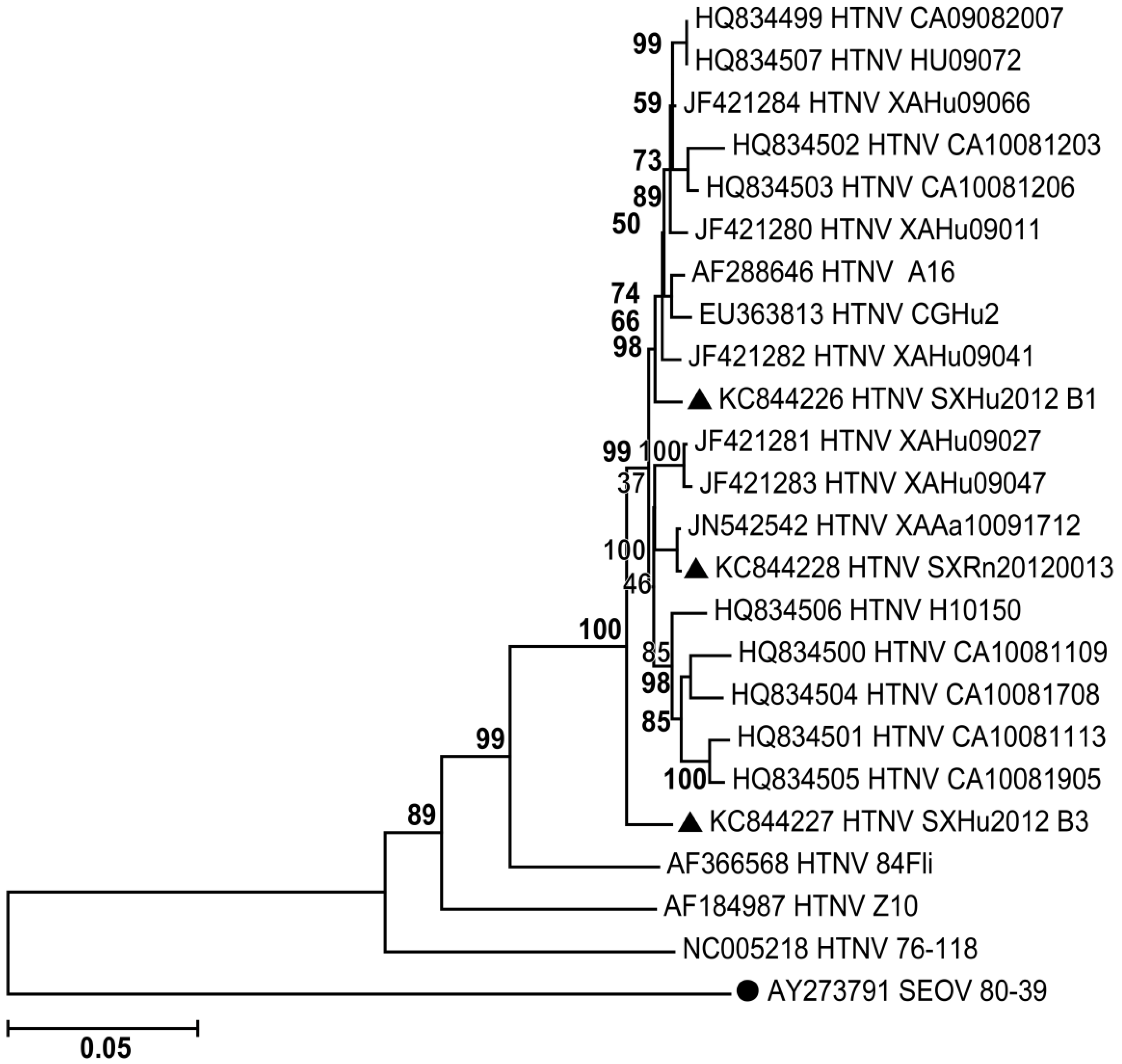
3.5. Phylogenetic Analysis

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References and Notes
- Sheedy, J.A.; Froeb, H.F.; Batson, H.A.; Conley, C.C.; Murphy, J.P.; Hunter, R.B.; Cugell, D.W.; Giles, R.B.; Bershadsky, S.C.; Vester, J.W.; et al. The clinical course of epidemic hemorrhagic fever. Am. J. Med. 1954, 16, 619–628. [Google Scholar] [CrossRef]
- Maes, P.; Clement, J.; Gavrilovskaya, I.; van Ranst, M. Hantaviruses: Immunology, treatment, and prevention. Viral Immunol. 2004, 17, 481–497. [Google Scholar]
- Vapalahti, O.; Mustonen, J.; Lundkvist, A.; Henttonen, H.; Plyusnin, A.; Vaheri, A. Hantavirus infections in Europe. Lancet Infect. Dis. 2003, 3, 653–661. [Google Scholar] [CrossRef]
- Schmaljohn, C.; Hjelle, B. Hantaviruses: A global disease problem. Emerg. Infect. Dis. 1997, 3, 95–104. [Google Scholar] [CrossRef]
- Chen, H.X.; Qiu, F.X. Epidemiologic surveillance on the hemorrhagic fever with renal syndrome in China. Chin. Med. J. (Engl.) 1993, 106, 857–863. [Google Scholar]
- Ma, C.; Yu, P.; Nawaz, M.; Zuo, S.; Jin, T.; Li, Y.; Li, J.; Li, H.; Xu, J. Hantaviruses in rodents and humans, Xi’an, PR China. J. Gen. Virol. 2012, 93, 2227–2236. [Google Scholar] [CrossRef]
- BioEdit Sequence Alignment Editor. Available online: http://www.mbio.ncsu.edu/BioEdit/bioedit.html (accessed on 28 January 2014).
- Dereeper, A.; Guignon, V.; Blanc, G.; Audic, S.; Buffet, S.; Chevenet, F.; Dufayard, J.F.; Guindon, S.; Lefort, V.; Lescot, M.; et al. Phylogeny.fr: Robust phylogenetic analysis for the non-specialist. Nucleic Acids Res. 2008, 36, W465–W469. [Google Scholar] [CrossRef] [Green Version]
- National Center for Biotechology Information. Available online: http://www.ncbi.nlm.nih.gov/genbank/ (accessed on 28 January 2014).
- Zhang, Y.Z.; Zou, Y.; Fu, Z.F.; Plyusnin, A. Hantavirus infections in humans and animals, China. Emerg. Infect. Dis. 2010, 16, 1195–1203. [Google Scholar] [CrossRef]
- Huggins, J.W.; Hsiang, C.M.; Cosgriff, T.M.; Guang, M.Y.; Smith, J.I.; Wu, Z.O.; LeDuc, J.W.; Zheng, Z.M.; Meegan, J.M.; Wang, Q.N.; et al. Prospective, double-blind, concurrent, placebo-controlled clinical trial of intravenous ribavirin therapy of hemorrhagic fever with renal syndrome. J. Infect. Dis. 1991, 164, 1119–1127. [Google Scholar] [CrossRef]
- Zoller, L.; Faulde, M.; Meisel, H.; Ruh, B.; Kimmig, P.; Schelling, U.; Zeier, M.; Kulzer, P.; Becker, C.; Roggendorf, M.; et al. Seroprevalence of hantavirus antibodies in Germany as determined by a new recombinant enzyme immunoassay. Eur. J. Clin. Microbiol. Infect. Dis. 1995, 14, 305–313. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ma, C.; Wang, Z.; Li, S.; Xing, Y.; Wu, R.; Wei, J.; Nawaz, M.; Tian, H.; Xu, B.; Wang, J.; et al. Analysis of an Outbreak of Hemorrhagic Fever with Renal Syndrome in College Students in Xi’an, China. Viruses 2014, 6, 507-515. https://doi.org/10.3390/v6020507
Ma C, Wang Z, Li S, Xing Y, Wu R, Wei J, Nawaz M, Tian H, Xu B, Wang J, et al. Analysis of an Outbreak of Hemorrhagic Fever with Renal Syndrome in College Students in Xi’an, China. Viruses. 2014; 6(2):507-515. https://doi.org/10.3390/v6020507
Chicago/Turabian StyleMa, Chaofeng, Zengguo Wang, Shen Li, Yuan Xing, Rui Wu, Jing Wei, Muhammad Nawaz, Huaiyu Tian, Bing Xu, Jingjun Wang, and et al. 2014. "Analysis of an Outbreak of Hemorrhagic Fever with Renal Syndrome in College Students in Xi’an, China" Viruses 6, no. 2: 507-515. https://doi.org/10.3390/v6020507
APA StyleMa, C., Wang, Z., Li, S., Xing, Y., Wu, R., Wei, J., Nawaz, M., Tian, H., Xu, B., Wang, J., & Yu, P. (2014). Analysis of an Outbreak of Hemorrhagic Fever with Renal Syndrome in College Students in Xi’an, China. Viruses, 6(2), 507-515. https://doi.org/10.3390/v6020507