Increased Plasma Cell-Free DNA Level during HTNV Infection: Correlation with Disease Severity and Virus Load

Abstract
:1. Introduction
2. Results and Discussion
2.1. Study Population Characteristics

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Characteristic | Value |
|---|---|---|
| Disease severity (No. of patients) | Mild | 10 |
| Moderate | 22 | |
| Severe | 24 | |
| Critical | 20 | |
| Stage of collection (No. of samples) | Febrile | 36 |
| Hypotensive | 9 | |
| Oliguric | 40 | |
| Diuretic | 56 | |
| Convalescent | 25 | |
| Age (ys) | Range | 9–73 |
| Mean | 42 | |
| Sex (No. of patients) | Male | 57 |
| Female | 19 | |
| Platelets min (109/L) | Range | 1–161 |
| Mean | 33.78 | |
| Creatinine max (µmol/L) | Range | 83.9–931.8 |
| Mean | 403.06 | |
| WBC max (109/L) | Range | 5.03–91 |
| Mean | 23.82 |
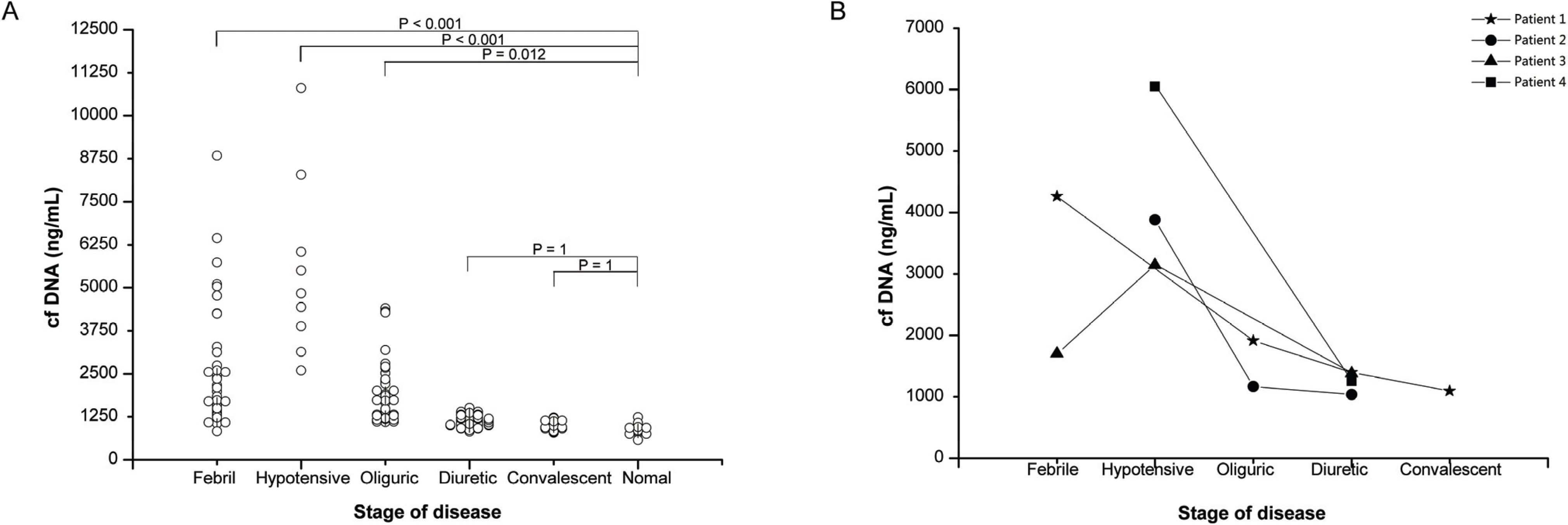
2.2. Cf-DNA Level in HFRS Patients

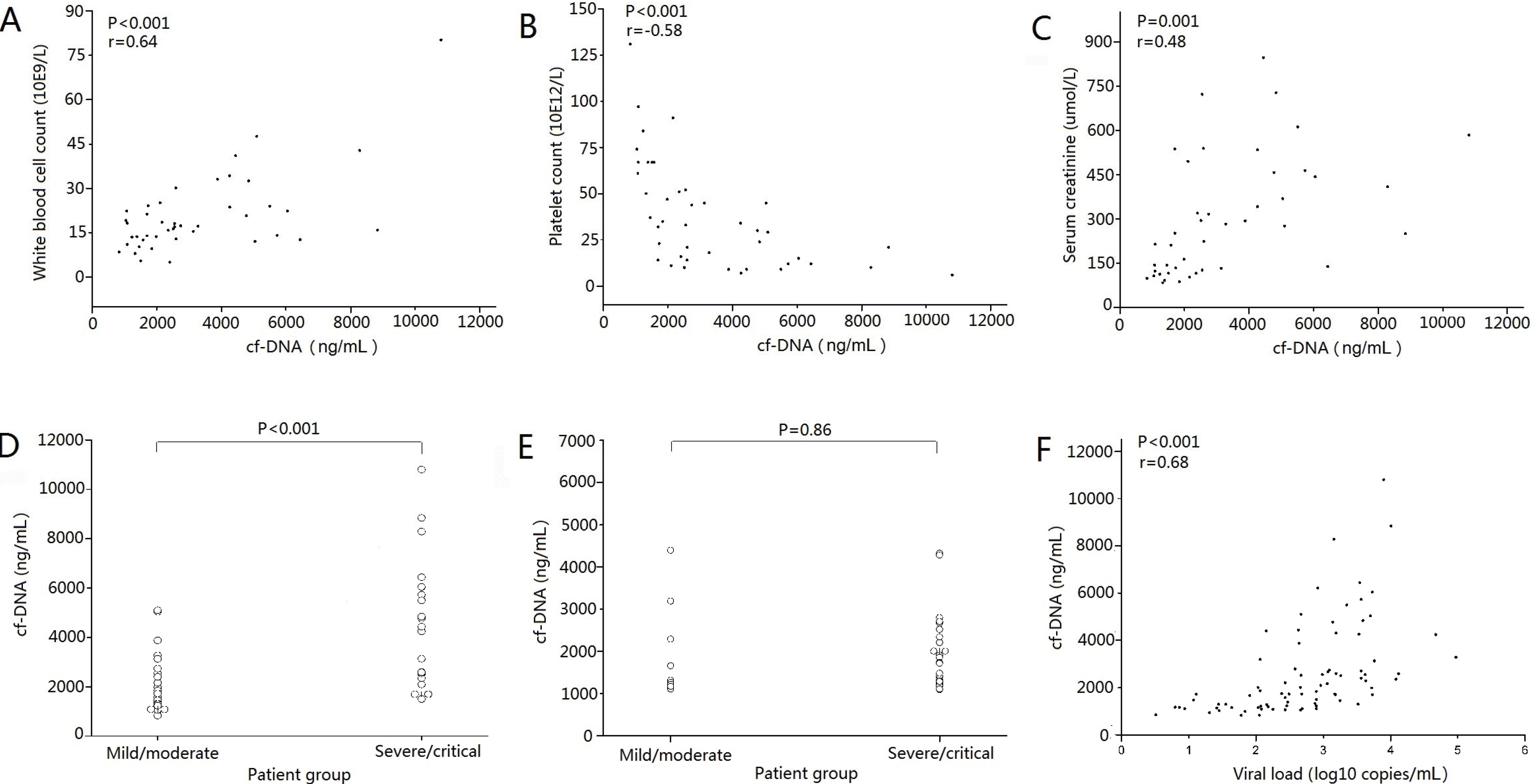
2.3. Cf-DNA Level and Disease Severity of HFRS

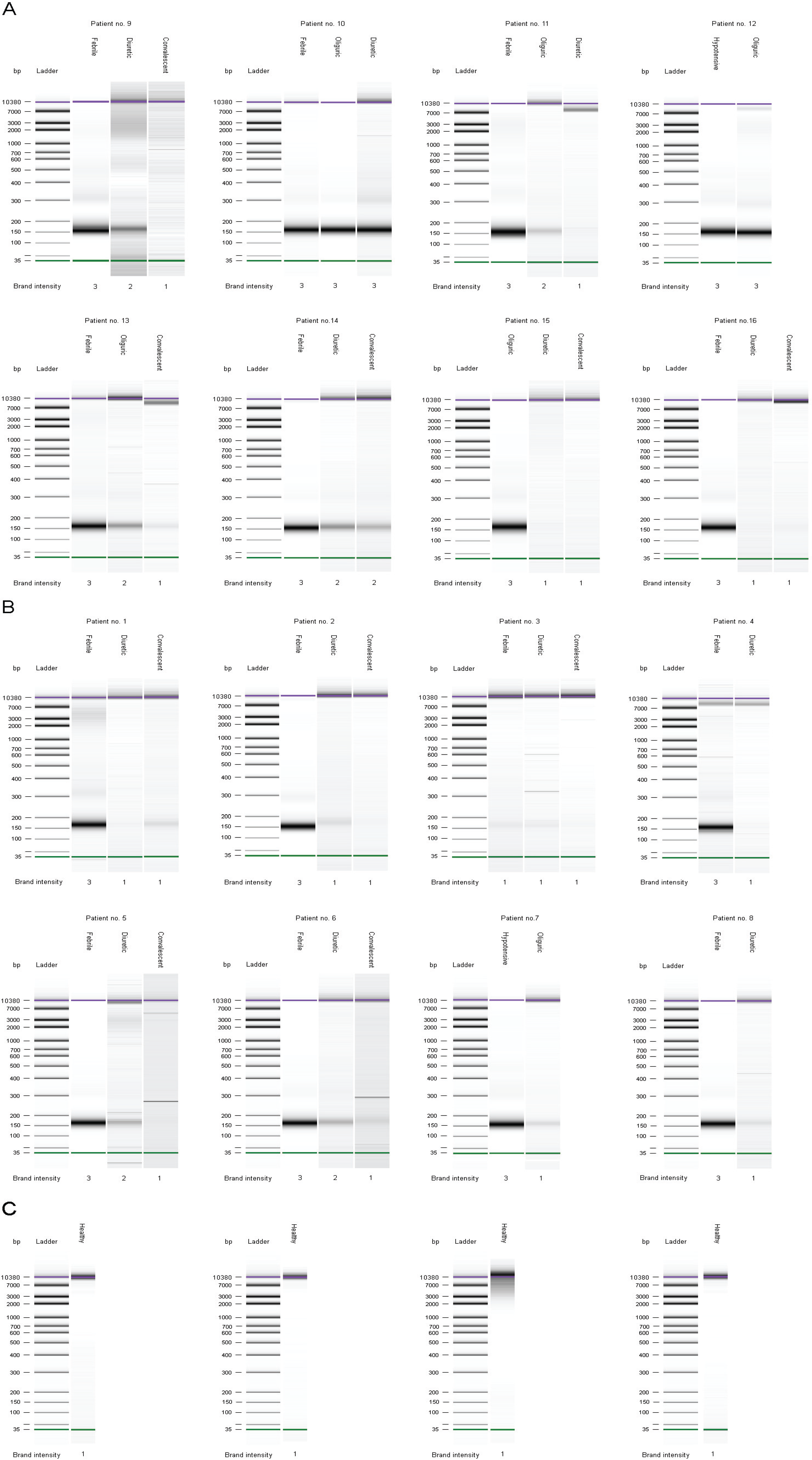
2.4. Qualitative Analysis of Plasma cf-DNA

2.5. Cf-DNA Sequencing and Alignment
2.6. Discussion
3. Experimental Section
3.1. Subjects
3.2. Clinical Data and Laboratory Tests
3.3. Quantification of Total Plasma cf-DNA
3.4. Extraction and Qualitative Analysis of Plasma cf-DNA
3.5. Illumina Sequencing
3.6. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Vaheri, A.; Strandin, T.; Hepojoki, J.; Sironen, T.; Henttonen, H.; Mäkelä, S.; Mustonen, J. Uncovering the mysteries of hantavirus infections. Nat. Rev. Microbiol. 2013, 11, 539–550. [Google Scholar] [CrossRef]
- Yi, J.; Xu, Z.; Zhuang, R.; Wang, J.; Zhang, Y.; Ma, Y.; Liu, B.; Zhang, Y.; Zhang, C.; Yan, G.; et al. Hantaan virus RNA load in patients having hemorrhagic fever with renal syndrome: Correlation with disease severity. J. Infect. Dis. 2013, 207, 1457–1461. [Google Scholar] [CrossRef]
- Huttunen, R.; Kuparinen, T.; Jylhävä, J.; Aittoniemi, J.; Vuento, R.; Huhtala, H.; Laine, J.; Syrjänen, J.; Hurme, M. Fatal outcome in bacteremia is characterized by high plasma cell free DNA concentration and apoptotic DNA fragmentation: A prospective cohort study. PLoS One 2011, 6, e21700. [Google Scholar]
- Swarup, V.; Rajeswari, M.R. Circulating (cell-free) nucleic acids—A promising, non-invasive tool for early detection of several human diseases. FEBS Lett. 2007, 581, 795–799. [Google Scholar]
- Tong, Y.-K.; Lo, Y.M. Diagnostic developments involving cell-free (circulating) nucleic acids. Clin. Chim. Acta 2006, 363, 187–196. [Google Scholar] [CrossRef]
- Tsang, J.; Jason, C.H.; Dennis Lo, Y.M. Circulating nucleic acids in plasma/serum. Pathology 2007, 39, 197–207. [Google Scholar] [CrossRef]
- Antonatos, D.; Patsilinakos, S.; Spanodimos, S.; Korkonikitas, P.; Tsigas, D. Cell-Free DNA Levels as a Prognostic Marker in Acute Myocardial Infarction. Ann. N. Y. Acad. Sci. 2006, 1075, 278–281. [Google Scholar]
- Rainer, T.H.; Lam, N.Y.; Man, C.Y.; Chiu, R.W.; Woo, K.S.; Lo, Y.M. Plasma β-globin DNA as a prognostic marker in chest pain patients. Clin. Chim. Acta 2006, 368, 110–113. [Google Scholar] [CrossRef]
- Stebbing, J.; Bower, M. Cell-Free DNA as a Biomarker in the Context of Cancer, Viruses, and Methylation. J. Infect. Dis. 2012, 205, 1032–1034. [Google Scholar] [CrossRef]
- Sigdel, T.K.; Vitalone, M.J.; Tran, T.Q.; Dai, H.; Hsieh, S.C.; Salvatierra, O.; Sarwal, M.M. A Rapid Noninvasive Assay for the Detection of Renal Transplant Injury. Transplantation 2013, 96, 97–101. [Google Scholar]
- Mustonen, J.; Mäkelä, S.; Outinen, T.; Laine, O.; Jylhävä, J.; Arstila, P.T.; Hurme, M.; Vaheri, A. The pathogenesis of nephropathia epidemica: New knowledge and unanswered questions. Antivir. Res. 2013, 100, 589–604. [Google Scholar] [CrossRef]
- Zaravinos, A.; Tzoras, S.; Apostolakis, S.; Lazaridis, K.; Spandidos, D.A. Levosimendan reduces plasma cell-free DNA levels in patients with ischemic cardiomyopathy. J. Thromb. Thrombolysis 2011, 31, 180–187. [Google Scholar] [CrossRef]
- Chen, Z.; Fadiel, A.; Naftolin, F.; Eichenbaum, K.D.; Xia, Y. Circulation DNA: Biological implications for cancer metastasis and immunology. Med. Hypotheses 2005, 65, 956–961. [Google Scholar]
- Chiba, S.; Baghdadi, M.; Akiba, H.; Yoshiyama, H.; Kinoshita, I.; Dosaka-Akita, H.; Fujioka, Y.; Ohba, Y.; Gorman, J.V.; Colgan, J.D.; et al. Tumor-infiltrating DCs suppress nucleic acid-mediated innate immune responses through interactions between the receptor TIM-3 and the alarmin HMGB1. Nat. Immunol. 2012, 13, 832–842. [Google Scholar] [CrossRef]
- Gougeon, M.L.; Melki, M.T.; Saïdi, H. HMGB1, an alarmin promoting HIV dissemination and latency in dendritic cells. Cell Death Differ. 2011, 19, 96–106. [Google Scholar] [CrossRef]
- Gugliesi, F.; Bawadekar, M.; De Andrea, M.; Dell’Oste, V.; Caneparo, V.; Tincani, A.; Gariglio, M.; Landolfo, S. Nuclear DNA Sensor IFI16 as Circulnating Protein in Autoimmune Diseases is a Signal of Damage that Impairs Endothelial Cells through High-Affinity Membrane Binding. PLoS One 2013, 8, e63045. [Google Scholar]
- Wang, M.; Wang, J.; Zhu, Y.; Xu, Z.; Yang, K.; Yang, A.; Jin, B. Cellular immune response to Hantaan virus nucleocapsid protein in the acute phase of hemorrhagic fever with renal syndrome: Correlation with disease severity. J. Infect. Dis. 2009, 199, 188–195. [Google Scholar]
- Expert 2100 software, version B.02.08 (SR2); Agilent Technologies Inc.: Santa Clara, CA, USA, 2012.
- Outinen, T.K.; Kuparinen, T.; Jylhävä, J.; Leppänen, S.; Mustonen, J.; Mäkelä, S.; Pörsti, I.; Syrjänen, J.; Vaheri, A.; Hurme, M. Plasma cell-free DNA levels are elevated in acute Puumala hantavirus infection. PLoS One 2012, 7, e31455. [Google Scholar]
- BWA software, version 0.7.5a-r405; Wellcome Trust Sanger Institute, Wellcome Trust Genome Campus: Cambridge, UK, 2009.
- Li, H. Aligning sequence reads, clone sequences and assembly contigs with BWA-MEM. ArXiv 2013, 1303, 3997. [Google Scholar]
- Li, H.; Durbin, R. Fast and accurate short read alignment with Burrows-Wheeler Transform. Bioinformatics 2009, 25, 1754–1760. [Google Scholar]
- Homo_sapiens.GRCh37.75. Available online: ftp://ftp.ensembl.org/pub/release-75/fasta/homo_sapiens/dna/ (accessed on 4 February 2014).
- HTNV genome. Available online: http://www.ncbi.nlm.nih.gov/genome/?term=X55901.1%2C+M14626.1%2C+M14627.1 (accessed on 4 February 2014).
- Statistical Package for the Social Sciences (SPSS), version 12.0; SPSS, Inc.: Chicago, IL, USA, 2008.
- Dwivedi, D.J.; Toltl, L.J.; Swystun, L.L.; Pogue, J.; Liaw, K.L.; Weitz, J.I.; Cook, D.J.; Fox-Robichaud, A.E.; Liaw, P.C.; The Canadian Critical Care Translational Biology Group. Prognostic utility and characterization of cell-free DNA in patients with severe sepsis. Crit. Care 2012, 16, 1–11. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yi, J.; Zhang, Y.; Zhang, Y.; Ma, Y.; Zhang, C.; Li, Q.; Liu, B.; Liu, Z.; Liu, J.; Zhang, X.; et al. Increased Plasma Cell-Free DNA Level during HTNV Infection: Correlation with Disease Severity and Virus Load. Viruses 2014, 6, 2723-2734. https://doi.org/10.3390/v6072723
Yi J, Zhang Y, Zhang Y, Ma Y, Zhang C, Li Q, Liu B, Liu Z, Liu J, Zhang X, et al. Increased Plasma Cell-Free DNA Level during HTNV Infection: Correlation with Disease Severity and Virus Load. Viruses. 2014; 6(7):2723-2734. https://doi.org/10.3390/v6072723
Chicago/Turabian StyleYi, Jing, Yun Zhang, Yusi Zhang, Ying Ma, Chunmei Zhang, Qi Li, Bei Liu, Zhijia Liu, Jiayun Liu, Xianqing Zhang, and et al. 2014. "Increased Plasma Cell-Free DNA Level during HTNV Infection: Correlation with Disease Severity and Virus Load" Viruses 6, no. 7: 2723-2734. https://doi.org/10.3390/v6072723
APA StyleYi, J., Zhang, Y., Zhang, Y., Ma, Y., Zhang, C., Li, Q., Liu, B., Liu, Z., Liu, J., Zhang, X., Zhuang, R., & Jin, B. (2014). Increased Plasma Cell-Free DNA Level during HTNV Infection: Correlation with Disease Severity and Virus Load. Viruses, 6(7), 2723-2734. https://doi.org/10.3390/v6072723