
Hyaluronic Acid Supplement as a Chondrogenic Adjuvant in Promoting the Therapeutic Efficacy of Stem Cell Therapy in Cartilage Healing

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Statement
2.2. Harvest and Cultivation of Bone Marrow Stem Cells
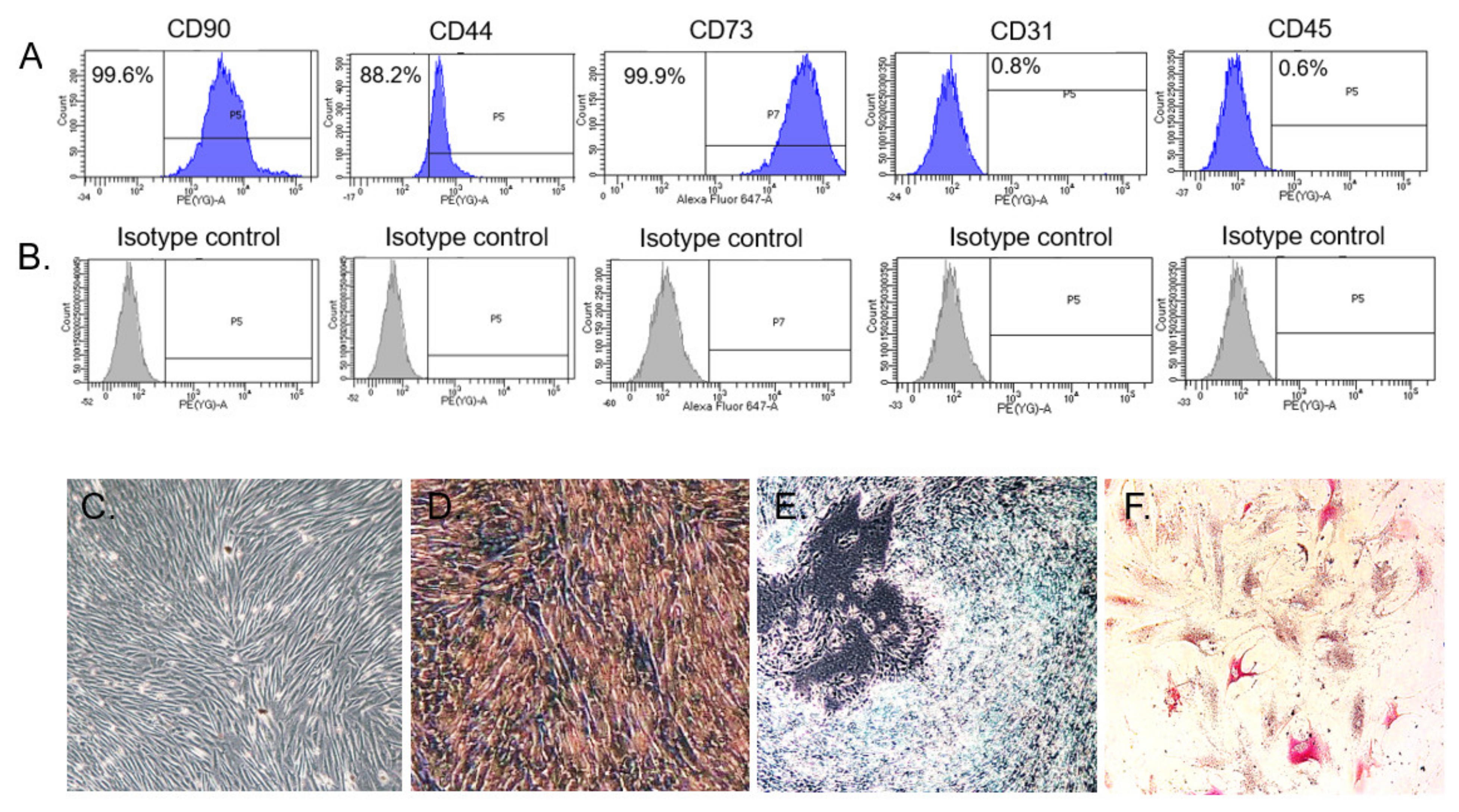
2.3. Flow Cytometry Analysis
2.4. Differentiation Assay
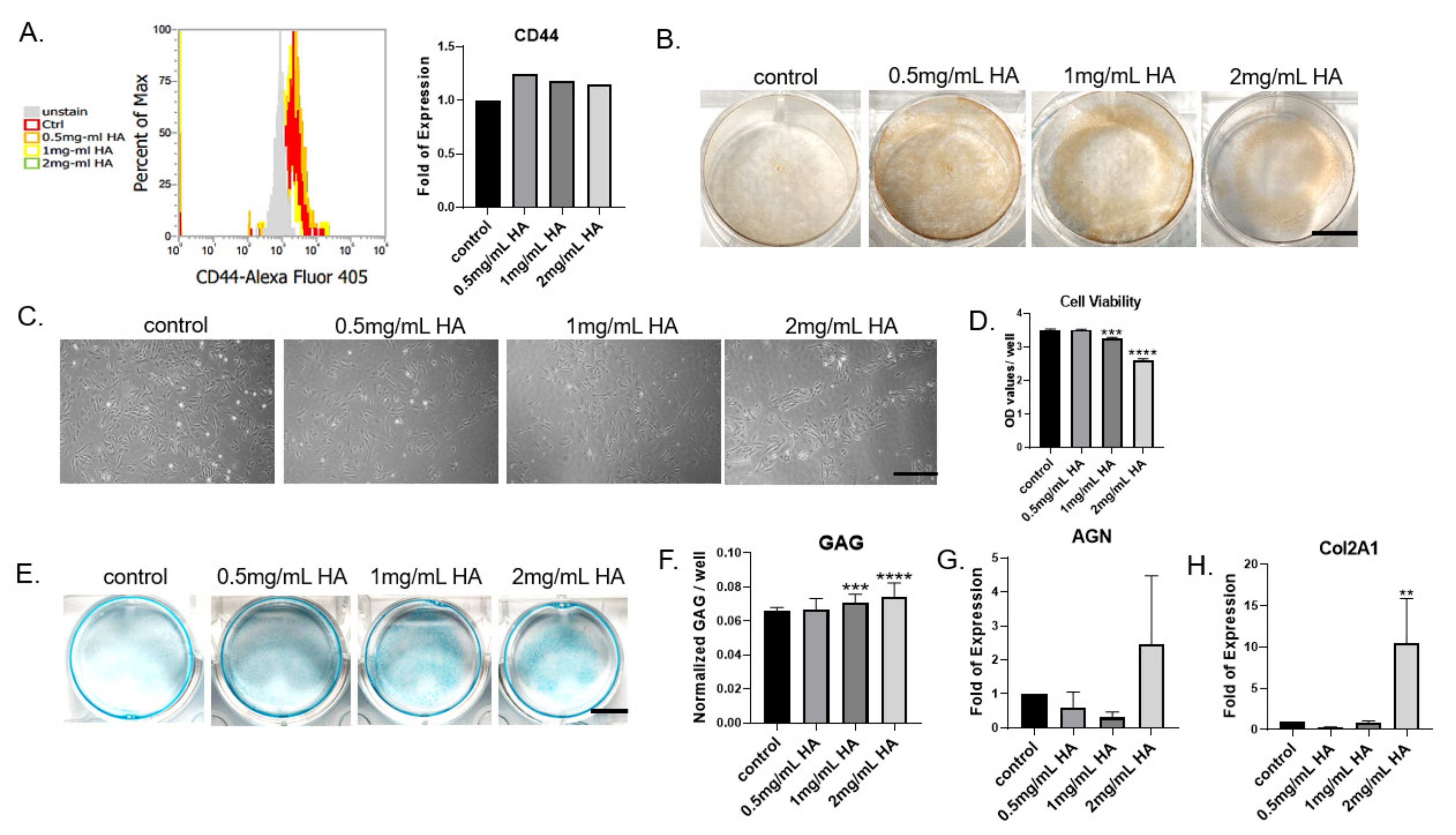
2.5. Effect of HA Treatment on CD44 Expression and Cell Viability
2.6. Effect of HA on BMSCs’ Glycosaminoglycan Synthesis
2.7. Effect of HA on BMSCs’ Chondrogenic Gene Expression
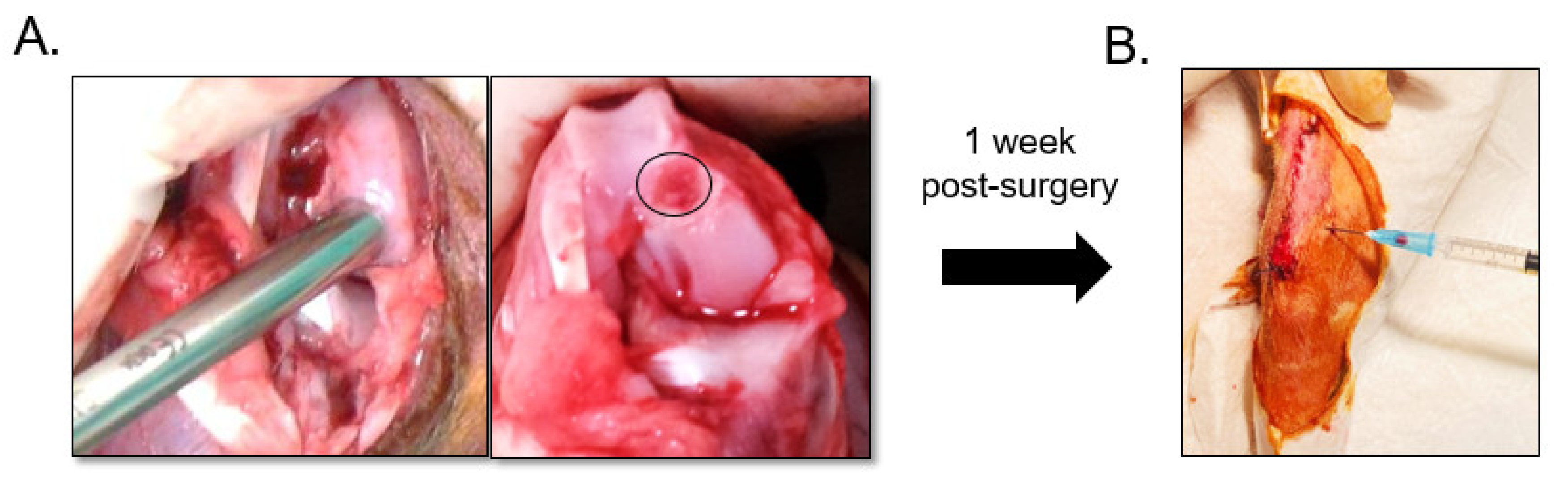
2.8. Rabbit Chondral Defect Model
2.9. In Vivo Intra-Articular Injection of BMSCs and HA
2.10. Macroscopic Analysis
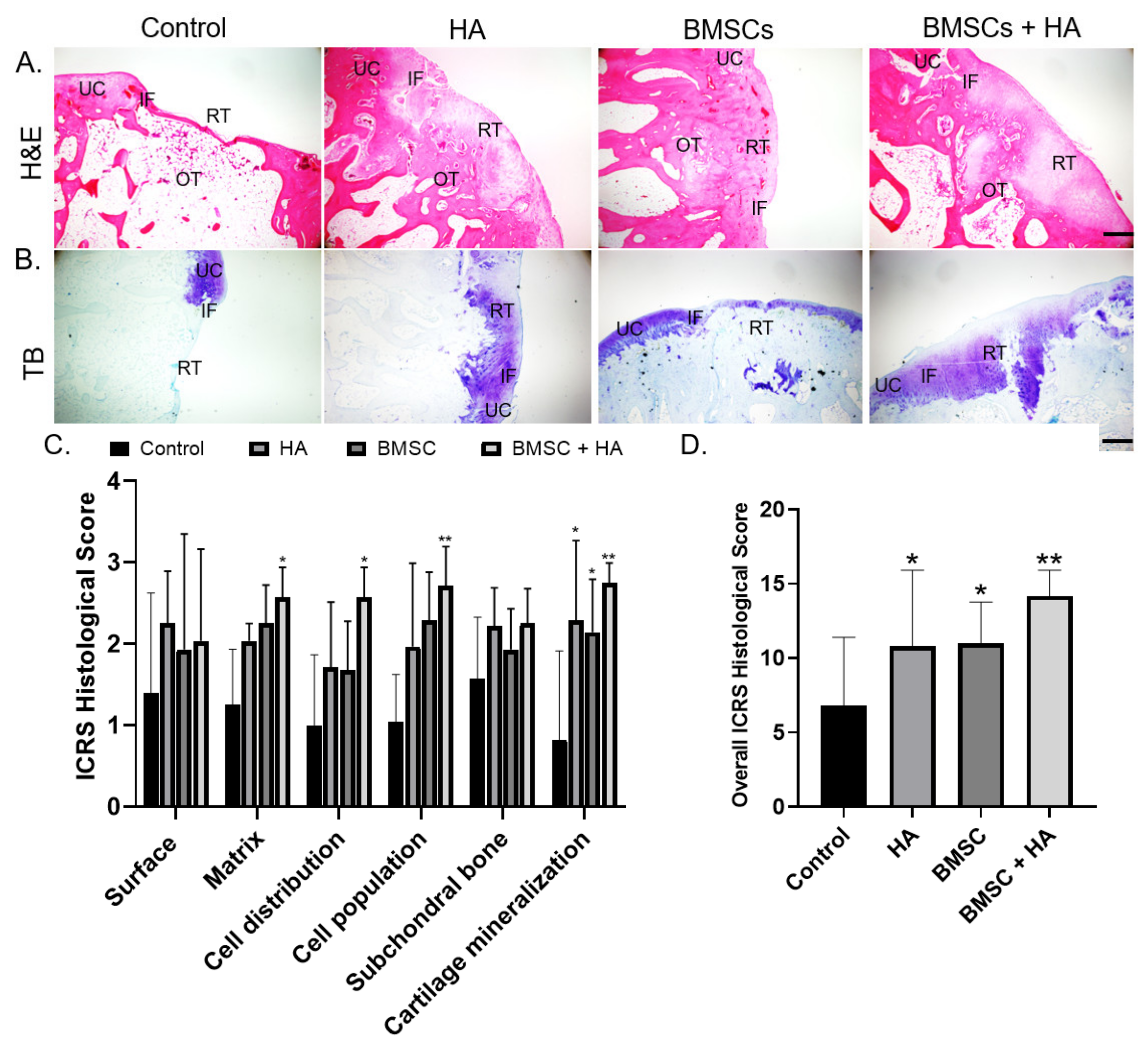
2.11. Histological Analysis
2.12. Statistical Analysis
3. Results
3.1. In Vitro
3.1.1. Characterization of BMSC Surface Marker Identification and Differentiation Assay
3.1.2. Effect of HA on CD44 Expression and Cell Viability
3.1.3. Effect of HA on Cell GAG Expression and Chondrogenic Gene Expression
3.2. In Vivo
3.2.1. Macroscopic Outcome
3.2.2. Histological Evaluation of Defect Healing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buckwalter, J.A.; Mankin, H.J. Articular cartilage: Tissue design and chondrocyte-matrix interactions. Instr. Course Lect. 1998, 47, 477–486. [Google Scholar] [PubMed]
- Brittberg, M.; Lindahl, A.; Nilsson, A.; Ohlsson, C.; Isaksson, O.; Peterson, L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N. Engl. J. Med. 1994, 331, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Brittberg, M.; Winalski, C.S. Evaluation of cartilage injuries and repair. J. Bone Jt. Surg. Am. Vol. 2003, 85-A (Suppl. 2), 58–69. [Google Scholar] [CrossRef] [PubMed]
- Glyn-Jones, S.; Palmer, A.J.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef]
- Chimutengwende-Gordon, M.; Donaldson, J.; Bentley, G. Current solutions for the treatment of chronic articular cartilage defects in the knee. EFORT Open Rev. 2020, 5, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Giri, T.K.; Alexander, A.; Agrawal, M.; Saraf, S.; Saraf, S.; Ajazuddin. Current Status of Stem Cell Therapies in Tissue Repair and Regeneration. Curr. Stem Cell Res. Ther. 2019, 14, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Dewan, A.K.; Gibson, M.A.; Elisseeff, J.H.; Trice, M.E. Evolution of autologous chondrocyte repair and comparison to other cartilage repair techniques. BioMed Res. Int. 2014, 2014, 272481. [Google Scholar] [CrossRef]
- Schenker, H.; Wild, M.; Rath, B.; Tingart, M.; Driessen, A.; Quack, V.; Betsch, M. Current overview of cartilage regeneration procedures. Der Orthopäde 2017, 46, 907–913. [Google Scholar] [CrossRef]
- Welch, T.; Mandelbaum, B.; Tom, M. Autologous Chondrocyte Implantation: Past, Present, and Future. Sports Med. Arthrosc. Rev. 2016, 24, 85–91. [Google Scholar] [CrossRef]
- Benya, P.D.; Shaffer, J.D. Dedifferentiated chondrocytes reexpress the differentiated collagen phenotype when cultured in agarose gels. Cell 1982, 30, 215–224. [Google Scholar] [CrossRef]
- Wong, C.C.; Chiu, L.H.; Lai, W.F.; Tsai, T.T.; Fang, C.L.; Chen, S.C.; Tsai, Y.H. Phenotypic re-expression of near quiescent chondrocytes: The effects of type II collagen and growth factors. J. Biomater. Appl. 2010, 25, 75–95. [Google Scholar] [CrossRef] [PubMed]
- Anz, A.W.; Bapat, A.; Murrell, W.D. Concepts in regenerative medicine: Past, present, and future in articular cartilage treatment. J. Clin. Orthop. Trauma 2016, 7, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baghaban Eslaminejad, M.; Malakooty Poor, E. Mesenchymal stem cells as a potent cell source for articular cartilage regeneration. World J. Stem Cells 2014, 6, 344–354. [Google Scholar] [CrossRef]
- Chamberlain, G.; Fox, J.; Ashton, B.; Middleton, J. Concise review: Mesenchymal stem cells: Their phenotype, differentiation capacity, immunological features, and potential for homing. Stem Cells 2007, 25, 2739–2749. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, K.L.; Wang, J. Cell-based articular cartilage repair: The link between development and regeneration. Osteoarthr. Cartil. 2015, 23, 351–362. [Google Scholar] [CrossRef] [Green Version]
- Hassan, M.; Yazid, M.D.; Yunus, M.H.M.; Chowdhury, S.R.; Lokanathan, Y.; Idrus, R.B.H.; Ng, A.M.H.; Law, J.X. Large-Scale Expansion of Human Mesenchymal Stem Cells. Stem Cells Int. 2020, 2020, 9529465. [Google Scholar] [CrossRef]
- Ogay, V.; Karzhauov, M.; Mukhambetova, A.; Raimagambetov, E.; Batpenov, N. Intra-articular injection of synovium-derived mesenchymal stem cells and hyaluronic acid promote regeneration of massive cartilage defects in rabbits. Central Asian J. Glob. Heal. 2013, 2, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Duan, X.; Fan, Z.; Chen, L.; Xing, F.; Xu, Z.; Chen, Q.; Xiang, Z. Mesenchymal Stem Cells in Combination with Hyaluronic Acid for Articular Cartilage Defects. Sci. Rep. 2018, 8, 9900. [Google Scholar] [CrossRef]
- Yamasaki, S.; Hashimoto, Y.; Takigami, J.; Terai, S.; Mera, H.; Nakamura, H.; Wakitani, S. Effect of the direct injection of bone marrow mesenchymal stem cells in hyaluronic acid and bone marrow stimulation to treat chondral defects in the canine model. Regen. Ther. 2015, 2, 42–48. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, J.A.; Jones, I.A.; Han, B.; Vangsness, C.T., Jr. Intra-articular Mesenchymal Stem Cell Therapy for the Human Joint: A Systematic Review. Am. J. Sports Med. 2018, 46, 3550–3563. [Google Scholar] [CrossRef]
- Nakamura, N.; Yokota, N.; Hattori, M.; Ohtsuru, T.; Otsuji, M.; Lyman, S.; Shimomura, K. Comparative Clinical Outcomes After Intra-articular Injection With Adipose-Derived Cultured Stem Cells or Noncultured Stromal Vascular Fraction for the Treatment of Knee Osteoarthritis: Response. Am. J. Sports Med. 2020, 48, Np19–np20. [Google Scholar] [CrossRef]
- Akmal, M.; Singh, A.; Anand, A.; Kesani, A.; Aslam, N.; Goodship, A.; Bentley, G. The effects of hyaluronic acid on articular chondrocytes. J. Bone Jt. Surgery. Br. Vol. 2005, 87, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- López-Ruiz, E.; Jiménez, G.; Álvarez de Cienfuegos, L.; Antic, C.; Sabata, R.; Marchal, J.A.; Gálvez-Martín, P. Advances of hyaluronic acid in stem cell therapy and tissue engineering, including current clinical trials. Eur. Cell Mater. 2019, 37, 186–213. [Google Scholar] [CrossRef] [PubMed]
- Barbucci, R.; Rappuoli, R.; Borzacchiello, A.; Ambrosio, L. Synthesis, chemical and rheological characterization of new hyaluronic acid-based hydrogels. J. Biomater. Sci. Polym. Ed. 2000, 11, 383–399. [Google Scholar] [CrossRef]
- Van den Borne, M.P.; Raijmakers, N.J.; Vanlauwe, J.; Victor, J.; De Jong, S.N.; Bellemans, J.; Saris, D.B. International Cartilage Repair Society (ICRS) and Oswestry macroscopic cartilage evaluation scores validated for use in Autologous Chondrocyte Implantation (ACI) and microfracture. Osteoarthr. Cartil. 2007, 15, 1397–1402. [Google Scholar] [CrossRef] [Green Version]
- Bergholt, N.L.; Lysdahl, H.; Lind, M.; Foldager, C.B. A Standardized Method of Applying Toluidine Blue Metachromatic Staining for Assessment of Chondrogenesis. Cartilage 2019, 10, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Mainil-Varlet, P.; Aigner, T.; Brittberg, M.; Bullough, P.; Hollander, A.; Hunziker, E.; Kandel, R.; Nehrer, S.; Pritzker, K.; Roberts, S.; et al. Histological assessment of cartilage repair: A report by the Histology Endpoint Committee of the International Cartilage Repair Society (ICRS). J. Bone Jt. Surg. Am. Vol. 2003, 85-A (Suppl. 2), 45–57. [Google Scholar] [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Amann, E.; Wolff, P.; Breel, E.; Van Griensven, M.; Balmayor, E.R. Hyaluronic acid facilitates chondrogenesis and matrix deposition of human adipose derived mesenchymal stem cells and human chondrocytes co-cultures. Acta Biomater. 2017, 52, 130–144. [Google Scholar] [CrossRef]
- Enomoto, T.; Akagi, R.; Ogawa, Y.; Yamaguchi, S.; Hoshi, H.; Sasaki, T.; Sato, Y.; Nakagawa, R.; Kimura, S.; Ohtori, S.; et al. Timing of Intra-Articular Injection of Synovial Mesenchymal Stem Cells Affects Cartilage Restoration in a Partial Thickness Cartilage Defect Model in Rats. Cartilage 2020, 11, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.B.; Hui, J.H.; Song, I.C.; Ardany, L.; Lee, E.H. Injectable mesenchymal stem cell therapy for large cartilage defects—A porcine model. Stem Cells 2007, 25, 2964–2971. [Google Scholar] [CrossRef] [Green Version]
- McIlwraith, C.W.; Frisbie, D.D.; Rodkey, W.G.; Kisiday, J.D.; Werpy, N.M.; Kawcak, C.E.; Steadman, J.R. Evaluation of intra-articular mesenchymal stem cells to augment healing of microfractured chondral defects. Arthroscopy 2011, 27, 1552–1561. [Google Scholar] [CrossRef] [PubMed]
- Satué, M.; Schüler, C.; Ginner, N.; Erben, R.G. Intra-articularly injected mesenchymal stem cells promote cartilage regeneration, but do not permanently engraft in distant organs. Sci. Rep. 2019, 9, 10153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, H.Y.; Karunanithi, P.; Loo, W.C.; Naveen, S.; Chen, H.; Hussin, P.; Chan, L.; Kamarul, T. The effects of staged intra-articular injection of cultured autologous mesenchymal stromal cells on the repair of damaged cartilage: A pilot study in caprine model. Arthritis Res. Ther. 2013, 15, R129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dicker, K.T.; Gurski, L.A.; Pradhan-Bhatt, S.; Witt, R.L.; Farach-Carson, M.C.; Jia, X. Hyaluronan: A simple polysaccharide with diverse biological functions. Acta Biomater. 2014, 10, 1558–1570. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.A.; Erickson, B.J.; Saltzman, B.M.; Mascarenhas, R.; Bach, B.R., Jr.; Cole, B.J.; Verma, N.N. Is Local Viscosupplementation Injection Clinically Superior to Other Therapies in the Treatment of Osteoarthritis of the Knee: A Systematic Review of Overlapping Meta-analyses. Arthroscopy 2015, 31, 2036–2045.e14. [Google Scholar] [CrossRef] [PubMed]
- Concoff, A.; Sancheti, P.; Niazi, F.; Shaw, P.; Rosen, J. The efficacy of multiple versus single hyaluronic acid injections: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 542. [Google Scholar] [CrossRef] [Green Version]
- Yoshioka, M.; Shimizu, C.; Harwood, F.L.; Coutts, R.D.; Amiel, D. The effects of hyaluronan during the development of osteoarthritis. Osteoarthr. Cartil. 1997, 5, 251–260. [Google Scholar] [CrossRef] [Green Version]
- Maniwa, S.; Ochi, M.; Motomura, T.; Nishikori, T.; Chen, J.; Naora, H. Effects of hyaluronic acid and basic fibroblast growth factor on motility of chondrocytes and synovial cells in culture. Acta Orthop. Scand. 2001, 72, 299–303. [Google Scholar] [CrossRef]
- Liu, S.; Zhang, Q.S.; Hester, W.; O’Brien, M.J.; Savoie, F.H.; You, Z. Hyaluronan protects bovine articular chondrocytes against cell death induced by bupivacaine at supraphysiologic temperatures. Am. J. Sports Med. 2012, 40, 1375–1383. [Google Scholar] [CrossRef]
- Grishko, V.; Xu, M.; Ho, R.; Mates, A.; Watson, S.; Kim, J.T.; Wilson, G.L.; Pearsall, A.W., IV. Effects of hyaluronic acid on mitochondrial function and mitochondria-driven apoptosis following oxidative stress in human chondrocytes. J. Biol. Chem. 2009, 284, 9132–9139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knudson, W.; Casey, B.; Nishida, Y.; Eger, W.; Kuettner, K.E.; Knudson, C.B. Hyaluronan oligosaccharides perturb cartilage matrix homeostasis and induce chondrocytic chondrolysis. Arthritis Rheum. 2000, 43, 1165–1174. [Google Scholar] [CrossRef]
- Sackstein, R.; Merzaban, J.S.; Cain, D.W.; Dagia, N.M.; Spencer, J.A.; Lin, C.P.; Wohlgemuth, R. Ex vivo glycan engineering of CD44 programs human multipotent mesenchymal stromal cell trafficking to bone. Nat. Med. 2008, 14, 181–187. [Google Scholar] [CrossRef]
- Marquass, B.; Schulz, R.; Hepp, P.; Zscharnack, M.; Aigner, T.; Schmidt, S.; Stein, F.; Richter, R.; Osterhoff, G.; Aust, G.; et al. Matrix-associated implantation of predifferentiated mesenchymal stem cells versus articular chondrocytes: In Vivo results of cartilage repair after 1 year. Am. J. Sports Med. 2011, 39, 1401–1412. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Primer Sequence | Size (Base Pair) |
|---|---|---|
| Col2a1 | F:GCACCCATGGACATTGGAGGG R:GACACGGAGTAGCACCATCG | 366 |
| AGN | F:GAGGAGATGGAGGGTGAGGTCTTT R:CTTCGCCTGTGTAGCAGCTG | 313 |
| β-ACTIN | F:CAACTGGGACGACATGGAGAAG R:TGAACGTCTCGAACATGATCTG | 152 |
| Features | Grade |
|---|---|
| Degree of defect repair | |
| In level with surrounding cartilage | 4 |
| 75% repair of defect depth | 3 |
| 50% repair of defect depth | 2 |
| 25% repair of defect depth | 1 |
| 0% repair of defect depth | 0 |
| Integration to border zone | |
| Complete integration with surrounding cartilage | 4 |
| Demarcating border < 1 mm | 3 |
| 3/4th of graft integrated, 1/4th with a notable border > 1 mm width | 2 |
| 1/2 of graft integrated with surrounding cartilage, 1/2 with a notable border > 1 mm | 1 |
| From no contact to 1/4th of graft integrated with surrounding cartilage | 0 |
| Macroscopic appearance | |
| Intact smooth surface | 4 |
| Fibrillated surface | 3 |
| Small, scattered fissures or cracks | 2 |
| Several small or few but large fissures | 1 |
| Total degeneration of grafted area | 0 |
| Overall repair assessment | |
| Grade I: normal | 12 |
| Grade II: nearly normal | 11–8 |
| Grade III: abnormal | 7–4 |
| Grade IV: severely abnormal | 3–1 |
| Feature | Score | |
|---|---|---|
| I. Surface | ||
| Smooth/continuous | 3 | |
| Discontinuities/irregularities | 0 | |
| II. Matrix | ||
| Hyaline | 3 | |
| Mixture: hyaline/fibrocartilage | 2 | |
| Fibrocartilage | 1 | |
| Fibrous tissue | 0 | |
| III. Cell distribution | ||
| Columnar | 3 | |
| Mixed: columnar/cluster | 2 | |
| Cluster | 1 | |
| Individual cells/disorganized | 0 | |
| IV. Cell population | ||
| Predominantly viable | 3 | |
| Partially viable | 1 | |
| <10% viable | 0 | |
| V. Subchondral bone | ||
| Normal | 3 | |
| Increased remodeling | 2 | |
| Bone necrosis/granulation tissue | 1 | |
| Detached/fracture/cells at base | 0 | |
| VI. Cartilage mineralization (calcified cartilage) | ||
| Normal | 3 | |
| Abnormal/inappropriate | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, C.-C.; Sheu, S.-D.; Chung, P.-C.; Yeh, Y.-Y.; Chen, C.-H.; Chang, Y.-W.; Kuo, T.-F. Hyaluronic Acid Supplement as a Chondrogenic Adjuvant in Promoting the Therapeutic Efficacy of Stem Cell Therapy in Cartilage Healing. Pharmaceutics 2021, 13, 432. https://doi.org/10.3390/pharmaceutics13030432
Wong C-C, Sheu S-D, Chung P-C, Yeh Y-Y, Chen C-H, Chang Y-W, Kuo T-F. Hyaluronic Acid Supplement as a Chondrogenic Adjuvant in Promoting the Therapeutic Efficacy of Stem Cell Therapy in Cartilage Healing. Pharmaceutics. 2021; 13(3):432. https://doi.org/10.3390/pharmaceutics13030432
Chicago/Turabian StyleWong, Chin-Chean, Shi-Da Sheu, Pei-Chun Chung, Yi-Yen Yeh, Chih-Hwa Chen, Yen-Wei Chang, and Tzong-Fu Kuo. 2021. "Hyaluronic Acid Supplement as a Chondrogenic Adjuvant in Promoting the Therapeutic Efficacy of Stem Cell Therapy in Cartilage Healing" Pharmaceutics 13, no. 3: 432. https://doi.org/10.3390/pharmaceutics13030432
APA StyleWong, C. -C., Sheu, S. -D., Chung, P. -C., Yeh, Y. -Y., Chen, C. -H., Chang, Y. -W., & Kuo, T. -F. (2021). Hyaluronic Acid Supplement as a Chondrogenic Adjuvant in Promoting the Therapeutic Efficacy of Stem Cell Therapy in Cartilage Healing. Pharmaceutics, 13(3), 432. https://doi.org/10.3390/pharmaceutics13030432