
Long-Term Oral Treatment with Non-Hypoglycemic Dose of Glibenclamide Reduces Diabetic Retinopathy Damage in the Goto-KakizakiRat Model


Abstract
:1. Introduction
2. Material and Methods
2.1. Animals and Animal Model; Ethical Concerns
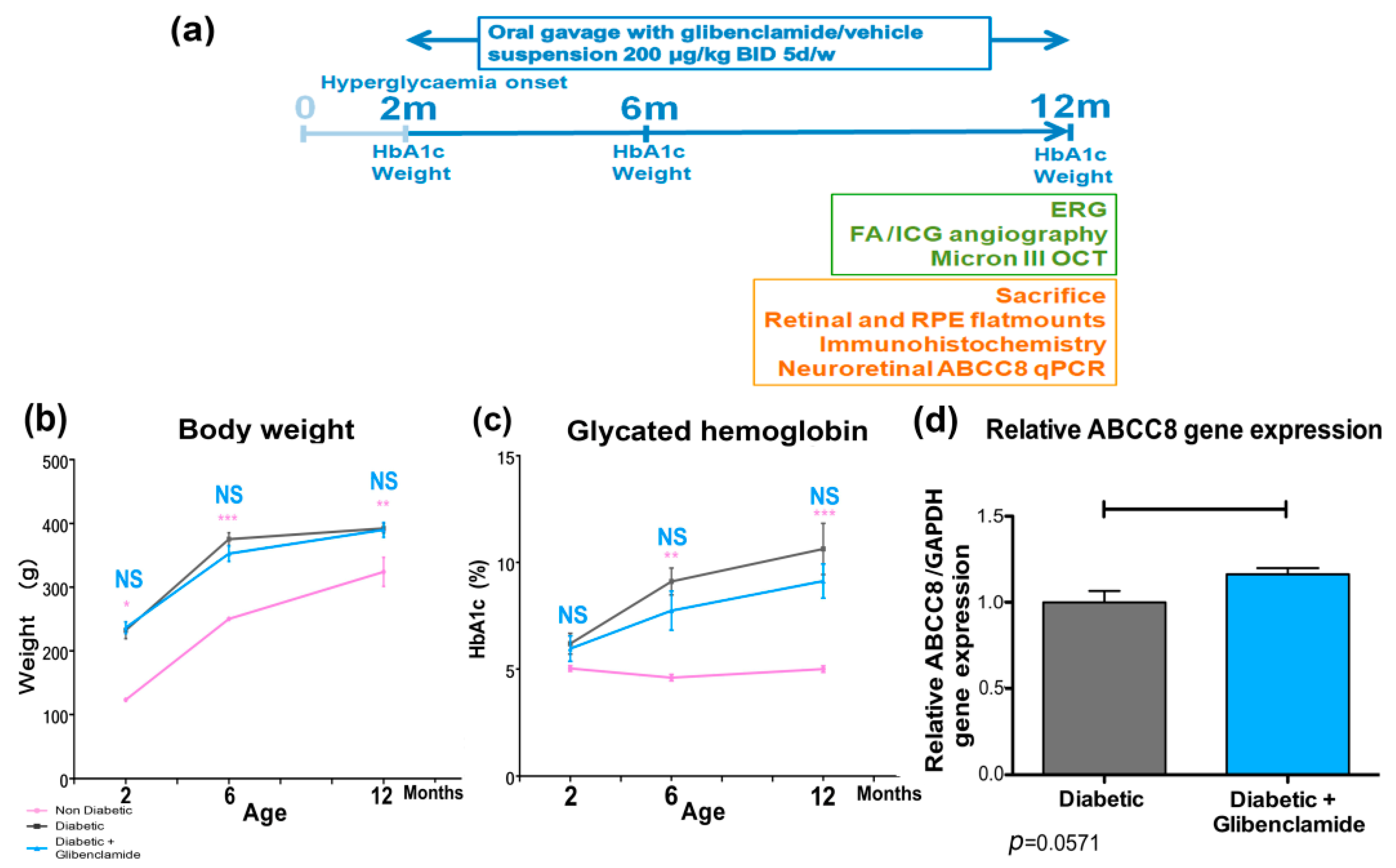
2.2. Long-Term Oral Glibenclamide Treatment
2.3. qPCR–ABCC8 Neuroretinal Expression
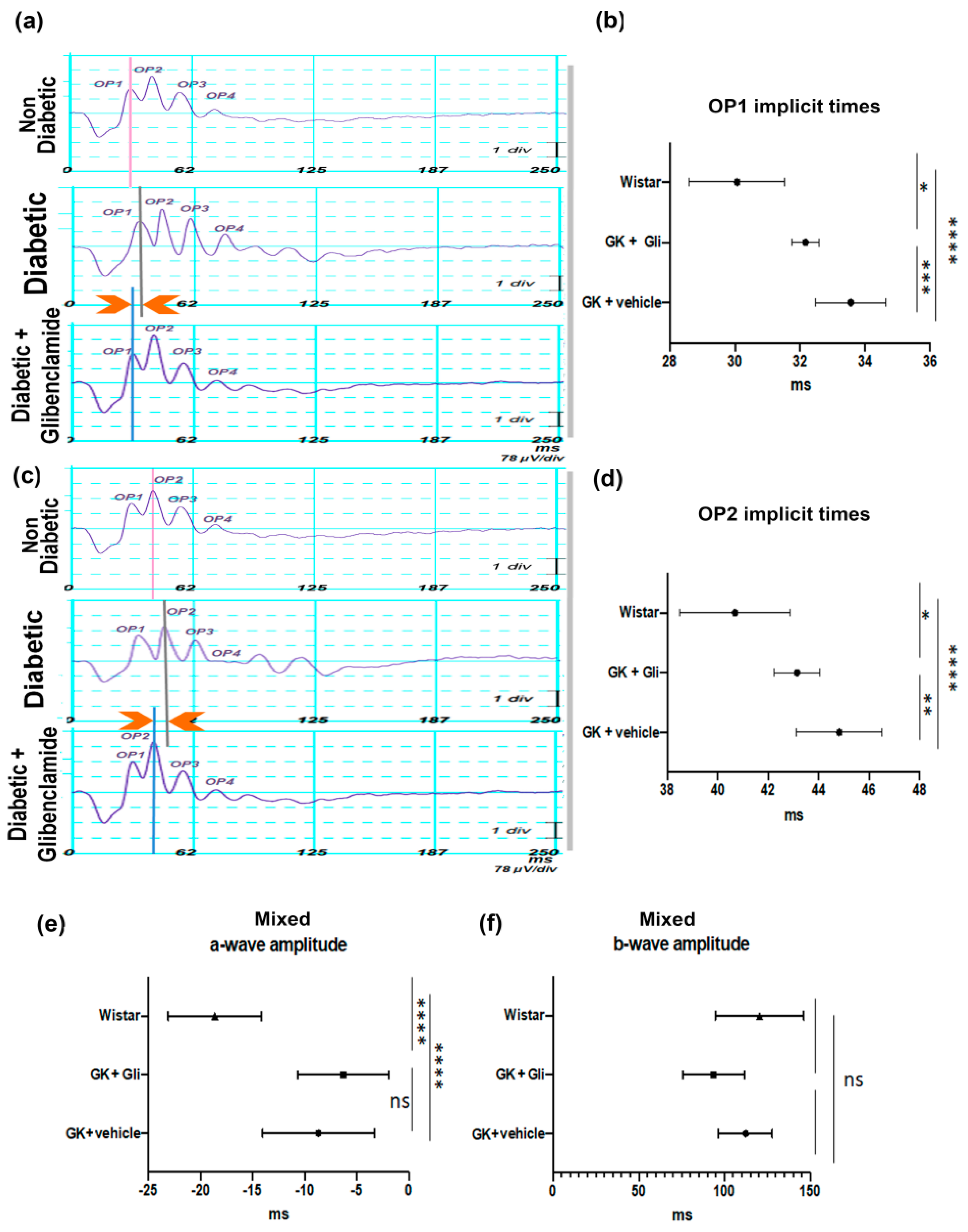
2.4. Electroretinography (ERG)—Visual Function Evaluation
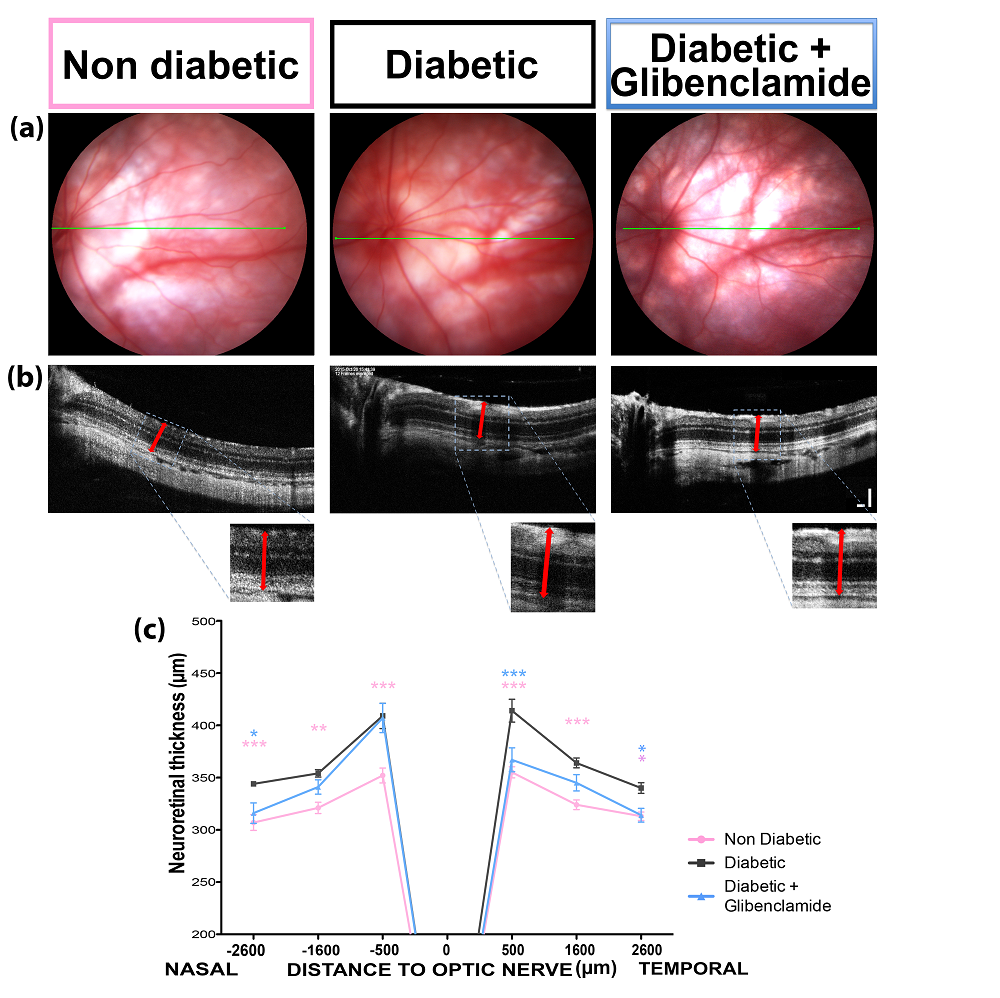
2.5. Fundoscopy, Optical Coherence Tomography (OCT)—Neuroretinal Thickness Measurement
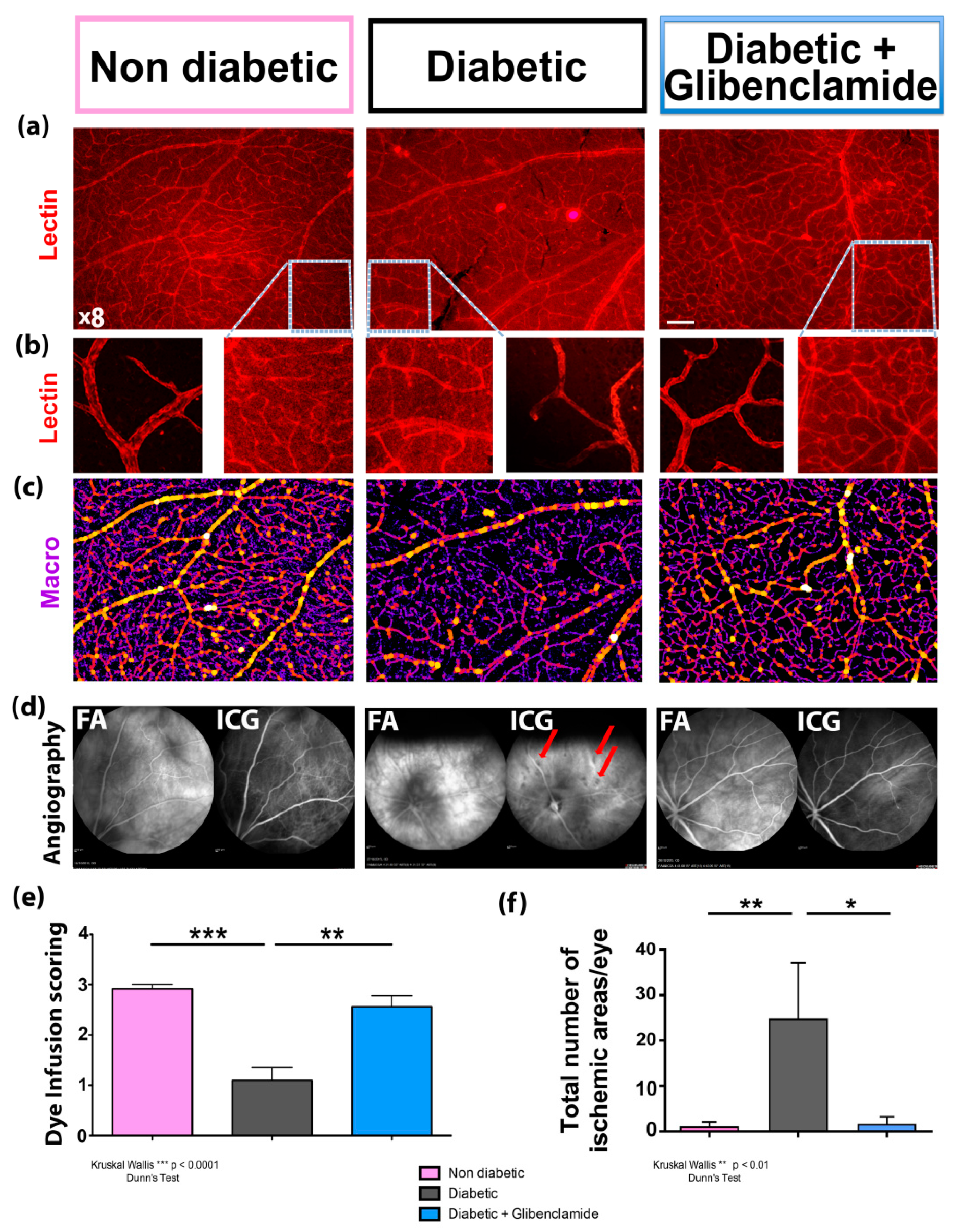
2.6. Fluorescein and Indocyanin Green Angiographies—Retinal and Choroidal Vascularization Imaging and Evaluation of Dye Vascular Infusion
2.7. Flatmounts, Immunohistochemistry and Home-Made Macro Analysis for Evaluation of Capillary Percentage among Retinal Vessels and RPE cell Areas Analysis
2.8. Statistics
3. Results
3.1. Long-Term Oral Glibenclamide at 200 µg/kg BID did Not Influence Body Weight and Glycemic Control in GK Rats–qPCR ABCC8 Expression
3.2. Long-Term Non-Hypoglycemic Oral Glibenclamide Treatment Improves Retinal Function in GK Rats
3.3. Long-Term Non-Hypoglycemic Oral Glibenclamide Treatment Reduces Retinal Edema in GK Rats
3.4. Long-Term Non-Hypoglycemic Oral Glibenclamide Improves Retinal Vascular Perfusion in Diabetic Goto-Kakizaki Rats
3.5. Long-Term Non-Hypoglycemic Oral Glibenclamide Prevented Outer Retinal Barrier Damages
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nentwich, M.M.; Ulbig, M.W. Diabetic Retinopathy—Ocular Complications of Diabetes Mellitus. World J. Diabetes 2015, 6, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Soni, D.; Sagar, P.; Takkar, B. Diabetic Retinal Neurodegeneration as a Form of Diabetic Retinopathy. Int. Ophthalmol. 2021. [CrossRef]
- Damian, I.; Nicoară, S.D. Correlations between Retinal Arterial Morphometric Parameters and Neurodegeneration in Patients with Type 2 Diabetes Mellitus with No or Mild Diabetic Retinopathy. Medicina 2021, 57, 244. [Google Scholar] [CrossRef]
- Li, Q.; Zemel, E.; Miller, B.; Perlman, I. Early Retinal Damage in Experimental Diabetes: Electroretinographical and Morphological Observations. Exp. Eye Res. 2002, 74, 615–625. [Google Scholar] [CrossRef]
- Tzekov, R.; Arden, G.B. The Electroretinogram in Diabetic Retinopathy. Surv. Ophthalmol. 1999, 44, 53–60. [Google Scholar] [CrossRef]
- Ciulla, T.A.; Pollack, J.S.; Williams, D.F. Visual Acuity Outcomes and Anti-VEGF Therapy Intensity in Diabetic Macular Oedema: A Real-World Analysis of 28 658 Patient Eyes. Br. J. Ophthalmol. 2021, 105, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Rittiphairoj, T.; Mir, T.A.; Li, T.; Virgili, G. Intravitreal Steroids for Macular Edema in Diabetes. Cochrane Database Syst. Rev. 2020, 11, CD005656. [Google Scholar] [CrossRef]
- Sharma, M.; Nazareth, I.; Petersen, I. Trends in Incidence, Prevalence and Prescribing in Type 2 Diabetes Mellitus between 2000 and 2013 in Primary Care: A Retrospective Cohort Study. BMJ Open 2016, 6, e010210. [Google Scholar] [CrossRef]
- Kurland, D.B.; Gerzanich, V.; Karimy, J.K.; Woo, S.K.; Vennekens, R.; Freichel, M.; Nilius, B.; Bryan, J.; Simard, J.M. The Sur1-Trpm4 Channel Regulates NOS2 Transcription in TLR4-Activated Microglia. J. Neuroinflamm. 2016, 13, 130. [Google Scholar] [CrossRef]
- Kunte, H.; Schmidt, S.; Eliasziw, M.; del Zoppo, G.J.; Simard, J.M.; Masuhr, F.; Weih, M.; Dirnagl, U. Sulfonylureas Improve Outcome in Patients with Type 2 Diabetes and Acute Ischemic Stroke. Stroke 2007, 38, 2526–2530. [Google Scholar] [CrossRef] [Green Version]
- Sheth, K.N.; Simard, J.M.; Elm, J.; Kronenberg, G.; Kunte, H.; Kimberly, W.T. Human Data Supporting Glyburide in Ischemic Stroke. Acta Neurochir. Suppl. 2016, 121, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Jha, R.M.; Mondello, S.; Bramlett, H.M.; Dixon, C.E.; Shear, D.A.; Dietrich, W.D.; Wang, K.K.W.; Yang, Z.; Hayes, R.L.; Poloyac, S.M.; et al. Glibenclamide Treatment in Traumatic Brain Injury: Operation Brain Trauma Therapy. J. Neurotrauma 2021, 38, 628–645. [Google Scholar] [CrossRef]
- Igarashi, T.; Sastre, C.; Wolcott, Z.; Kimberly, W.T. Continuous Glibenclamide Prevents Hemorrhagic Transformation in a Rodent Model of Severe Ischemia-Reperfusion. J. Stroke Cereb. Dis. 2021, 30, 105595. [Google Scholar] [CrossRef]
- Caffes, N.; Kurland, D.B.; Gerzanich, V.; Simard, J.M. Glibenclamide for the Treatment of Ischemic and Hemorrhagic Stroke. Int. J. Mol. Sci. 2015, 16, 4973–4984. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Chang, Y.; He, Y.; Lyu, C.; Li, H.; Zhu, J.; Liu, K.; Hu, Y.; Huang, K.; Pan, S. Glimepiride and Glibenclamide Have Comparable Efficacy in Treating Acute Ischemic Stroke in Mice. Neuropharmacology 2020, 162, 107845. [Google Scholar] [CrossRef]
- Wen, L.; Huang, B.; Tu, R.; Wan, K.; Zhang, H.; Zhang, X. Effectiveness and Safety of Glibenclamide for Stroke: Protocol for a Systematic Review and Meta-Analysis. BMJ Open 2021, 11, e043585. [Google Scholar] [CrossRef]
- Beltrand, J.; Elie, C.; Busiah, K.; Fournier, E.; Boddaert, N.; Bahi-Buisson, N.; Vera, M.; Bui-Quoc, E.; Ingster-Moati, I.; Berdugo, M.; et al. Sulfonylurea therapy benefits neurological and psychomotor functions in patients with neonatal diabetes owing to potassium channel mutations. Diabetes Care 2015, 38, 2033–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltrand, J.; Busiah, K.; Vaivre-Douret, L.; Fauret, A.L.; Berdugo, M.; Cavé, H.; Polak, M. Neonatal Diabetes Mellitus. Front. Pediatr. 2020, 8, 540718, Published 30 September 2020. [Google Scholar] [CrossRef]
- Zhang, Q.-Q.; Li, W.-S.; Liu, Z.; Zhang, H.-L.; Ba, Y.-G.; Zhang, R.-X. Metformin Therapy and Cognitive Dysfunction in Patients with Type 2 Diabetes: A Meta-Analysis and Systematic Review. Medicine (Baltim.) 2020, 99, e19378. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.D.; Guo, Y.; Bernstein, S.L. SUR1-Associated Mechanisms Are Not Involved in Ischemic Optic Neuropathy 1 Day Post-Injury. PLoS ONE 2016, 11, e0148855. [Google Scholar] [CrossRef]
- Berdugo, M.; Delaunay, K.; Naud, M.-C.; Guegan, J.; Moulin, A.; Savoldelli, M.; Picard, E.; Radet, L.; Jonet, L.; Djerada, Z.; et al. The Antidiabetic Drug Glibenclamide Exerts Direct Retinal Neuroprotection. Transl. Res. 2020. [Google Scholar] [CrossRef]
- Ravera, S.; Caicci, F.; Degan, P.; Maggi, D.; Manni, L.; Puddu, A.; Nicolò, M.; Traverso, C.E.; Panfoli, I. Inhibitory Action of Antidiabetic Drugs on the Free Radical Production by the Rod Outer Segment Ectopic Aerobic Metabolism. Antioxidants (Basel) 2020, 9, 1133. [Google Scholar] [CrossRef]
- Díaz, A.; López-Grueso, R.; Gambini, J.; Monleón, D.; Mas-Bargues, C.; Abdelaziz, K.M.; Viña, J.; Borrás, C. Sex Differences in Age-Associated Type 2 Diabetes in Rats-Role of Estrogens and Oxidative Stress. Oxidative Med. Cell. Longev. 2019, 6734836. [Google Scholar] [CrossRef] [PubMed]
- Portha, B. Anomalies programmées de la sécrétion d’insuline dans le diabète de type 2: Le paradigme du rat GK [Transmitted beta-cell dysfunction as a cause for type 2-diabetes]. Med. Sci. (Paris) 2003, 19, 847–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakizaki, M.; Masaki, N. Spontaneous diabetes produced by selective breeding of normal Wistar rats. Proc. Jpn. Acad. 1975, 51, 85–90. [Google Scholar]
- Miyamoto, K.; Ogura, K.; Nishiwaki, H.; Matsuda, N.; Honda, Y.; Kato, S.; Ishida, H.; Seino, Y. Evaluation of retinal microcirculatory alterations in the Goto-Kakizaki rat. A spontaneous model of non-insulin-dependent diabetes. Investig. Ophthalmol. Vis. Sci. 1996, 37, 898–905. [Google Scholar]
- Campos, A.; Martins, J.; Campos, E.J.; Silva, R.; Ambrósio, A.F. Choroidal and retinal structural, cellular and vascular changes in a rat model of Type 2 diabetes. Biomed. Pharmacother. Biomed. Pharmacother. 2020, 132, 110811. [Google Scholar] [CrossRef] [PubMed]
- Omri, S.; Behar-Cohen, F.; Rothschild, P.R.; Gélizé, E.; Jonet, L.; Jeanny, J.C.; Omri, B.; Crisanti, P. PKCzeta mediates breakdown of outer blood-retinal barriers in diabetic retinopathy. PLoS ONE 2013, 8, e81600. [Google Scholar] [CrossRef] [Green Version]
- Rothschild, P.R.; Salah, S.; Berdugo, M.; Gelize, E.; Delaunay, K.; Naud, M.C.; Klein, C.; Moulin, A.; Savoldelli, M.; Bergin, C.; et al. ROCK-1 Mediates Diabetes-Induced Retinal Pigment Epithelial and Endothelial Cell Blebbing: Contribution to Diabetic Retinopathy. Sci. Rep. 2017, 7, 8834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hachana, S.; Pouliot, M.; Couture, R.; Vaucher, E. Diabetes-Induced Inflammation and Vascular Alterations in the Goto–Kakizaki Rat Retina. Curr. Eye Res. 2020. [Google Scholar] [CrossRef]
- Wang, W.; Liu, S.; Qiu, Z.; He, M.; Wang, L.; Li, Y.; Huang, W. Choroidal Thickness in Diabetes and Diabetic Retinopathy: A Swept Source OCT Study. Investig. Ophthalmol. Vis. Sci. 2020, 61, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omri, S.; Behar-Cohen, F.; de Kozak, Y.; Sennlaub, F.; Verissimo, M.L.; Jonet, L.; Savoldelli, M.; Omri, B.; Crisanti, P. Microglia/macrophages migrate through retinal epithelium barrier by a transcellular route in diabetic retinopathy: Role of PKCzeta in the Goto Kakizaki rat model. Am. J. Pathol. 2011, 179, 942. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.S.; Feola, A.; Motz, C.T.; Ottensmeyer, A.L.; Chesler, K.C.; Dunn, R.; Thulé, P.M.; Pardue, M.T. Retinal Deficits Precede Cognitive and Motor Deficits in a Rat Model of Type II Diabetes. Investig. Ophthalmol. Vis. Sci. 2019, 60, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Weymouth, A.E.; Vingrys, A.J. electroretinography: Methods for extraction and interpretation of rod and cone responses. Prog. Retin. Eye Res. 2007, 27, 1–44. [Google Scholar] [CrossRef] [PubMed]
- Pardue, M.T.; Barnes, C.S.; Kim, M.K.; Aung, M.H.; Amarnath, R.; Olson, D.E.; Thulé, P.M. Rodent Hyperglycemia-Induced Inner Retinal Deficits are Mirrored in Human Diabetes. Trans. Vis. Sci. Tech. 2014, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Hancock, H.A.; Kraft, T.W. Oscillatory potential analysis and ERGs of normal and diabetic rats. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1002–1008. [Google Scholar] [CrossRef] [Green Version]
- Daruich, A.; Matet, A.; Moulin, A.; Kowalczuk, L.; Nicolas, M.; Sellam, A.; Rothschild, P.R.; Omri, S.; Gélizé, E.; Jonet, L.; et al. Mechanisms of macular edema: Beyond the surface. Prog. Retin. Eye Res. 2018, 63, 20–68. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Xu, Y.; Xie, P.; Cheng, H.; Song, Q.; Su, T.; Yuan, S.; Liu, Q. Retinal Neurodegeneration in db/db Mice at the Early Period of Diabetes. J. Ophthalmol. 2015, 757412. [Google Scholar] [CrossRef]
- Tanaka, Y.; Takagi, R.; Ohta, T.; Sasase, T.; Kobayashi, M.; Toyoda, F.; Shimmura, M.; Kinoshita, N.; Takano, H.; Kakehashi, A. Pathological Features of Diabetic Retinopathy in Spontaneously Diabetic Torii Fatty Rats. J. Diabetes Res. 2019, 8724818. [Google Scholar] [CrossRef] [Green Version]
- Griepp, D.W.; Lee, J.; Moawad, C.M.; Davati, C.; Runnels, J.; Fiani, B. BIIB093 (Intravenous Glibenclamide) for the Prevention of Severe Cerebral Edema. Surg. Neurol. Int. 2021, 12, 80. [Google Scholar] [CrossRef]
- Zhao, J.; Yang, F.; Song, C.; Li, L.; Yang, X.; Wang, X.; Yu, L.; Guo, J.; Wang, K.; Fu, F.; et al. Glibenclamide Advantage in Treating Edema After Intracerebral Hemorrhage (GATE-ICH): Study Protocol for a Multicenter Randomized, Controlled, Assessor-Blinded Trial. Front. Neurol. 2021, 12, 656520. [Google Scholar] [CrossRef] [PubMed]
- Simard, J.M.; Chen, M.; Tarasov, K.V.; Bhatta, S.; Ivanova, S.; Melnitchenko, L.; Tsymbalyuk, N.; West, G.A.; Gerzanich, V. Newly Expressed SUR1-Regulated NC(Ca-ATP) Channel Mediates Cerebral Edema after Ischemic Stroke. Nat. Med. 2006, 12, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Lin, X.; Zhang, S.; Xiu, H.; Pan, C.; Cui, W. A Protective Role of Glibenclamide in Inflammation-Associated Injury. Mediat. Inflamm. 2017, 2017, 3578702. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; You, J.; Yao, Y.; Xie, M. High Glucose Induces Pyroptosis of Retinal Microglia through NLPR3 Inflammasome Signaling. Arq. Bras. Oftalmol. 2021, 84, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Chen, L.; Yao, G.-M.; Yan, H.-L.; Wang, L. Effects of Quercetin on Diabetic Retinopathy and Its Association with NLRP3 Inflammasome and Autophagy. Int. J. Ophthalmol. 2021, 14, 42–49. [Google Scholar] [CrossRef]
- Louie, H.H.; Shome, A.; Kuo, C.Y.; Rupenthal, I.D.; Green, C.R.; Mugisho, O.O. Connexin43 Hemichannel Block Inhibits NLRP3 Inflammasome Activation in a Human Retinal Explant Model of Diabetic Retinopathy. Exp. Eye Res. 2021, 202, 108384. [Google Scholar] [CrossRef]
- Rabbani, S.I.; Devi, K.; Khanam, S. Protective role of glibenclamide against nicotinamide-streptozotocin induced nuclear damage in diabetic Wistar rats. J. Pharm. Pharm. 2010, 1, 18–23. [Google Scholar]
- Ladrière, L.; Malaisse-Lagae, F.; Fuhlendorff, J.; Malaisse, W.J. Repaglinide, glibenclamide and glimepiride administration to normal and hereditarily diabetic rats. Eur. J. Pharmacol. 1997, 335, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, Y.; Miura, K.; Takesue, K.; Mine, T.; Wada, R.; Uchida, Y.; Ito, S.; Yagihashi, S. Decreased blood glucose excursion by nateglinide ameliorated neuropathic changes in Goto-Kakizaki rats, an animal model of non-obese type 2 diabetes. Metabolism 2002, 51, 1452–1457. [Google Scholar] [CrossRef]
- Pandarekandy, S.T.; Sreejesh, P.G.; Thampi, B.S.H.; Sreekumaran, E. Hypoglycaemic Effect of Glibenclamide: A Critical Study on the Basis of Creatinine and Lipid Peroxidation Status of Streptozotocin-induced Diabetic Rat. Indian J. Pharm. Sci. 2017, 79. [Google Scholar] [CrossRef]
- Blitzer, A.L.; Ham, S.A.; Colby, K.A.; Skondra, D. Association of Metformin Use with Age-Related Macular Degeneration: A Case-Control Study. JAMA Ophthalmol. 2021, 139, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Romdhoniyyah, D.F.; Harding, S.P.; Cheyne, C.P.; Beare, N.A.V. Metformin, A Potential Role in Age-Related Macular Degeneration: A Systematic Review and Meta-Analysis. Ophthalmology 2021, 10, 245–260. [Google Scholar] [CrossRef]
- Daruich, A.; Jaworski, T.; Henry, H.; Zola, M.; Youale, J.; Parenti, L.; Naud, M.-C.; Delaunay, K.; Bertrand, M.; Berdugo, M.; et al. Oral Ursodeoxycholic Acid Crosses the Blood Retinal Barrier in Patients with Retinal Detachment and Protects Against Retinal Degeneration in an Ex Vivo Model. Neurotherapeutics 2021. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Primer Reference | ||
|---|---|---|---|
| ABCC8 | TaqMan™Gene Expression Assay (FAM) Rn01476317_m1 | #4331182 | Life Technologie SAS |
| GAPDH | TaqMan™Gene Expression Assay (FAM) Rn01775763_g1 | #4331182 | Life Technologie SAS |
| Non-Diabetic Females | Diabetic | Diabetic + GLI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age (Months) | Mean | SD | n | Mean | SD | n | Mean | SD | n |
| 2 | 4.94 | 0.3 | 5 | 6.28 | 0.64 | 8 | 5.96 | 1.33 | 5 |
| 6 | 4.6 | 0.27 | 3 | 9.15 | 0.65 | 8 | 7.74 | 2.05 | 5 |
| 12 | 5 | 0.27 | 3 | 10.62 | 1.63 | 8 | 9.125 | 1.6 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berdugo, M.; Delaunay, K.; Lebon, C.; Naud, M.-C.; Radet, L.; Zennaro, L.; Picard, E.; Daruich, A.; Beltrand, J.; Kermorvant-Duchemin, E.; et al. Long-Term Oral Treatment with Non-Hypoglycemic Dose of Glibenclamide Reduces Diabetic Retinopathy Damage in the Goto-KakizakiRat Model. Pharmaceutics 2021, 13, 1095. https://doi.org/10.3390/pharmaceutics13071095
Berdugo M, Delaunay K, Lebon C, Naud M-C, Radet L, Zennaro L, Picard E, Daruich A, Beltrand J, Kermorvant-Duchemin E, et al. Long-Term Oral Treatment with Non-Hypoglycemic Dose of Glibenclamide Reduces Diabetic Retinopathy Damage in the Goto-KakizakiRat Model. Pharmaceutics. 2021; 13(7):1095. https://doi.org/10.3390/pharmaceutics13071095
Chicago/Turabian StyleBerdugo, Marianne, Kimberley Delaunay, Cécile Lebon, Marie-Christine Naud, Lolita Radet, Léa Zennaro, Emilie Picard, Alejandra Daruich, Jacques Beltrand, Elsa Kermorvant-Duchemin, and et al. 2021. "Long-Term Oral Treatment with Non-Hypoglycemic Dose of Glibenclamide Reduces Diabetic Retinopathy Damage in the Goto-KakizakiRat Model" Pharmaceutics 13, no. 7: 1095. https://doi.org/10.3390/pharmaceutics13071095
APA StyleBerdugo, M., Delaunay, K., Lebon, C., Naud, M. -C., Radet, L., Zennaro, L., Picard, E., Daruich, A., Beltrand, J., Kermorvant-Duchemin, E., Polak, M., Crisanti, P., & Behar-Cohen, F. F. (2021). Long-Term Oral Treatment with Non-Hypoglycemic Dose of Glibenclamide Reduces Diabetic Retinopathy Damage in the Goto-KakizakiRat Model. Pharmaceutics, 13(7), 1095. https://doi.org/10.3390/pharmaceutics13071095