

Pharmacometric Modeling of the Impact of Azelastine Nasal Spray on SARS-CoV-2 Viral Load and Related Symptoms in COVID-19 Patients

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Studies Included in the Analysis
2.2. Data Analysis
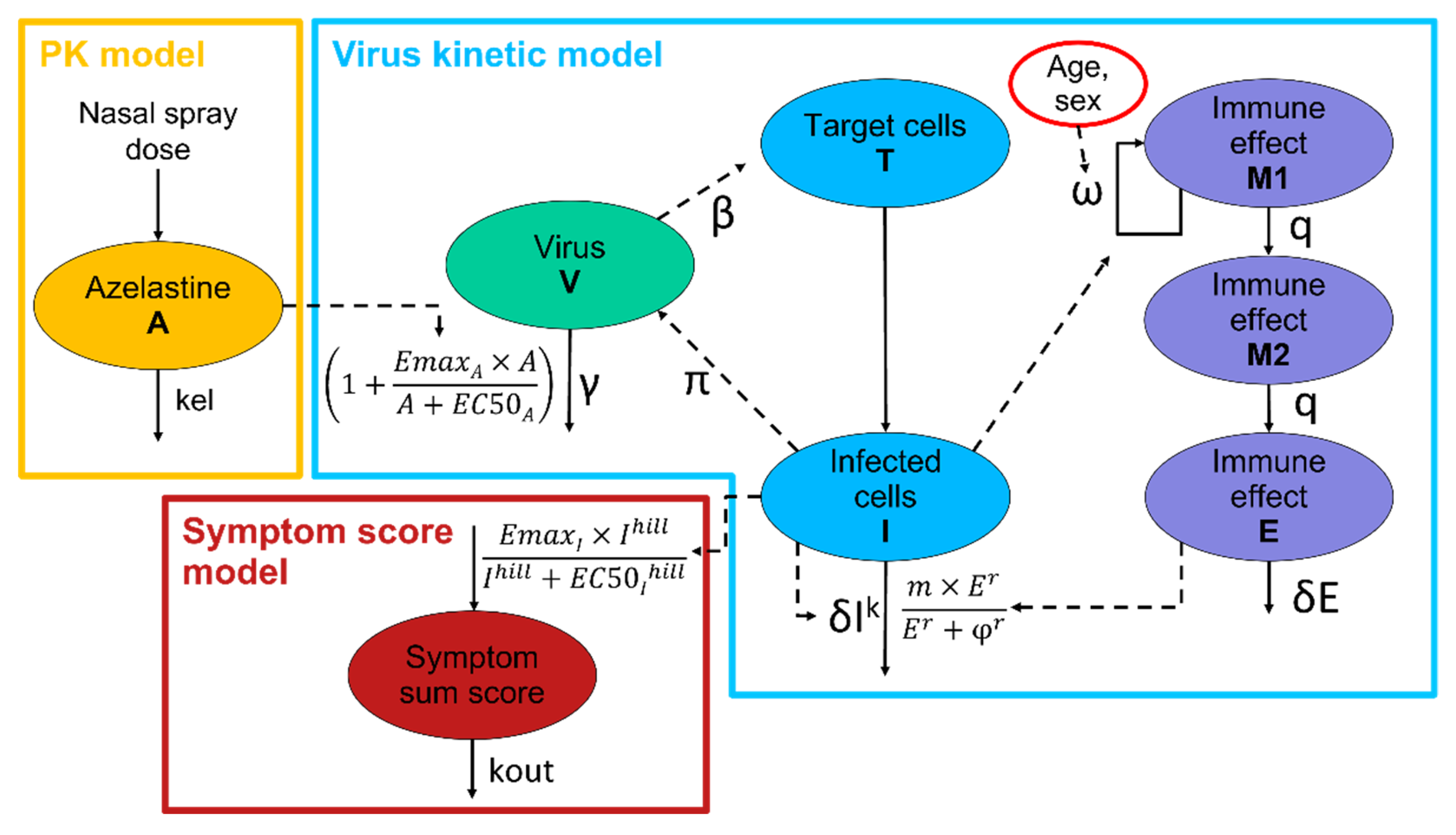
2.3. Model Development
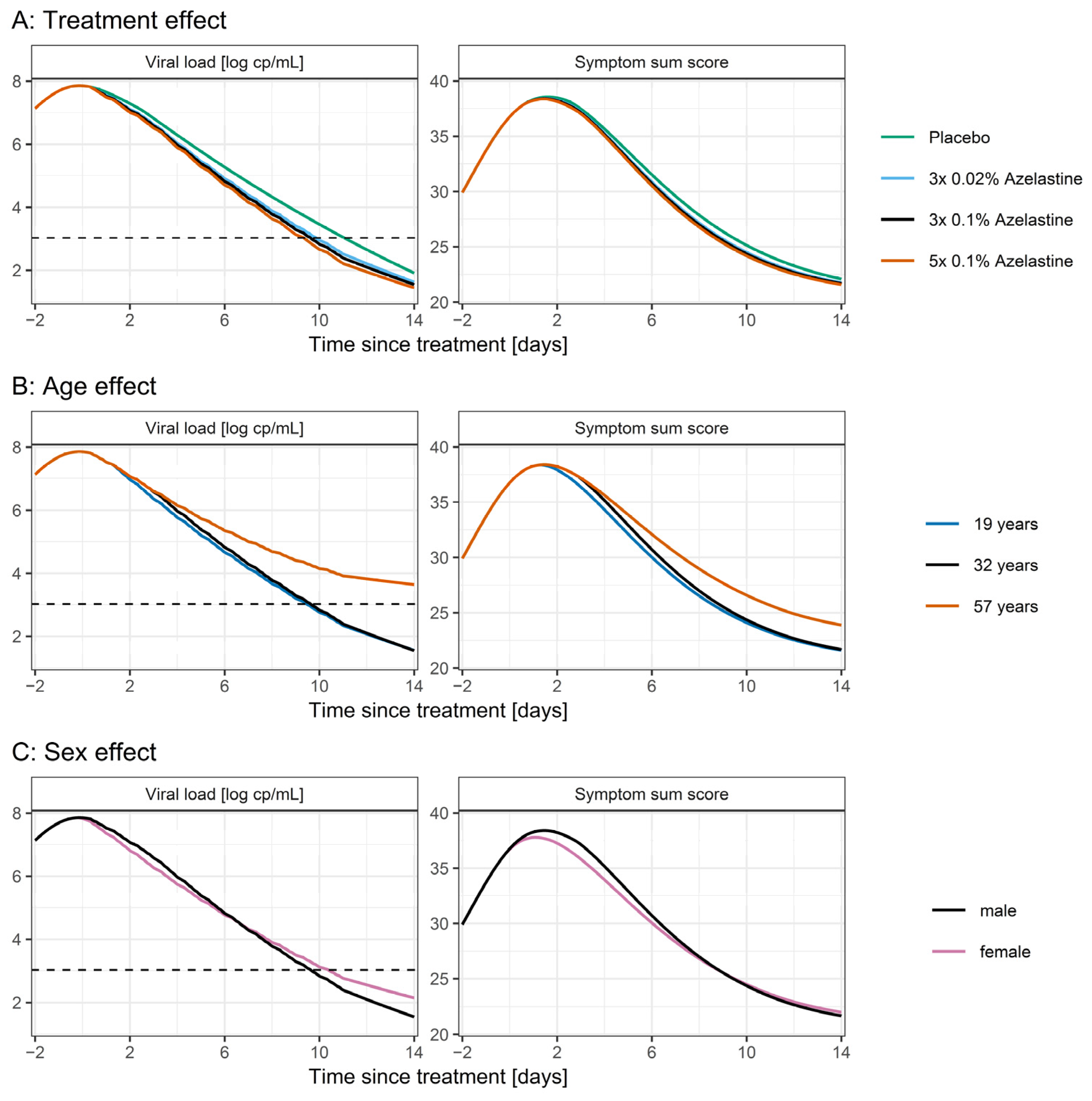
2.4. Simulations
3. Results
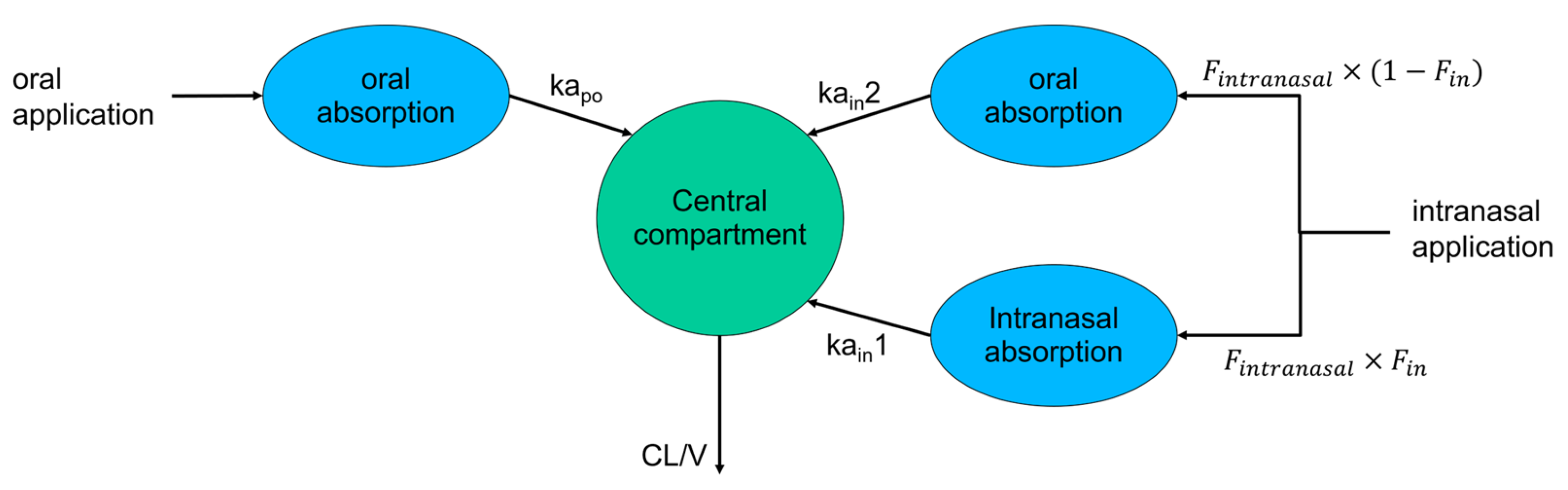
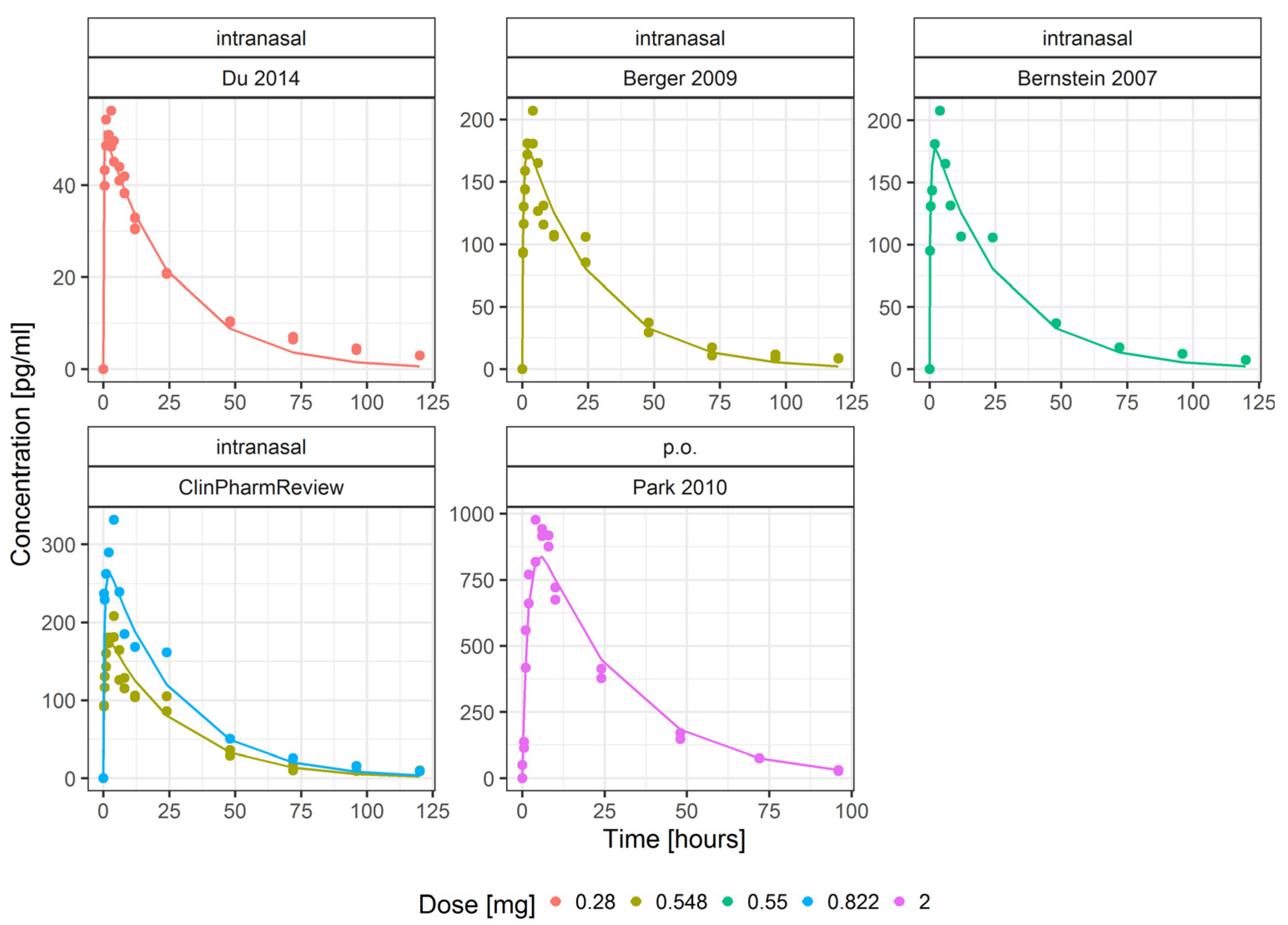
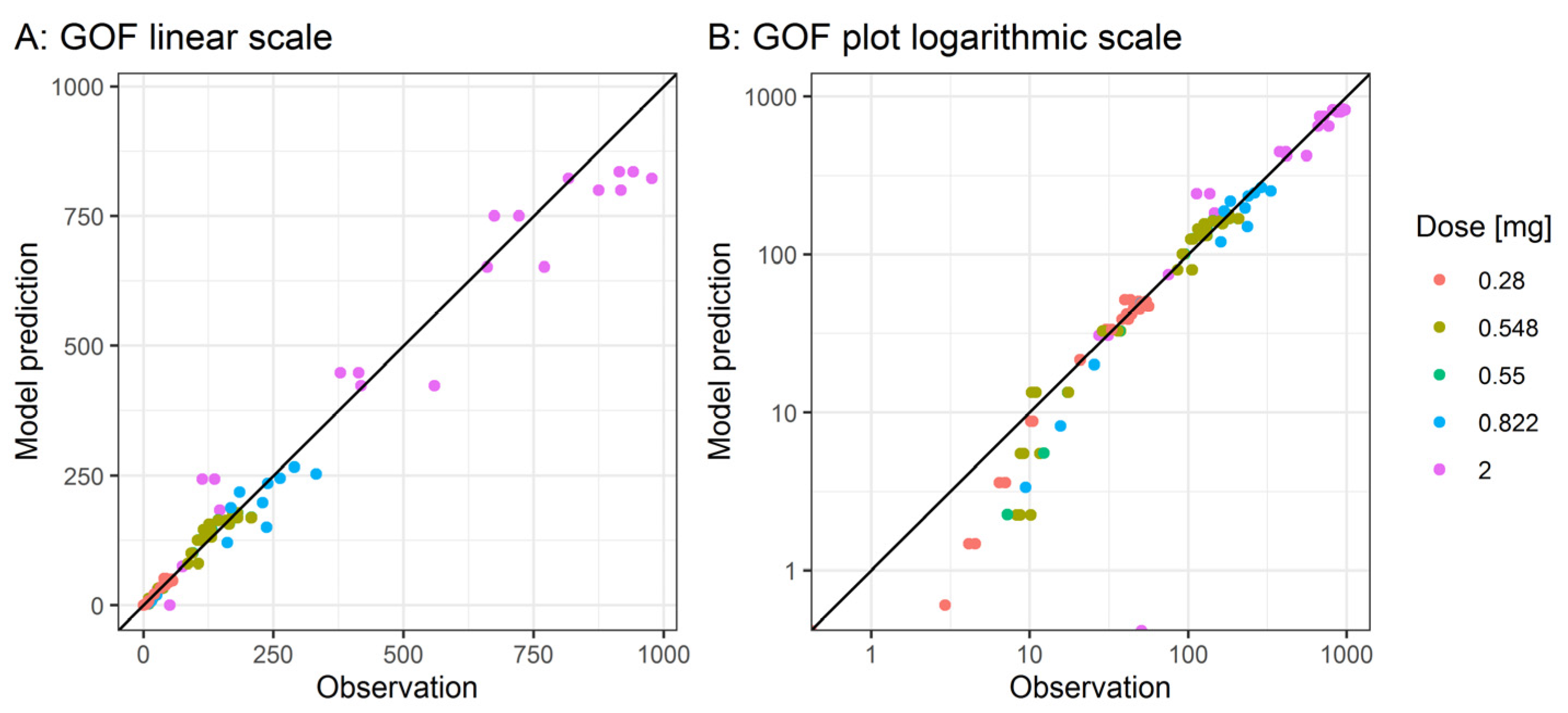
3.1. Pharmacokinetic Model
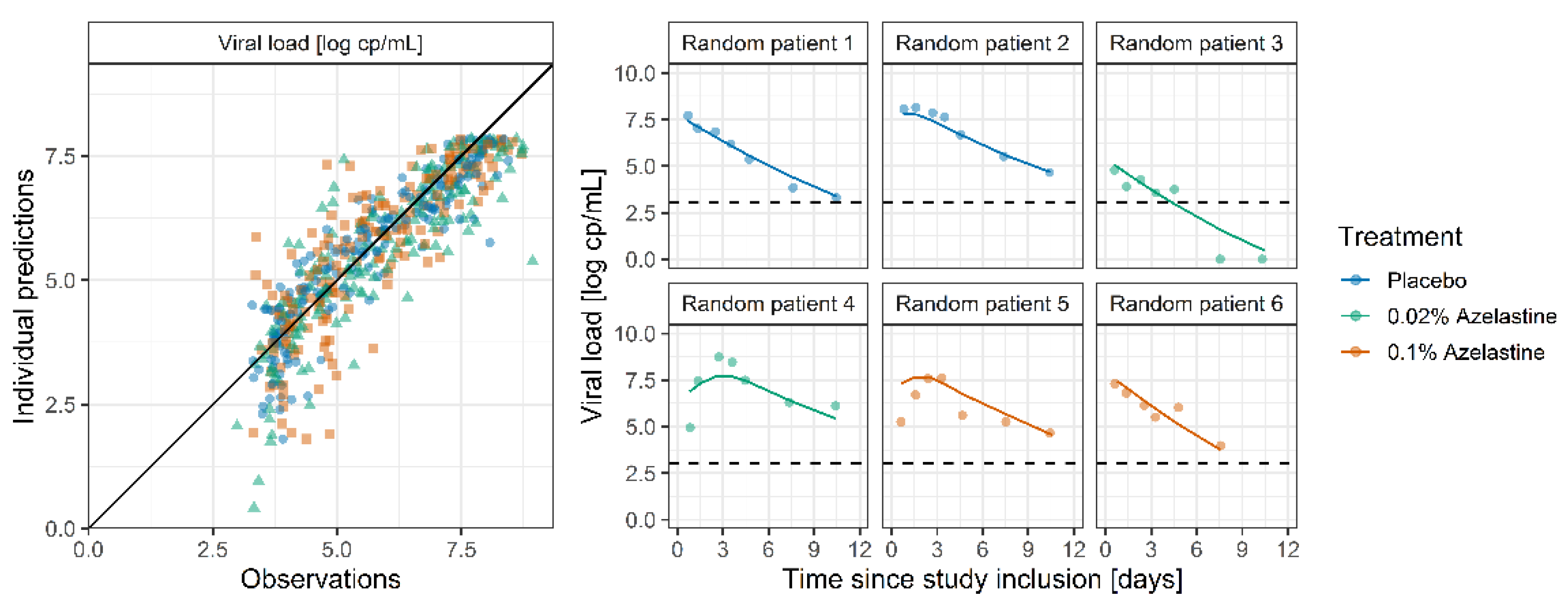
3.2. PK-Virus Kinetic Model
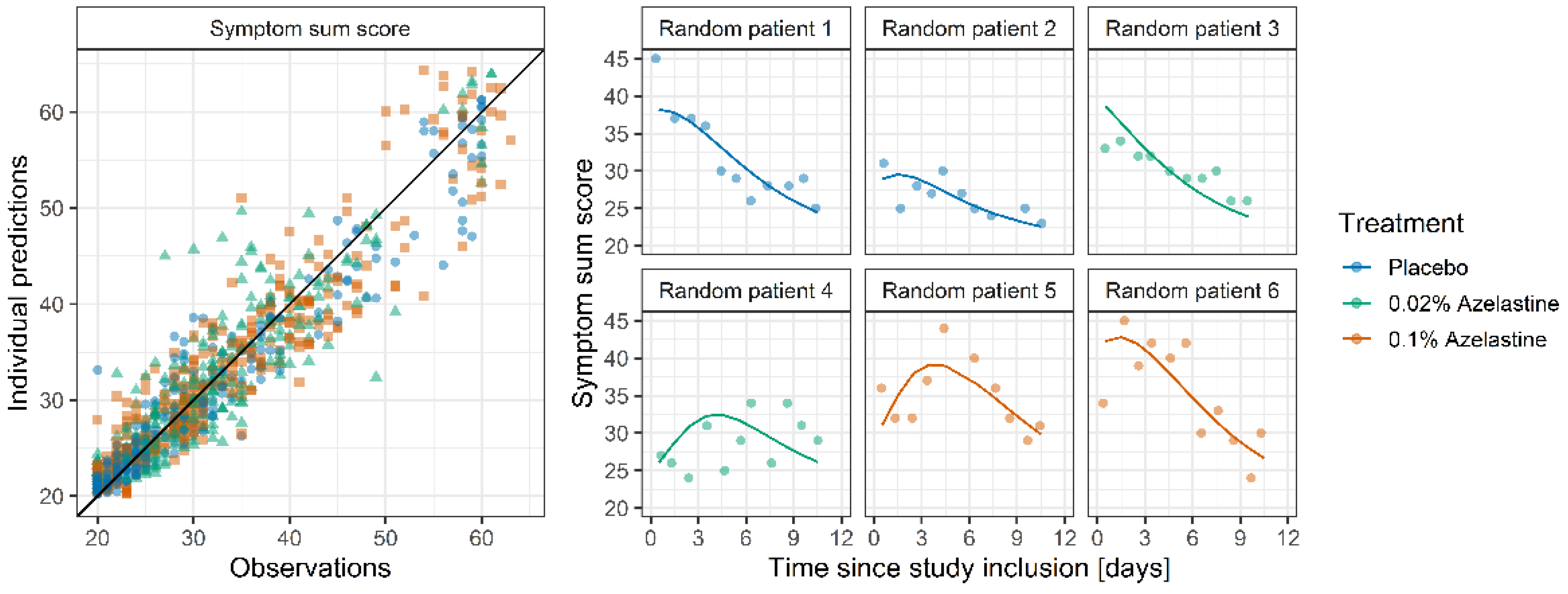
3.3. Symptom Score Model
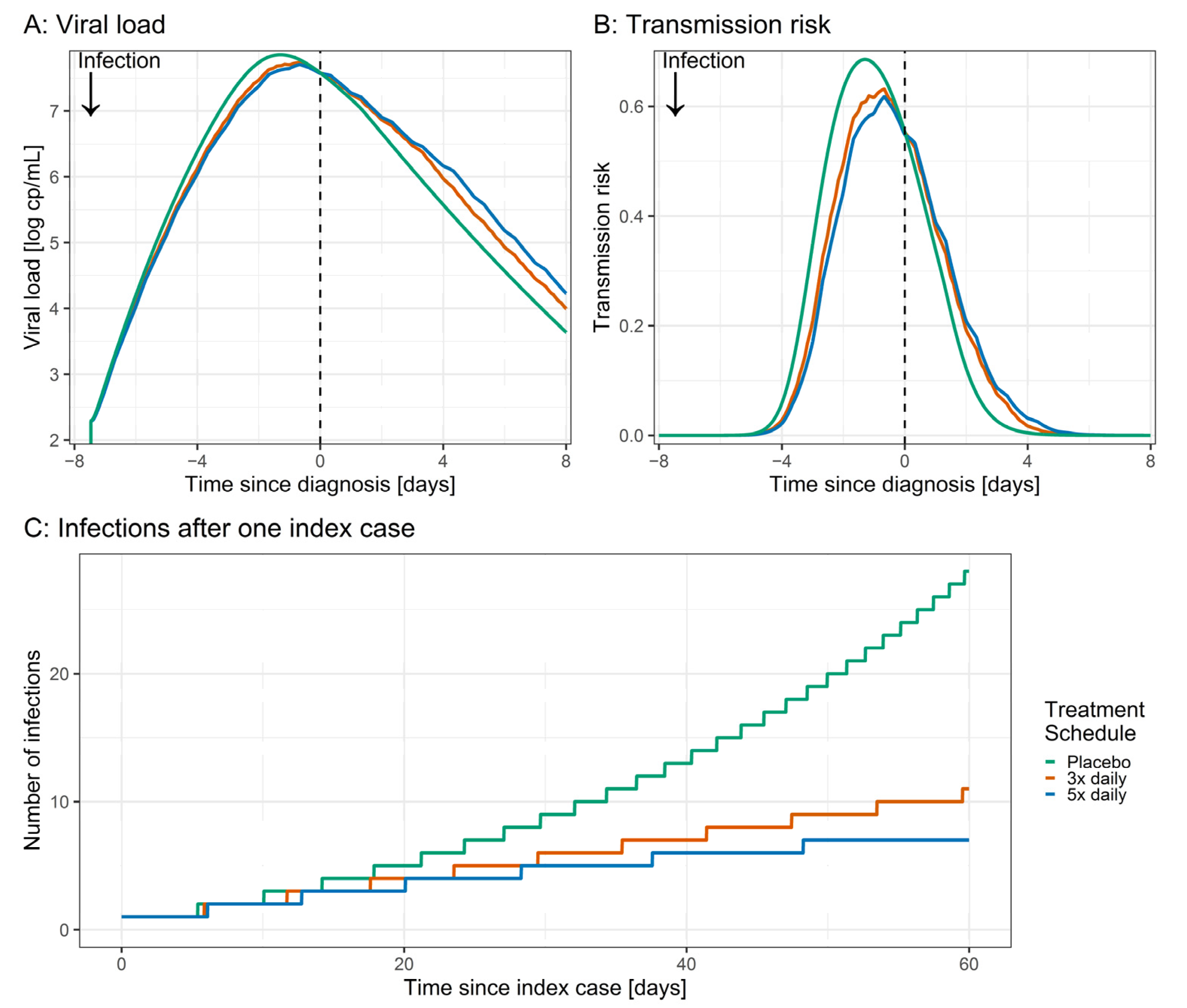
3.4. Simulations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Administration | Doses [mg] | n | Age [Years] (Range) | BMI [kg/m2] | Sex [% Male] (n) |
|---|---|---|---|---|---|---|
| Du 2014 [6] | Intranasal | 0.280 | 22 | 37.4 (21–55) | 24.57 | 54.5 (12) |
| Berger 2009 [7] | Intranasal | 0.548 | 36 | (18–50) | na | 100 (36) |
| Bernstein 2007 [8] | Intranasal | 0.550 | na | na | na | 100 |
| ClinPharmReview [9] | Intranasal | 0.548, 0.822 | 18 | (18–50) | na | 100 (18) |
| Park 2010 [10] | po | 2 | 23 | 23.0 (19–27) | na | 100 (23) |



| Parameter | Parameter Description | Unit | Estimate | RSE 1 |
|---|---|---|---|---|
| Fixed effects | ||||
| V1/F | Volume of distribution | L | 1960 | 3.6% |
| CL/F | Clearance rate | L/h | 72.9 | 3.3% |
| Kapo | po absorption rate | 1/h | 0.55 | 8.7% |
| Fintranasal | Intranasal relative bioavailability | - | 0.368 | 4.3% |
| Kain1 | Intranasal fast absorption rate | 1/h | 100 | FIX |
| Kain2 | Intranasal slow absorption rate | 1/h | 1.75 | 20.9% |
| Fin (1 spray) | Intranasal fraction absorbed fast (1 spray) | - | 1 | FIX |
| Fin (2 sprays) | Intranasal fraction absorbed fast (2 sprays) | - | 0.492 | 6.8% |
| Residual error | ||||
| Prop. error | Proportional error | %CV | 15.0 | 16.6 |
| Add. error | Additive error | SD; pg/mL | 11.0 | 59.8 |
References
- Reznikov, L.R.; Norris, M.H.; Vashisht, R.; Bluhm, A.P.; Li, D.; Liao, Y.-S.J.; Brown, A.; Butte, A.J.; Ostrov, D.A. Identification of Antiviral Antihistamines for COVID-19 Repurposing. Biochem. Biophys. Res. Commun. 2021, 538, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Corren, J. Review of Azelastine Nasal Spray in the Treatment of Allergic and Non-Allergic Rhinitis. Expert Opin. Pharmacother. 2007, 8, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Ge, S.; Lu, J.; Hou, Y.; Lv, Y.; Wang, C.; He, H. Azelastine Inhibits Viropexis of SARS-CoV-2 Spike Pseudovirus by Binding to SARS-CoV-2 Entry Receptor ACE2. Virology 2021, 560, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Konrat, R.; Papp, H.; Kimpel, J.; Rössler, A.; Szijártó, V.; Nagy, G.; Madai, M.; Zeghbib, S.; Kuczmog, A.; Lanszki, Z.; et al. The Anti-Histamine Azelastine, Identified by Computational Drug Repurposing, Inhibits Infection by Major Variants of SARS-CoV-2 in Cell Cultures and Reconstituted Human Nasal Tissue. Front. Pharmacol. 2022, 13, 861295. [Google Scholar] [CrossRef]
- Klussmann, J.; Grosheva, M.; Meiser, P.; Lehmann, C.; Szijártó, V.; Nagy, G.; Konrat, R.; Flegel, M.; Holzer, F.; Groß, D.; et al. COVID-19: Azelastine Nasal Spray Reduces Virus-Load in Nasal Swabs (CARVIN) Early Intervention with Azelastine Nasal Spray May Reduce Viral Load in SARS-CoV-2 Infected Patients—Results from a Randomized, Double-Blind, Placebo-Controlled Phase II Clinical Trial; PREPRINT (Version 1). 2022. Available online: https://www.researchsquare.com/article/rs-1893502/v1 (accessed on 19 September 2022).
- Du, D.; Targett, D.; Stolberg, E.; Canali, A. A Clinical Pharmacokinetic Study Comparing Two Azelastine Hydrochloride Nasal Formulations in a Single-Dose Design. Eur. J. Drug Metab. Pharmacokinet. 2014, 39, 69–75. [Google Scholar] [CrossRef]
- Berger, W.E. Pharmacokinetic Characteristics and Safety and Tolerability of a Reformulated Azelastine Hydrochloride Nasal Spray in Patients with Chronic Rhinitis. Expert Opin. Drug Metab. Toxicol. 2009, 5, 91–102. [Google Scholar] [CrossRef]
- Bernstein, J.A. Azelastine Hydrochloride: A Review of Pharmacology, Pharmacokinetics, Clinical Efficacy and Tolerability. Curr. Med. Res. Opin. 2007, 23, 2442–2452. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research Clinical Pharmacology and Biopharmaceutics Review(s), Application Number 22-371s000. 2008. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022371s000ClinPharm.pdf (accessed on 23 September 2022).
- Park, Y.S.; Kim, S.H.; Kim, Y.J.; Yang, S.C.; Lee, M.H.; Shaw, L.M.; Kang, J.S. Determination of Azelastine in Human Plasma by Validated Liquid Chromatography Coupled to Tandom Mass Spectrometry (LC-ESI/MS/MS) for the Clinical Studies. Int. J. Biomed. Sci. 2010, 6, 120–127. [Google Scholar]
- Wojtyniak, J.G.; Britz, H.; Selzer, D.; Schwab, M.; Lehr, T. Data Digitizing: Accurate and Precise Data Extraction for Quantitative Systems Pharmacology and Physiologically-Based Pharmacokinetic Modeling. CPT Pharmacomet. Syst. Pharmacol. 2020, 9, 322–331. [Google Scholar] [CrossRef]
- Mould, D.R.; Upton, R.N. Basic Concepts in Population Modeling, Simulation, and Model-Based Drug Development-Part 2: Introduction to Pharmacokinetic Modeling Methods. CPT Pharmacomet. Syst. Pharmacol. 2013, 2, e38. [Google Scholar] [CrossRef]
- Goyal, A.; Duke, E.R.; Cardozo-Ojeda, E.F.; Schiffer, J.T. Modeling explains prolonged SARS-CoV-2 nasal shedding relative to lung shedding in remdesivir-treated rhesus macaques. iScience 2022, 25, 104448. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Cardozo-Ojeda, E.F.; Schiffer, J.T. Potency and Timing of Antiviral Therapy as Determinants of Duration of SARS-CoV-2 Shedding and Intensity of Inflammatory Response. Sci. Adv. 2020, 6, eabc7112. [Google Scholar] [CrossRef] [PubMed]
- Néant, N.; Lingas, G.; Le Hingrat, Q.; Ghosn, J.; Engelmann, I.; Lepiller, Q.; Gaymard, A.; Ferré, V.; Hartard, C.; Plantier, J.C.; et al. Modeling SARS-CoV-2 Viral Kinetics and Association with Mortality in Hospitalized Patients from the French COVID Cohort. Proc. Natl. Acad. Sci. USA 2021, 118, e2017962118. [Google Scholar] [CrossRef] [PubMed]
- Perelson, A.S.; Ke, R. Mechanistic Modeling of SARS-CoV-2 and Other Infectious Diseases and the Effects of Therapeutics. Clin. Pharmacol. Ther. 2021, 109, 829–840. [Google Scholar] [CrossRef]
- Wählby, U.; Jonsson, E.N.; Karlsson, M.O. Comparison of Stepwise Covariate Model Building Strategies in Population Pharmacokinetic-Pharmacodynamic Analysis. AAPS PharmSci 2002, 4, E27. [Google Scholar] [CrossRef]
- Goyal, A.; Reeves, D.B.; Fabian Cardozo-Ojeda, E.; Schiffer, J.T.; Mayer, B.T. Viral Load and Contact Heterogeneity Predict SARS-CoV-2 Transmission and Super-Spreading Events. eLife 2021, 10, e63537. [Google Scholar] [CrossRef]
- an der Heiden, M. SARS-CoV-2-Nowcasting Und -R-Schaetzung; Zenodo: Berlin, Germany, 2022. [Google Scholar]
- Schipper, N.G.M.; Verhoef, J.C.; Merkus, F.W.H.M. The Nasal Mucociliary Clearance: Relevance to Nasal Drug Delivery. Pharm. Res. 1991, 8, 807–814. [Google Scholar] [CrossRef]
- Furubayashi, T.; Kamaguchi, A.; Kawaharada, K.; Masaoka, Y.; Kataoka, M.; Yamashita, S.; Higashi, Y.; Sakane, T. Evaluation of the Contribution of the Nasal Cavity and Gastrointestinal Tract to Drug Absorption Following Nasal Application to Rats. Biol. Pharm. Bull. 2007, 30, 608–611. [Google Scholar] [CrossRef]
- Furubayashi, T.; Kamaguchi, A.; Kawaharada, K.; Masaoka, Y.; Kataoka, M.; Yamashita, S.; Higashi, Y.; Sakane, T. Kinetic Model to Predict the Absorption of Nasally Applied Drugs from in Vitro Transcellular Permeability of Drugs. Biol. Pharm. Bull. 2007, 30, 1007–1010. [Google Scholar] [CrossRef]
- Marc, A.; Kerioui, M.; Blanquart, F.; Bertrand, J.; Mitjà, O.; Corbacho-Monné, M.; Marks, M.; Guedj, J. Quantifying the Relationship between Sars-Cov-2 Viral Load and Infectiousness. eLife 2021, 10, e69302. [Google Scholar] [CrossRef]
- Robert Koch Institute. Wöchentlicher Lagebericht Des RKI Zur Coronavirus-Krankheit-2019 (COVID-19); Robert Koch Institute: Berlin, Germany, 2022. [Google Scholar]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex Differences in Immune Responses That Underlie COVID-19 Disease Outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Starke, K.R.; Petereit-Haack, G.; Schubert, M.; Kämpf, D.; Schliebner, A.; Hegewald, J.; Seidler, A. The Age-Related Risk of Severe Outcomes Due to COVID-19 Infection: A Rapid Review, Meta-Analysis, and Meta-Regression. Int. J. Environ. Res. Public Health 2020, 17, 5974. [Google Scholar] [CrossRef] [PubMed]
- Jun, T.; Nirenberg, S.; Weinberger, T.; Sharma, N.; Pujadas, E.; Cordon-Cardo, C.; Kovatch, P.; Huang, K. Analysis of Sex-Specific Risk Factors and Clinical Outcomes in COVID-19. Commun. Med. 2021, 1, 3. [Google Scholar] [CrossRef] [PubMed]





| Group | n | Age [Years] (sd) | Weight [kg] (sd) | Sex [% male] (n) |
|---|---|---|---|---|
| Placebo | 27 | 33 (13.6) | 70 (16.3) | 48.1 (13) |
| 0.02% azelastine | 28 | 28 (12.8) | 70.5 (15.7) | 53.6 (15) |
| 0.1% azelastine | 27 | 35 (13.1) | 75 (15.7) | 44.4 (12) |
| All | 82 | 32 (13.1) | 71.5 (15.8) | 48.8 (40) |
| Parameter | Value (RSE 1/Shrinkage) * | Unit | Source | Parameter Description |
|---|---|---|---|---|
| PK model | ||||
| kel | 49.9 | day−1 | [20] | Azelastine elimination rate |
| PK-virus kinetic model | ||||
| ALAG | 6.51 (3.2%) | days | estimated | Time between infection and diagnosis |
| β | 8.89 × 10−9 (1.2%) | virion−1day−1 | estimated | Viral infectivity |
| γ | 1.92 (6.7%) | day−1 | estimated | Virus elimination rate |
| δ | 3.1 | day−1cellsk | [14] | Elimination rate of infected cells |
| ω | 2.75 × 10−5 | day−1cells−1 | [14] | Extend of T-cell response |
| π | 398 | day−1 | [14] | Virus production rate |
| k | 0.08 | - | [14] | Fast immune response |
| q | 2.4 × 10−5 | day−1 | [14] | Differentiation rate of T-cells |
| δE | 1 | day−1 | [14] | Elimination rate of T-cell response |
| m | 3 | day−1cells−1 | [14] | Maximum T-cell response |
| r | 10 | - | [14] | Hill coefficient of T-cell response |
| ϕ | 100 | cells | [14] | Half maximum effective effector cell level |
| I0 | 1 | cells | [14] | Baseline number of infected cells |
| M0 | 1 | cells | [14] | Baseline number of T-cells effect cells |
| T0 | 107 | cells | [14] | Baseline number of target cells |
| EmaxA | 0.37 (2.9%) | - | estimated | Maximum azelastine effect |
| EC50A | 0.0629 (5.1%) | µg | estimated | Half maximum effective azelastine amount |
| Sex—ω | 1.95 (9.8%) | - | estimated | Covariate effect of sex on ω |
| Age—ω | −0.287 (2.9%) | - | estimated | Covariate effect of age on ω |
| IIV ALAG | 58.0 (16.1%/9%) | %CV | estimated | Interindividual variability on ALAG |
| AE | 1.2 (0.8%) | SD, log cp/mL | estimated | Additive residual error viral load |
| Symptom score model | ||||
| Kout | 0.37 (5.9%) | day−1 | estimated | Output rate |
| EmaxI | 15 (8.3%) | - | estimated | Maximum input rate |
| EC50I | 5.01 × 105 (9%) | cells | estimated | Half maximal effective infected cells |
| hill | 0.298 (5.9%) | - | estimated | Hill coefficient |
| IIV Emax | 78.7 (9%/3%) | %CV | estimated | Interindividual variability on Emax |
| PE | 10–9 (2.6%) | %CV | estimated | Proportional residual error symptom sum score |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dings, C.; Meiser, P.; Holzer, F.; Flegel, M.; Selzer, D.; Nagy, E.; Mösges, R.; Klussmann, J.P.; Lehr, T. Pharmacometric Modeling of the Impact of Azelastine Nasal Spray on SARS-CoV-2 Viral Load and Related Symptoms in COVID-19 Patients. Pharmaceutics 2022, 14, 2059. https://doi.org/10.3390/pharmaceutics14102059
Dings C, Meiser P, Holzer F, Flegel M, Selzer D, Nagy E, Mösges R, Klussmann JP, Lehr T. Pharmacometric Modeling of the Impact of Azelastine Nasal Spray on SARS-CoV-2 Viral Load and Related Symptoms in COVID-19 Patients. Pharmaceutics. 2022; 14(10):2059. https://doi.org/10.3390/pharmaceutics14102059
Chicago/Turabian StyleDings, Christiane, Peter Meiser, Frank Holzer, Michael Flegel, Dominik Selzer, Eszter Nagy, Ralph Mösges, Jens Peter Klussmann, and Thorsten Lehr. 2022. "Pharmacometric Modeling of the Impact of Azelastine Nasal Spray on SARS-CoV-2 Viral Load and Related Symptoms in COVID-19 Patients" Pharmaceutics 14, no. 10: 2059. https://doi.org/10.3390/pharmaceutics14102059
APA StyleDings, C., Meiser, P., Holzer, F., Flegel, M., Selzer, D., Nagy, E., Mösges, R., Klussmann, J. P., & Lehr, T. (2022). Pharmacometric Modeling of the Impact of Azelastine Nasal Spray on SARS-CoV-2 Viral Load and Related Symptoms in COVID-19 Patients. Pharmaceutics, 14(10), 2059. https://doi.org/10.3390/pharmaceutics14102059