
Simulation-Based Gastrointestinal Endoscopy Sedations: A Novel Validation to Multidrug Pharmacodynamic Modeling
 ,
,
Abstract
:1. Background
2. Methods
2.1. Search Strategy and Article Identification
- (1)
- Contained at least one three-drug combinational regimen. If an identified study included both three- and two-drug regimens, both regimens are qualified for simulation.
- (2)
- The three drugs must be intravenous midazolam, propofol, and an opioid (alfentanil, fentanyl, remifentanil, or morphine).
- (3)
- Studies were performed for gastrointestinal endoscopy.
- (4)
- Studies must report procedure and recovery time.
- (5)
- English literature.
2.2. Simulation Setup
- (1)
- Midazolam typically lasts 30 to 60 min [18]. The dose is not divided and given at induction.
- (2)
- Fentanyl reaches peak effect-site concentration (Ce) at 3.6 min and more than 50% Ce remains at 30 min [19]. The dose is not divided and given at induction.
- (3)
- Alfentanil reaches peak Ce at 1.4 min, with a rapid decline over the first ten minutes after a bolus [19]. It is divided into equivalent doses at 10 min intervals and avoided 10 min before the procedure concludes.
- (4)
- Propofol’s time to peak effect (TTPE) is 1.6–1.7 min [20]. The total dose is divided into boluses at 2 to 3 min intervals or greater if the total dose is small. It is avoided in the final two minutes.
2.3. Pharmacologic Models
2.4. Outcome Assessment
3. Results
3.1. Study Eligibility Search Results
3.2. Recovery and Time Definition Modification in the Identified Studies
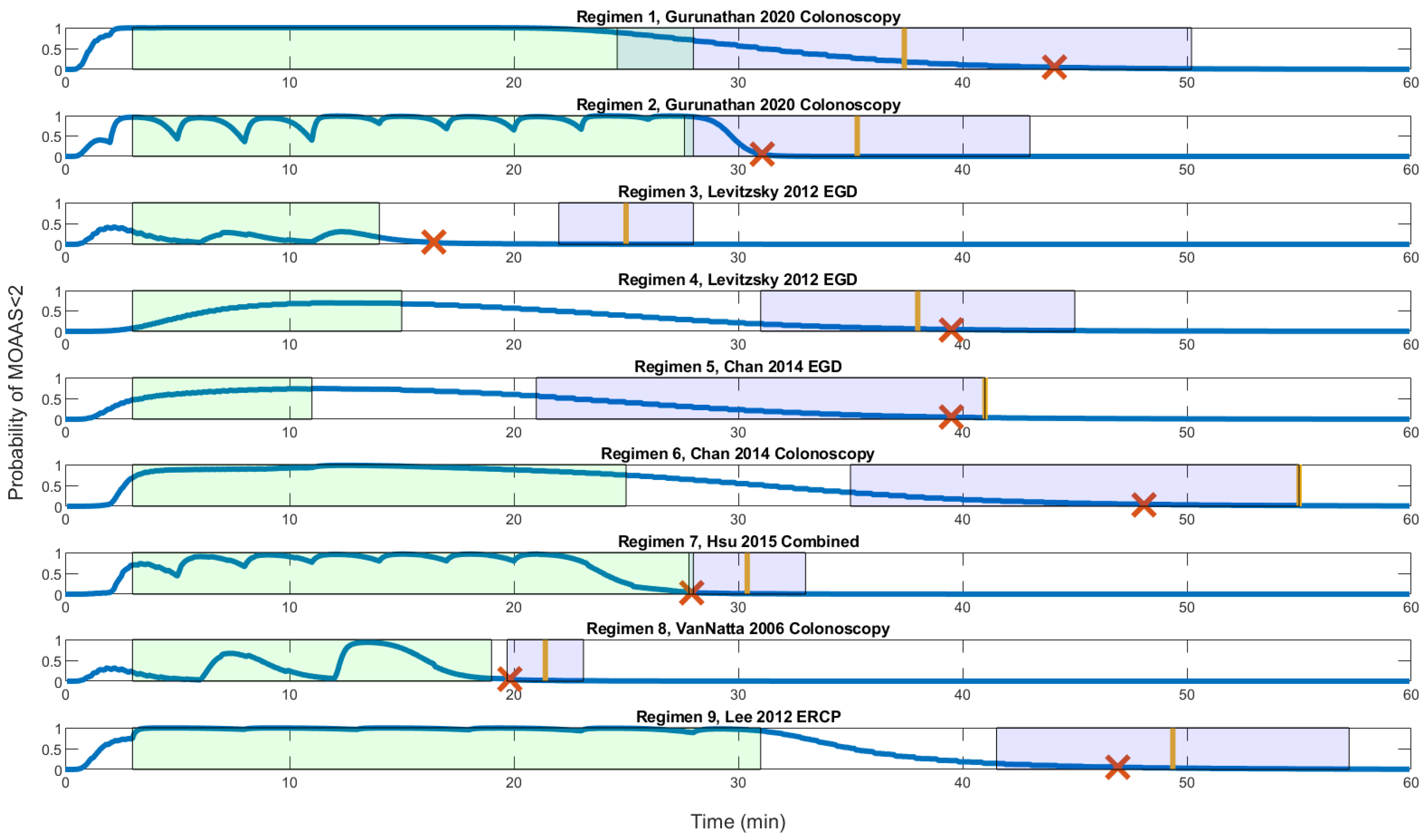
3.3. Recovery Profile of the Clinical Studies and Model Comparison
3.4. Model Intraprocedural Sedation Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liou, J.Y.; Tsou, M.Y.; Ting, C.K. Response surface models in the field of anesthesia: A crash course. Acta Anaesthesiol. Taiwanica Off. J. Taiwan Soc. Anesthesiol. 2015, 53, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Liou, J.Y.; Ting, C.K.; Mandell, M.S.; Chang, K.Y.; Teng, W.N.; Huang, Y.Y.; Tsou, M.Y. Predicting the Best Fit: A Comparison of Response Surface Models for Midazolam and Alfentanil Sedation in Procedures with Varying Stimulation. Anesth. Analg. 2016, 123, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Tallarida, R.J.; Stone, D.J., Jr.; McCary, J.D.; Raffa, R.B. Response surface analysis of synergism between morphine and clonidine. J. Pharmacol. Exp. Ther. 1999, 289, 8–13. [Google Scholar] [PubMed]
- Minto, C.F.; Schnider, T.W.; Short, T.G.; Gregg, K.M.; Gentilini, A.; Shafer, S.L. Response surface model for anesthetic drug interactions. Anesthesiology 2000, 92, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Mertens, M.J.; Olofsen, E.; Engbers, F.H.; Burm, A.G.; Bovill, J.G.; Vuyk, J. Propofol reduces perioperative remifentanil requirements in a synergistic manner: Response surface modeling of perioperative remifentanil-propofol interactions. Anesthesiology 2003, 99, 347–359. [Google Scholar] [CrossRef]
- Nieuwenhuijs, D.J.; Olofsen, E.; Romberg, R.R.; Sarton, E.; Ward, D.; Engbers, F.; Vuyk, J.; Mooren, R.; Teppema, L.J.; Dahan, A. Response surface modeling of remifentanil-propofol interaction on cardiorespiratory control and bispectral index. Anesthesiology 2003, 98, 312–322. [Google Scholar] [CrossRef]
- Bouillon, T.W.; Bruhn, J.; Radulescu, L.; Andresen, C.; Shafer, T.J.; Cohane, C.; Shafer, S.L. Pharmacodynamic interaction between propofol and remifentanil regarding hypnosis, tolerance of laryngoscopy, bispectral index, and electroencephalographic approximate entropy. Anesthesiology 2004, 100, 1353–1372. [Google Scholar] [CrossRef]
- Hendrickx, J.F.; Eger, E.I.; Sonner, J.M.; Shafer, S.L. Is synergy the rule? A review of anesthetic interactions producing hypnosis and immobility. Anesth. Analg. 2008, 107, 494–506. [Google Scholar] [CrossRef]
- Liou, J.Y.; Ting, C.K.; Teng, W.N.; Mandell, M.S.; Tsou, M.Y. Adaptation of non-linear mixed amount with zero amount response surface model for analysis of concentration-dependent synergism and safety with midazolam, alfentanil, and propofol sedation. Br. J. Anaesth. 2018, 120, 1209–1218. [Google Scholar] [CrossRef]
- Hannivoort, L.N.; Vereecke, H.E.; Proost, J.H.; Heyse, B.E.; Eleveld, D.J.; Bouillon, T.W.; Struys, M.M.; Luginbuhl, M. Probability to tolerate laryngoscopy and noxious stimulation response index as general indicators of the anaesthetic potency of sevoflurane, propofol, and remifentanil. Br. J. Anaesth. 2016, 116, 624–631. [Google Scholar] [CrossRef] [Green Version]
- Liou, J.Y.; Ting, C.K.; Hou, M.C.; Tsou, M.Y. A Response Surface Model Exploration of Dosing Strategies in Gastrointestinal Endoscopies Using Midazolam and Opioids. Medicine 2016, 95, e3520. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Y.; Ting, C.K.; Liou, J.Y.; Chen, K.H.; Tsou, M.Y.; Chang, W.K. A previously published propofol-remifentanil response surface model does not predict patient response well in video-assisted thoracic surgery. Medicine 2017, 96, e6895. [Google Scholar] [CrossRef] [PubMed]
- LaPierre, C.D.; Johnson, K.B.; Randall, B.R.; White, J.L.; Egan, T.D. An exploration of remifentanil-propofol combinations that lead to a loss of response to esophageal instrumentation, a loss of responsiveness, and/or onset of intolerable ventilatory depression. Anesth. Analg. 2011, 113, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.B.; Hightower, C.D.; Wood, D.A.; Miller, K.M.; Aisenberg, J. Moderate level sedation during endoscopy: A prospective study using low-dose propofol, meperidine/fentanyl, and midazolam. Gastrointest. Endosc. 2004, 59, 795–803. [Google Scholar] [CrossRef]
- Angsuwatcharakon, P.; Rerknimitr, R.; Ridtitid, W.; Kongkam, P.; Poonyathawon, S.; Ponauthai, Y.; Sumdin, S.; Kullavanijaya, P. Cocktail sedation containing propofol versus conventional sedation for ERCP: A prospective, randomized controlled study. BMC Anesthesiol. 2012, 12, 20. [Google Scholar] [CrossRef]
- Lee, T.H.; Lee, C.K.; Park, S.H.; Lee, S.H.; Chung, I.K.; Choi, H.J.; Cha, S.W.; Moon, J.H.; Cho, Y.D.; Hwangbo, Y.; et al. Balanced propofol sedation versus propofol monosedation in therapeutic pancreaticobiliary endoscopic procedures. Dig. Dis. Sci. 2012, 57, 2113–2121. [Google Scholar] [CrossRef]
- VanNatta, M.E.; Rex, D.K. Propofol alone titrated to deep sedation versus propofol in combination with opioids and/or benzodiazepines and titrated to moderate sedation for colonoscopy. Am. J. Gastroenterol. 2006, 101, 2209–2217. [Google Scholar] [CrossRef]
- Schwagmeier, R.; Alincic, S.; Striebel, H.W. Midazolam pharmacokinetics following intravenous and buccal administration. Br. J. Clin. Pharmacol. 1998, 46, 203–206. [Google Scholar] [CrossRef]
- Shafer, S.L.; Varvel, J.R. Pharmacokinetics, pharmacodynamics, and rational opioid selection. Anesthesiology 1991, 74, 53–63. [Google Scholar] [CrossRef]
- Schnider, T.W.; Minto, C.F.; Shafer, S.L.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Youngs, E.J. The influence of age on propofol pharmacodynamics. Anesthesiology 1999, 90, 1502–1516. [Google Scholar] [CrossRef]
- Levitzky, B.E.; Lopez, R.; Dumot, J.A.; Vargo, J.J. Moderate sedation for elective upper endoscopy with balanced propofol versus fentanyl and midazolam alone: A randomized clinical trial. Endoscopy 2012, 44, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Maitre, P.O.; Vozeh, S.; Heykants, J.; Thomson, D.A.; Stanski, D.R. Population pharmacokinetics of alfentanil: The average dose-plasma concentration relationship and interindividual variability in patients. Anesthesiology 1987, 66, 3–12. [Google Scholar] [CrossRef]
- Zomorodi, K.; Donner, A.; Somma, J.; Barr, J.; Sladen, R.; Ramsay, J.; Geller, E.; Shafer, S.L. Population pharmacokinetics of midazolam administered by target controlled infusion for sedation following coronary artery bypass grafting. Anesthesiology 1998, 89, 1418–1429. [Google Scholar] [CrossRef]
- Shafer, S.L.; Varvel, J.R.; Aziz, N.; Scott, J.C. Pharmacokinetics of fentanyl administered by computer-controlled infusion pump. Anesthesiology 1990, 73, 1091–1102. [Google Scholar] [CrossRef] [PubMed]
- Schnider, T.W.; Minto, C.F.; Gambus, P.L.; Andresen, C.; Goodale, D.B.; Shafer, S.L.; Youngs, E.J. The influence of method of administration and covariates on the pharmacokinetics of propofol in adult volunteers. Anesthesiology 1998, 88, 1170–1182. [Google Scholar] [CrossRef] [PubMed]
- Vereecke, H.E.; Proost, J.H.; Heyse, B.; Eleveld, D.J.; Katoh, T.; Luginbuhl, M.; Struys, M.M. Interaction between nitrous oxide, sevoflurane, and opioids: A response surface approach. Anesthesiology 2013, 118, 894–902. [Google Scholar] [CrossRef]
- Vuyk, J.; Mertens, M.J.; Olofsen, E.; Burm, A.G.; Bovill, J.G. Propofol anesthesia and rational opioid selection: Determination of optimal EC50-EC95 propofol-opioid concentrations that assure adequate anesthesia and a rapid return of consciousness. Anesthesiology 1997, 87, 1549–1562. [Google Scholar] [CrossRef]
- Gurunathan, U.; Rahman, T.; Williams, Z.; Vandeleur, A.; Sriram, S.; Harch, J.; Boggett, S.; Hill, C.; Bowyer, A.; Royse, C. Effect of Midazolam in Addition to Propofol and Opiate Sedation on the Quality of Recovery After Colonoscopy: A Randomized Clinical Trial. Anesth. Analg. 2020, 131, 741–750. [Google Scholar] [CrossRef]
- Chan, W.H.; Chang, S.L.; Lin, C.S.; Chen, M.J.; Fan, S.Z. Target-controlled infusion of propofol versus intermittent bolus of a sedative cocktail regimen in deep sedation for gastrointestinal endoscopy: Comparison of cardiovascular and respiratory parameters. J. Dig. Dis. 2014, 15, 18–26. [Google Scholar] [CrossRef]
- Hsu, C.D.; Huang, J.M.; Chuang, Y.P.; Wei, H.Y.; Su, Y.C.; Wu, J.Y.; Wang, W.M.; Hsu, H.T.; Huang, H.F.; Lu, I.C.; et al. Propofol target-controlled infusion for sedated gastrointestinal endoscopy: A comparison of propofol alone versus propofol-fentanyl-midazolam. Kaohsiung J. Med. Sci. 2015, 31, 580–584. [Google Scholar] [CrossRef] [Green Version]
- Bill, K.; Fee, J.; Clarke, R.J.J.o.t.R.S.o.M. Psychomotor and clinical assessment of flumazenil as an antagonist of midazolam. J. R. Soc. Med. 1991, 84, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Luginbuhl, M.; Vuilleumier, P.; Schumacher, P.; Stuber, F. Anesthesia or sedation for gastroenterologic endoscopies. Curr. Opin. Anaesthesiol. 2009, 22, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Struys, M.M.; De Smet, T.; Mortier, E.P. Simulated drug administration: An emerging tool for teaching clinical pharmacology during anesthesiology training. Clin. Pharmacol. Ther. 2008, 84, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H. Medical simulation is needed in anesthesia training to achieve patient’s safety. Korean J. Anesthesiol. 2013, 64, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Saddawi-Konefka, D.; Cooper, J.B. Anesthesia and simulation: An historic relationship. In Comprehensive Healthcare Simulation: Anesthesiology; Springer: Berlin/Heidelberg, Germany, 2020; pp. 3–13. [Google Scholar]
- ASGE Standards of Practice Committee; Early, D.S.; Lightdale, J.R.; Vargo, J.J., 2nd; Acosta, R.D.; Chandrasekhara, V.; Chathadi, K.V.; Evans, J.A.; Fisher, D.A.; Fonkalsrud, L.; et al. Guidelines for sedation and anesthesia in GI endoscopy. Gastrointest. Endosc. 2018, 87, 327–337. [Google Scholar] [CrossRef]
- McQuaid, K.R.; Laine, L. A systematic review and meta-analysis of randomized, controlled trials of moderate sedation for routine endoscopic procedures. Gastrointest. Endosc. 2008, 67, 910–923. [Google Scholar] [CrossRef]
- Vinik, H.R.; Bradley, E.L., Jr.; Kissin, I. Triple anesthetic combination: Propofol-midazolam-alfentanil. Anesth. Analg. 1994, 78, 354–358. [Google Scholar] [CrossRef]
- Aldrete, J.A.; Kroulik, D.J.A. A postanesthetic recovery score. Analg. Anesth. 1970, 49, 924–934. [Google Scholar] [CrossRef]
- Motsch, J.; Wandel, C.; Neff, S.; Martin, E. A comparative study of the use of sevoflurane and propofol in ambulatory surgery. Anaesthesist 1996, 45 Suppl. 1, S57–S62. [Google Scholar]
- Orhon, Z.N.; Devrim, S.; Celik, M.; Dogan, Y.; Yildirim, A.; Basok, E.K. Comparison of recovery profiles of propofol and sevoflurane anesthesia with bispectral index monitoring in percutaneous nephrolithotomy. Korean J. Anesthesiol. 2013, 64, 223–228. [Google Scholar] [CrossRef]
- Haenggi, M.; Ypparila-Wolters, H.; Hauser, K.; Caviezel, C.; Takala, J.; Korhonen, I.; Jakob, S.M. Intra- and inter-individual variation of BIS-index and Entropy during controlled sedation with midazolam/remifentanil and dexmedetomidine/remifentanil in healthy volunteers: An interventional study. Crit. Care 2009, 13, R20. [Google Scholar] [CrossRef] [Green Version]
- Gašparović, S.; Rustemović, N.; Opačić, M.; Premužić, M.; Korušić, A.; Božikov, J.; Bates, T.J.W.j.o.g.W. Clinical analysis of propofol deep sedation for 1,104 patients undergoing gastrointestinal endoscopic procedures: A three year prospective study. World J. Gastroenterol. 2006, 12, 327. [Google Scholar] [CrossRef] [PubMed]
- Dossa, F.; Megetto, O.; Yakubu, M.; Zhang, D.D.Q.; Baxter, N.N. Sedation practices for routine gastrointestinal endoscopy: A systematic review of recommendations. BMC Gastroenterol. 2021, 21, 22. [Google Scholar] [CrossRef] [PubMed]
- Eleveld, D.J.; Colin, P.; Absalom, A.R.; Struys, M. Pharmacokinetic-pharmacodynamic model for propofol for broad application in anaesthesia and sedation. Br. J. Anaesth. 2018, 120, 942–959. [Google Scholar] [CrossRef] [PubMed]
- Heyse, B.; Proost, J.H.; Schumacher, P.M.; Bouillon, T.W.; Vereecke, H.E.; Eleveld, D.J.; Luginbuhl, M.; Struys, M.M. Sevoflurane remifentanil interaction: Comparison of different response surface models. Anesthesiology 2012, 116, 311–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Observation | Score |
|---|---|
| Responds readily to name spoken in normal tone | 5 |
| Lethargic response to name spoken in normal tone | 4 |
| Responds only after name is called loudly and/or repeatedly | 3 |
| Responds only after mild prodding or shaking | 2 |
| Does not respond to mild prodding or shaking | 1 |
| Does not respond to trapezius squeeze (pain) | 0 |
| Regimen | Sedation Target | Recovery Evaluation | Recovery Target | Procedure | Tp (min) | Trs (min) | Trs SD (min) |
|---|---|---|---|---|---|---|---|
| 1 [21] | Not reported | Eye opening | Eye opening | Colonoscopy | 25 | 9.4 | 12.8 |
| 2 [21] | Not reported | Eye opening | Eye opening | Colonoscopy | 25 | 7.3 | 7.7 |
| 3 [22] | Moderate | MOAA/S | 5 | EGD | 11 | 11 | 3 |
| 4 [22] | Moderate | MOAA/S | 5 | EGD | 12 | 23 | 7 |
| 5 [23] | Deep | Reverse OOA/S | 1 | EGD | 8 | 30 | –20 |
| 6 [23] | Deep | Reverse OOA/S | 1 | Colonoscopy | 22 | 30 | –20 |
| 7 [24] | Deep | MOAA/S | 5 | Combined EGD and colonoscopy | 25 | 2.4 | 2.6 |
| 8 [17] | Moderate | MOAA/S | Talking | Colonoscopy | 16 | 2.4 | 1.7 |
| 9 [16] | Moderate | Modified Aldrete score | 10 | ERCP | 28 | 18.37 | 7.86 |
| Regimen | Study Protocols | Simulation Setup |
|---|---|---|
| 1 [21] | Midazolam: 0.04 mg/kg | Midazolam: 2.5 mg |
| Fentanyl: 77.5 μg | Fentanyl: 78 μg | |
| Propofol: 276 mg | Propofol: 30 mg at 0, 2, 4, 6, 8, 10, 12, 14, 16 min | |
| 2 [21] | Fentanyl: 66.9 μg | Fentanyl: 67 μg |
| Propofol: 329 mg | Propofol: 40 mg at 0, 11, 23 min; 30 mg at 2, 5, 8, 14, 17, 20, 26 min | |
| 3 [22] | Midazolam: 1 mg | Midazolam: 1 mg |
| Fentanyl: 50 μg | Fentanyl: 50 μg | |
| Propofol: 10 mg at induction, 5–10 mg every 30 s after assessment, total 50 mg | Propofol: 30 mg at 0 min; 10 mg at 6, 11 min | |
| 4 [22] | Midazolam: 3 mg | Midazolam: 3 mg |
| Fentanyl: 100 μg | Fentanyl: 100 μg | |
| 5 [23] | Midazolam: 3 mg | Midazolam: 3 mg |
| Alfentanil: 600 μg | Alfentanil: 600 μg | |
| Propofol: 10 mg | Propofol:10 mg at 0 min | |
| 6 [23] | Midazolam: 3.8 mg | Midazolam: 3.8 mg |
| Alfentanil: 800 μg | Alfentanil: 400 μg at 0, 10 min | |
| Propofol: 23 mg | Propofol: 10 mg at 2, 11 min | |
| 7 [24] | Midazolam: 1.1 mg | Midazolam: 1.1 mg |
| Fentanyl: 52.5 μg | Fentanyl: 52.5 μg | |
| Propofol: 159 mg | Propofol: 20 mg at 0, 2, 5, 8, 11, 14, 17, 20 min | |
| 8 [17] | Midazolam: 1 mg | Midazolam: 1 mg |
| Fentanyl 50 μg | Fentanyl: 50 μg | |
| Propofol: 82.5 mg | Propofol: 30 mg at 0, 12 min; 20 mg at 6 min | |
| 9 [16] | Midazolam: 0.05 mg/kg | Midazolam: 3.25 mg |
| Fentanyl: 50 μg | Fentanyl: 50 μg | |
| Propofol: 145.64 mg | Propofol: 20 mg at 0, 8, 13, 18, 23 min; 30 mg at 3 min; 15 mg at 28 min |
| Regimen | Trm (min) | Tro (min) | Tro Range (min) | Ratio of Intraprocedural Deep Sedation |
|---|---|---|---|---|
| 1 [21] | 44.1 | 37.4 | 24.6–50.2 | - |
| 2 [21] | 31.1 | 35.3 | 27.6–43.0 | - |
| 3 [22] | 16.4 | 25.0 | 22.0–28.0 | 0.00 |
| 4 [22] | 39.5 | 38.0 | 31.0–45.0 | 0.71 |
| 5 [23] | 39.5 | 41.0 | 21.0–41.0 | 0.94 |
| 6 [23] | 48.1 | 55.0 | 35.0–55.0 | 1.00 |
| 7 [24] | 27.9 | 30.4 | 27.8–33.0 | 0.83 |
| 8 [17] | 19.8 | 21.4 | 19.7–23.1 | 0.26 |
| 9 [16] | 46.9 | 49.4 | 41.5–57.2 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liou, J.-Y.; Wang, H.-Y.; Kuo, I.-T.; Chang, W.-K.; Ting, C.-K. Simulation-Based Gastrointestinal Endoscopy Sedations: A Novel Validation to Multidrug Pharmacodynamic Modeling. Pharmaceutics 2022, 14, 2056. https://doi.org/10.3390/pharmaceutics14102056
Liou J-Y, Wang H-Y, Kuo I-T, Chang W-K, Ting C-K. Simulation-Based Gastrointestinal Endoscopy Sedations: A Novel Validation to Multidrug Pharmacodynamic Modeling. Pharmaceutics. 2022; 14(10):2056. https://doi.org/10.3390/pharmaceutics14102056
Chicago/Turabian StyleLiou, Jing-Yang, Hsin-Yi Wang, I-Ting Kuo, Wen-Kuei Chang, and Chien-Kun Ting. 2022. "Simulation-Based Gastrointestinal Endoscopy Sedations: A Novel Validation to Multidrug Pharmacodynamic Modeling" Pharmaceutics 14, no. 10: 2056. https://doi.org/10.3390/pharmaceutics14102056
APA StyleLiou, J. -Y., Wang, H. -Y., Kuo, I. -T., Chang, W. -K., & Ting, C. -K. (2022). Simulation-Based Gastrointestinal Endoscopy Sedations: A Novel Validation to Multidrug Pharmacodynamic Modeling. Pharmaceutics, 14(10), 2056. https://doi.org/10.3390/pharmaceutics14102056