
Investigation of Trends in the Research on Transferrin Receptor-Mediated Drug Delivery via a Bibliometric and Thematic Analysis



Abstract
:1. Introduction
1.1. Transferrin
1.2. Transferrin Receptors
1.2.1. Transferrin Receptor 1 (TfR 1)
1.2.2. Transferrin Receptor 2 (TfR 2)
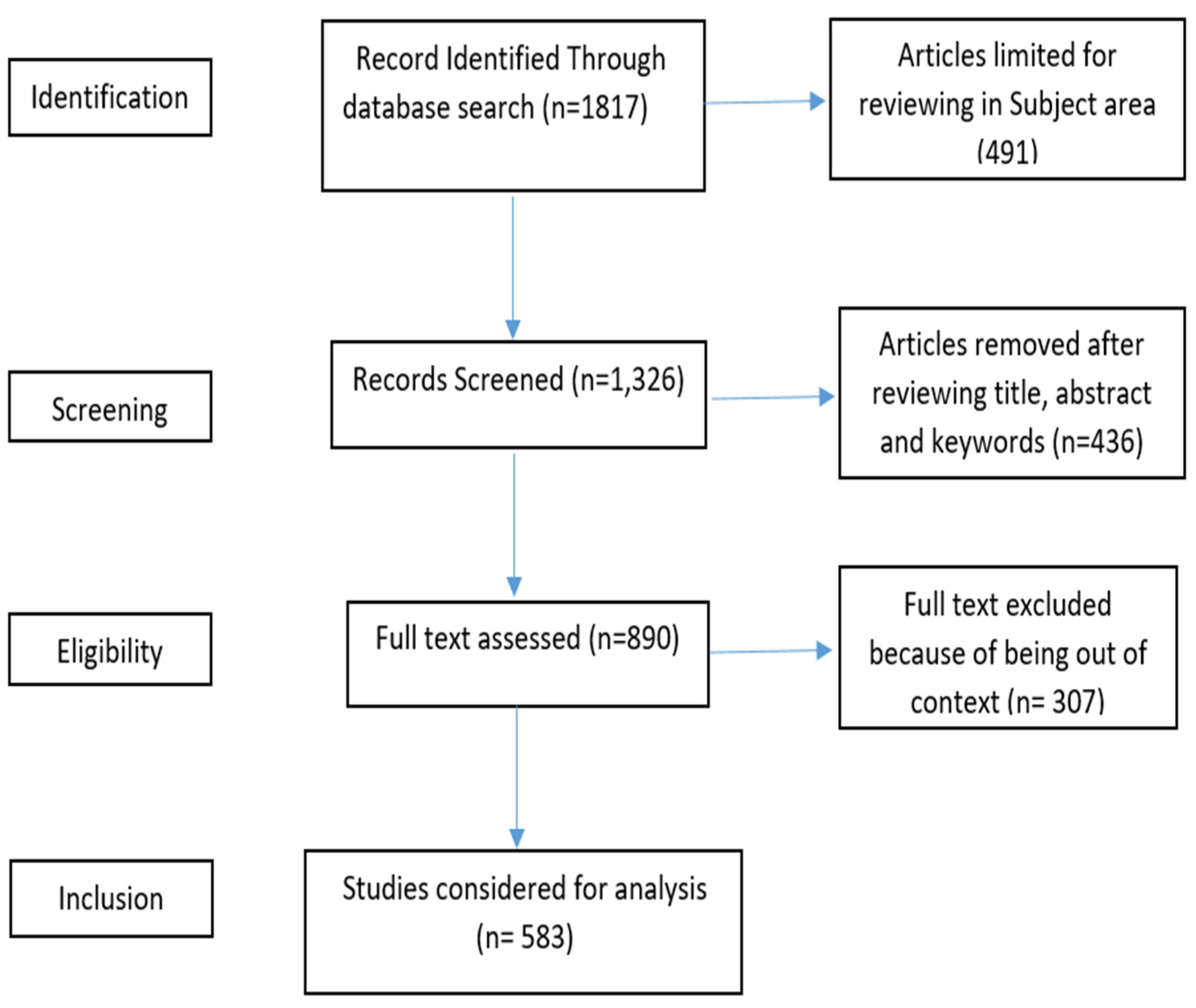
2. Materials and Methods
3. Results and Discussion
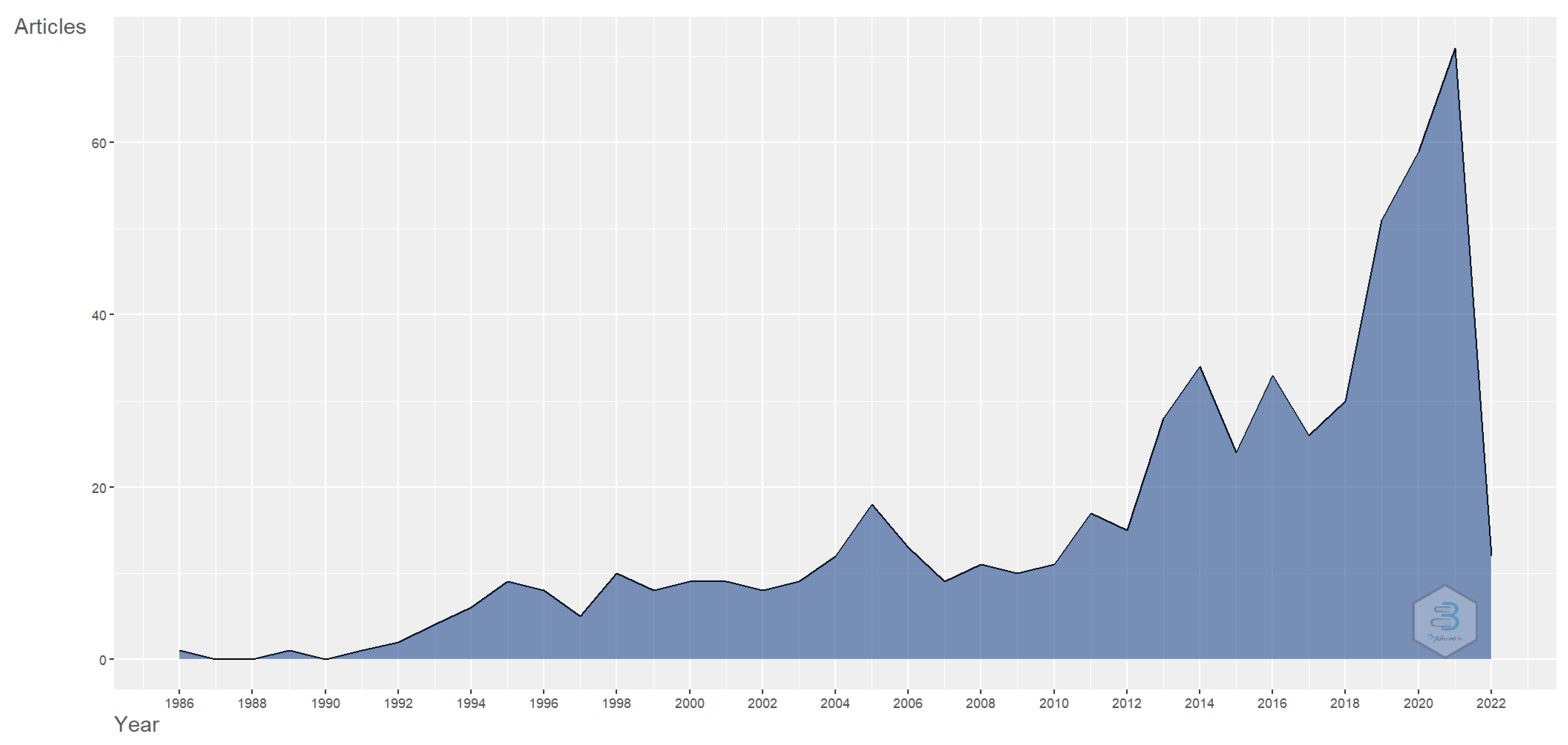
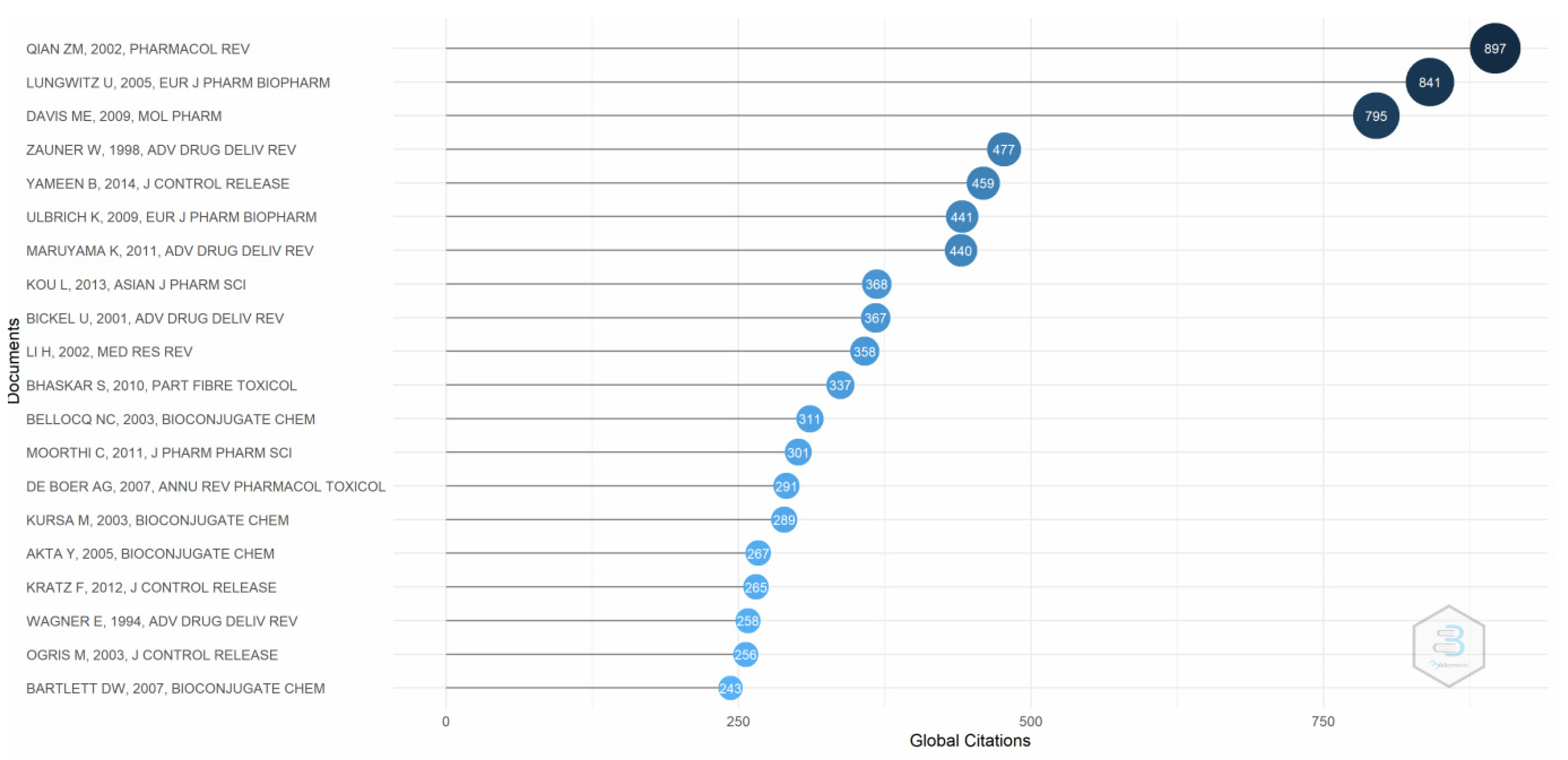
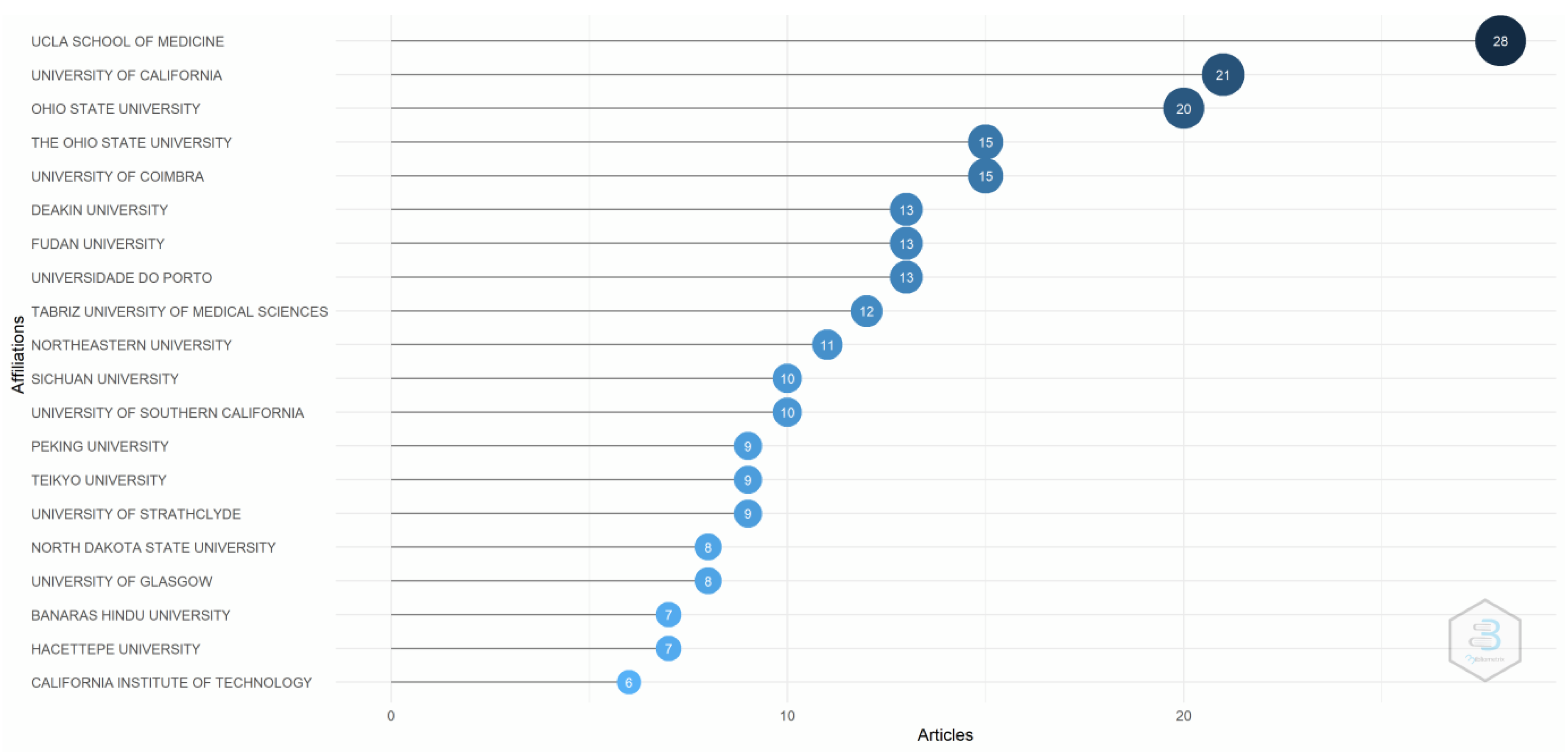
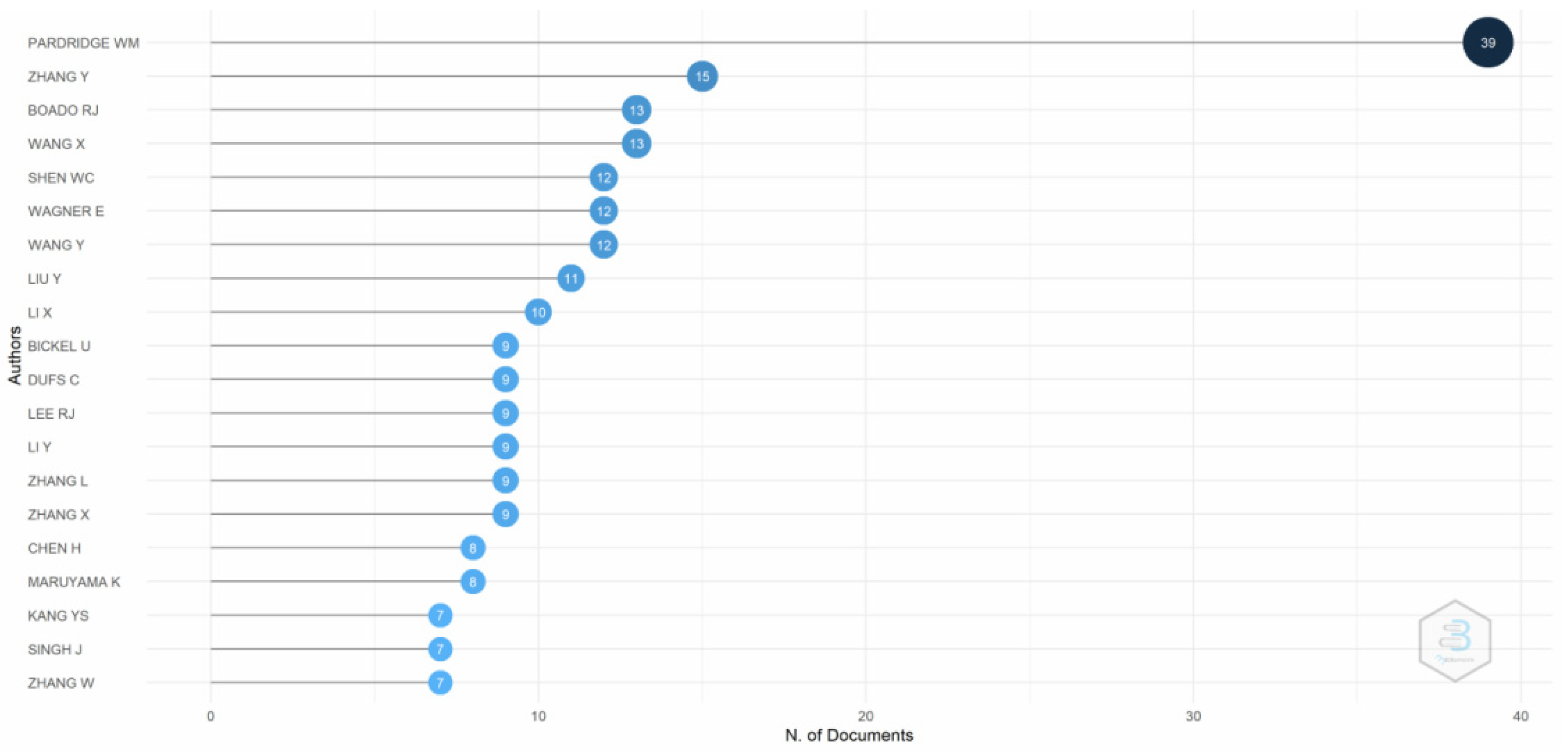
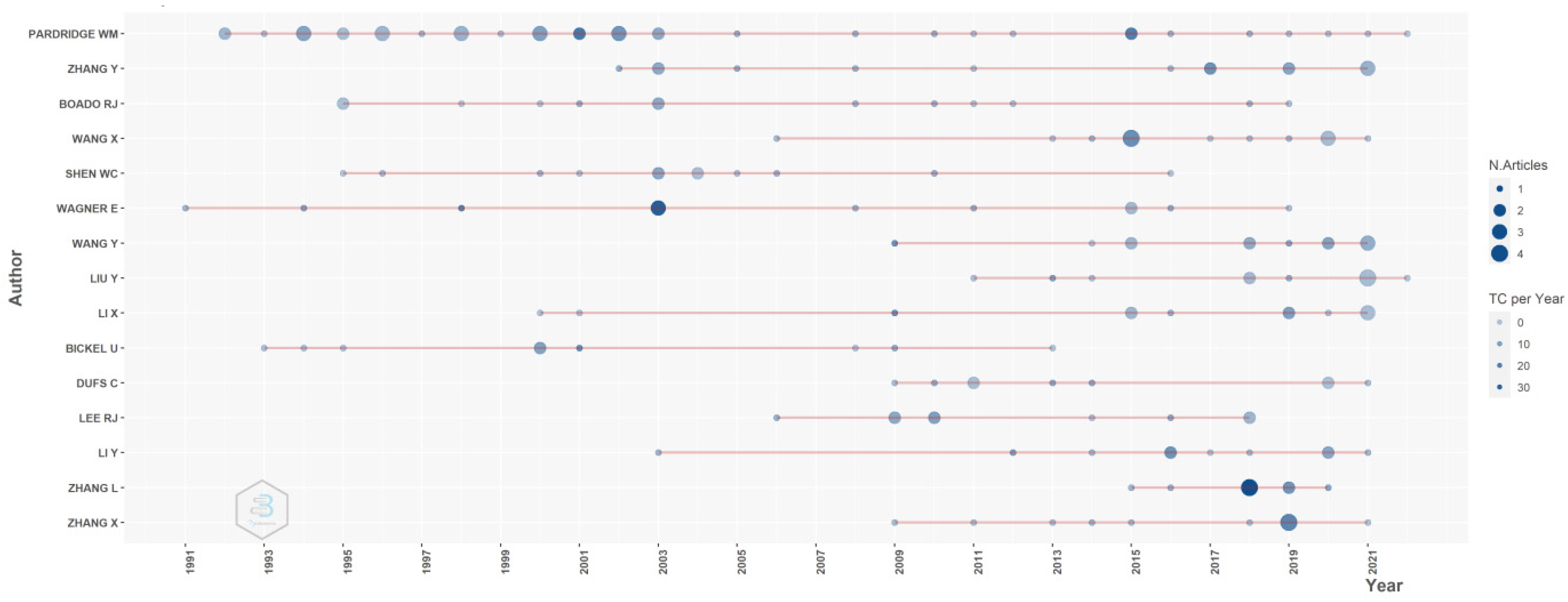
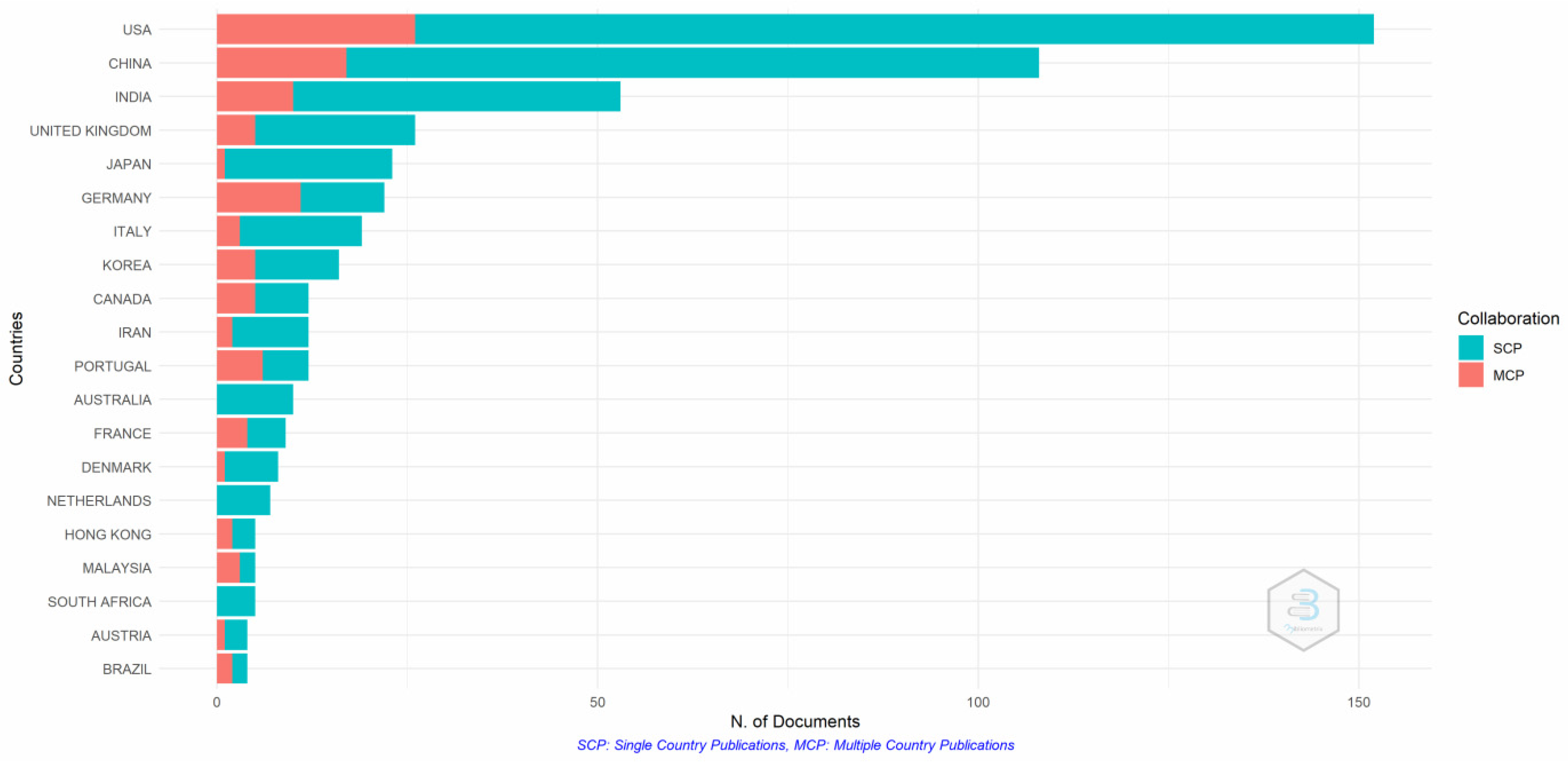
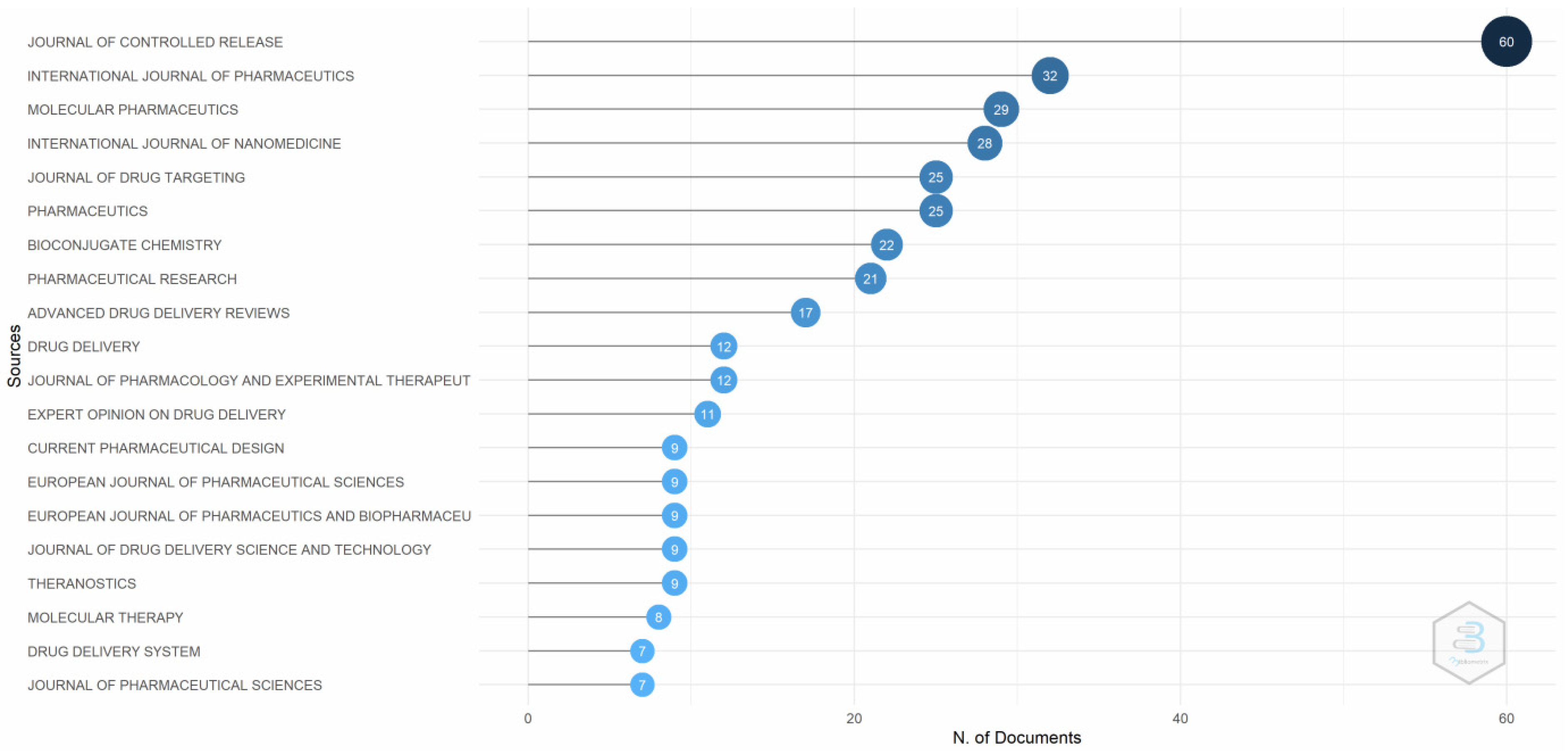
3.1. Performance Analysis
3.2. Science Mapping
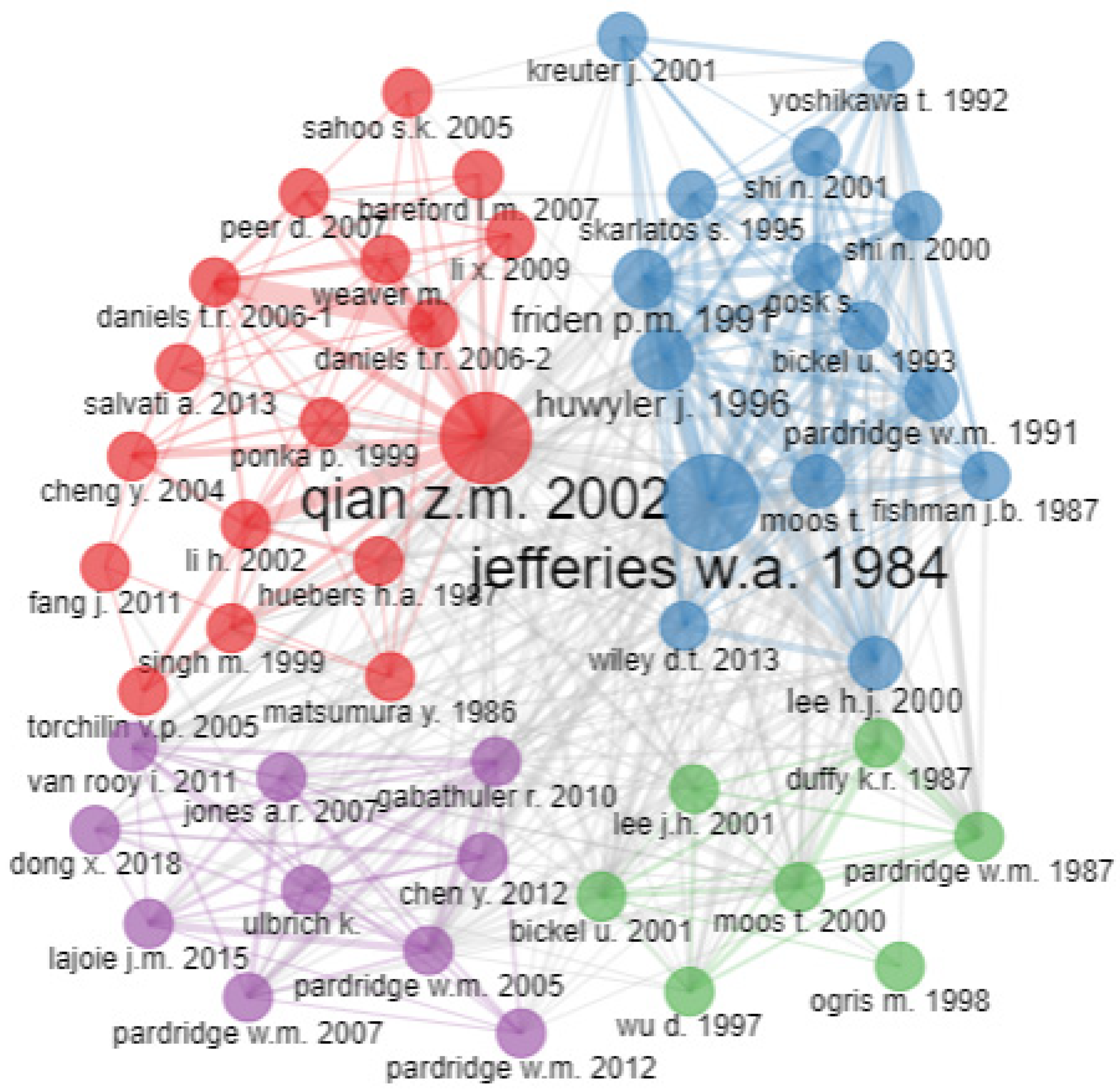
3.2.1. Co-Citation Analysis
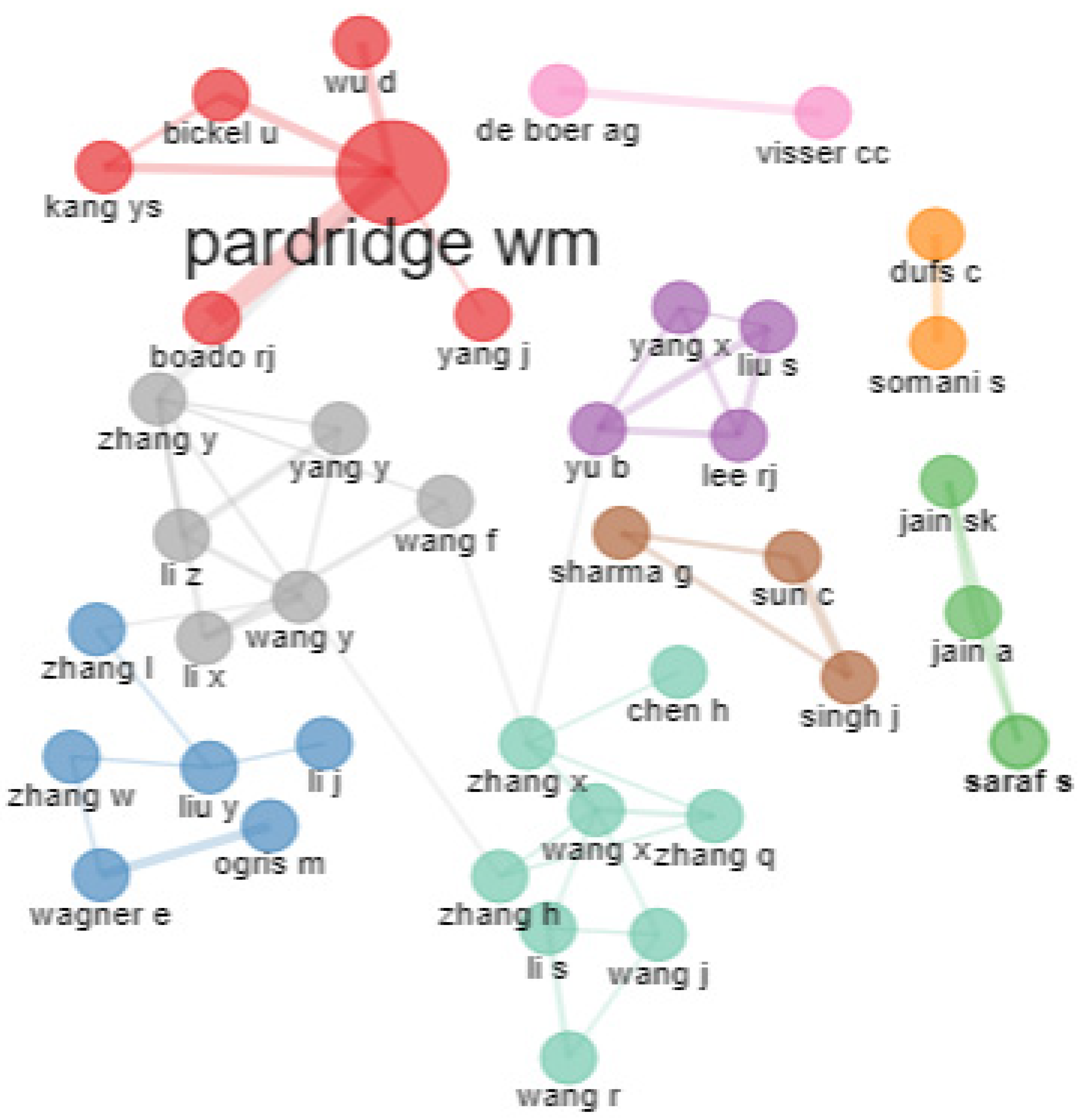
3.2.2. Bibliographic Coupling
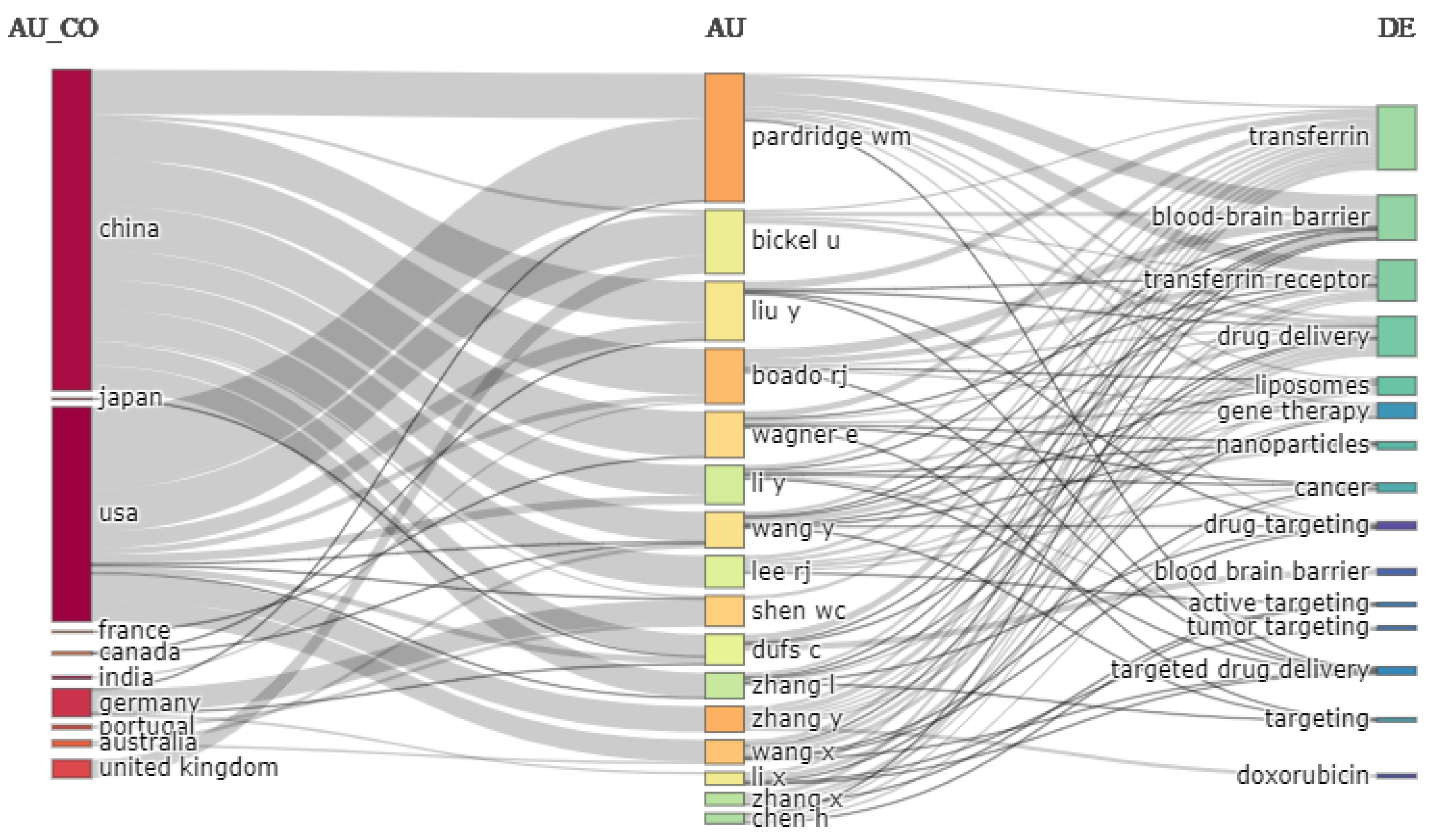
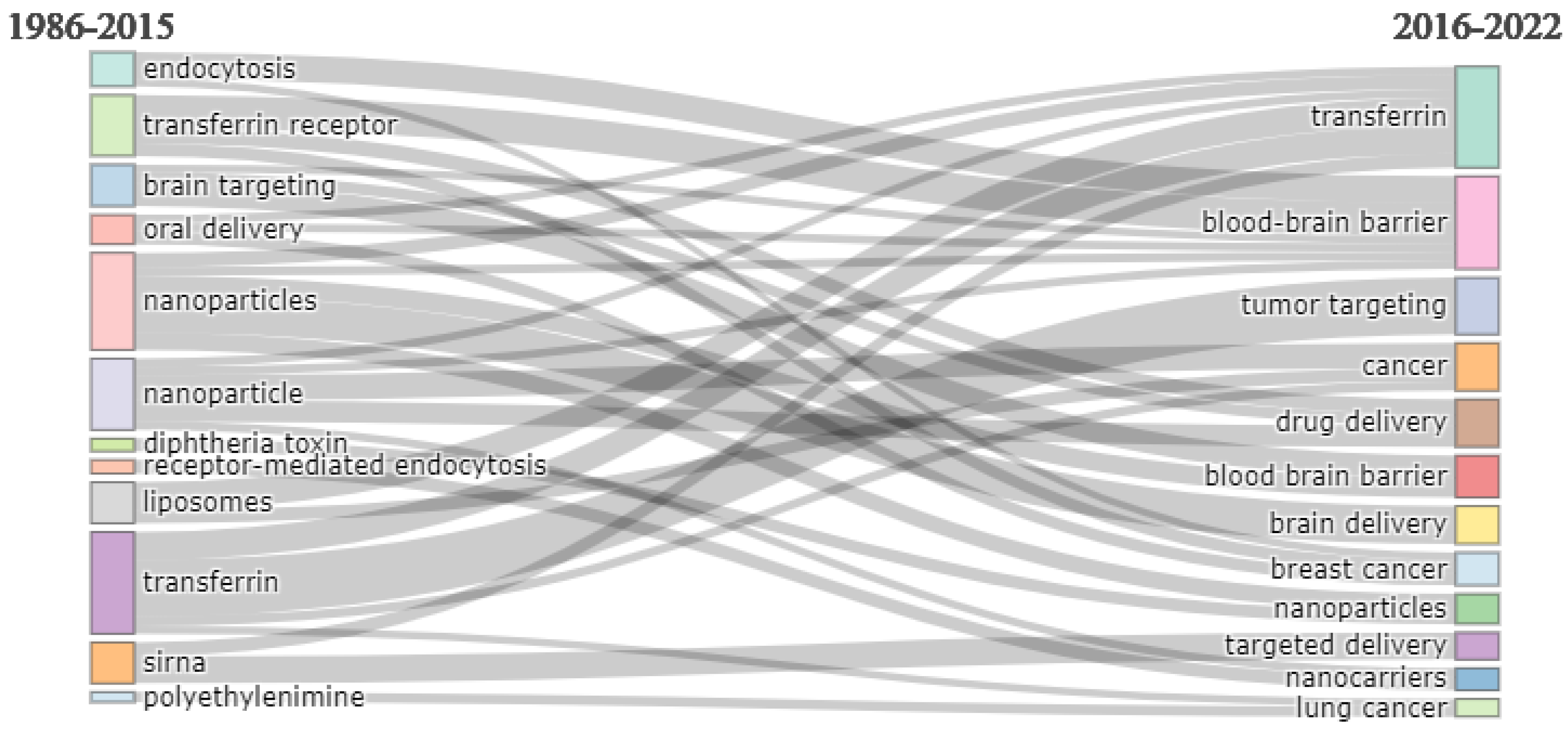
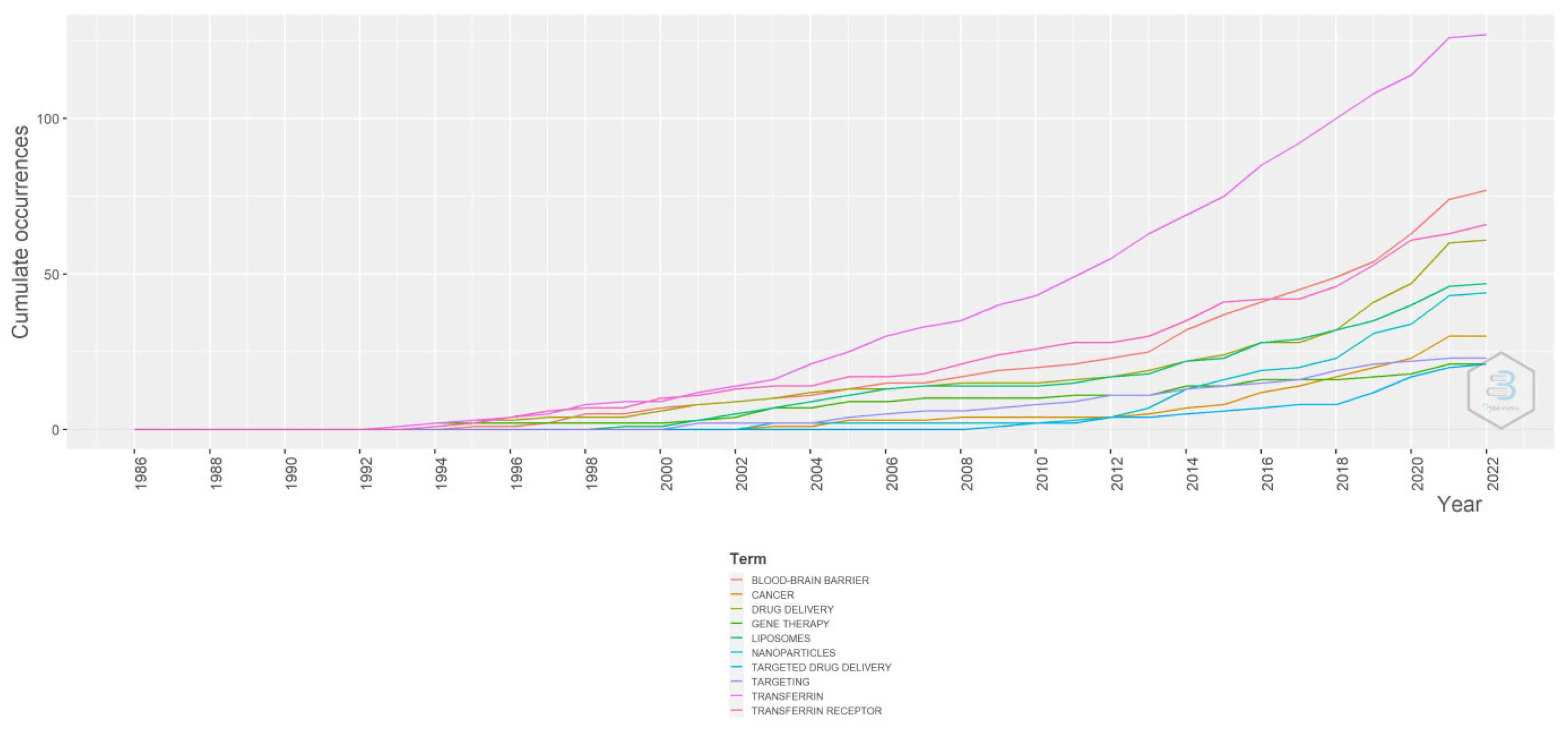
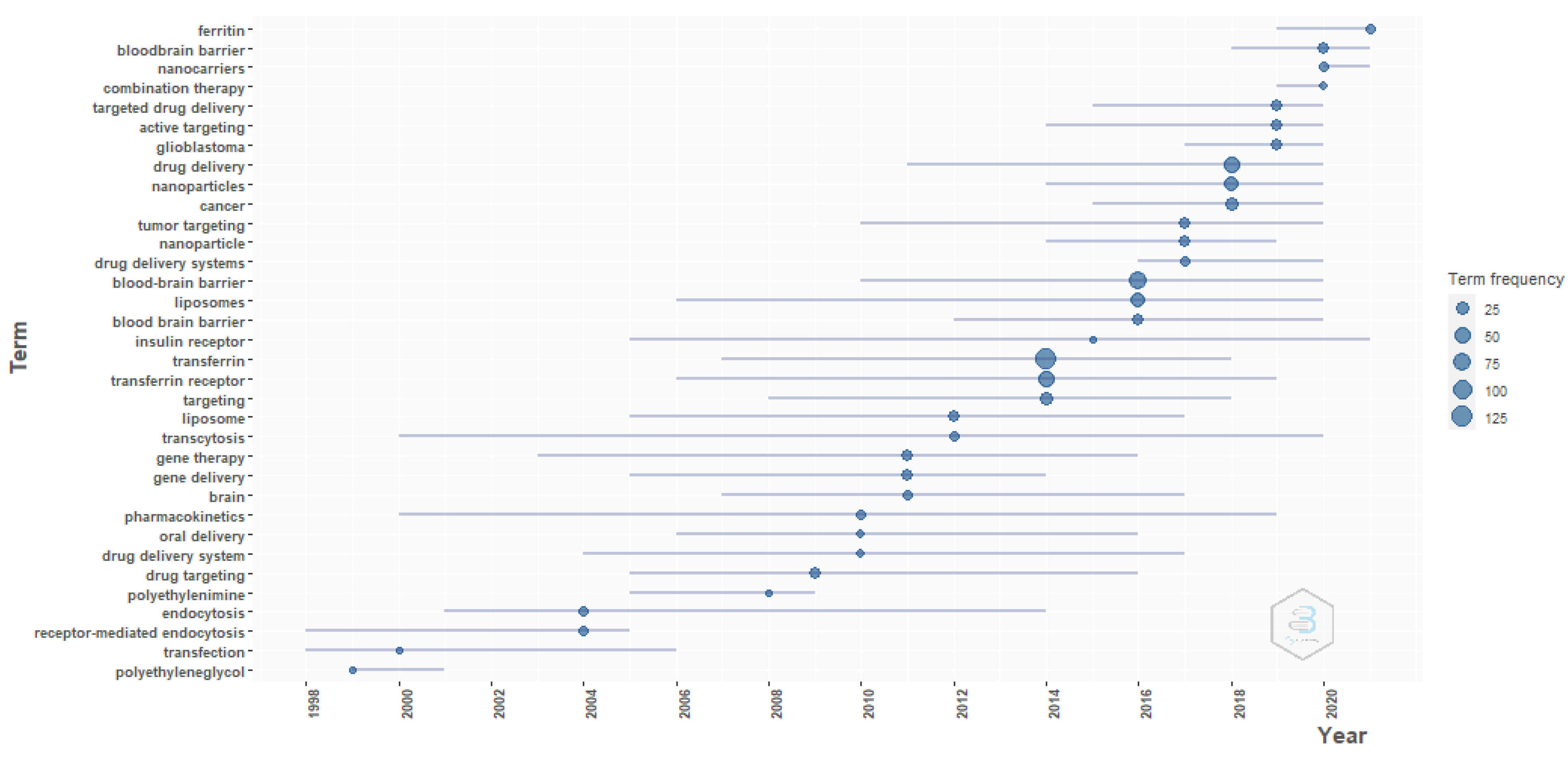
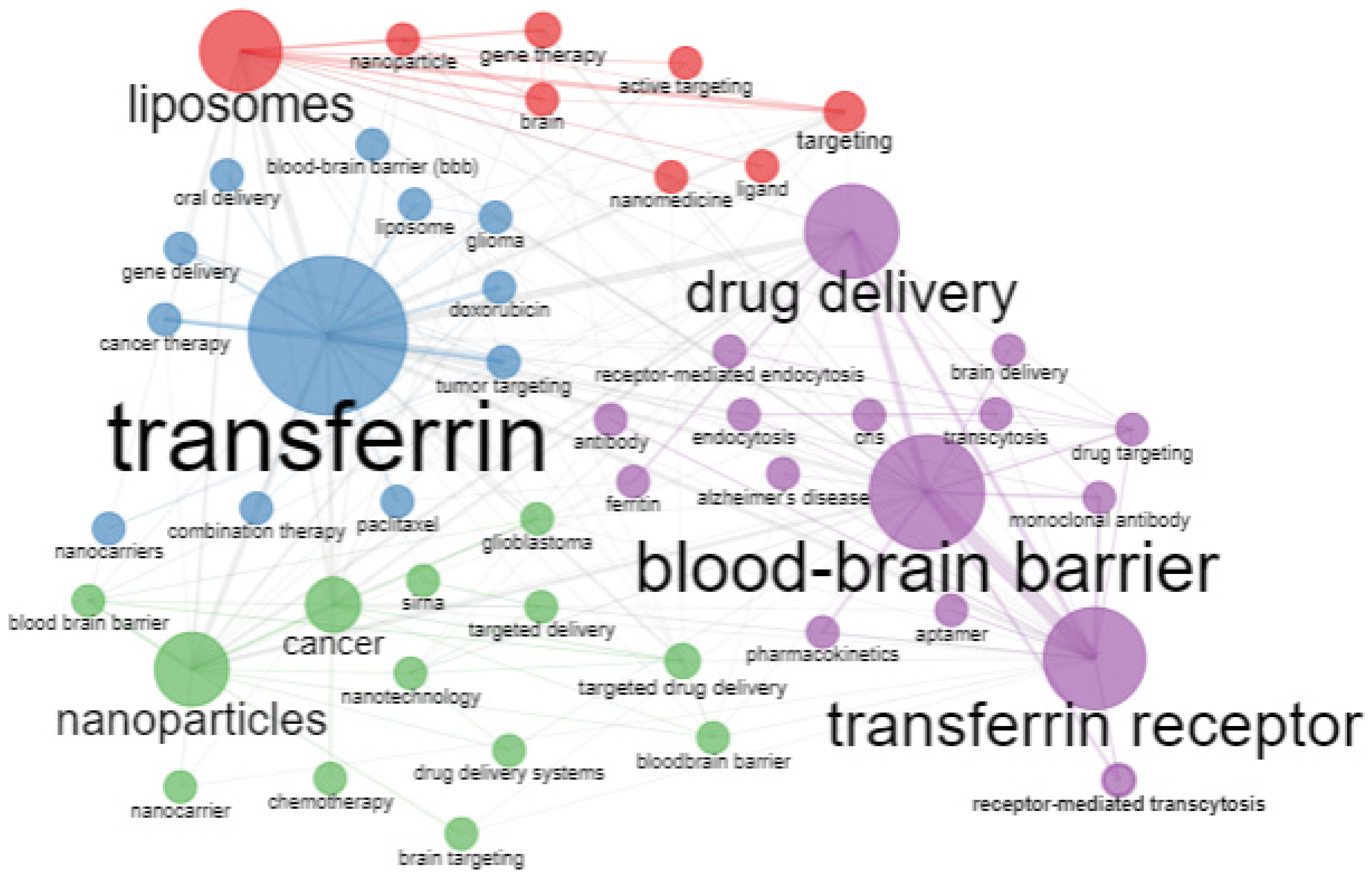
3.3. Word and Co-Word Analysis
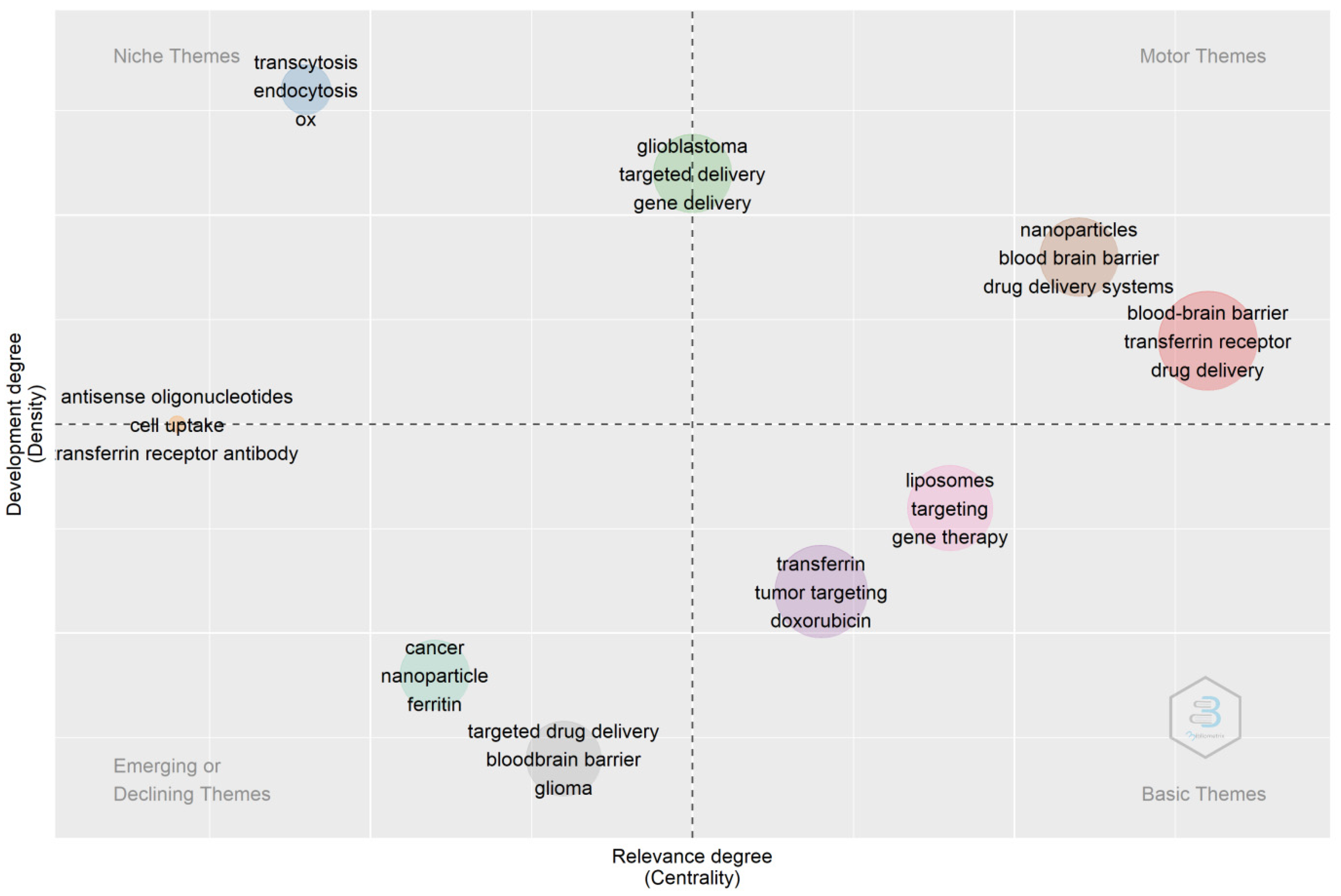
4. Thematic Analysis
4.1. Transferrin/Transferrin Receptor-Mediated Drug Delivery to the Brain
4.2. Transferrin/Transferrin Receptor-Mediated Gene Delivery
4.3. Transferrin/Transferrin Receptor-Mediated Drug Delivery to Cancer Cells
4.4. Transferrin/Transferrin Receptor-Mediated Drug Delivery Systems
4.4.1. Liposomes
4.4.2. Nanoparticles
5. Future Research Directions
- Although there has been an increase in the research on transferrin/transferrin receptor-mediated drug delivery systems, most existing studies were carried out in blood–brain barrier models or mouse or rat animal models. However, chronic treatment with anti-transferrin receptor monoclonal antibodies was found to have a low therapeutic index in Rhesus monkeys [55]. Therefore, preclinical studies in primate models are more suitable for future clinical investigation research.
- Transferrin receptors are highly expressed in the blood–brain barrier, liver, kidney, heart, spleen, and tumor cells [18]. The drug can also be present in high concentrations in other tissues when administered via the intravenous route. Therefore, histopathological and toxicological studies of peripheral tissues should be included in future research.
- Transferrin receptors are involved in the cellular uptake of iron, and iron is crucial to many biological functions [19]. Therefore, in future research targeting transferrin receptors for the delivery of therapeutic or diagnostic agents, the change in the fate of iron uptake should be evaluated.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mills, J.K.; Needham, D. Targeted Drug Delivery. Expert Opin. Ther. Pat. 1999, 9, 1499–1513. [Google Scholar] [CrossRef]
- Li, H.; Sun, H.; Qian, Z.M. The Role of the Transferrin–Transferrin-Receptor System in Drug Delivery and Targeting. Trends Pharmacol. Sci. 2002, 23, 206–209. [Google Scholar] [CrossRef]
- Dufès, C.; Al Robaian, M.; Somani, S. Transferrin and the Transferrin Receptor for the Targeted Delivery of Therapeutic Agents to the Brain and Cancer Cells. Ther. Deliv. 2013, 4, 629–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, T.R.; Bernabeu, E.; Rodríguez, J.A.; Patel, S.; Kozman, M.; Chiappetta, D.A.; Holler, E.; Ljubimova, J.Y.; Helguera, G.; Penichet, M.L. The Transferrin Receptor and the Targeted Delivery of Therapeutic Agents against Cancer. Biochim. Biophys. Acta-Gen. Subj. 2012, 1820, 291–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callens, C.; Moura, I.C.; Lepelletier, Y.; Coulon, S.; Renand, A.; Dussiot, M.; Ghez, D.; Benhamou, M.; Monteiro, R.C.; Bazarbachi, A.; et al. Recent Advances in Adult T-Cell Leukemia Therapy: Focus on a New Anti-Transferrin Receptor Monoclonal Antibody. Leukemia 2008, 22, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Voinea, M.; Dragomir, E.; Manduteanu, I.; Simionescu, M. Binding and Uptake of Transferrin-Bound Liposomes Targeted to Transferrin Receptors of Endothelial Cells. Vascul. Pharmacol. 2002, 39, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Prades, R.; Guerrero, S.; Araya, E.; Molina, C.; Salas, E.; Zurita, E.; Selva, J.; Egea, G.; López-Iglesias, C.; Teixidó, M.; et al. Delivery of Gold Nanoparticles to the Brain by Conjugation with a Peptide That Recognizes the Transferrin Receptor. Biomaterials 2012, 33, 7194–7205. [Google Scholar] [CrossRef] [PubMed]
- Steinlein, L.M.; Graf, T.N.; Ikeda, R.A. Production and Purification of N-Terminal Half-Transferrin in Pichia Pastoris. Protein Expr. Purif. 1995, 6, 619–624. [Google Scholar] [CrossRef]
- Kawabata, H. Transferrin and Transferrin Receptors Update. Free Radic. Biol. Med. 2019, 133, 46–54. [Google Scholar] [CrossRef]
- de Jong, G.; van Eijk, H.G. Microheterogeneity of Human Serum Transferrin: A Biological Phenomenon Studied by Isoelectric Focusing in Immobilized PH Gradients. Electrophoresis 1988, 9, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W. Transferrin Function in Zinc Absorption and Transport. Exp. Biol. Med. 1976, 151, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Cochran, M.; Coates, J.; Neoh, S. The Competitive Equilibrium between Aluminium and Ferric Ions for the Binding Sites of Transferrin. FEBS Lett. 1984, 176, 129–132. [Google Scholar] [CrossRef] [Green Version]
- Harris, W.R.; Madsen, L.J. Equilibrium Studies on the Binding of Cadmium(II) to Human Serum Transferrin. Biochemistry 2002, 27, 284–288. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.R.; Pecoraro, V.L. Thermodynamic Binding Constants for Gallium Transferrin. Biochemistry 2002, 22, 292–299. [Google Scholar] [CrossRef]
- Gomme, P.T.; Mccann, K.B.; Bertolini, J. Transferrin: Structure, Function and Potential Therapeutic Actions. Drug Discov. Today 2005, 10, 267–273. [Google Scholar] [CrossRef] [PubMed]
- MacGillivray, R.T.A.; Mendez, E.; Shewale, J.G.; Sinha, S.K.; Lineback-Zins, J.; Brew, K. The Primary Structure of Human Serum Transferrin. The Structures of Seven Cyanogen Bromide Fragments and the Assembly of the Complete Structure. J. Biol. Chem. 1983, 258, 3543–3553. [Google Scholar] [CrossRef]
- Bailey, S.; Evans, R.W.; Garratt, R.C.; Gorinskv, B.; Mydin, A.; Horsburg, C.; Jhoti, H.; Lindley, P.F.; Hasnain, S.; Sarra, R.; et al. Molecular Structure of Serum Transferrin at 3: 3-A Resolution. Biochemistry 1988, 27, 5804–5812. [Google Scholar] [CrossRef]
- Li, H.; Qian, Z.M. Transferrin/Transferrin Receptor-Mediated Drug Delivery. Med. Res. Rev. 2002, 22, 225–250. [Google Scholar] [CrossRef]
- de Jong, G.; van Dijk, J.P.; van Eijk, H.G. The Biology of Transferrin. Clin. Chim. Acta 1990, 190, 1–46. [Google Scholar] [CrossRef]
- Silva, A.M.N.; Moniz, T.; de Castro, B.; Rangel, M. Human Transferrin: An Inorganic Biochemistry Perspective. Coord. Chem. Rev. 2021, 449, 214186. [Google Scholar] [CrossRef]
- Macedo, M.F.; de Sousa, M. Transferrin and the Transferrin Receptor: Of Magic Bullets and Other Concerns. Inflamm. Allergy-Drug Targets 2008, 7, 41–52. [Google Scholar] [CrossRef]
- Mason, D.Y.; Taylor, C.R. Distribution of Transferrin, Ferritin, and Lactoferrin in Human Tissues. J. Clin. Pathol. 1978, 31, 316–327. [Google Scholar] [CrossRef] [Green Version]
- Huebers, H.A.; Finch, C.A. The Physiology of Transferrin and Transferrin Receptors. Physiol. Rev. 1987, 67, 520–582. [Google Scholar] [CrossRef]
- Rossiello, R.; Carriero, M.V.; Giordano, G.G. Distribution of Ferritin, Transferrin and Lactoferrin in Breast Carcinoma Tissue. J. Clin. Pathol. 1984, 37, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Larsen, B.; Snyder, I.S.; Galask, R.P. Transferrin Concentration in Human Amniotic Fluid. Am. J. Obstet. Gynecol. 1973, 117, 952–954. [Google Scholar] [CrossRef]
- Murakami, Y.; Saito, K.; Ito, H.; Hashimoto, Y. Transferrin Isoforms in Cerebrospinal Fluid and Their Relation to Neurological Diseases. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2019, 95, 198–210. [Google Scholar] [CrossRef] [Green Version]
- Rahmanto, Y.S.; Bal, S.; Loh, K.H.; Yu, Y.; Richardson, D.R. Melanotransferrin: Search for a Function. Biochim. Biophys. Acta-Gen. Subj. 2012, 1820, 237–243. [Google Scholar] [CrossRef]
- Yu, Y.; Jiang, L.; Wang, H.; Shen, Z.; Cheng, Q.; Zhang, P.; Wang, J.; Wu, Q.; Fang, X.; Duan, L.; et al. Hepatic Transferrin Plays a Role in Systemic Iron Homeostasis and Liver Ferroptosis. Blood 2020, 136, 726–739. [Google Scholar] [CrossRef]
- Ponka, P.; Lok, C.N. The Transferrin Receptor : Role in Health and Disease. Int. J. Biochem. Cell Biol. 1999, 31, 1111–1137. [Google Scholar] [CrossRef]
- Speeckaert, M.M.; Speeckaert, R.; Delanghe, J.R. Biological and Clinical Aspects of Soluble Transferrin Receptor. Crit. Rev. Clin. Lab. Sci. 2010, 47, 213–228. [Google Scholar] [CrossRef]
- Skikne, B.S. Serum Transferrin Receptor. Am. J. Hematol. 2008, 83, 872–875. [Google Scholar] [CrossRef] [PubMed]
- Gammella, E.; Buratti, P.; Cairo, G.; Recalcati, S. The Transferrin Receptor: The Cellular Iron Gate. Metallomics 2017, 9, 1367–1375. [Google Scholar] [CrossRef]
- Aisen, P. Transferrin Receptor 1. Int. J. Biochem. Cell Biol. 2004, 36, 2137–2143. [Google Scholar] [CrossRef] [PubMed]
- Pantopoulos, K. Iron Metabolismo and the IRE/IRP Regulation System. Ann. N. Y. Acad. Sci. 2004, 1012, 1–13. [Google Scholar] [CrossRef]
- Kawabata, H.; Nakamaki, T.; Ikonomi, P.; Smith, R.D.; Germain, R.S.; Phillip Koeffler, H. Expression of Transferrin Receptor 2 in Normal and Neoplastic Hematopoietic Cells. Blood 2001, 98, 2714–2719. [Google Scholar] [CrossRef] [PubMed]
- Roetto, A.; Mezzanotte, M.; Pellegrino, R.M. The Functional Versatility of Transferrin Receptor 2 and Its Therapeutic Value. Pharmaceuticals 2018, 11, 115. [Google Scholar] [CrossRef] [Green Version]
- Trinder, D.; Baker, E. Transferrin Receptor 2: A New Molecule in Iron Metabolism. Int. J. Biochem. Cell Biol. 2003, 35, 292–296. [Google Scholar] [CrossRef]
- Verma, S.; Gustafsson, A. Investigating the Emerging COVID-19 Research Trends in the Field of Business and Management: A Bibliometric Analysis Approach. J. Bus. Res. 2020, 118, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Donthu, N.; Kumar, S.; Mukherjee, D.; Pandey, N.; Lim, W.M. How to Conduct a Bibliometric Analysis: An Overview and Guidelines. J. Bus. Res. 2021, 133, 285–296. [Google Scholar] [CrossRef]
- Aparicio, G.; Iturralde, T.; Maseda, A. Conceptual Structure and Perspectives on Entrepreneurship Education Research: A Bibliometric Review. Eur. Res. Manag. Bus. Econ. 2019, 25, 105–113. [Google Scholar] [CrossRef]
- Pinto, G.; Rastogi, S.; Kadam, S.; Sharma, A. Bibliometric Study on Dividend Policy. Qual. Res. Financ. Mark. 2020, 12, 72–95. [Google Scholar] [CrossRef]
- Aria, M.; Cuccurullo, C. Bibliometrix: An R-Tool for Comprehensive Science Mapping Analysis. J. Informetr. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- Uluyol, B.; Secinaro, S.; Calandra, D.; Lanzalonga, F. Mapping Waqf Research: A Thirty-Year Bibliometric Analysis. J. Islam. Account. Bus. Res. 2021, 12, 748–767. [Google Scholar] [CrossRef]
- Mongeon, P.; Paul-Hus, A. The Journal Coverage of Web of Science and Scopus: A Comparative Analysis. Scientometrics 2015, 106, 213–228. [Google Scholar] [CrossRef]
- Romasanta, A.K.S.; van der Sijde, P.; Hellsten, I.; Hubbard, R.E.; Keseru, G.M.; van Muijlwijk-Koezen, J.; de Esch, I.J.P. When Fragments Link: A Bibliometric Perspective on the Development of Fragment-Based Drug Discovery. Drug Discov. Today 2018, 23, 1596–1609. [Google Scholar] [CrossRef]
- Brimo Alsaman, M.Z.; Sallah, H.; Badawi, R.; Ghawi, A.; Shashaa, M.N.; Kassem, L.H.; Ghazal, A. Syrian Medical, Dental and Pharmaceutical Publication in the Last Decade: A Bibliometric Analysis. Ann. Med. Surg. 2021, 66, 102441. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Kuang, L.; Zhao, J.; Ross, A.E.; Wang, Z.; Ciolino, J.B. Bibliometric and Visualized Analysis of Ocular Drug Delivery from 2001 to 2020. J. Control. Release 2022, 345, 625–645. [Google Scholar] [CrossRef]
- Huang, Z.; Zhang, X.; Wu, L.; Hu, P.; Huang, Y.; Pan, X.; Wu, C. Progress on Pharmaceutical Sciences/Pharmacy Postgraduate Education: A Bibliometric Perspective. J. Pharm. Innov. 2022, 1–13. [Google Scholar] [CrossRef]
- Lungwitz, U.; Breunig, M.; Blunk, T.; Göpferich, A. Polyethylenimine-Based Non-Viral Gene Delivery Systems. Eur. J. Pharm. Biopharm. 2005, 60, 247–266. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.E. The first targeted delivery of siRNA in humans via a self-assembling, cyclodextrin polymer-based nanoparticle: From concept to clinic. Mol. Pharm. 2009, 6, 659–668. [Google Scholar] [CrossRef]
- Bickel, U.; Yoshikawa, T.; Pardridge, W.M. Delivery of Peptides and Proteins through the Blood-Brain Barrier. Adv. Drug Deliv. Rev. 1993, 10, 205–245. [Google Scholar] [CrossRef]
- Walus, L.R.; Pardridge, W.M.; Starzyk, R.M.; Friden, P.M. Enhanced Uptake of RsCD4 across the Rodent and Primate Blood-Brain Barrier after Conjugation to Anti-Transferrin Receptor Antibodies. J. Pharmacol. Exp. Ther. 1996, 277, 1067–1075. [Google Scholar]
- Friden, P.M.; Olson, T.S.; Obar, R.; Walus, L.R.; Putney, S.D. Characterization, Receptor Mapping and Blood-Brain Barrier Transcytosis of Antibodies to the Human Transferrin Receptor. J. Pharmacol. Exp. Ther. 1996, 278, 1491–1498. [Google Scholar] [PubMed]
- Song, B.W.; Vinters, H.V.; Wu, D.; Pardridge, W.M. Enhanced Neuroprotective Effects of Basic Fibroblast Growth Factor in Regional Brain Ischemia after Conjugation to a Blood-Brain Barrier Delivery Vector. J. Pharmacol. Exp. Ther. 2002, 301, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Pardridge, W.M.; Boado, R.J.; Patrick, D.J.; Hui, E.K.W.; Lu, J.Z. Blood-Brain Barrier Transport, Plasma Pharmacokinetics, and Neuropathology Following Chronic Treatment of the Rhesus Monkey with a Brain Penetrating Humanized Monoclonal Antibody Against the Human Transferrin Receptor. Mol. Pharm. 2018, 15, 5207–5216. [Google Scholar] [CrossRef]
- Shi, N.; Boado, R.J.; Pardridge, W.M. Receptor-Mediated Gene Targeting to Tissues In Vivo Following Pegylated Immunoliposomes. In Vivo (Brooklyn) 2001, 18, 2–6. [Google Scholar]
- Zhang, Y.; Zhu, C.; Pardridge, W.M. Antisense Gene Therapy of Brain Cancer with an Artificial Virus Gene Delivery System. Mol. Ther. 2002, 6, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Koppu, S.; Oh, Y.J.; Edrada-Ebel, R.A.; Blatchford, D.R.; Tetley, L.; Tate, R.J.; Dufès, C. Tumor Regression after Systemic Administration of a Novel Tumor-Targeted Gene Delivery System Carrying a Therapeutic Plasmid DNA. J. Control. Release 2010, 143, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Dos, B.; Rodrigues, S.; Lakkadwala, S.; Kaneko, T.; Singh, J. Dual-Modified Liposome for Targeted and Enhanced Gene Delivery into Mice Brain. J. Pharmacol. Exp. Ther. 2020, 374, 354–365. [Google Scholar] [CrossRef]
- Lim, C.J.; Shen, W.C. Transferrin-Oligomers as Potential Carriers in Anticancer Drug Delivery. Pharm. Res. 2004, 21, 1985–1992. [Google Scholar] [CrossRef]
- Nie, Y.; Schaffert, D.; Rödl, W.; Ogris, M.; Wagner, E.; Günther, M. Dual-Targeted Polyplexes: One Step towards a Synthetic Virus for Cancer Gene Therapy. J. Control. Release 2011, 152, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Ge, P.; Liu, Y.; Chen, Q.; Su, Z.; Du, Y.; Luo, S.; Zhao, X.; Cao, X.; Song, H.; Zhu, X. Transferrin Receptors/Magnetic Resonance Dual-Targeted Nano platform for Precise Chemo-Photodynamic Synergistic Cancer Therapy. Nanomed. Nanotechnol. Biol. Med. 2022, 39, 102467. [Google Scholar] [CrossRef]
- Micklus, M.J.; Greig, N.H.; Tung, J.; Rapoport, S.I. Targeting of Liposomes to the Blood-Brain Barrier in Rats. Drug Deliv. 2008, 1, 21–26. [Google Scholar] [CrossRef]
- Maruyama, K.; Ishida, O.; Takizawa, T.; Moribe, K. Possibility of Active Targeting to Tumor Tissues with Liposomes. Adv. Drug Deliv. Rev. 1999, 40, 89–102. [Google Scholar] [CrossRef]
- Huwyler, J.; Yang, J.; Pardridge, W.M. Receptor-Mediated Delivery of Daunomycin Using Immunoliposomes: Pharmacokinetics and Tissue Distribution in the Rat. J. Pharmacol. Exp. Ther. 1997, 282, 1541–1546. [Google Scholar]
- Tsai, H.E.; Liu, L.F.; Dusting, G.J.; Weng, W.T.; Chen, S.C.; Kung, M.L.; Tee, R.; Liu, G.-S.; Tai, M.-H. Pro-Opiomelanocortin Gene Delivery Suppresses the Growth of Established Lewis Lung Carcinoma through a Melanocortin-1 Receptor-Independent Pathway. J. Gene Med. 2012, 14, 44–53. [Google Scholar] [CrossRef]
- Sharma, G.; Modgil, A.; Sun, C.; Singh, J. Grafting of Cell-Penetrating Peptide to Receptor-Targeted Liposomes Improves Their Transfection Efficiency and Transport across Blood-Brain Barrier Model. J. Pharm. Sci. 2012, 101, 2468–2478. [Google Scholar] [CrossRef] [PubMed]
- De Luca, M.A.; Lai, F.; Corrias, F.; Caboni, P.; Bimpisidis, Z.; Maccioni, E.; Fadda, A.M.; Di Chiara, G. Lactoferrin- and Antitransferrin-Modified Liposomes for Brain Targeting of the NK3 Receptor Agonist Senktide: Preparation and in Vivo Evaluation. Int. J. Pharm. 2015, 479, 129–137. [Google Scholar] [CrossRef]
- Yuan, Q.; Zhao, L. The Mulberry (Morus Alba L.) Fruit—A Review of Characteristic Components and Health Benefits. J. Agric. Food Chem. 2017, 65, 10383–10394. [Google Scholar] [CrossRef]
- Sriraman, S.K.; Salzano, G.; Sarisozen, C.; Torchilin, V. Anti-Cancer Activity of Doxorubicin-Loaded Liposomes Co-Modified with Transferrin and Folic Acid. Eur. J. Pharm. Biopharm. 2016, 105, 40–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadia, K.; Markoutsa, E.; Mourtas, S.; Giannou, A.D.; La Ferla, B.; Nicotra, F.; Salmona, M.; Klepetsanis, P.; Stathopoulos, G.T.; Antimisiaris, S.G. Multifunctional LUV. Liposomes Decorated for B.B.B. and Amyloid Targeting. A. In Vitro Proof-of-Concept. Eur. J. Pharm. Sci. 2017, 101, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Mojarad-Jabali, S.; Farshbaf, M.; Hemmati, S.; Sarfraz, M.; Motasadizadeh, H.; Shahbazi Mojarrad, J.; Atyabi, F.; Zakeri-Milani, P.; Valizadeh, H. Comparison of Three Synthetic Transferrin Mimetic Small Peptides to Promote the Blood–Brain Barrier Penetration of Vincristine Liposomes for Improved Glioma Targeted Therapy. Int. J. Pharm. 2022, 613, 121395. [Google Scholar] [CrossRef] [PubMed]
- Bhagwat, G.S.; Athawale, R.B.; Gude, R.P.; Md, S.; Alhakamy, N.A.; Fahmy, U.A.; Kesharwani, P. Formulation and Development of Transferrin Targeted Solid Lipid Nanoparticles for Breast Cancer Therapy. Front. Pharmacol. 2020, 11, 2064. [Google Scholar] [CrossRef] [PubMed]
- Kuang, Y.; An, S.; Guo, Y.; Huang, S.; Shao, K.; Liu, Y.; Li, J.; Ma, H.; Jiang, C. T7 Peptide-Functionalized Nanoparticles Utilizing R.N.A. Interference for Glioma Dual Targeting. Int. J. Pharm. 2013, 454, 11–20. [Google Scholar] [CrossRef]
- Moglia, I.; Santiago, M.; Guerrero, S.; Soler, M.; Olivera-Nappa, A.; Kogan, M.J. Enhanced Cellular Uptake of H-Chain Human Ferritin Containing Gold Nanoparticles. Pharmaceutics 2021, 13, 1966. [Google Scholar] [CrossRef]
- Olivier, J.C.; Huertas, R.; Hwa, J.L.; Calon, F.; Pardridge, W.M. Synthesis of Pegylated Immunonanoparticles. Pharm. Res. 2002, 19, 1137–1143. [Google Scholar] [CrossRef]
- Pinheiro, R.G.R.; Granja, A.; Loureiro, J.A.; Pereira, M.C.; Pinheiro, M.; Neves, A.R.; Reis, S. Quercetin Lipid Nanoparticles Functionalized with Transferrin for Alzheimer’s Disease. Eur. J. Pharm. Sci. 2020, 148, 105314. [Google Scholar] [CrossRef]
- Yoon, S.; Kim, Y.; Youn, Y.S.; Oh, K.T.; Kim, D.; Lee, E.S. Transferrin-Conjugated PH-Responsive γ-Cyclodextrin Nanoparticles for Antitumoral Topotecan Delivery. Pharmaceutics 2020, 12, 1109. [Google Scholar] [CrossRef]
- Zheng, Y.; Yu, B.; Weecharangsan, W.; Piao, L.; Darby, M.; Mao, Y.; Koynova, R.; Yang, X.; Li, H.; Xu, S.; et al. Transferrin-Conjugated Lipid-Coated PLGA Nanoparticles for Targeted Delivery of Aromatase Inhibitor 7α-APTADD to Breast Cancer Cells. Int. J. Pharm. 2010, 390, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Jain, A.; Chase, G.; Singh, S.K.; Saxena, A.K.; Jain, S.K. Transferrin-Appended PEGylated Nanoparticles for Temozolomide Delivery to Brain: In Vitro Characterisation. J. Microencapsul. 2010, 28, 21–28. [Google Scholar] [CrossRef]
- Lei, Y.; Hamada, Y.; Li, J.; Cong, L.; Wang, N.; Li, Y.; Zheng, W.; Jiang, X. Targeted Tumor Delivery and Controlled Release of Neuronal Drugs with Ferritin Nanoparticles to Regulate Pancreatic Cancer Progression. J. Control. Release 2016, 232, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ogris, M.; Wagner, E.; Pelisek, J.; Rüffer, M. Nanoparticles Bearing Polyethyleneglycol-Coupled Transferrin as Gene Carriers: Preparation and in Vitro Evaluation. Int. J. Pharm. 2003, 259, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Dixit, S.; Miller, K.; Zhu, Y.; McKinnon, E.; Novak, T.; Kenney, M.E.; Broome, A.M. Dual Receptor-Targeted Theranostic Nanoparticles for Localized Delivery and Activation of Photodynamic Therapy Drug in Glioblastomas. Mol. Pharm. 2015, 12, 3250. [Google Scholar] [CrossRef] [PubMed]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Results |
|---|---|
| Main information about the data | |
| Timespan | 1986–2022 |
| Sources (journals, books, etc.) | 130 |
| Documents | 583 |
| Average years from publication | 9.23 |
| Average citations per document | 50.04 |
| Average citations per year per doc | 4.87 |
| References | 41,320 |
| Document Types | |
| Article | 398 |
| Book chapter | 10 |
| Conference paper | 14 |
| Editorial | 7 |
| Note | 2 |
| Review | 145 |
| Short survey | 3 |
| Document Contents | |
| Keywords plus ID | 6002 |
| Author’s keywords (DE) | 1365 |
| Authors | |
| Authors | 2245 |
| Author appearances | 3148 |
| Authors of single-authored documents | 26 |
| Authors of multi-authored documents | 2219 |
| Author Collaboration | |
| Single-authored documents | 34 |
| Documents per author | 0.256 |
| Authors per document | 3.91 |
| Co-authors per document | 5.48 |
| Collaboration index | 4.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaur, T.; Upadhyay, J.; Pukale, S.; Mathur, A.; Ansari, M.N. Investigation of Trends in the Research on Transferrin Receptor-Mediated Drug Delivery via a Bibliometric and Thematic Analysis. Pharmaceutics 2022, 14, 2574. https://doi.org/10.3390/pharmaceutics14122574
Kaur T, Upadhyay J, Pukale S, Mathur A, Ansari MN. Investigation of Trends in the Research on Transferrin Receptor-Mediated Drug Delivery via a Bibliometric and Thematic Analysis. Pharmaceutics. 2022; 14(12):2574. https://doi.org/10.3390/pharmaceutics14122574
Chicago/Turabian StyleKaur, Tarnjot, Jyoti Upadhyay, Sudeep Pukale, Ashish Mathur, and Mohd Nazam Ansari. 2022. "Investigation of Trends in the Research on Transferrin Receptor-Mediated Drug Delivery via a Bibliometric and Thematic Analysis" Pharmaceutics 14, no. 12: 2574. https://doi.org/10.3390/pharmaceutics14122574
APA StyleKaur, T., Upadhyay, J., Pukale, S., Mathur, A., & Ansari, M. N. (2022). Investigation of Trends in the Research on Transferrin Receptor-Mediated Drug Delivery via a Bibliometric and Thematic Analysis. Pharmaceutics, 14(12), 2574. https://doi.org/10.3390/pharmaceutics14122574