

Oral Pharmacokinetics of Hydroxycinnamic Acids: An Updated Review
 , ,
, , 
Abstract
:1. Introduction
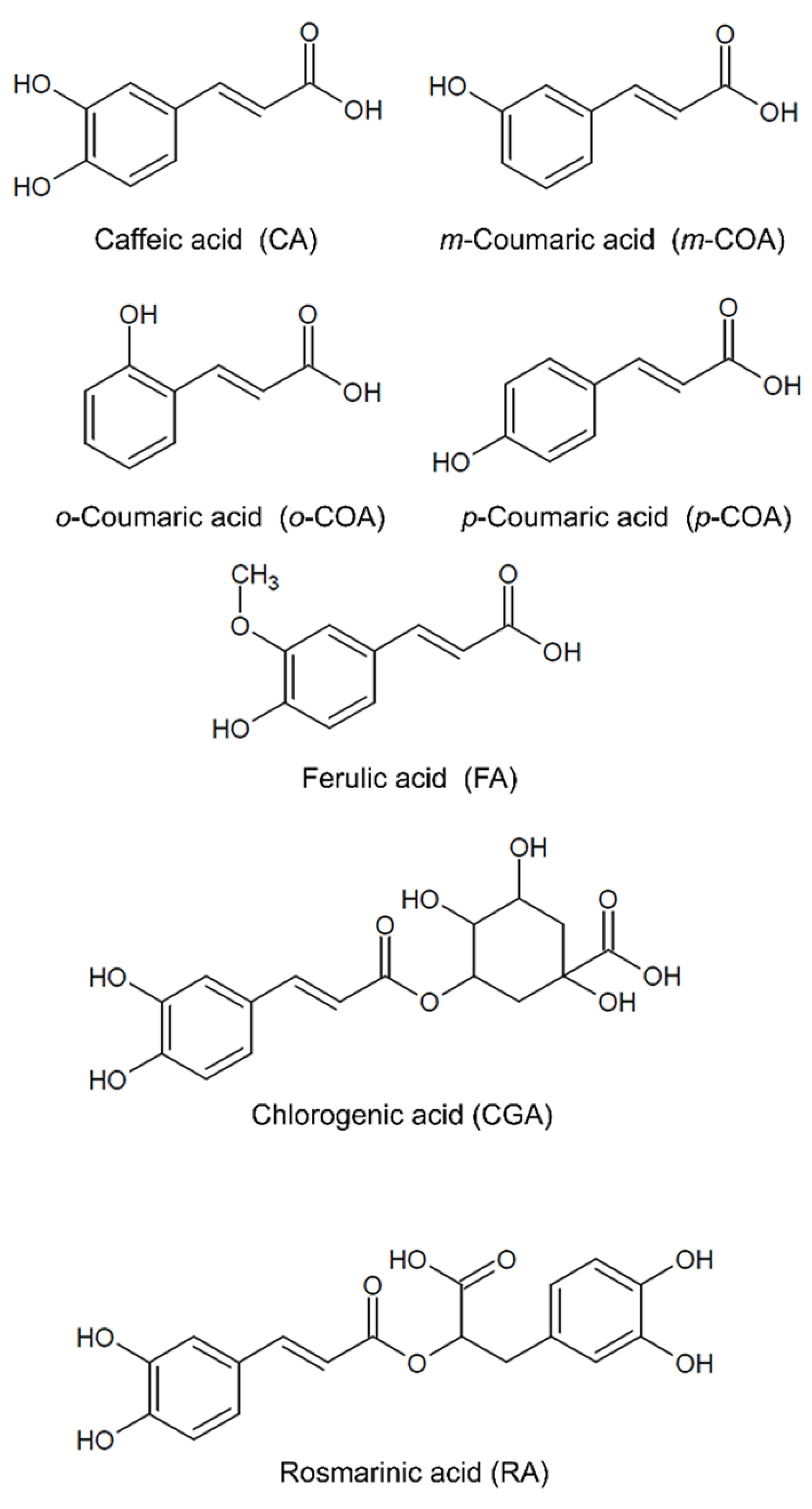
2. Water Solubility of Hydroxycinnamic Acids (HCAs)

{kind=link}
{kind=link}
{kind=link}
| HCA | MW (g/mol) | Water Solubility (mg/mL) a | pKa | Log P | Log D (pH 7.4) | PSA (Å) | HBD | HBA | RB | References |
|---|---|---|---|---|---|---|---|---|---|---|
| CA | 180 | 0.178 (pH 7.4) 0.188 (pH 6.5) 0.300 (25 °C) 0.420 (pH 3) 0.550 (pH 3.42/15 °C) 0.980 (pH 3.37/25 °C) 1.230 (pH 3.34/30 °C) 1.770 (37 °C) 2.040 (pH 3.25/40 °C) 2.920 (pH 3.17/50 °C) 6.510 (pH 7.2) | 4.36–4.70 7.60–9.46 11.17–11.85 | 0.93–4.60 | −1.78–1.74 | 77.75–81.00 | 3 | 4 | 2 | [28,29,31,32,33,34,35,36,37,38,39,40,41] |
| CGA | 354 | 40.000 (25 °C) | 3.33 7.8–8.26 | −0.45 | −3.91–3.57 | 164.74 | 6 | 9 | 5 | [31,40,42,43,44,45,46] |
| m-COA | 164 | 1.540 (25 °C) | 4.48–4.60 10.35–10.39 | 1.83 | −1.34 | 57.53 | 2 b | 3 b | 2 b | [38,39,47,48,49] |
| o-COA | 164 | 0.490 (25 °C) | 4.00–4.13 9.58–9.60 | 1.5 | N.A. | 57.53 | 2 | 3 | 2 b | [47,48,49,50] |
| p-COA | 164 | 0.344 (25 °C) 0.700 (37 °C) | 4.36–4.70 8.84–9.92 | 1.43–4.45 | −1.32 | 56.20–57.50 | 2 | 3 | 2 | [32,33,38,40,47,51,52] |
| FA | 194 | 0.333 (25 °C) 0.454 (25 °C) 0.570 (pH 3.54/15 °C) 0.710 (pH 3) 0.780 (pH 3.46/25 °C) 0.920 (pH 3.40/30 °C) 0.950 (pH 3.40/30 °C) 1.490 (37 °C) 1.760 (pH 3.31/40 °C) 2.190 (pH 3.18/50 °C) 5.420 (pH 7.4) 6.630 (pH 7.2) | 4.58–4.96 9.68–9.99 | 1.25–4.12 | −1.38–1.23 | 66.80 | 2 | 4 | 3 | [29,32,33,36,38,39,40,41,50,51,52,53,54] |
| RA | 360 | 1.800 (pH 1.2/ 25 °C) | 2.92 8.36 9.56 10.62 | 1.63–1.78 | −2.45 | 144.52–145.00 | 5 | 8 | 7 | [39,55,56,57,58] |
3. Stability of Hydroxycinnamic Acids (HCAs)
4. Absorption, Distribution, Metabolism and Elimination (ADME) of Hydroxycinnamic Acids (HCAs)
4.1. In Vitro Studies
4.1.1. Absorption
4.1.2. Metabolism
4.2. Ex Vivo Studies
4.3. In Situ Studies
4.4. In Vivo Studies
4.4.1. Absorption
4.4.2. Distribution
4.4.3. Metabolism
4.4.4. Elimination
4.4.5. Absolute Oral Bioavailability
5. Strategies to Improve Oral Bioavailability
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Razzaghi-Asl, N.; Garrido, J.; Khazraei, H.; Borges, F.; Firuzi, O. Antioxidant Properties of Hydroxycinnamic Acids: A Review of Structure-Activity Relationships. Curr. Med. Chem. 2013, 20, 4436–4450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha, L.D.; Monteiro, M.C.; Teodoro, A.J. Anticancer Properties of Hydroxycinnamic Acids—A Review. Cancer Clin. Oncol. 2012, 1, 109–121. [Google Scholar] [CrossRef]
- Taofiq, O.; González-Paramás, A.M.; Barreiro, M.F.; Ferreira, I.C.F.R.; McPhee, D.J. Hydroxycinnamic Acids and Their Derivatives: Cosmeceutical Significance, Challenges and Future Perspectives, a Review. Molecules 2017, 22, 281. [Google Scholar] [CrossRef] [PubMed]
- Amoah, S.K.S.; Sandjo, L.P.; Kratz, J.M.; Biavatti, M.W. Rosmarinic Acid—Pharmaceutical and Clinical Aspects. Planta Med. 2016, 82, 388–406. [Google Scholar] [CrossRef] [Green Version]
- Pei, K.; Ou, J.; Huang, J.; Ou, S. P-Coumaric Acid and Its Conjugates: Dietary Sources, Pharmacokinetic Properties and Biological Activities. J. Sci. Food Agric. 2016, 96, 2952–2962. [Google Scholar] [CrossRef]
- Tajik, N.; Tajik, M.; Mack, I.; Enck, P. The Potential Effects of Chlorogenic Acid, the Main Phenolic Components in Coffee, on Health: A Comprehensive Review of the Literature. Eur. J. Nutr. 2017, 56, 2215–2244. [Google Scholar] [CrossRef]
- Magnani, C.; Isaac, V.L.B.; Correa, M.A.; Salgado, H.R.N. Caffeic Acid: A Review of Its Potential Use in Medications and Cosmetics. Anal. Methods 2014, 6, 3203–3210. [Google Scholar] [CrossRef]
- Kumar, N.; Pruthi, V. Potential Applications of Ferulic Acid from Natural Sources. Biotechnol. Rep. 2014, 4, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Alagawany, M.; Abd El-Hack, M.E.; Farag, M.R.; Gopi, M.; Karthik, K.; Malik, Y.S.; Dhama, K. Rosmarinic Acid: Modes of Action, Medicinal Values and Health Benefits. Anim. Health Res. Rev. 2017, 18, 1–10. [Google Scholar] [CrossRef]
- Fachel, F.N.S.; Schuh, R.S.; Veras, K.S.; Bassani, V.L.; Koester, L.S.; Henriques, A.T.; Braganhol, E.; Teixeira, H.F. An Overview of the Neuroprotective Potential of Rosmarinic Acid and Its Association with Nanotechnology-Based Delivery Systems: A Novel Approach to Treating Neurodegenerative Disorders. Neurochem. Int. 2019, 122, 47–58. [Google Scholar] [CrossRef]
- Naveed, M.; Hejazi, V.; Abbas, M.; Kamboh, A.A.; Khan, G.J.; Shumzaid, M.; Ahmad, F.; Babazadeh, D.; FangFang, X.; Modarresi-Ghazani, F.; et al. Chlorogenic Acid (CGA): A Pharmacological Review and Call for Further Research. Biomed. Pharmacother. 2018, 97, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, C.; Santangelo, R. Ferulic Acid: Pharmacological and Toxicological Aspects. Food Chem. Toxicol. 2014, 65, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Selka, A.; Moutombi, F.J.N.; Jean-François, J.; Touaibia, M. Hydroxycinnamic Acids and Their Related Synthetic Analogs: An Update of Pharmacological Activities. Mini-Rev. Med. Chem. 2021, 21, 1516–1544. [Google Scholar] [CrossRef] [PubMed]
- Lafay, S.; Gil-Izquierdo, A. Bioavailability of Phenolic Acids. Phytochem. Rev. 2008, 7, 301–311. [Google Scholar] [CrossRef]
- Zhao, Z.; Moghadasian, M.H. Bioavailability of Hydroxycinnamates: A Brief Review of in Vivo and in Vitro Studies. Phytochem. Rev. 2010, 9, 133–145. [Google Scholar] [CrossRef]
- Savjani, K.T.; Gajjar, A.K.; Savjani, J.K. Drug Solubility: Importance and Enhancement Techniques. ISRN Pharm. 2012, 2012, 195727. [Google Scholar] [CrossRef] [Green Version]
- Horter, D.; Dressman, J.B. Influence of Physiochemical Properties on Dissolution of Drugs. Adv. Drug Deliv. Rev. 1997, 25, 3–14. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services; Food and Drug Administration. Guidance for Industry—Waiver of In Vivo Bioavailability and Bioequivalence Studies for Immediate-Release Solid Oral Dosage Forms Based on a Biopharmaceutics Classification System; Center for Drug Evaluation and Research: Silver Spring, MD, USA, 2017. [Google Scholar]
- United States National Library of Medicine. The Efficacy and Safety of Caffeic Acid for Esophageal Cancer (NCT03070262). Available online: ClinicalTrials.gov/show/NCT03070262 (accessed on 27 May 2022).
- United States National Library of Medicine. The Effects of Coffee Main Constituents (Caffeine and Chlorogenic Acid) Supplementation on Inflammatory, Metabolic Factors, Hepatic Steatosis and Fibrosis in None-Alcoholic Fatty Liver Patients with Type 2 Diabetes (NCT02929901). Available online: ClinicalTrials.gov/show/NCT02929901 (accessed on 27 May 2022).
- United States National Library of Medicine. Effect of Chlorogenic Acid on Patients with Impaired Glucose Tolerance (NCT02621060). Available online: ClinicalTrials.gov/show/NCT02621060 (accessed on 27 May 2022).
- United States National Library of Medicine. Caffeic Acid Combining High-Dose Dexamethasone in Management of ITP. Available online: ClinicalTrials.gov/show/NCT02556814 (accessed on 27 May 2022).
- United States National Library of Medicine. Dietary Polyphenols and Glycation in Renal Insufficiency (NCT02524938). Available online: ClinicalTrials.gov/show/NCT02524938 (accessed on 27 May 2022).
- United States National Library of Medicine. Evaluation of Effects of Green Coffee Bean Extract (GCE) on Physiological and Psychological Variables (NCT02388672). Available online: ClinicalTrials.gov/show/NCT02388672 (accessed on 27 May 2022).
- United States National Library of Medicine. Caffeic Acid Tablets as a Second-Line Therapy for ITP (NCT02351622). Available online: ClinicalTrials.gov/show/NCT02351622 (accessed on 27 May 2022).
- United States National Library of Medicine. Efficacy of Spearmint Tea in Relieving Osteoarthritis of the Knee (NCT01380015). Available online: ClinicalTrials.gov/show/NCT01380015 (accessed on 27 May 2022).
- United States National Library of Medicine. Mint Tea for the Treatment of Nasal Polyps (NCT00465543). Available online: ClinicalTrials.gov/show/NCT00465543 (accessed on 27 May 2022).
- Rastogi, H.; Jana, S. Evaluation of Physicochemical Properties and Intestinal Permeability of Six Dietary Polyphenols in Human Intestinal Colon Adenocarcinoma Caco-2 Cells. Eur. J. Drug Metab. Pharmacokinet. 2016, 41, 33–43. [Google Scholar] [CrossRef]
- Saija, A.; Tomaino, A.; Trombetta, D.; De Pasquale, A.; Uccella, N.; Barbuzzi, T.; Paolino, D.; Bonina, F. In Vitro and in Vivo Evaluation of Caffeic and Ferulic Acids as Topical Photoprotective Agents. Int. J. Pharm. 2000, 199, 39–47. [Google Scholar] [CrossRef]
- Box, K.; Comer, J. Using Measured PKa, LogP and Solubility to Investigate Supersaturation and Predict BCS Class. Curr. Drug Metab. 2008, 9, 869–878. [Google Scholar] [CrossRef]
- de Campos Buzzi, F.; Franzoi, C.L.; Antonini, G.; Fracasso, M.; Filho, V.C.; Yunes, R.A.; Niero, R. Antinociceptive Properties of Caffeic Acid Derivatives in Mice. Eur. J. Med. Chem. 2009, 44, 4596–4602. [Google Scholar] [CrossRef] [PubMed]
- Kfoury, M.; Landy, D.; Auezova, L.; Greige-Gerges, H.; Fourmentin, S. Effect of Cyclodextrin Complexation on Phenylpropanoids’ Solubility and Antioxidant Activity. Beilstein J. Org. Chem. 2014, 10, 2322–2331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beneduci, A.; Furia, E.; Russo, N.; Marino, T. Complexation Behaviour of Caffeic, Ferulic and p-Coumaric Acids towards Aluminium Cations: A Combined Experimental and Theoretical Approach. New J. Chem. 2017, 41, 5182–5190. [Google Scholar] [CrossRef]
- Kfoury, M.; Geagea, C.; Ruellan, S.; Greige-Gerges, H.; Fourmentin, S. Effect of Cyclodextrin and Cosolvent on the Solubility and Antioxidant Activity of Caffeic Acid. Food Chem. 2019, 278, 163–169. [Google Scholar] [CrossRef]
- Cheng, J.C.; Dai, F.; Zhou, B.; Yang, L.; Liu, Z.L. Antioxidant Activity of Hydroxycinnamic Acid Derivatives in Human Low Density Lipoprotein: Mechanism and Structure-Activity Relationship. Food Chem. 2007, 104, 132–139. [Google Scholar] [CrossRef]
- Divakar, S.; Maheswaran, M.M. Structural Studies on Inclusion Compounds of β-Cyclodextrin with Some Substituted Phenols. J. Incl. Phenom. Mol. Recognit. Chem. 1997, 27, 113–126. [Google Scholar] [CrossRef]
- Im, N.R.; Kim, K.M.; Young, S.J.; Park, S.N. Physical Characteristics and in Vitro Skin Permeation of Elastic Liposomes Loaded with Caffeic Acid-Hydroxypropyl-β-Cyclodextrin. Korean J. Chem. Eng. 2016, 33, 2738–2746. [Google Scholar] [CrossRef]
- Nile, S.H.; Ko, E.Y.; Kim, D.H.; Keum, Y.S. Screening of Ferulic Acid Related Compounds as Inhibitors of Xanthine Oxidase and Cyclooxygenase-2 with Anti-Inflammatory Activity. Braz. J. Pharmacogn. 2016, 26, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Adomako-Bonsu, A.G.; Chan, S.L.; Pratten, M.; Fry, J.R. Antioxidant Activity of Rosmarinic Acid and Its Principal Metabolites in Chemical and Cellular Systems: Importance of Physico-Chemical Characteristics. Toxicol. Vitro 2017, 40, 248–255. [Google Scholar] [CrossRef]
- Váňová, J.; Liimatta, L.J.; Česla, P.; Wiedmer, S.K. Determination of Distribution Constants of Antioxidants by Electrokinetic Chromatography. Cogent Chem. 2017, 3, 1–11. [Google Scholar] [CrossRef]
- Mota, F.L.; Queimada, A.J.; Pinho, S.P.; Macedo, E.A. Aqueous Solubility of Some Natural Phenolic Compounds. Ind. Eng. Chem. Res. 2008, 47, 5182–5189. [Google Scholar] [CrossRef] [Green Version]
- Ren, J.; Jiang, X.; Li, C.; Li, K.; Chen, Z.; Ma, G. Absorptive Profile of Chlorogenic Acid in Rats. Pharmazie 2007, 62, 689–692. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Parrilla, E.; Palos, R.; De La Rosa, L.A.; Frontana-Uribe, B.A.; González-Aguilar, G.A.; Machi, L.; Ayala-Zavala, J.F. Formation of Two 1:1 Chlorogenic Acid: β-Cyclodextrin Complexes at PH 5: Spectroscopic, Thermodynamic and Voltammetric Study. J. Mex. Chem. Soc. 2010, 54, 103–110. [Google Scholar] [CrossRef]
- Sanchez, M.B.; Miranda-Perez, E.; Verjan, J.C.G.; de los Angeles Fortis Barrera, M.; Perez-Ramos, J.; Alarcon-Aguilar, F.J. Potential of the Chlorogenic Acid as Multitarget Agent: Insulin-Secretagogue and PPAR α/γ Dual Agonist. Biomed. Pharmacother. 2017, 94, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Farrell, T.L.; Dew, T.P.; Poquet, L.; Hanson, P.; Williamson, G. Absorption and Metabolism of Chlorogenic Acids in Cultured Gastric Epithelial Monolayers. Drug Metab. Dispos. 2011, 39, 2338–2346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakkou, Z.; Maciuk, A.; Leblais, V.; Bouanani, N.E.; Mekhfi, H.; Bnouham, M.; Aziz, M.; Ziyyat, A.; Rauf, A.; Hadda, T.B.; et al. Antihypertensive and Vasodilator Effects of Methanolic Extract of Inula Viscosa: Biological Evaluation and POM Analysis of Cynarin, Chlorogenic Acid as Potential Hypertensive. Biomed. Pharmacother. 2017, 93, 62–69. [Google Scholar] [CrossRef]
- Benvidi, A.; Dadras, A.; Abbasi, S.; Tezerjani, M.D.; Rezaeinasab, M.; Tabaraki, R.; Namazian, M. Experimental and Computational Study of the PKa of Coumaric Acid Derivatives. J. Chin. Chem. Soc. 2019, 66, 589–593. [Google Scholar] [CrossRef]
- Stȩpnik, K.E.; Malinowska, I.; Rój, E. In Vitro and in Silico Determination of Oral, Jejunum and Caco-2 Human Absorption of Fatty Acids and Polyphenols. Micellar Liquid Chromatography. Talanta 2014, 130, 265–273. [Google Scholar] [CrossRef]
- Šmidovnik, A.; Stražišar, M.; Jazbec, P.; Fir, M.M.; Prošek, M. Effect of Complexation Cyclodextrins with Phenolic Acids and Coenzyme Q10on Their Physico-Chemical Properties and Bioavailability. Acta Chim. Slov. 2010, 57, 9–16. [Google Scholar]
- Dey, P.; Sarkar, I.; Dutta, S.; Saha, M.R.; Chaudhuri, T.K. Correlative Metabolomic Fingerprinting and Molecular Docking Studies of Dermatological Phytotherapeutics of South-Eastern Himalaya. J. Tradit. Complement. Med. 2019, 9, 243–248. [Google Scholar] [CrossRef]
- Jablonsky, M.; Haz, A.; Sladkova, A.; Strizincova, P.; Skulcova, A.; Majova, V.; Jablonsky, J. Nutraceuticals as Phenolic Bioactive Compounds Analysis of Softwood Bark and Their Possibilities of Industry Applications. J. Hyg. Eng. Des. 2019, 26, 93–99. [Google Scholar]
- Ota, A.; Abramovič, H.; Abram, V.; Poklar Ulrih, N. Interactions of P-Coumaric, Caffeic and Ferulic Acids and Their Styrenes with Model Lipid Membranes. Food Chem. 2011, 125, 1256–1261. [Google Scholar] [CrossRef]
- Monti, D.; Tampucci, S.; Chetoni, P.; Burgalassi, S.; Saino, V.; Centini, M.; Staltari, L.; Anselmi, C. Permeation and Distribution of Ferulic Acid and Its α-Cyclodextrin Complex from Different Formulations in Hairless Rat Skin. AAPS PharmSciTech 2011, 12, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Zhang, Z.; Shen, H.; Zheng, J.; Zhang, G. Comparison of Structures, Physicochemical Properties and in Vitro Bioactivity between Ferulic Acid-β-Cyclodextrin Conjugate and the Corresponding Inclusion Complex. Food Res. Int. 2019, 125, 108619. [Google Scholar] [CrossRef] [PubMed]
- Nath, L.S.; Khan, S.A.; Ahmad, A. Computer Aided Screening of Natural Products in Search of Lead Molecules for Design and Development of Potent Anti-Inflammatory Agents. Sch. Acad. J. Pharm. 2014, 3, 496–503. [Google Scholar]
- El-Boshy, M.; Header, E.; ElSawy, N.; Basalamah, M.; Mubarak, M.; Hadda, T. Studies on the Constituents of Rosmarinus Officinalis and Their Synergistic Effect in Experimental Diabetic Rats. J. Investig. Biochem. 2015, 4, 36. [Google Scholar] [CrossRef]
- Al Danaf, N.; Melhem, R.A.; Assaf, K.I.; Nau, W.M.; Patra, D. Photophysical Properties of Neutral and Dissociated Forms of Rosmarinic Acid. J. Lumin. 2016, 175, 50–56. [Google Scholar] [CrossRef]
- Veras, K.S.; Silveira Fachel, F.N.; Delagustin, M.G.; Teixeira, H.F.; Barcellos, T.; Henriques, A.T.; Bassani, V.L.; Koester, L.S. Complexation of Rosmarinic Acid with Hydroxypropyl-β-Cyclodextrin and Methyl-β-Cyclodextrin: Formation of 2:1 Complexes with Improved Antioxidant Activity. J. Mol. Struct. 2019, 1195, 582–590. [Google Scholar] [CrossRef]
- Daina, A.; Michielin, O.; Zoete, V. SwissADME: A Free Web Tool to Evaluate Pharmacokinetics, Drug-Likeness and Medicinal Chemistry Friendliness of Small Molecules; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Abuhelwa, A.Y.; Williams, D.B.; Upton, R.N.; Foster, D.J.R. Food, Gastrointestinal PH, and Models of Oral Drug Absorption. Eur. J. Pharm. Biopharm. 2017, 112, 234–248. [Google Scholar] [CrossRef]
- Di, L.; Kerns, E.H.; Hong, Y.; Chen, H. Development and Application of High Throughput Plasma Stability Assay for Drug Discovery. Int. J. Pharm. 2005, 297, 110–119. [Google Scholar] [CrossRef]
- Gayoso, L.; Claerbout, A.S.; Calvo, M.I.; Cavero, R.Y.; Astiasarán, I.; Ansorena, D. Bioaccessibility of Rutin, Caffeic Acid and Rosmarinic Acid: Influence of the in Vitro Gastrointestinal Digestion Models. J. Funct. Foods 2016, 26, 428–438. [Google Scholar] [CrossRef]
- Zorić, Z.; Markić, J.; Pedisić, S.; Bučevic-Popović, V.; Generalic-Mekinić, I.; Grebenar, K.; Kulišić-Bilušic, T. Stability of Rosmarinic Acid in Aqueous Extracts from Different Lamiaceae Species after in Vitro Digestion with Human Gastrointestinal Enzymes. Food Technol. Biotechnol. 2016, 54, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Porfírio, S.; Falé, P.L.V.; Madeira, P.J.A.; Florêncio, M.H.; Ascensão, L.; Serralheiro, M.L.M. Antiacetylcholinesterase and Antioxidant Activities of Plectranthus Barbatus Tea, after in Vitro Gastrointestinal Metabolism. Food Chem. 2010, 122, 179–187. [Google Scholar] [CrossRef]
- Costa, P.; Grevenstuk, T.; Rosa da Costa, A.M.; Gonçalves, S.; Romano, A. Antioxidant and Anti-Cholinesterase Activities of Lavandula Viridis L’Hér Extracts after in Vitro Gastrointestinal Digestion. Ind. Crops Prod. 2014, 55, 83–89. [Google Scholar] [CrossRef]
- Tagliazucchi, D.; Verzelloni, E.; Bertolini, D.; Conte, A. In Vitro Bio-Accessibility and Antioxidant Activity of Grape Polyphenols. Food Chem. 2010, 120, 599–606. [Google Scholar] [CrossRef]
- D’Antuono, I.; Garbetta, A.; Linsalata, V.; Minervini, F.; Cardinali, A. Polyphenols from Artichoke Heads (Cynara cardunculus (L.) Subsp. Scolymus Hayek): In Vitro Bio-Accessibility, Intestinal Uptake and Bioavailability. Food Funct. 2015, 6, 1268–1277. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Egashira, Y.; Sanada, H. Ferulic Acid Is Quickly Absorbed from Rat Stomach as the Free Form and Then Conjugated Mainly in Liver. J. Nutr. 2004, 134, 3083–3088. [Google Scholar] [CrossRef] [Green Version]
- Bermúdez-Soto, M.J.; Tomás-Barberán, F.A.; García-Conesa, M.T. Stability of Polyphenols in Chokeberry (Aronia melanocarpa) Subjected to in Vitro Gastric and Pancreatic Digestion. Food Chem. 2007, 102, 865–874. [Google Scholar] [CrossRef]
- Siracusa, L.; Kulisic-Bilusic, T.; Politeo, O.; Krause, I.; Dejanovic, B.; Ruberto, G. Phenolic Composition and Antioxidant Activity of Aqueous Infusions from Capparis spinosa L. and Crithmum maritimum L. before and after Submission to a Two-Step in Vitro Digestion Model. J. Agric. Food Chem. 2011, 59, 12453–12459. [Google Scholar] [CrossRef]
- Budryn, G.; Pałecz, B.; Rachwał-Rosiak, D.; Oracz, J.; Zaczyńska, D.; Belica, S.; Navarro-González, I.; Meseguer, J.M.V.; Pérez-Sánchez, H. Effect of Inclusion of Hydroxycinnamic and Chlorogenic Acids from Green Coffee Bean in β-Cyclodextrin on Their Interactions with Whey, Egg White and Soy Protein Isolates. Food Chem. 2015, 168, 276–287. [Google Scholar] [CrossRef]
- Celli, N.; Dragani, L.K.; Murzilli, S.; Pagliani, T.; Poggi, A. In Vitro and in Vivo Stability of Caffeic Acid Phenethyl Ester, a Bioactive Compound of Propolis. J. Agric. Food Chem. 2007, 55, 3398–3407. [Google Scholar] [CrossRef]
- Narita, Y.; Inouye, K. Degradation Kinetics of Chlorogenic Acid at Various PH Values and Effects of Ascorbic Acid and Epigallocatechin Gallate on Its Stability under Alkaline Conditions. J. Agric. Food Chem. 2013, 61, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Uang, Y.S.; Kang, F.L.; Hsu, K.Y. Determination of Caffeic Acid in Rabbit Plasma by High-Performance Liquid Chromatography. J. Chromatogr. B Biomed. Sci. Appl. 1995, 673, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Li, Q.; Zhang, M.; Liu, Z.; Yin, W.; Liu, W.; Chen, X.; Bi, K. LC-MS Determination and Pharmacokinetics of p-Coumaric Acid in Rat Plasma after Oral Administration of p-Coumaric Acid and Freeze-Dried Red Wine. J. Agric. Food Chem. 2010, 58, 12083–12088. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Li, Q.; Jia, Y.; Zhao, L.; Xiao, F.; Lv, C.; Xu, H.; Chen, X.; Bi, K. A UFLC-MS/MS Method for Simultaneous Quantitation of Spinosin, Mangiferin and Ferulic Acid in Rat Plasma: Application to a Comparative Pharmacokinetic Study in Normal and Insomnic Rats. J. Mass Spectrom. 2012, 47, 1333–1340. [Google Scholar] [CrossRef]
- Kerns, E.H.; Di, L.; Petusky, S.; Farris, M.; Ley, R.; Jupp, P. Combined Application of Parallel Artificial Membrane Permeability Assay and Caco-2 Permeability Assays in Drug Discovery. J. Pharm. Sci. 2004, 93, 1440–1453. [Google Scholar] [CrossRef]
- Sarmento, B.; Andrade, F.; Da Silva, S.B.; Rodrigues, F.; Das Neves, J.; Ferreira, D. Cell-Based in Vitro Models for Predicting Drug Permeability. Expert Opin. Drug Metab. Toxicol. 2012, 8, 607–621. [Google Scholar] [CrossRef]
- De Souza, J.; Freitas, Z.M.F.; Storpirtis, S. Modelos in Vitro Para Determinação Da Absorção de Fármacos e Previsão Da Relação Dissolução/Absorção. Rev. Bras. Ciências Farm. 2007, 43, 515–527. [Google Scholar] [CrossRef] [Green Version]
- Avdeef, A. The Rise of PAMPA. Expert Opin. Drug Metab. Toxicol. 2005, 1, 325–342. [Google Scholar] [CrossRef]
- Petit, C.; Bujard, A.; Skalicka-Woźniak, K.; Cretton, S.; Houriet, J.; Christen, P.; Carrupt, P.A.; Wolfender, J.L. Prediction of the Passive Intestinal Absorption of Medicinal Plant Extract Constituents with the Parallel Artificial Membrane Permeability Assay (PAMPA). Planta Med. 2016, 82, 424–431. [Google Scholar] [CrossRef] [Green Version]
- Petit, C.; Ceccarelli, M.; Cretton, S.; Houriet, J.; Skalicka-Woźniak, K.; Christen, P.; Carrupt, P.A.; Goracci, L.; Wolfender, J.L. Passive Intestinal Absorption of Representative Plant Secondary Metabolites: A Physicochemical Study. Planta Med. 2017, 83, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avdeef, A. Absorption and Drug Development: Solubility, Permeability, and Charge State, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Li, D.; Kerns, E. Drug-Like Properties: Concepts, Structure Design and Methods from ADME to Toxicity Optimization, 2nd ed.; Academic Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Egan, W.J.; Merz, K.M.; Baldwin, J.J. Prediction of Drug Absorption Using Multivariate Statistics. J. Med. Chem. 2000, 43, 3867–3877. [Google Scholar] [CrossRef]
- Ghose, A.K.; Viswanadhan, V.N.; Wendoloski, J.J. A Knowledge-Based Approach in Designing Combinatorial or Medicinal Chemistry Libraries for Drug Discovery. 1. A Qualitative and Quantitative Characterization of Known Drug Databases. J. Comb. Chem. 1999, 1, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Lipinski, C.A.; Lombardo, F.; Dominy, B.W.; Feeney, P.J. Experimental and Computational Approaches to Estimate Solubility and Permeability in Drug Discovery and Development Settings. Adv. Drug Deliv. Rev. 1997, 23, 3–25. [Google Scholar] [CrossRef]
- Muegge, I.; Heald, S.L.; Brittelli, D. Simple Selection Criteria for Drug-like Chemical Matter. J. Med. Chem. 2001, 44, 1841–1846. [Google Scholar] [CrossRef] [PubMed]
- Oprea, T.I. Property Distribution of Drug-Related Chemical Databases. J. Comput. Aided Mol. Des. 2000, 14, 251–264. [Google Scholar] [CrossRef]
- Veber, D.F.; Johnson, S.R.; Cheng, H.Y.; Smith, B.R.; Ward, K.W.; Kopple, K.D. Molecular Properties That Influence the Oral Bioavailability of Drug Candidates. J. Med. Chem. 2002, 45, 2615–2623. [Google Scholar] [CrossRef] [PubMed]
- Zmuidinavicius, D.; Didziapetris, R.; Japertas, P.; Avdeef, A.; Petrauskas, A. Classification Structure-Activity Relations (C-SAR) in Prediction of Human Intestinal Absorption. J. Pharm. Sci. 2003, 92, 621–633. [Google Scholar] [CrossRef] [PubMed]
- Van de Waterbeemd, H.; Lennernas, H.; Artursson, P. Drug Bioavailability: Estimation of Solubility, Permeability, Absorption and Bioavailability, 1st ed.; Wiley-VCH: Weinheim, Germany, 2003. [Google Scholar]
- Sugano, K.; Kansy, M.; Artursson, P.; Avdeef, A.; Bendels, S.; Di, L.; Ecker, G.F.; Faller, B.; Fischer, H.; Gerebtzoff, G.; et al. Coexistence of Passive and Carrier-Mediated Processes in Drug Transport. Nat. Rev. Drug Discov. 2010, 9, 597–614. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Chow, E.C.Y.; Liu, S.; Du, Y.; Pang, K.S. The Caco-2 Cell Monolayer: Usefulness and Limitations. Expert Opin. Drug Metab. Toxicol. 2008, 4, 395–411. [Google Scholar] [CrossRef]
- Gomez-Lechon, M.; Donato, M.; Lahoz, A.; Castell, J. Cell Lines: A Tool for In Vitro Drug Metabolism Studies. Curr. Drug Metab. 2008, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Konishi, Y.; Shimizu, M. Transepithelial Transport of Ferulic Acid by Monocarboxylic Acid Transporter in Caco-2 Cell Monolayers. Biosci. Biotechnol. Biochem. 2003, 67, 856–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konishi, Y.; Kobayashi, S.; Shimizu, M. Transepithelial Transport of P-Coumaric Acid and Gallic Acid in Caco-2 Cell Monolayers. Biosci. Biotechnol. Biochem. 2003, 67, 2317–2324. [Google Scholar] [CrossRef]
- Konishi, Y.; Kobayashi, S. Microbial Metabolites of Ingested Caffeic Acid Are Absorbed by the Monocarboxylic Acid Transporter (MCT) in Intestinal Caco-2 Cell Monolayers. J. Agric. Food Chem. 2004, 52, 6418–6424. [Google Scholar] [CrossRef] [PubMed]
- Konishi, Y.; Kobayashi, S. Transepithelial Transport of Chlorogenic Acid, Caffeic Acid, and Their Colonic Metabolites in Intestinal Caco-2 Cell Monolayers. J. Agric. Food Chem. 2004, 52, 2518–2526. [Google Scholar] [CrossRef] [PubMed]
- Falé, P.L.; Ascensão, L.; Serralheiro, M.L.M. Effect of Luteolin and Apigenin on Rosmarinic Acid Bioavailability in Caco-2 Cell Monolayers. Food Funct. 2013, 4, 426–431. [Google Scholar] [CrossRef]
- Monente, C.; Ludwig, I.A.; Stalmach, A.; De Peña, M.P.; Cid, C.; Crozier, A. In Vitro Studies on the Stability in the Proximal Gastrointestinal Tract and Bioaccessibility in Caco-2 Cells of Chlorogenic Acids from Spent Coffee Grounds. Int. J. Food Sci. Nutr. 2015, 66, 657–664. [Google Scholar] [CrossRef]
- Qiang, Z.; Ye, Z.; Hauck, C.; Murphy, P.A.; McCoy, J.-A.; Widrlechner, M.P.; Reddy, M.B.; Hendrich, S. Permeability of Rosmarinic Acid in Prunella Vulgaris and Ursolic Acid in Salvia Officinalis Extracts across Caco-2 Cell Monolayers. J. Ethnopharmacol. 2011, 137, 1107–1112. [Google Scholar] [CrossRef] [Green Version]
- Farrell, T.L.; Poquet, L.; Dew, T.P.; Barber, S.; Williamson, G. Predicting Phenolic Acid Absorption in Caco-2 Cells: A Theoretical Permeability Model and Mechanistic Study. Drug Metab. Dispos. 2012, 40, 397–406. [Google Scholar] [CrossRef]
- Gómez-Juaristi, M.; Sarria, B.; Goya, L.; Bravo-Clemente, L.; Mateos, R. Experimental Confounding Factors Affecting Stability, Transport and Metabolism of Flavanols and Hydroxycinnamic Acids in Caco-2 Cells. Food Res. Int. 2020, 129, 108797. [Google Scholar] [CrossRef]
- Yang, J.H.; Zhang, L.; Li, J.S.; Chen, L.H.; Zheng, Q.; Chen, T.; Chen, Z.P.; Fu, T.M.; Di, L.Q. Enhanced Oral Bioavailability and Prophylactic Effects on Oxidative Stress and Hepatic Damage of an Oil Solution Containing a Rosmarinic Acid-Phospholipid Complex. J. Funct. Foods 2015, 19, 63–73. [Google Scholar] [CrossRef]
- Mortelé, O.; Jörissen, J.; Spacova, I.; Lebeer, S.; van Nuijs, A.L.N.; Hermans, N. Demonstrating the Involvement of an Active Efflux Mechanism in the Intestinal Absorption of Chlorogenic Acid and Quinic Acid Using a Caco-2 Bidirectional Permeability Assay. Food Funct. 2021, 12, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Villalva, M.; Jaime, L.; Aguado, E.; Nieto, J.A.; Reglero, G.; Santoyo, S. Anti-Inflammatory and Antioxidant Activities from the Basolateral Fraction of Caco-2 Cells Exposed to a Rosmarinic Acid Enriched Extract. J. Agric. Food Chem. 2018, 66, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Cha, K.H.; Kim, C.Y.; Nho, C.W.; Pan, C.H. Bioavailability of Hydroxycinnamic Acids from Crepidiastrum Denticulatum Using Simulated Digestion and Caco-2 Intestinal Cells. J. Agric. Food Chem. 2014, 62, 5290–5295. [Google Scholar] [CrossRef]
- Poquet, L.; Clifford, M.N.; Williamson, G. Transport and Metabolism of Ferulic Acid through the Colonic Epithelium. Drug Metab. Dispos. 2008, 36, 190–197. [Google Scholar] [CrossRef]
- Bergmann, H.; Rogoll, D.; Scheppach, W.; Melcher, R.; Richling, E. The Ussing Type Chamber Model to Study the Intestinal Transport and Modulation of Specific Tight-Junction Genes Using a Colonic Cell Line. Mol. Nutr. Food Res. 2009, 53, 1211–1225. [Google Scholar] [CrossRef]
- Karlsson, J.; Ungell, A.L.; Gråsjö, J.; Artursson, P. Paracellular Drug Transport across Intestinal Epithelia: Influence of Charge and Induced Water Flux. Eur. J. Pharm. Sci. 1999, 9, 47–56. [Google Scholar] [CrossRef]
- Giacomini, K.M.; Huang, S.M.; Tweedie, D.J.; Benet, L.Z.; Brouwer, K.L.R.; Chu, X.; Dahlin, A.; Evers, R.; Fischer, V.; Hillgren, K.M.; et al. Membrane Transporters in Drug Development. Nat. Rev. Drug Discov. 2010, 9, 215–236. [Google Scholar] [CrossRef]
- Zhou, W.; Shan, J.; Wang, S.; Cai, B.; Di, L. Transepithelial Transport of Phenolic Acids in Flos Lonicerae Japonicae in Intestinal Caco-2 Cell Monolayers. Food Funct. 2015, 6, 3072–3080. [Google Scholar] [CrossRef]
- Li, F.-R.; Fu, Y.-Y.; Jiang, D.-H.; Wu, Z.; Zhou, Y.-J.; Guo, L.; Dong, Z.-M.; Wang, Z.-Z. Reversal Effect of Rosmarinic Acid on Multidrug Resistance in SGC7901/Adr Cell. J. Asian Nat. Prod. Res. 2013, 15, 276–285. [Google Scholar] [CrossRef]
- Hong, Y.J.; Yang, S.Y.; Nam, M.H.; Koo, Y.C.; Lee, K.W. Caffeic Acid Inhibits the Uptake of 2-Amino-1-Methyl-6-Phenylimidazo-[4,5-b]Pyridine (PhIP) by Inducing the Efflux Transporters Expression in Caco-2 Cells. Biol. Pharm. Bull. 2015, 38, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teng, Y.; Wang, C.C.N.; Liao, W.; Lan, Y.; Hung, C. Caffeic Acid Attenuates Multi-Drug Resistance in Cancer Cells by Inhibiting Efflux Function of Human P-Glycoprotein. Molecules 2020, 25, 247. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Zhu, Y.; Li, F.; Zhang, G.; Shi, J.; Ou, R.; Tong, Y. Spica Prunellae and Its Marker Compound Rosmarinic Acid Induced the Expression of Efflux Transporters through Activation of Nrf2-Mediated Signaling Pathway in HepG2 Cells. J. Ethnopharmacol. 2016, 193, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Yin, D.; Li, J.; Shao, F.; Zhang, Q.; Jiang, Q.; Zhang, M.; Yang, Y. Rosmarinic Acid, the Active Component of Salvia Miltiorrhizae, Improves Gliquidone Transport by Regulating the Expression and Function of P-Gp and BCRP in Caco-2 Cells. Pharmazie 2020, 75, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Muthusamy, G.; Balupillai, A.; Ramasamy, K.; Shanmugam, M.; Gunaseelan, S.; Mary, B.; Prasad, N.R. Ferulic Acid Reverses ABCB1-Mediated Paclitaxel Resistance in MDR Cell Lines. Eur. J. Pharmacol. 2016, 786, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Muthusamy, G.; Gunaseelan, S.; Prasad, N.R. Ferulic Acid Reverses P-Glycoprotein-Mediated Multidrug Resistance via Inhibition of PI3K/Akt/NF-ΚB Signaling Pathway. J. Nutr. Biochem. 2019, 63, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Kern, S.M.; Bennett, R.N.; Needs, P.W.; Mellon, F.A.; Kroon, P.A.; Garcia-Conesa, M.T. Characterization of Metabolites of Hydroxycinnamates in the in Vitro Model of Human Small Intestinal Epithelium Caco-2 Cells. J. Agric. Food Chem. 2003, 51, 7884–7891. [Google Scholar] [CrossRef]
- Achour, M.; Saguem, S.; Sarriá, B.; Bravo, L.; Mateos, R. Bioavailability and Metabolism of Rosemary Infusion Polyphenols Using Caco-2 and HepG2 Cell Model Systems. J. Sci. Food Agric. 2018, 98, 3741–3751. [Google Scholar] [CrossRef] [Green Version]
- Mateos, R.; Goya, L.; Bravo, L. Uptake and Metabolism of Hydroxycinnamic Acids (Chlorogenic, Caffeic, and Ferulic Acids) by HepG2 Cells as a Model of the Human Liver. J. Agric. Food Chem. 2006, 54, 8724–8732. [Google Scholar] [CrossRef] [Green Version]
- Su, J.; Jia, F.; Lu, J.; Chen, W.; Sun, H.; Liu, T.; Wu, X. Characterization of the Metabolites of Rosmarinic Acid in Human Liver Microsomes Using Liquid Chromatography Combined with Electrospray Ionization Tandem Mass Spectrometry. Biomed. Chromatogr. 2020, 34, e4806. [Google Scholar] [CrossRef]
- Moridani, M.Y.; Scobie, H.; O’Brien, P.J. Metabolism of Caffeic Acid by Isolated Rat Hepatocytes and Subcellular Fractions. Toxicol. Lett. 2002, 133, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Moridani, M.Y.; Scobie, H.; Jamshidzadeh, A.; Salehi, P.; O’Brien, P.J. Caffeic Acid, Chlorogenic Acid, and Dihydrocaffeic Acid Metabolism: Glutathione Conjugate Formation. Drug Metab. Dispos. 2001, 29, 1432–1439. [Google Scholar] [PubMed]
- Wong, C.C.; Meinl, W.; Glatt, H.R.; Barron, D.; Stalmach, A.; Steiling, H.; Crozier, A.; Williamson, G. In Vitro and in Vivo Conjugation of Dietary Hydroxycinnamic Acids by UDP-Glucuronosyltransferases and Sulfotransferases in Humans. J. Nutr. Biochem. 2010, 21, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Gonthier, M.P.; Remesy, C.; Scalbert, A.; Cheynier, V.; Souquet, J.M.; Poutanen, K.; Aura, A.M. Microbial Metabolism of Caffeic Acid and Its Esters Chlorogenic and Caftaric Acids by Human Faecal Microbiota in Vitro. Biomed. Pharmacother. 2006, 60, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Parkar, S.G.; Trower, T.M.; Stevenson, D.E. Fecal Microbial Metabolism of Polyphenols and Its Effects on Human Gut Microbiota. Anaerobe 2013, 23, 12–19. [Google Scholar] [CrossRef]
- Ludwig, I.A.; Paz de Peña, M.; Concepción, C.; Alan, C. Catabolism of Coffee Chlorogenic Acids by Human Colonic Microbiota. BioFactors 2013, 39, 623–632. [Google Scholar] [CrossRef]
- Shen, H.; Tong, X.; Yang, J.; Yu, L.; Zhou, H.; Wang, Y.; He, Y.; Wan, H.; Li, C. Biotransformation of Natural Hydroxycinnamic Acids by Gut Microbiota from Normal and Cerebral Ischemia-Reperfusion Injured Rats: A Comparative Study. Food Funct. 2020, 11, 5389–5395. [Google Scholar] [CrossRef]
- Bel-Rhlid, R.; Crespy, V.; Pagé-Zoerkler, N.; Nagy, K.; Raab, T.; Hansen, C.E. Hydrolysis of Rosmarinic Acid from Rosemary Extract with Esterases and Lactobacillus Johnsonii in Vitro and in a Gastrointestinal Model. J. Agric. Food Chem. 2009, 57, 7700–7705. [Google Scholar] [CrossRef]
- Luo, Z.; Liu, Y.; Zhao, B.; Tang, M.; Dong, H.; Zhang, L.; Lv, B.; Wei, L. Ex Vivo and in Situ Approaches Used to Study Intestinal Absorption. J. Pharmacol. Toxicol. Methods 2013, 68, 208–216. [Google Scholar] [CrossRef]
- Deußer, H.; Rogoll, D.; Scheppach, W.; Volk, A.; Melcher, R.; Richling, E. Gastrointestinal Absorption and Metabolism of Apple Polyphenols Ex Vivo by the Pig Intestinal Mucosa in the Ussing Chamber. Biotechnol. J. 2013, 8, 363–370. [Google Scholar] [CrossRef]
- Erk, T.; Hauser, J.; Williamson, G.; Renouf, M.; Steiling, H.; Dionisi, F.; Richling, E. Structure- and Dose-Absorption Relationships of Coffee Polyphenols. BioFactors 2014, 40, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Garrait, G.; Jarrige, J.F.; Blanquet, S.; Beyssac, E.; Cardot, J.M.; Alric, M. Gastrointestinal Absorption and Urinary Excretion of Trans-Cinnamic and p-Coumaric Acids in Rats. J. Agric. Food Chem. 2006, 54, 2944–2950. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Shi, J.; Xu, W.; Heinrich, M.; Wang, J.; Deng, W. Ex Vivo and in Situ Evaluation of “Dispelling-Wind” Chinese Medicine Herb-Drugs on Intestinal Absorption of Chlorogenic Acid. Phytother. Res. 2015, 29, 1974–1981. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.P.E.; Chowrimootoo, G.; Choudhury, R.; Debnam, E.S.; Srai, S.K.; Rice-Evans, C. The Small Intestine Can Both Absorb and Glucuronidate Luminal Flavonoids. FEBS Lett. 1999, 458, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelber, O.; Wittwer, A.; Lapke, C.; Kroll, U.; Weiser, D.; Okpanyi, S.N.; Heilmann, J. Ex Vivo/in Vitro Absorption of STW 5 (Iberogast®) and Its Extract Components. Phytomedicine 2006, 13, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Konishi, Y.; Zhao, Z.; Shimizu, M. Phenolic Acids Are Absorbed from the Rat Stomach with Different Absorption Rates. J. Agric. Food Chem. 2006, 54, 7539–7543. [Google Scholar] [CrossRef]
- Wang, S.J.; Zeng, J.; Yang, B.K.; Zhong, Y.M. Bioavailability of Caffeic Acid in Rats and Its Absorption Properties in the Caco-2 Cell Model. Pharm. Biol. 2014, 52, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Lafay, S.; Morand, C.; Manach, C.; Besson, C.; Scalbert, A. Absorption and Metabolism of Caffeic Acid and Chlorogenic Acid in the Small Intestine of Rats. Br. J. Nutr. 2006, 96, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Lafay, S.; Gil-Izquierdo, A.; Manach, C.; Morand, C.; Besson, C.; Scalbert, A. Chlorogenic Acid Is Absorbed in Its Intact Form in the Stomach of Rats. J. Nutr. 2006, 136, 1192–1197. [Google Scholar] [CrossRef] [Green Version]
- Silberberg, M.; Morand, C.; Mathevon, T.; Besson, C.; Manach, C.; Scalbert, A.; Remesy, C. The Bioavailability of Polyphenols Is Highly Governed by the Capacity of the Intestine and of the Liver to Secrete Conjugated Metabolites. Eur. J. Nutr. 2006, 45, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.; Crespy, V.; Levrat-Verny, M.-A.; Leenhardt, F.; Leuillet, M.; Demigné, C.; Rémésy, C. The Bioavailability of Ferulic Acid Is Governed Primarily by the Food Matrix Rather than Its Metabolism in Intestine and Liver in Rats. J. Nutr. 2002, 132, 1962–1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camarasa, J.; Escubedo, E.; Adzet, T. Pharmacokinetics of Caffeic Acid in Rats by a High-Performance Liquid Chromatography Method. J. Pharm. Biomed. Anal. 1988, 6, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Konishi, Y.; Hitomi, Y.; Yoshida, M.; Yoshioka, E. Pharmacokinetic Study of Caffeic and Rosmarinic Acids in Rats after Oral Administration. J. Agric. Food Chem. 2005, 53, 4740–4746. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, W.; Ma, X.; Chu, Y.; Li, S.; Guo, J.; Jia, Y.; Zhou, S.; Zhu, Y.; Liu, C. Simultaneous Determination of Caffeic Acid and Its Major Pharmacologically Active Metabolites in Rat Plasma by LC-MS/MS and Its Application in Pharmacokinetic Study. Biomed. Chromatogr. 2015, 29, 552–559. [Google Scholar] [CrossRef]
- Qi, W.; Zhao, T.; Yang, W.W.; Wang, G.H.; Yu, H.; Zhao, H.X.; Yang, C.; Sun, L.X. Comparative Pharmacokinetics of Chlorogenic Acid after Oral Administration in Rats. J. Pharm. Anal. 2011, 1, 270–274. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.W.; Kim, J.M.; Jeong, J.S.; Son, M.; Lee, H.S.; Lee, M.G.; Kang, H.E. Pharmacokinetics of Chlorogenic Acid and Corydaline in DA-9701, a New Botanical Gastroprokinetic Agent, in Rats. Xenobiotica 2014, 44, 635–643. [Google Scholar] [CrossRef]
- De Oliveira, D.M.; Sampaio, G.R.; Pinto, C.B.; Catharino, R.R.; Bastos, D.H.M. Bioavailability of Chlorogenic Acids in Rats after Acute Ingestion of Maté Tea (Ilex Paraguariensis) or 5-Caffeoylquinic Acid. Eur. J. Nutr. 2017, 56, 2541–2556. [Google Scholar] [CrossRef]
- Chen, L.; Liu, C.S.; Chen, Q.Z.; Wang, S.; Xiong, Y.A.; Jing, J.; Lv, J.J. Characterization, Pharmacokinetics and Tissue Distribution of Chlorogenic Acid-Loaded Self-Microemulsifying Drug Delivery System. Eur. J. Pharm. Sci. 2017, 100, 102–108. [Google Scholar] [CrossRef]
- Konishi, Y.; Hitomi, Y.; Yoshioka, E. Intestinal Absorption of P-Coumaric and Gallic Acids in Rats after Oral Administration. J. Agric. Food Chem. 2004, 52, 2527–2532. [Google Scholar] [CrossRef]
- Lv, H.; Zou, M.; Yu, W.; Sun, B.; Cui, Y. Simultaneous Determination of Gallic Acid and p-Coumaric Acid in Rat Plasma by UPLC-MS/MS and Its Application to a Comparative Pharmacokinetic Study after Oral Administration of Monomer Compound and Red Wine Extract. J. Polyphen. 2019, 1, 1–11. [Google Scholar]
- Kim, H.; Choi, Y.; An, Y.; Jung, Y.-R.; Lee, J.-Y.; Lee, H.-J.; Jeong, J.; Kim, Z.; Kim, K. Development of P-Coumaric Acid Analysis in Human Plasma and Its Clinical Application to PK/PD Study. J. Clin. Med. 2020, 10, 108. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, C.; Zhang, Y.; Mi, S.; Wang, N. Pharmacokinetics of Ferulic Acid and Potential Interactions with Honghua and Clopidogrel in Rats. J. Ethnopharmacol. 2011, 137, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Z.; Zhang, K.; Yang, G.; Wang, Z.; Zhao, J.; Hu, R.; Feng, N. Ethyl Oleate-Containing Nanostructured Lipid Carriers Improve Oral Bioavailability of Trans-Ferulic Acid Ascompared with Conventional Solid Lipid Nanoparticles. Int. J. Pharm. 2016, 511, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.S.; Chen, L.; Hu, Y.N.; Dai, J.L.; Ma, B.; Tang, Q.F.; Tan, X.M. Self-Microemulsifying Drug Delivery System for Improved Oral Delivery and Hypnotic Efficacy of Ferulic Acid. Int. J. Nanomed. 2020, 15, 2059–2070. [Google Scholar] [CrossRef] [PubMed]
- Baba, S.; Osakabe, N.; Natsume, M.; Terao, J. Orally Administered Rosmarinic Acid Is Present as the Conjugated and/or Methylated Forms in Plasma, and Is Degraded and Metabolized to Conjugated Forms of Caffeic Acid, Ferulic Acid and m-Coumaric Acid. Life Sci. 2004, 75, 165–178. [Google Scholar] [CrossRef]
- Wang, J.; Li, G.; Rui, T.; Kang, A.; Li, G.; Fu, T.; Li, J.; Di, L.; Cai, B. Pharmacokinetics of Rosmarinic Acid in Rats by LC-MS/MS: Absolute Bioavailability and Dose Proportionality. RSC Adv. 2017, 7, 9057–9063. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.-H.; Mao, K.-J.; Huang, P.; Ye, Y.-J.; Guo, H.-S.; Cai, B.-C. Effect of Piperine on the Bioavailability and Pharmacokinetics of Rosmarinic Acid in Rat Plasma Using UPLC-MS/MS. Xenobiotica 2018, 48, 178–185. [Google Scholar] [CrossRef]
- Wang, X.; Qian, Y.; Li, X.; Jia, X.; Yan, Z.; Han, M.; Qiao, M.; Ma, X.; Chu, Y.; Zhou, S.; et al. Rapid Determination of Rosmarinic Acid and Its Two Bioactive Metabolites in the Plasma of Rats by LC–MS/MS and Application to a Pharmacokinetics Study. Biomed. Chromatogr. 2021, 35, e4984. [Google Scholar] [CrossRef]
- Omar, M.H.; Mullen, W.; Stalmach, A.; Auger, C.; Rouanet, J.M.; Teissedre, P.L.; Caldwell, S.T.; Hartley, R.C.; Crozier, A. Absorption, Disposition, Metabolism, and Excretion of [3-14C]Caffeic Acid in Rats. J. Agric. Food Chem. 2012, 60, 5205–5214. [Google Scholar] [CrossRef]
- Chen, W.C.; Huang, P.W.; Yang, W.L.; Chen, Y.L.; Shih, Y.N.; Wang, H.J. Fundamentals of Pharmacokinetics to Assess the Correlation Between Plasma Drug Concentrations and Different Blood Sampling Methods. Pharm. Res. 2019, 36, 1–15. [Google Scholar] [CrossRef]
- Shargel, L.; Yu, A.B.C. Applied Biopharmaceutics and Pharmakinetics, 7th ed.; Appleton & Lange Reviews; McGraw-Hill, Medical Pub. Division: New York, NY, USA, 2016. [Google Scholar]
- Davies, B.; Morris, T. Physiological Parameters in Laboratory Animals and Humans. Pharm. Res. 1993, 10, 1093–1095. [Google Scholar] [CrossRef] [PubMed]
- Kurlbaum, M.; Högger, P. Plasma Protein Binding of Polyphenols from Maritime Pine Bark Extract (USP). J. Pharm. Biomed. Anal. 2011, 54, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Lee, C.H.; Park, S.J.; Lee, H.S.; Choi, M.K.; Song, I.S. Involvement of Organic Anion Transporters in the Pharmacokinetics and Drug Interaction of Rosmarinic Acid. Pharmaceutics 2021, 13, 83. [Google Scholar] [CrossRef] [PubMed]
- Azuma, K.; Ippoushi, K.; Nakayama, M.; Ito, H.; Higashio, H.; Terao, J. Absorption of Chlorogenic Acid and Caffeic Acid in Rats after Oral Administration. J. Agric. Food Chem. 2000, 48, 5496–5500. [Google Scholar] [CrossRef]
- Yan, N.; Tang, Z.; Xu, Y.; Li, X.; Wang, Q. Pharmacokinetic Study of Ferulic Acid Following Transdermal or Intragastric Administration in Rats. AAPS PharmSciTech 2020, 21, 1–7. [Google Scholar] [CrossRef]
- Kishida, K.; Matsumoto, H. Urinary Excretion Rate and Bioavailability of Chlorogenic Acid, Caffeic Acid, p-Coumaric Acid, and Ferulic Acid in Non-Fasted Rats Maintained under Physiological Conditions. Heliyon 2019, 5, e02708. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, R.; Srai, S.K.; Debnam, E.; Rice-Evans, C.A. Urinary Excretion of Hydroxycinnamates and Flavonoids after Oral and Intravenous Administration. Free Radic. Biol. Med. 1999, 27, 278–286. [Google Scholar] [CrossRef]
- Stompor-Goracy, M.; Machaczka, M. Recent advances in biological activity, new formulations and prodrugs of ferulic acid. Int. J. Mol. Sci. 2021, 22, 12889. [Google Scholar] [CrossRef] [PubMed]
- Veras, K.S.; Fachel, F.N.S.; Teixeira, H.F.; Koester, L.S. Technological strategies applied for rosmarinic acid delivery through different routes—A review. J. Drug Deliv. Sci. Technol. 2022, 69, 103054. [Google Scholar] [CrossRef]
- Shukla, D.; Nandi, N.K.; Singh, B.; Singh, A.; Kumar, B.; Narang, R.K.; Singh, C. Ferulic acid-loaded drug delivery systems for biomedical applications. J. Drug Deliv. Sci. Technol. 2022, 75, 103621. [Google Scholar] [CrossRef]



| HCA | Animal Species | Dose (mg/kg) | Cmax (mg/L) | Tmax (h) | t1/2 (h) | MRT0→∞ (h) | AUC0→∞ (mg h/L) | Vd (L/kg) | Cl (L/h kg) | AUC0→∞/Dose | F (%) | References |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CA | Sprague-Dawley rats | 120.0 | - | - | absorption: 0.08 α: 0.14 β: 3.14 | - | 278.3 | 0.518 | 0.115 | 2.32 | 26.54 | [146] |
| CA | Wistar rats | 18.0 | 2.023 a 0.409 b | 0.17 a 0.17 b | 0.58 a 0.57 b | - - | 1.755 a,c 0.329 b,c | - - | - - | 0.0975 a,c 0.0183 b,c | - - | [147] |
| CA | Sprague-Dawley rats | 20.0 | 7.871 | 0.33 | 1.25 | 1.72 | 14.03 | - | 0.702 | 3.4 | [148] | |
| CA | Sprague–Dawley rats | 10.0 | 0.25 | 0.33 | β: 2.13 | 2.96 | 0.355 | 2.41 | 3.35 | 0.0355 | 14.7 | [141] |
| CGA | Wistar rats | 50.0 | 0.55 | 0.48 | 1.7 | - | 1.61 | 97.5 | 39 | 0.003 | - | [149] |
| CGA | Sprague–Dawley rats | 1.0 2.0 4.0 8.0 | 0.00245 0.00912 0.019 0.021 | 0.25 0.5 1.5 0.75 | - - - - | - - - - | 0.0078 c 0.017 c 0.041 c 0.065 c | - - - - | 0.618–0.726 | 0.0078 0.0085 0.0103 0.0081 | 0.478 0.522 0.718 0.569 | [150] |
| CGA | Wistar rats | 240.0 | 1.855 | 0.5 | - | - | - | - | - | - | - | [151] |
| CGA | Kunming mices | 1200.0 | 82.6 | 0.17 | - | - | 51.388 c | - | - | 0.0428 | - | [152] |
| p-COA | Sprague-Dawley rats | 16.4 | 27.17 a 16.29 b | 0.17 a 0.17 b | 0.27 a - | - - | 8.176 a,c - | - - | - - | 0.499 a - | - - | [153] |
| p-COA | Wistar rats | 2.35 | 3.15 | 0.17 | 1.28 | - | 2.32 | - | - | 0.987 | 51.8 | [75] |
| p-COA | Wistar rats | 7.38 | 4.29 | 0.18 | 0.77 | - | 2.502 | - | - | 0.339 | - | [154] |
| p-COA | Human | 258 * | 0.02195 | 0.5 | 0.9 | - | 0.2082 | - | - | 0.00008 | - | [155] |
| FA | Sprague-Dawley rats | 10.0 | 8.175 | 0.03 | absorption: 0.07 α: 0.16 β: 1.77 | - | 2.962 | - | - | 0.296 | - | [156] |
| FA | Sprague-Dawley rats | 80.0 | 9.98 | 1.33 | 2.14 | 3.33 | 34.75 | - | - | 0.434 | - | [157] |
| FA | Wistar rats | 40.0 | 73.2 | 0.58 | 1.39 | 1.40 d | 82.86 c | 1.22 × 106 | 2.5 × 105 | 2.072 | - | [158] |
| RA | Sprague-Dawley rats | 50.0 | 1.667 | 0.5 | - | - | - | - | - | - | - | [159] |
| RA | Wistar rats | 36.0 | 0.489 a 0.166 b | 0.17 a 0.08 b | 0.95 a 1.1 b | - - | 0.3624 a,c 0.0996 b,c | - - | - - | 0.01 a,c 0.003 a,c | - - | [147] |
| RA | Sprague-Dawley rats | 50.0 | 0.327 | 0.33 | 6.77 | - | 1.395 | - | - | 0.028 | - | [105] |
| RA | Sprague-Dawley rats | 12.5 25.0 50.0 | 0.215 0.362 0.791 | 0.14 0.18 0.31 | 5.54 5.24 4.92 | 7.32 7.25 6.11 | 0.867 1.310 1.867 | 111.83 141.81 197.65 | 15 19.2 27.6 | 0.069 0.053 0.037 | 1.69 1.28 0.91 | [160] |
| RA | Sprague-Dawley rats | 50.0 | 0.416 | 0.15 | 5.02 | - | 1.246 | - | - | 0.025 | - | [161] |
| RA | Sprague-Dawley rats | 50.0 | 1.088 | 0.19 | 1.34 | 1.57 | 0.972 | - | - | 0.019 | 4.13 | [162] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veras, K.S.; Fachel, F.N.S.; de Araújo, B.V.; Teixeira, H.F.; Koester, L.S. Oral Pharmacokinetics of Hydroxycinnamic Acids: An Updated Review. Pharmaceutics 2022, 14, 2663. https://doi.org/10.3390/pharmaceutics14122663
Veras KS, Fachel FNS, de Araújo BV, Teixeira HF, Koester LS. Oral Pharmacokinetics of Hydroxycinnamic Acids: An Updated Review. Pharmaceutics. 2022; 14(12):2663. https://doi.org/10.3390/pharmaceutics14122663
Chicago/Turabian StyleVeras, Kleyton Santos, Flávia Nathiely Silveira Fachel, Bibiana Verlindo de Araújo, Helder Ferreira Teixeira, and Letícia Scherer Koester. 2022. "Oral Pharmacokinetics of Hydroxycinnamic Acids: An Updated Review" Pharmaceutics 14, no. 12: 2663. https://doi.org/10.3390/pharmaceutics14122663
APA StyleVeras, K. S., Fachel, F. N. S., de Araújo, B. V., Teixeira, H. F., & Koester, L. S. (2022). Oral Pharmacokinetics of Hydroxycinnamic Acids: An Updated Review. Pharmaceutics, 14(12), 2663. https://doi.org/10.3390/pharmaceutics14122663