1. Introduction
Primary open-angle glaucoma (POAG) is the second leading cause of blindness, affecting over 50 million people worldwide [
1,
2]. POAG is mainly induced by the accumulation of aqueous humour in the anterior chamber of the eye, causing elevated intraocular pressure (IOP). The increase in IOP causes mechanical stress to the posterior segment of the eye, and is correlated to retinal ganglion cell death [
3]. POAG is insidious, as it is painless, i.e., the patients do not feel symptoms until damage is already done to the optic nerve fibers, resulting in irreversible vision loss [
4,
5]. Therefore, management of IOP is essential for the wellbeing of POAG patients.
Various pharmacological agents exist, either reducing aqueous humour production (beta-blockers, alpha agonists, carbonic anhydrase inhibitors) or enhancing its elimination (prostaglandin analogues, muscarinic agonists) [
6,
7]. Today, the two most effective pharmacological classes are beta-blockers and prostaglandin analogues, which both present some drawbacks [
7,
8]. On one hand, beta-blockers are contraindicated for patients with asthma or with a history of cardiac disease. On the other hand, prostaglandin analogues rely on preservatives, such as benzalkonium chloride (BAK) or polyquaternium, for their solubilization which can cause redness of the eye as well as corneal inflammation upon repeated administration [
7,
9,
10,
11,
12,
13,
14]. The choice of treatment in the first intention is left to the practitioner, often leading to the use of prostaglandin analogues [
8,
15].
With current packaging technologies, such as single-dose or preservative-free eye drops (PFED) in multidose bottles, the use of preservatives is outdated. In terms of efficacy, PFED formulations are not inferior to formulas containing BAK [
13]. Therefore, prostaglandin analogues are reformulated without the use of preservatives as stabilizers and solubilizers [
10,
16], often using ricin oil or propylene glycol as cosolvent [
12]. Indeed, PFED formulations were shown to have a better ocular tolerance, especially regarding surface parameters such as an increased tear break-up time or less burning/stinging sensation upon instillation [
11,
12,
13]. Better ocular tolerance is particularly important as it will lead to a better patient adherence and a more successful management of the IOP, hence delaying onset of irreversible symptoms such as vision loss. Polysorbate 80 (PS80) is a surfactant used in the commercial eye-drops Restasis
® as a solubilizer for cyclosporine [
17,
18], it could be used as a substitute for BAK and potentially be better tolerated than both BAK and ricin oil, as brought to light by Fukuda et al. during in vitro/in vivo studies [
19,
20].
Another key excipient identified for the development of a prostaglandin analogue formulation is sodium hyaluronate (NaHA). Indeed, this high molecular weight polymer has two interesting features. First, it can increase the viscosity of the final formulation which is considered an asset for ocular drug delivery, as it can compensate for the fast clearance of the tear film [
21]. Secondly, NaHA has been proven to have a cytoprotective effect on the corneal surface [
22,
23,
24], which can be altered by prostaglandin analogue treatment [
25]. Therefore, the aim of this work is to evaluate PS80 as a solubilizing agent for prostaglandin analogues, coupled with NaHA for its cytoprotective and thickening effects.
2. Materials and Methods
2.1. Materials
Pyrene 98% purity was purchased from Acros Organics (Illkirch, France). Latanoprost and travoprost were kindly provided by Sanofi Chinoin (Budapest, Hungary). High molecular weight sodium hyaluronate (NaHA) SZE grade, with an intrinsic viscosity of 2.5 m3/kg was purchased from Shiseido CO., LTD. (Kakegawa-shi, Japan). Polysorbate 80 (PS80), Protasorb™ O-20-NF, was purchased from Protameen Chemicals (Totowa, NJ, USA). NMR Deuterium oxide (D2O) 99.8% purity was purchased from Carlo Erba reagents S.A.S. (Milano, Italy). Sodium dihydrogenphosphate (NaH2PO4), disodium hydrogen phosphate (Na2HPO4), sodium chloride (NaCl), calcium chloride dihydrate (CaCl2·2H2O), magnesium chloride (MgCl2), potassium chloride (KCl), sodium bicarbonate (NaHCO3), and acetonitrile were purchased from Sigma Aldrich (Saint-Quentin Fallavier, France). Travatan® commercial solution was purchased from Alcon® (Hünenberg, Switzerland).
2.2. Fluorescence Spectroscopy
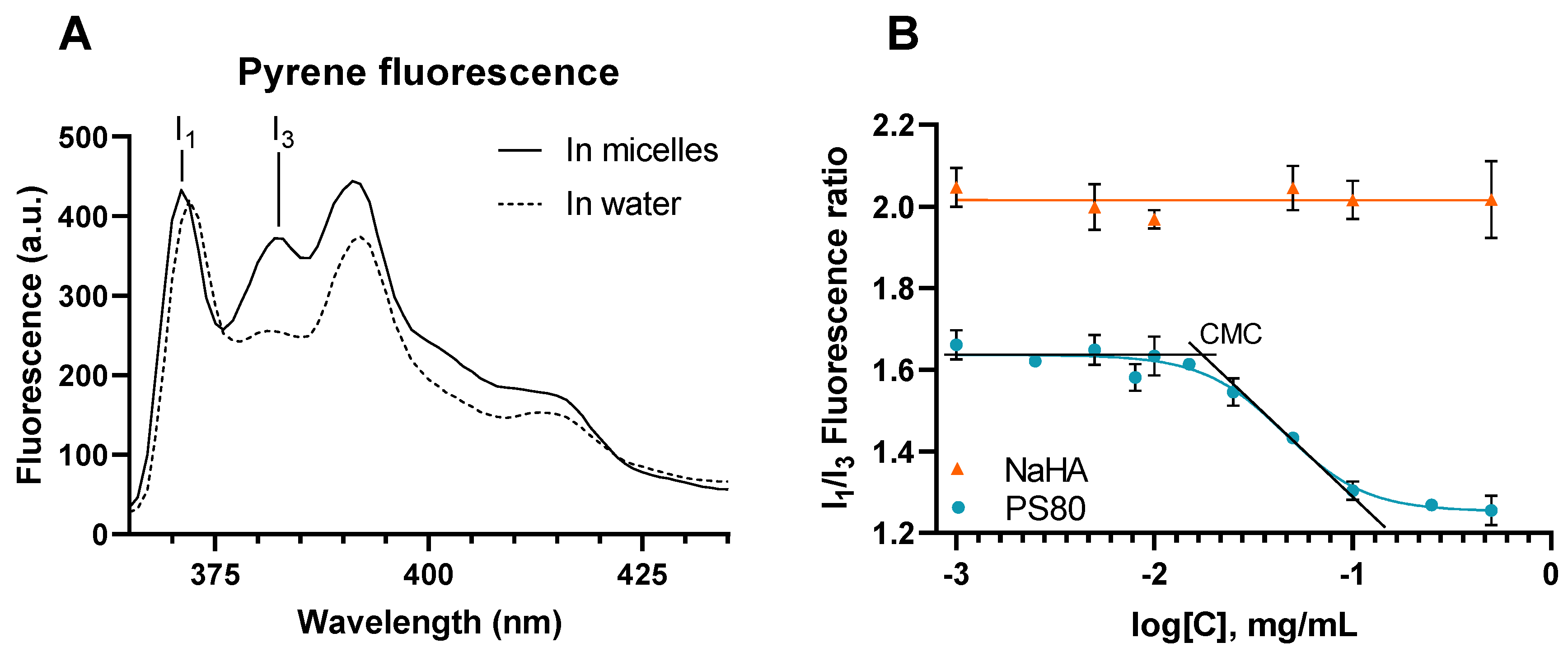
Pyrene is a lipophilic fluorescent probe often used to determine the critical micellar concentration (CMC) of surfactants. Indeed, it has the interesting feature of being sensitive to the polarity of its environment and partitioning into micelles leading to an hyperchromicity [
26]. First, 40 mg of pyrene were dissolved into 10 mL of ethanol, this solution was diluted in water to achieve a stock solution with a concentration of 7.5 µM. This stock solution was used as solvent to prepare PS80 and NaHA solutions of different concentrations in triplicate. Fluorescence measurements were performed using a Varian Cary Eclipse fluorescence spectrophotometer and processed with the Cary Eclipse software version 1.1.132 (Agilent Technologies, Santa Clara, CA, USA). The data were acquired using an excitation wavelength of 230 nm with a 20 nm slit and by recording an emission scan from 350 to 450 nm with a 2.5 nm slit. Peaks 1 and 3, used to determine the fluorescence ratio I
1/I
3, were at approximately 372 and 383 nm, respectively. PS80 CMC was determined using a sigmoidal non-linear variable slope regression performed using GraphPad Prism version 8.0.2 for windows (GraphPad Software, San Diego, CA, USA). CMC was considered as the abscissa of the point at which the top of the sigmoid and the tangent to the inflection point crossed.
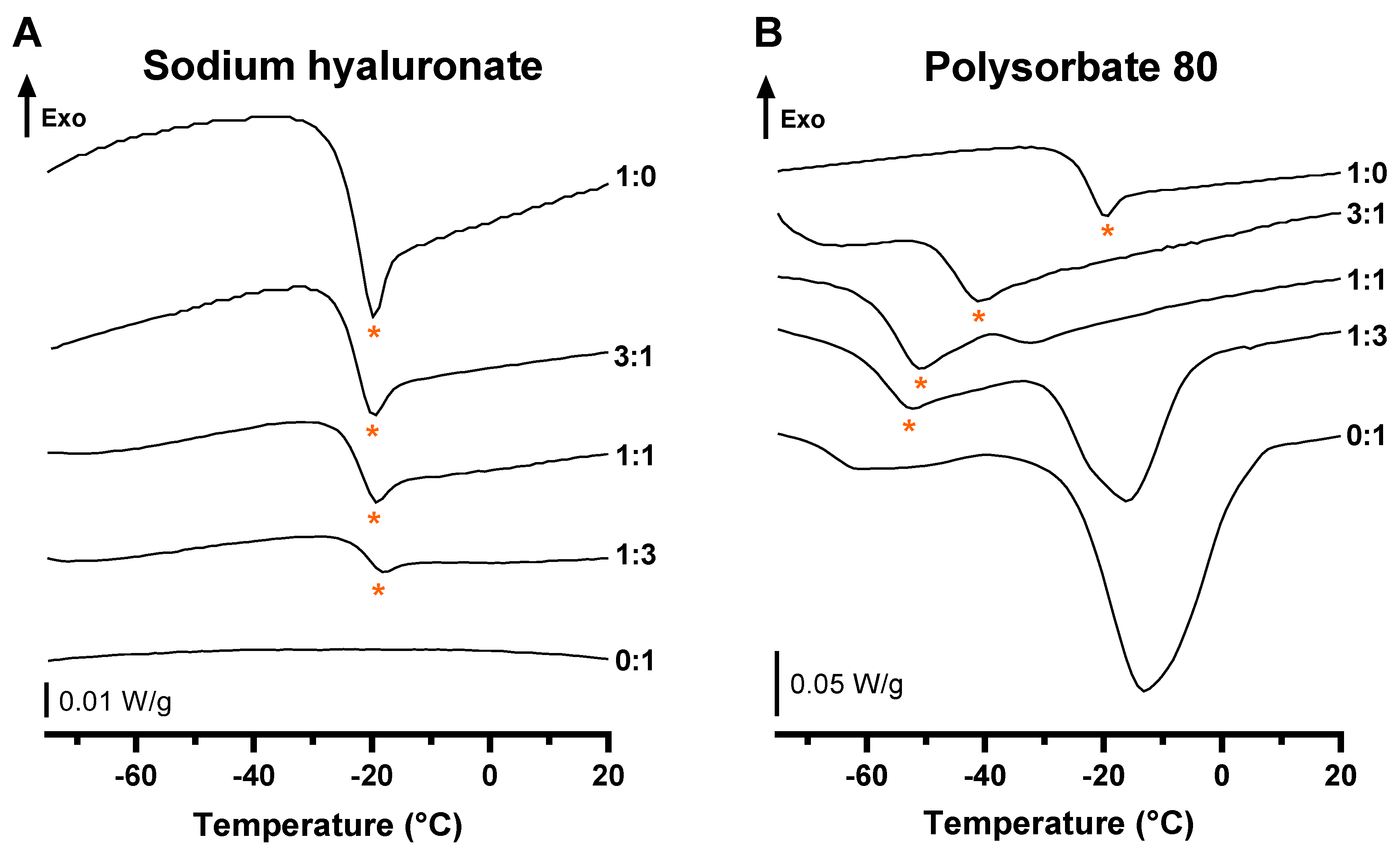
2.3. Differential Scanning Calorimetry (DSC)
The differential scanning calorimetry (DSC) studies were performed using a DSC 3 thermal analysis device (Mettler-Toledo GmbH, Greinfensee, Switzerland) calibrated upstream with high-purity zinc (99.99%, Tfus = 419.6 ± 0.7 °C, ΔfusH = 107.5 ± 3.2 J.g−1), high-purity indium (99.99%, Tfus = 156.6 ± 0.3 °C, ΔfusH = 28.45 ± 0.60 J.g−1) and controlled with both, and Milli-Q water (Merck Millipore, Burlington, MA, USA). Each sample was introduced in a 100 µL aluminum pan which was hermetically sealed afterwards. The conditions of the sample preparation, as well as the applied temperature program, were strictly identical to avoid any thermal history dependence of the samples. The cycle, performed twice on each sample, was freezing from ambient temperature to −80 °C at a rate of 5 °C/min, then holding for 3 min at −80 °C, then heating to 25 °C, at a rate of 5 °C/min under a 60 mL/min dry air flow. Travoprost, NaHA and PS80 were analyzed either alone or as binary drug:excipient blends at different weight ratios (1:3, 1:1 and 3:1, respectively). Measurements were performed on 3 independent samples (n = 3). Thermogram evaluation was performed using STARe version 16.30 (Mettler-Toledo GmbH, Greinfensee, Switzerland).
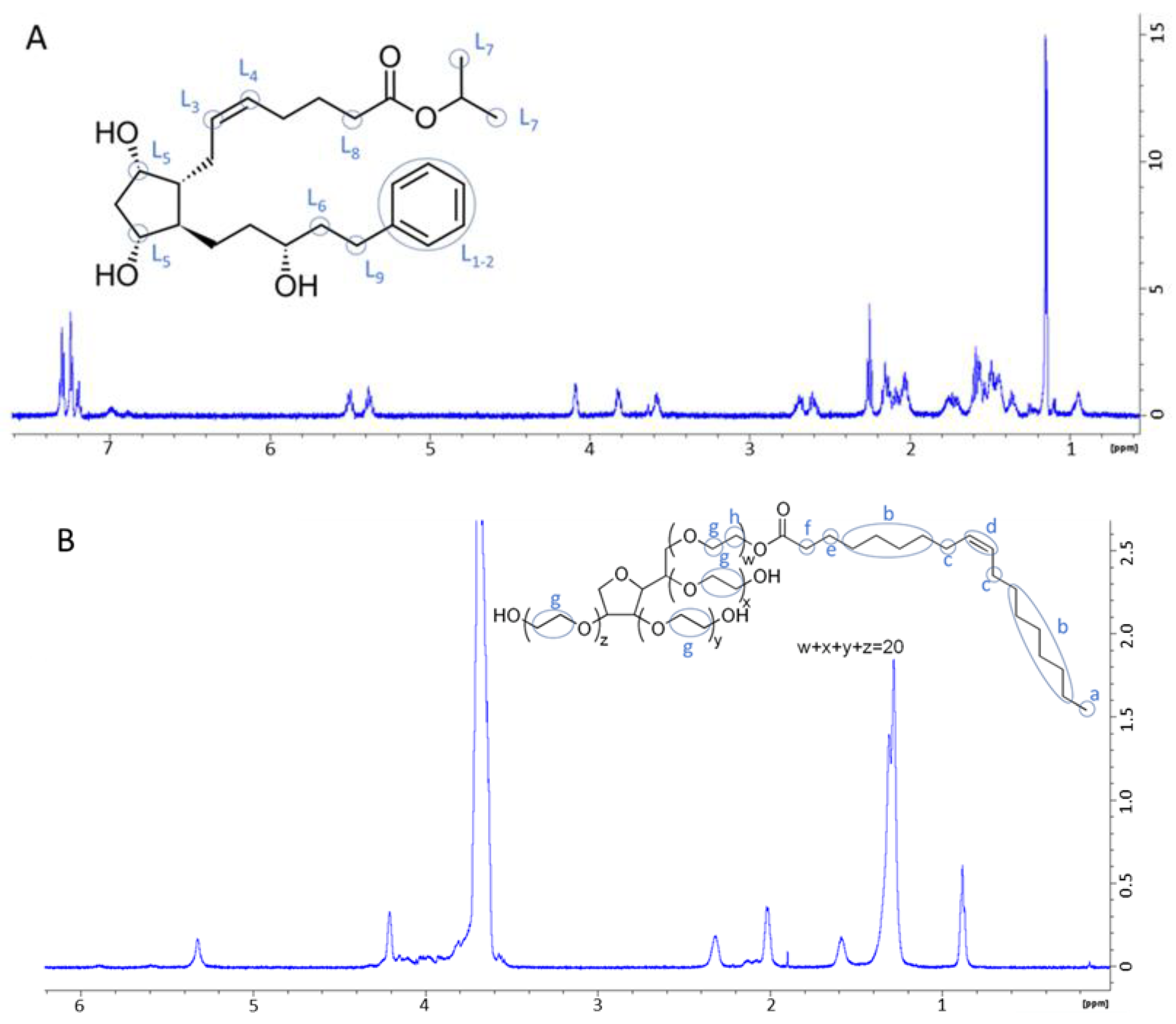
2.4. Nuclear Magnetic Resonance (NMR) Spectroscopy
As the pharmacological class lead, Latanoprost was used for the NMR studies to better transpose results to other prostaglandin analogues. NMR analysis solutions of PS80, latanoprost, as well as 50:50 mixtures, were prepared in D2O. Firstly, 1 mg of liquid raw material or mixture was weighed in a 1.5 mL Eppendorf tube. Secondly, 0.6 mL of D2O was added before vortexing for 2 min. Samples were left resting for 24 h at ambient temperature then vortexed again 2 min prior to transferring into NMR tubes. NMR acquisition was performed using a Bruker NMR Spectrometer (Bruker, Fällanden, Switzerland) operating at a 1H Larmor frequency of 600 MHz, at 25 °C, using a BBI probe. Data were treated using the software Bruker TopSpin version 4.0.9. Samples were studied by one dimensional 1H NMR, as well as 1H-1H correlation spectroscopy (COSY) and 1H-13C heteronuclear single-quantum coherence spectroscopy (HSQC) for signal attribution. Next, 2D rotating frame Overhauser effect spectroscopy (ROESY) experiments were performed to assess intermolecular hydrogen proximity with a mixing time of 600 ms, a recovery delay of 1.5 s, and 256 time increments with 320 scans per increment. The 1H NMR spectra were referenced to the resonance line of HOD at 4.70 ppm.
2.5. Preparation of the Eye Drops
The preservative-free eye drops (PFED) were prepared by a two-step method as described in the patent US 2014 0228364A1 [
27]. First, 400 mg of sodium dihydrogen phosphate, 474 mg of disodium hydrogen phosphate and 473 mg of sodium chloride were dissolved in 100 mL of water for injection. Then, 30 mL of this buffer was used to solubilize 100 mg of NaHA, under magnetic stirring for at least 6 h. Four mg of travoprost and 100 mg of PS80 were added to the NaHA solution and mixed for 30 min until complete dissolution. The last 70 mL of the phosphate buffer were added to this travoprost solution and mixed for 90 min. Finally, pH was adjusted to 6.7 with 0.5 M NaOH or HCl and the solution was filtered through a 0.22 µm polyethersulfone (PES) membrane. Final concentrations were 40 µg/mL of travoprost, and 1 mg/mL of sodium hyaluronate and PS80, as shown in
Table 1.
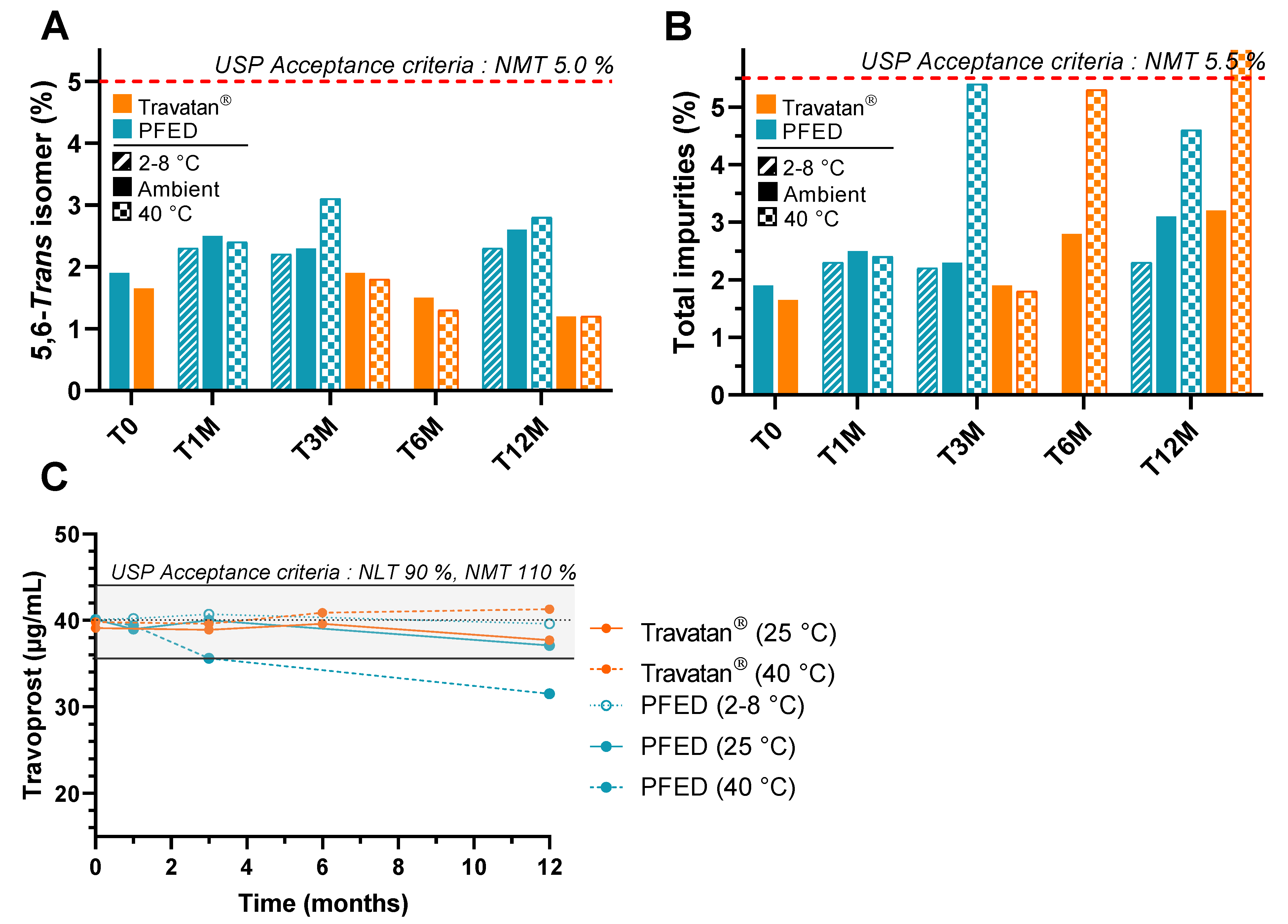
2.6. Stability Study
2.6.1. Design of the Study
The PFED formulation and the comparator were stored in climatic chambers at different temperatures (2–8 °C, 25 °C and 40 °C), protected from daylight. The solutions were assayed by HPLC-UV. Travoprost content, 5,6-trans isomer, 15-keto derivative, and total impurities were used to assess the stability of the eye drops in accordance with the USP monograph for travoprost ophthalmic solutions [
28].
2.6.2. Travoprost HPLC-UV Assay
Samples were diluted at 1:2 in acetonitrile and filtered through a 0.22 µm PTFE syringe filter prior to analysis. Analysis was performed with an HP Agilent 1100 series HPLC system (Santa Clara, CA, USA) and a Raptor C18 5 µm 4.6 × 150 mm column purchased from Restek (Center county, PA, USA). HPLC was carried out at 40 °C with a mobile phase flow rate of 1 mL/min. The mobile phase composition was a gradient of Acetonitrile/Phosphate buffer 10 mM pH 3 from 38/62 to 50/50 v/v from 0 to 26 min, then held at 50/50 v/v from 26 to 29 min, and finally going back to 38/62 v/v from 29 to 40 min. The detection wavelength was set at 200 nm. The calibration curve ranged from 5 to 25 µg/mL. Linearity was assessed by a coefficient of determination R2 > 0.995, as well as a back-calculated bias of less than 5% for each concentration point of the standard curve. Accuracy was evaluated by a recovery of control samples at a target concentration between 95 and 105%. Precision was confirmed with a coefficient of variation inferior to 3% for control samples. Repeatability of injection was inferior to 0.4%.
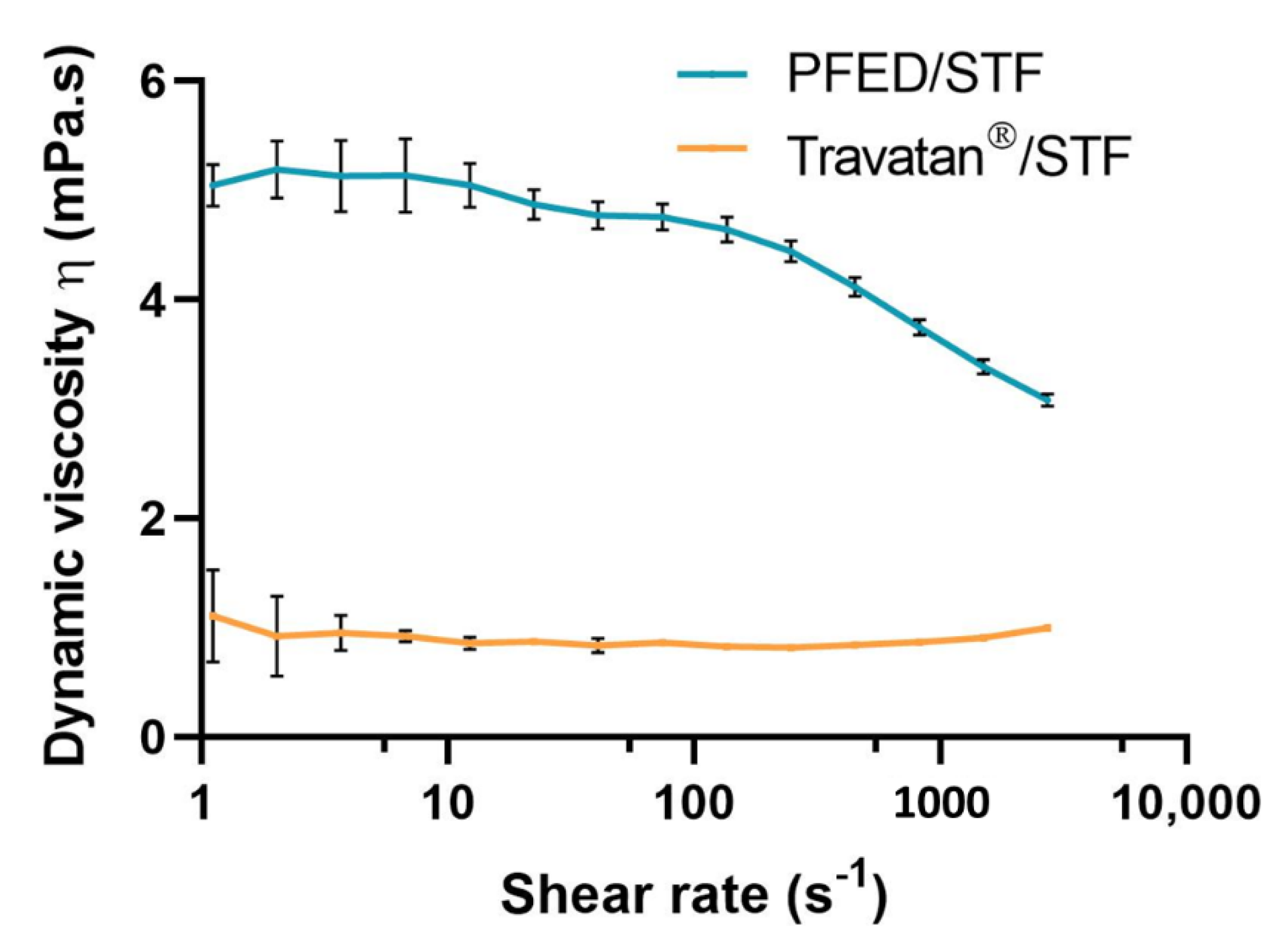
2.7. Rheological Studies
Dynamic viscosity, η, was measured for the PFED formulation and Travatan
®. In order to have a more biorelevant measure, samples were diluted in simulated tear fluid (STF), mimicking the dilution upon instillation. A Sample:STF ratio of 30:7 was used [
29,
30,
31]. The composition of STF used is detailed in
Table 2 below [
32,
33].
Rotational measurements were carried out on a controlled shear rate MCR102 Rheometer and data were analyzed using the Rheocompass™ software version 1.25 (Anton Paar, Graz, Austria). A stainless-steel cone-plate geometry (1° angle, 50 mm diameter, 100 µm gap) was used. Measurements were performed at physiological eye temperature (35 °C) for a shear rate ranging from 1 to 3000 s−1. Results are presented as the mean ± SD of 6 independent experiments.
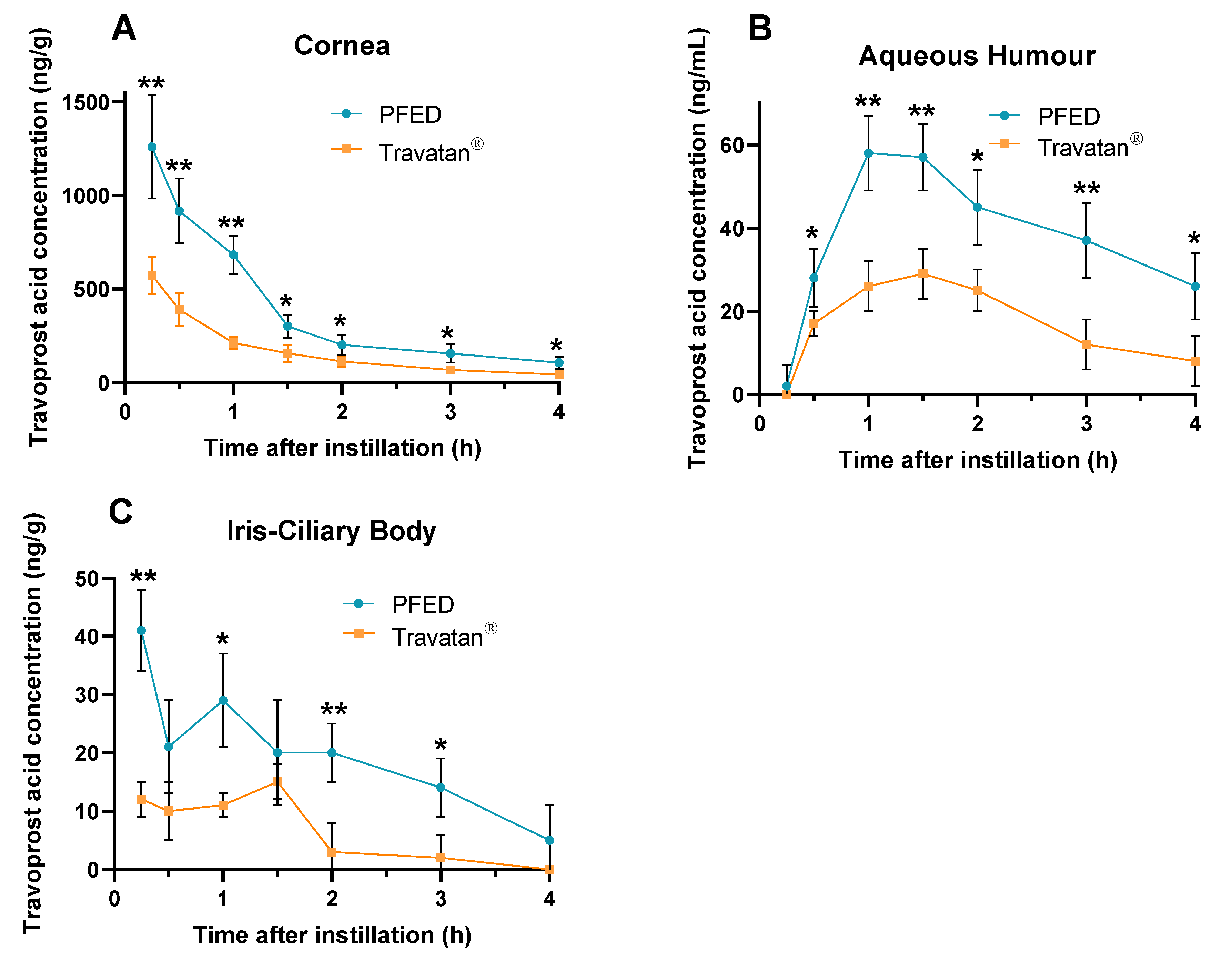
2.8. In Vivo Studies
2.8.1. Design of the Study
The ocular pharmacokinetic study was performed with 42 pigmented Dutch Belted female rabbits, aged 12 to 14 weeks and separated into two groups, one treated with Travatan
® and one treated with PFED. Instillation of 30 µL was completed in both eyes at t = 0 h then, at times 0.25, 0.5, 1, 1.5, 2, 3 and 4 h, three rabbits were euthanized and the aqueous humour (AH), cornea, and iris-ciliary body (ICB) were dissected and assayed for travoprost acid, the active moiety. Cornea, iris and conjunctivae of each eye were examined and rated using the Draize’s scale [
34]. At each point the mean and standard deviation of 6 eyes was represented. To assess the difference between PFED and Travatan
®, an unpaired t-test with Welch’s correction was performed using GraphPad Prism version 8.0.2 for windows (GraphPad Software, San Diego, CA, USA). The area under curve (AUC) was calculated from 0.25 to 4 h using the linear-up log-down trapezoidal rule [
35]. The elimination half-life (t
1/2) for cornea and aqueous humour was determined with the log-linear regression of the tissue concentrations–time curve terminal phase. Composition of Travatan
® is presented in
Table 3 below.
2.8.2. Travoprost acid RRLC-MS/MS Assay
Travoprost acid was quantified in rabbit cornea, iris-ciliary body and aqueous humour using an RRLC-MS/MS method. Travoprost acid was extracted from the samples using ethyl acetate, the obtained solution was dried and reconstituted in 50/50 methanol/water. Chromatographic separation was performed on a Halo C18 2.7 µm 2.1 × 100 mm column (Interchim, San Diego, CA, USA) using an Agilent 1200 series rapid-resolution liquid chromatography (RR-LC) system (Santa Clara, CA, USA). A 10 µL sample was injected and eluted using a mobile phase composed of 40/60 formic acid 0.1% and a mix of acetonitrile/methanol 350/200 v/v at a 0.2 mL/min flow rate. Mass spectrometry detection was performed using an Agilent triple quadrupole 6410 (Santa Clara, CA, USA) with a capillary voltage of 4 kV, a nebulization pressure of 20 psi and a drying gas at 350 °C with a 7 mL/min flow. Calibration curves ranged from 0.05 to 10 ng/10 µL injected, with a coefficient of determination R2 > 0.998.
4. Discussion
We presented, in the first part of this article, preformulation studies regarding the key excipients of the formula NaHA and PS80, and the active substance. To begin, we chose pyrene as a fluorescent probe because its LogP is 6.0 [
39]. Indeed, it was interesting to mimic the behavior of lipophilic drugs such as prostaglandin analogues. This first study showed that the excipient NaHA did not exhibit any affinity for it, therefore showing its lack of physicochemical interaction with liposoluble drugs. This finding was further confirmed by the DSC studies. Indeed, no shifts in the Tg of travoprost occurred with varying ratios of NaHA:Travoprost. This method has been successfully used to predict the compatibility of components within pharmaceutical mixtures [
40,
41,
42]. As no incompatibility was brought to light between travoprost and NaHA, the latter was further used in the final PFED formulation.
On the other hand, for PS80, the fluorescence studies showed a decrease in the I
1/I
3 ratio with increasing PS80 concentrations. The determined CMC of PS80 was approximately 0.019 mg/mL (or 0.015 mM), which is consistent with the literature, ranging from 0.018 mM, determined by surface tension measurement [
43], to 0.015 mM obtained with a fluorescence-based method using the derivative pyrene-3-carboxaldehyde [
44]. Therefore, the observed effect can be attributed to PS80 micelles formation, into which pyrene is integrated, showing PS80 potential to solubilize lipophilic drugs given concentrations higher than the CMC.
Furthermore, DSC studies showed a clear effect of the presence of PS80 on the thermal events. The shift in Tg towards lower values of temperature was similar to the effect of plasticizers in a polymer melt, which testifies to a miscibility of the different molecules as well as an improvement in solubility [
45,
46]. This demonstrated a physicochemical interaction between PS80 and prostaglandin analogues. This result is in accordance with the eutectic effect that was highlighted in the Results section, related to PS80 thermal behavior when mixed with travoprost. PS80 is a non-ionic surfactant, meaning it has both a lipophilic and a hydrophilic moiety. When its concentration is high enough it self-assembles into micelles, grouping the lipophilic parts in its core and exposing the hydrophilic fragment to the surrounding water [
47].
This was further clarified by the NMR studies. Indeed, NMR has previously been used to assess the molecular organization between prostaglandin analogues and solubilizers such as cyclodextrins [
48] or other surfactants [
10]. The orientation suggested in this work seems to be similar to the one explicated by Ochiai et al., suggesting that in micelles of BAK and PEG-Stearate the latanoprost is encapsulated in the hydrophobic core with a preferential orientation, presenting the cyclopentyl fragment towards the hydrophilic parts of the surfactants, therefore limiting its exposure to water [
10]. Besides, NMR studies conducted with NaHA and latanoprost did not display physicochemical interactions in solution.
In the second part of this work, we studied a final product: PFED containing travoprost as an active substance, solubilized and stabilized by PS80, with NaHA as a thickener and potential cytoprotective agent. PS80 has already been used in eye drops as a solubilizer for cyclosporine [
18], and this work confirmed its potential to further solubilize prostaglandin analogues in drug delivery while maintaining stability in solution.
According to the ICH guideline Q1A(R2) on stability studies for drug products, a period of 12 months is the minimum that has to be covered at room temperature (25 °C) at the time of submission [
49]. As the stability results at 40 °C at 12 months were not within the USP criteria, the stability studies at room temperature were the bare minimum for a submission, but would have to be continued for longer periods of time to secure long-term stability data. So far, however, the PS80 and NaHA seem to be satisfying excipients regarding the travoprost stability at room temperature.
Rotational rheological studies were performed to assess the dynamic viscosity of PFED and Travatan
® upon instillation. Travatan
® exhibited a Newtonian-like behavior with a constant viscosity over the shear rate range analyzed. The mean viscosity of 0.9 mPa·s at 35 °C was slightly higher than pure water at this temperature (0.7 mPa·s) [
50]. Therefore, it is expected that, upon instillation, Travatan
® will rapidly mix with tear fluid [
51,
52,
53]. The first challenge in ocular drug delivery is to overcome the high clearance of lacrimal fluid upon instillation. It has been reported that the tear fluid is entirely renewed within 2–3 min under physiological conditions, therefore leading to a fast clearance of the eye drops [
54,
55]. On the other hand, an increase in viscosity, as displayed for PFED, can lengthen the residence time of the eye drop on the ocular surface [
30,
55,
56,
57]. Indeed, NaHA was added to the eye drop formulation to thicken the solution. As expected, adding a high molecular weight polymer increased the viscosity at low shear and turned the solution into a shear-thinning fluid [
58,
59].
The in vivo studies conducted on rabbits exhibited an increase in AUC for the three studied structures of the eye, cornea, AH, and ICB. AUC represents the total drug exposure over the studied period. In our study, this improvement in AUC seemed to be linked to a greater absorption of travoprost, as the elimination constants were similar for the PFED and the comparator. This greater AUC observed after single-drop instillation of PFED related to Travatan
® (between 2.2- and 3.2-fold for the AH and the ICB, respectively) could be linked to its rheological behavior. As it was discussed for dry eye formulations containing 0.1% NaHA [
60], the rheological properties of the final dosage can improve its in vivo residence time, therefore extending the exposure time of the cornea to the drug product [
30,
52,
53]. Another mechanism could be involved into this enhanced ocular bioavailability. Indeed, PS80 has been reported to improve travoprost uptake in vivo in rabbits in a nano-emulsion drug formulation compared to Travatan
® [
61]. Further studies, such as a permeability study or an evaluation of the residence time, could unveil the relative contribution of these two mechanisms on the AUC increase. With such an increase in ocular bioavailability, the therapeutic dose of travoprost could potentially be lowered [
62,
63]; therefore, limiting systemic exposition and side effects while maintaining the therapeutic effect.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}