
Real-Life Therapeutic Concentration Monitoring of Long-Acting Cabotegravir and Rilpivirine: Preliminary Results of an Ongoing Prospective Observational Study in Switzerland

 , , , ,
, , , ,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcomes
2.3. Drug Level Measurements
2.4. Pharmacokinetic Modelling
3. Preliminary Results
3.1. Study Population
3.2. Adverse Events
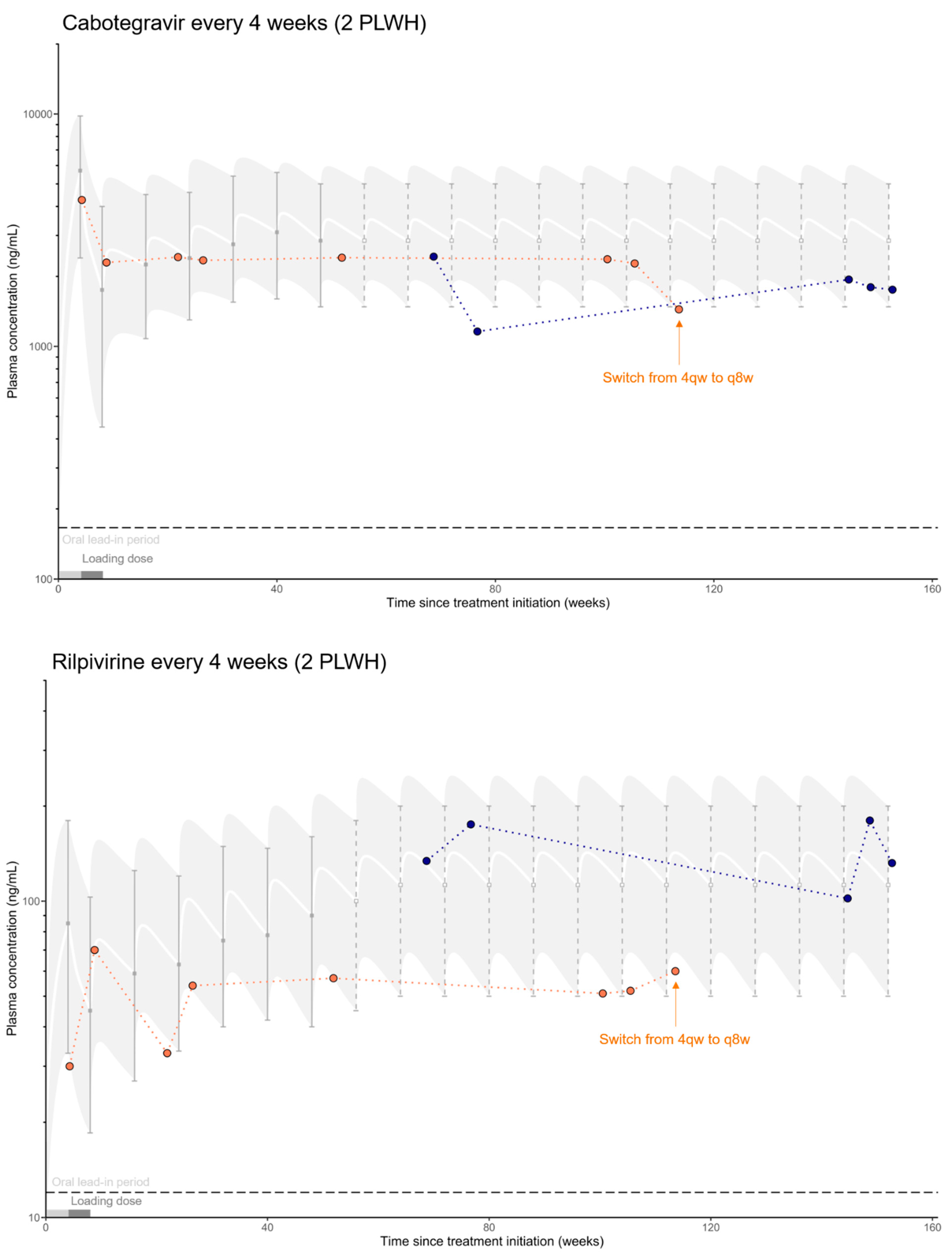
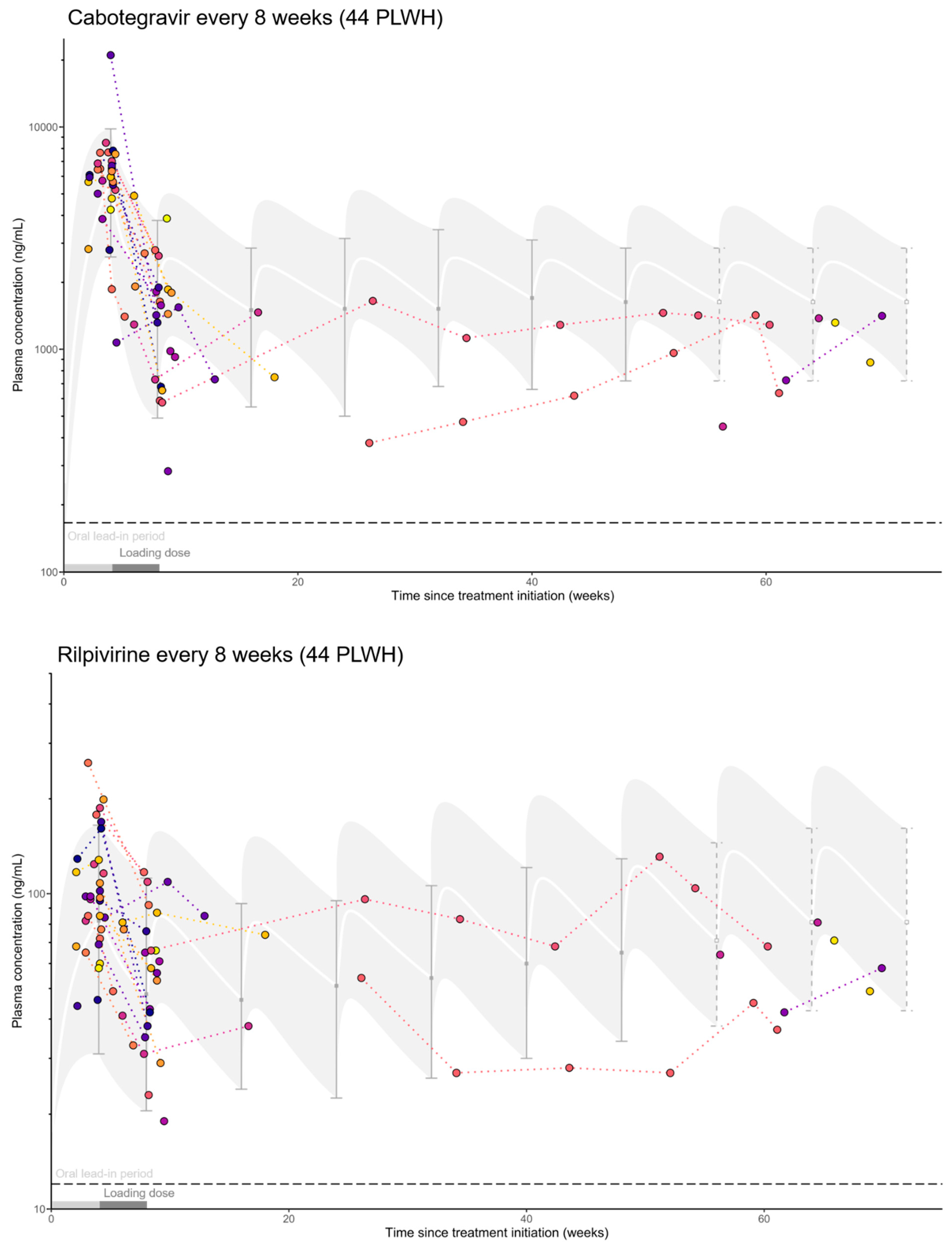
3.3. Pharmacokinetics
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thoueille, P.; Choong, E.; Cavassini, M.; Buclin, T.; Decosterd, L.A. Long-acting antiretrovirals: A new era for the management and prevention of HIV infection. J. Antimicrob. Chemother. 2022, 77, 290–302. [Google Scholar] [CrossRef] [PubMed]
- ViiV Healthcare. Product Monograph of Vocabria and Cabenuva. 2020. Available online: https://viivhealthcare.com/content/dam/cf-viiv/viiv-healthcare/en_GB/medicines/CABENUVA-VOCABRIA-PM-26-Mar-2021.pdf (accessed on 22 April 2022).
- Hodge, D.; Back, D.J.; Gibbons, S.; Khoo, S.H.; Marzolini, C. Pharmacokinetics and drug–drug interactions of long-acting intramuscular cabotegravir and rilpivirine. Clin. Pharm. 2021, 60, 835–853. [Google Scholar] [CrossRef] [PubMed]
- FDA Approves First Injectable Treatment for HIV Pre-Exposure Prevention. U.S. Food & Drug Administration, 20 December 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-injectable-treatment-hiv-pre-exposure-prevention (accessed on 28 April 2022).
- Margolis, D.A.; Gonzalez-Garcia, J.; Stellbrink, H.J.; Eron, J.J.; Yazdanpanah, Y.; Podzamczer, D.; Lutz, T.; Angel, J.B.; Richmond, G.J.; Clotet, B.; et al. Long-acting intramuscular cabotegravir and rilpivirine in adults with HIV-1 infection (LATTE-2): 96-week results of a randomised, open-label, phase 2b, non-inferiority trial. Lancet 2017, 390, 1499–1510. [Google Scholar] [CrossRef]
- Orkin, C.; Arasteh, K.; Górgolas Hernández-Mora, M.; Pokrovsky, V.; Overton, E.T.; Girard, P.M.; Oka, S.; Walmsley, S.; Bettacchi, C.; Brinson, C.; et al. Long-acting cabotegravir and rilpivirine after oral induction for HIV-1 infection. N. Engl. J. Med. 2020, 382, 1124–1135. [Google Scholar] [CrossRef]
- Swindells, S.; Andrade-Villanueva, J.F.; Richmond, G.J.; Rizzardini, G.; Baumgarten, A.; Masiá, M.; Latiff, G.; Pokrovsky, V.; Bredeek, F.; Smith, G.; et al. Long-acting cabotegravir and rilpivirine for maintenance of HIV-1 suppression. N. Engl. J. Med. 2020, 382, 1112–1123. [Google Scholar] [CrossRef]
- Overton, E.T.; Richmond, G.; Rizzardini, G.; Jaeger, H.; Orrell, C.; Nagimova, F.; Bredeek, F.; García Deltoro, M.; Swindells, S.; Andrade-Villanueva, J.F.; et al. Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: A randomised, multicentre, open-label, phase 3b, non-inferiority study. Lancet 2021, 396, 1994–2005. [Google Scholar] [CrossRef]
- Cutrell, A.G.; Schapiro, J.M.; Perno, C.F.; Kuritzkes, D.R.; Quercia, R.; Patel, P.; Polli, J.W.; Dorey, D.; Wang, Y.; Wu, S.; et al. Exploring predictors of HIV-1 virologic failure to long-acting cabotegravir and rilpivirine: A multivariable analysis. AIDS 2021, 35, 1333–1342. [Google Scholar] [CrossRef]
- Punyawudho, B.; Singkham, N.; Thammajaruk, N.; Dalodom, T.; Kerr, S.J.; Burger, D.M.; Ruxrungtham, K. Therapeutic drug monitoring of antiretroviral drugs in HIV-infected patients. Expert. Rev. Clin. Pharm. 2016, 9, 1583–1595. [Google Scholar] [CrossRef]
- Neyens, M.; Crauwels, H.M.; Perez-Ruixo, J.J.; Rossenu, S. Population pharmacokinetics of the rilpivirine long-acting formulation after intramuscular dosing in healthy subjects and people living with HIV. J. Antimicrob. Chemother. 2021, 76, 3255–3262. [Google Scholar] [CrossRef]
- Han, K.; Patel, P.; Baker, M.; Margolis, D.; Spreen, W.; Ford, S. Population pharmacokinetics of cabotegravir in healthy adult subjects and HIV-1 infected patients following administration of oral tablet and long-acting Intramuscular injection. In Proceeding of the 22nd International AIDS Conference, Amsterdam, The Netherlands, 23–27 July 2018. [Google Scholar]
- Scherrer, A.U.; Traytel, A.; Braun, D.L.; Calmy, A.; Battegay, M.; Cavassini, M.; Furrer, H.; Schmid, P.; Bernasconi, E.; Stoeckle, M.; et al. Cohort profile update: The swiss HIV cohort study (SHCS). Int. J. Epidemiol. 2022, 51, 33j–34j. [Google Scholar] [CrossRef]
- Swiss HIV Cohort Study. Available online: http://www.shcs.ch/ (accessed on 27 May 2022).
- Compendium.ch. VOCABRIA Depot Susp Inj 600 mg/3 mL. Approved by Swissmedic. Available online: https://compendium.ch/product/1484015-vocabria-depot-susp-inj-600-mg-3ml (accessed on 22 April 2022).
- Compendium.ch. REKAMBYS Depot Susp Inj 900 mg/3 mL. Approved by Swissmedic. Available online: https://compendium.ch/product/1483717-rekambys-depot-susp-inj-900-mg-3ml (accessed on 22 April 2022).
- Surve, D.H.; Jindal, A.B. Recent advances in long-acting nanoformulations for delivery of antiretroviral drugs. J. Control. Release 2020, 324, 379–404. [Google Scholar] [CrossRef]
- Courlet, P.; Alves Saldanha, S.; Cavassini, M.; Marzolini, C.; Choong, E.; Csajka, C.; Günthard, H.F.; André, P.; Buclin, T.; Desfontaine, V.; et al. Development and validation of a multiplex UHPLC-MS/MS assay with stable isotopic internal standards for the monitoring of the plasma concentrations of the antiretroviral drugs bictegravir, cabotegravir, doravirine, and rilpivirine in people living with HIV. J. Mass Spectrom 2020, 55, e4506. [Google Scholar] [CrossRef]
- Colombo, S.; Beguin, A.; Telenti, A.; Biollaz, J.; Buclin, T.; Rochat, B.; Decosterd, L.A. Intracellular measurements of anti-HIV drugs indinavir, amprenavir, saquinavir, ritonavir, nelfinavir, lopinavir, atazanavir, efavirenz and nevirapine in peripheral blood mononuclear cells by liquid chromatography coupled to tandem mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2005, 819, 259–276. [Google Scholar] [CrossRef]
- Fayet Mello, A.; Buclin, T.; Franc, C.; Colombo, S.; Cruchon, S.; Guignard, N.; Biollaz, J.; Telenti, A.; Decosterd, L.A.; Cavassini, M. Cell disposition of raltegravir and newer antiretrovirals in HIV-infected patients: High inter-individual variability in raltegravir cellular penetration. J. Antimicrob. Chemother. 2011, 66, 1573–1581. [Google Scholar] [CrossRef] [Green Version]
- BD Vacutainer® CPT™ Cell Preparation Tube with Sodium Citrate for the Separation of Mononuclear Cells from Whole Blood. Becton, Dickinson and Co.: Franklin Lakes, NJ, USA. Available online: https://www.bdj.co.jp/pas/products/mekkin/1f3pro00000r5drz-att/bd-cpt-manual-362760-362761.pdf (accessed on 22 April 2022).
- Barrett, J.S.; Labbe, L.; Pfister, M. Application and impact of population pharmacokinetics in the assessment of antiretroviral pharmacotherapy. Clin. Pharm. 2005, 44, 591–625. [Google Scholar] [CrossRef]
- Sheiner, L.B.; Ludden, T.M. Population pharmacokinetics/dynamics. Annu. Rev. Pharm. Toxicol. 1992, 32, 185–209. [Google Scholar] [CrossRef]
- Buclin, T.; Thoma, Y.; Widmer, N.; André, P.; Guidi, M.; Csajka, C.; Decosterd, L.A. The steps to therapeutic drug monitoring: A structured approach illustrated with imatinib. Front. Pharm. 2020, 11, 177. [Google Scholar] [CrossRef]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Orkin, C.; Oka, S.; Philibert, P.; Brinson, C.; Bassa, A.; Gusev, D.; Degen, O.; García, J.G.; Morell, E.B.; Tan, D.H.S.; et al. Long-acting cabotegravir plus rilpivirine for treatment in adults with HIV-1 infection: 96-week results of the randomised, open-label, phase 3 FLAIR study. Lancet HIV 2021, 8, e185–e196. [Google Scholar] [CrossRef]
- University of Liverpool. Cabotegravir (IM) PK Fact Sheet. Produced February 2021. Available online: https://liverpool-hiv-hep.s3.amazonaws.com/prescribing_resources/pdfs/000/000/171/original/HIV_FactSheet_CAB_IM_2021_Feb.pdf?1632406449 (accessed on 9 May 2022).
- University of Liverpool. Rilpivirine (IM) PK Fact Sheet. Produced February 2021. Available online: www.hiv-druginteractions.org/prescribing_resources/hiv-pk-rilpivirine-im (accessed on 9 May 2022).
- Landovitz, R.J.; Li, S.; Grinsztejn, B.; Dawood, H.; Liu, A.Y.; Magnus, M.; Hosseinipour, M.C.; Panchia, R.; Cottle, L.; Chau, G.; et al. Safety, tolerability, and pharmacokinetics of long-acting injectable cabotegravir in low-risk HIV-uninfected individuals: HPTN 077, a phase 2a randomized controlled trial. PLoS Med. 2018, 15, e1002690. [Google Scholar] [CrossRef] [Green Version]
- Margolis, D.A.; Brinson, C.C.; Smith, G.H.R.; de Vente, J.; Hagins, D.P.; Eron, J.J.; Griffith, S.K.; Clair, M.H.S.; Stevens, M.C.; Williams, P.E.; et al. Cabotegravir plus rilpivirine, once a day, after induction with cabotegravir plus nucleoside reverse transcriptase inhibitors in antiretroviral-naive adults with HIV-1 infection (LATTE): A randomised, phase 2b, dose-ranging trial. Lancet Infect. Dis. 2015, 15, 1145–1155. [Google Scholar] [CrossRef]
- Azijn, H.; Tirry, I.; Vingerhoets, J.; de Bethune, M.P.; Kraus, G.; Boven, K.; Jochmans, D.; Van Craenenbroeck, E.; Picchio, G.; Rimsky, L.T. TMC278, a next-generation nonnucleoside reverse transcriptase inhibitor (NNRTI), active against wild-type and NNRTI-resistant HIV-1. Antimicrob. Agents Chemother. 2010, 54, 718–727. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency (EMA). BIKTARVY Film-Coated Tablets. Summary of the Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/biktarvy-epar-product-information_en.pdf (accessed on 4 May 2022).
- Aouri, M.; Barcelo, C.; Guidi, M.; Rotger, M.; Cavassini, M.; Hizrel, C.; Buclin, T.; Decosterd, L.A.; Csajka, C.; Swiss, H.I.V. Cohort Study. Population pharmacokinetics and pharmacogenetics analysis of rilpivirine in HIV-1-infected individuals. Antimicrob. Agents Chemother. 2017, 61, e00899-16. [Google Scholar] [CrossRef] [Green Version]
- Yapa, H.J.A.; Moyle, G.; Else, L.; Khoo, S.; Back, D.; Karolia, Z.; Higgs, C.; Boffito, M. Pharmacokinetics (PK) of tenofovir (TFV), emtricitabine (FTC), and rilpivirine (RPV) over 10 days following drug cessation. In Proceedings of the 14th European Aids Conference, Brussels, Belgium, 16–19 October 2013. [Google Scholar]
- Néant, N.; Solas, C.; Bouazza, N.; Lê, M.P.; Yazdanpanah, Y.; Dhiver, C.; Bregigeon, S.; Mokhtari, S.; Peytavin, G.; Tamalet, C.; et al. Concentration–response model of rilpivirine in a cohort of HIV-1-infected naive and pre-treated patients. J. Antimicrob. Chemother. 2019, 74, 1992–2002. [Google Scholar] [CrossRef]
- de Ronde, W.; Smit, D.L. Anabolic androgenic steroid abuse in young males. Endocr. Connect. 2020, 9, R102–R111. [Google Scholar] [CrossRef] [Green Version]
- Kam, P.C.; Yarrow, M. Anabolic steroid abuse: Physiological and anaesthetic considerations. Anaesthesia 2005, 60, 685–692. [Google Scholar] [CrossRef]
- Cirrincione, L.R.; Huang, K.J. Sex and gender differences in clinical pharmacology: Implications for transgender medicine. Clin. Pharm. Ther. 2021, 110, 897–908. [Google Scholar] [CrossRef]
- Kulkarni, T.A.; Bade, A.N.; Sillman, B.; Shetty, B.L.D.; Wojtkiewicz, M.S.; Gautam, N.; Hilaire, J.R.; Sravanam, S.; Szlachetka, A.; Lamberty, B.G.; et al. A year-long extended release nanoformulated cabotegravir prodrug. Nat. Mater. 2020, 19, 910–920. [Google Scholar] [CrossRef] [PubMed]
- Gautam, N.; McMillan, J.M.; Kumar, D.; Bade, A.N.; Pan, Q.; Kulkarni, T.A.; Li, W.; Sillman, B.; Smith, N.A.; Shetty, B.L.D.; et al. Lipophilic nanocrystal prodrug-release defines the extended pharmacokinetic profiles of a year-long cabotegravir. Nat. Commun. 2021, 12, 3453. [Google Scholar] [CrossRef] [PubMed]
- Hilaire, J.R.; Bade, A.N.; Sillman, B.; Gautam, N.; Herskovitz, J.; Dyavar Shetty, B.L.; Wojtkiewicz, M.S.; Szlachetka, A.; Lamberty, B.G.; Sravanam, S.; et al. Creation of a long-acting rilpivirine prodrug nanoformulation. J. Control. Release 2019, 311–312, 201–211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Population Characteristics Recorded at Last Cohort Visit or Last Sample Collection (n = 46) | Median (Range) or Number (%) | [Missing Data, (%)] |
|---|---|---|
| Demographic characteristics | ||
| Sex: | ||
| Male | 38 (83) | |
| Female | 8 (17) | |
| Ethnicity: | ||
| Caucasian | 29 (63) | |
| Black | 6 (13) | |
| Hispanic American | 3 (7) | |
| Asian | 3 (7) | |
| Unknown | 5 (10) | |
| Age (year) | 45 (28–62) | |
| Body weight (kg) | 83 (63–120) | |
| Height (cm) | 177 (161–189) | |
| BMI (kg/m2) | 26 (19–37) | |
| Physiological characteristics | ||
| Serum creatinine (μmol/L) | 85 (46–131) | [4, (9)] |
| CLCR (mL/min) a | 111 (61–176) | [4, (9)] |
| eGFR (mL/min/1.73 m2) b | 92 (44–145) | [4, (9)] |
| CKD stage (mL/min/1.73 m2) | ||
| G1: ≥90 | 21 (46) | [4, (9)] |
| G2: 60–89 | 19 (41) | |
| G3a: 45–59 | 1 (2) | |
| G3b: 30–44 | 1 (2) | |
| Liver function | ||
| Albumin (g/L) | 44 (36–51) | [17, (37)] |
| Bilirubin (μmol/L) | 7 (3–19) | [13, (28)] |
| AST (UI/L) | 24 (13–44) | [4, (9)] |
| ALT (UI/L) | 26 (9–67) | [4, (9)] |
| Heart blood pressure: | ||
| Diastolic pressure (mmHg) | 80 (60–107) | [4, (9)] |
| Systolic pressure (mmHg) | 130 (108–180) | [4, (9)] |
| Malabsorption after gastrectomy | 1 (2) | |
| HIV molecular biology | ||
| CD4 (cells/mm3) | 667 (191–1192) | [4, (9)] |
| HIV RNA (copies/mL) | ||
| <50 | 43 (94) | [1, (2)] |
| >50 and <200 | 2 (4) | |
| Previous antiretroviral therapy, no. (%): | ||
| Bictegravir/Tenofovir alafenamide/Emtricitabine | 18 (39) | [5, (10)] |
| Elvitegravir/Tenofovir alafenamide/Emtricitabine/Cobicistat | 6 (13) | |
| Dolutegravir/Lamivudine | 3 (7) | |
| Darunavir/Tenofovir alafenamide/Emtricitabine/Cobicistat | 3 (7) | |
| Other | 11 (24) | |
| Antiretroviral therapy, no. (%): | ||
| Long-acting regimen | ||
| CAB-RPV q4w | 2 (4) | |
| CAB-RPV q8w | 44 (96) | |
| Followed oral lead-in period | 38 (83) | |
| Number of comedications, no. (%): | ||
| 0 | 15 (33) | [4, (9)] |
| 1 | 10 (22) | |
| 2 | 3 (7) | |
| 3 | 5 (10) | |
| 4 | 1 (2) | |
| ≥5 | 8 (17) |
| Adverse Events Categories | Number Reported in the TDM Request Forms (%) (n = 91) | Number of PLWH (%) (n = 46) |
|---|---|---|
| No adverse events, no. (%) | 67 (74%) | 32 (70%) |
| Any adverse event, no. (%) | 20 (22%) | 14 (30%) |
| Injection site reaction a | 11 (12%) | 8 (17%) |
| Pyrexia b | 1 (1%) | 1 (2%) |
| Fatigue c | 5 (5%) | 4 (9%) |
| Headache | 3 (3%) | 2 (4%) |
| Musculoskeletal pain d | 5 (5%) | 4 (9%) |
| Gastrointestinal disorders e | 2 (2%) | 2 (4%) |
| Sleep disorders f | 2 (2%) | 2 (4%) |
| Missing data | 4 (4%) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thoueille, P.; Alves Saldanha, S.; Schaller, F.; Munting, A.; Cavassini, M.; Braun, D.; Günthard, H.F.; Kusejko, K.; Surial, B.; Furrer, H.; et al. Real-Life Therapeutic Concentration Monitoring of Long-Acting Cabotegravir and Rilpivirine: Preliminary Results of an Ongoing Prospective Observational Study in Switzerland. Pharmaceutics 2022, 14, 1588. https://doi.org/10.3390/pharmaceutics14081588
Thoueille P, Alves Saldanha S, Schaller F, Munting A, Cavassini M, Braun D, Günthard HF, Kusejko K, Surial B, Furrer H, et al. Real-Life Therapeutic Concentration Monitoring of Long-Acting Cabotegravir and Rilpivirine: Preliminary Results of an Ongoing Prospective Observational Study in Switzerland. Pharmaceutics. 2022; 14(8):1588. https://doi.org/10.3390/pharmaceutics14081588
Chicago/Turabian StyleThoueille, Paul, Susana Alves Saldanha, Fabian Schaller, Aline Munting, Matthias Cavassini, Dominique Braun, Huldrych F. Günthard, Katharina Kusejko, Bernard Surial, Hansjakob Furrer, and et al. 2022. "Real-Life Therapeutic Concentration Monitoring of Long-Acting Cabotegravir and Rilpivirine: Preliminary Results of an Ongoing Prospective Observational Study in Switzerland" Pharmaceutics 14, no. 8: 1588. https://doi.org/10.3390/pharmaceutics14081588
APA StyleThoueille, P., Alves Saldanha, S., Schaller, F., Munting, A., Cavassini, M., Braun, D., Günthard, H. F., Kusejko, K., Surial, B., Furrer, H., Rauch, A., Ustero, P., Calmy, A., Stoeckle, M., Battegay, M., Marzolini, C., Andre, P., Guidi, M., Buclin, T., ... on behalf of the Swiss HIV Cohort Study. (2022). Real-Life Therapeutic Concentration Monitoring of Long-Acting Cabotegravir and Rilpivirine: Preliminary Results of an Ongoing Prospective Observational Study in Switzerland. Pharmaceutics, 14(8), 1588. https://doi.org/10.3390/pharmaceutics14081588