
An Adequate Pharmaceutical Quality System for Personalized Preparation

Abstract
:1. Introduction
- Dosage adjustments;
- Adaptation of pharmaceutical forms and routes of administration;
- Adaptation of pharmacy compounding to intolerances and pathologies;
- No treatment: rare diseases, veterinary medicines, shortages, etc.;
- Instability of certain medicines;
- Improved adherence to treatment;
2. Personalized Preparation Quality: Definitions and Legislation
- Allow preparations to be available for stock, so as to respond to the immediate needs of some patients. This already happens in some European countries, per the definition of “stocks preparation” provided by the European pharmacopeia: pharmaceutical preparations prepared in advance and stored until a supply request is received [10].
- Increase the typified formulas, and do not require these to be included in a formulary, since this system is not dynamic; rather it is based on a scientific justification that demonstrates its effectiveness and safety.
- Extend the regulations to the development of all routes of administration and pharmaceutical forms, e.g., that sterile forms be included. This will make it possible to cover all prescriptions and needs, guaranteeing the required quality.
- Address the need to consider the differences between industrially manufactured and personalized medicine.
- Consider the concept of designed quality (a concept discussed in detail in this article).
- Consider the demands of the next generation of personalized medicines, such as 3D Printing and CAR-T cell therapy.
3. A Review of the Evolution of Quality Management Systems for Medicines
3.1. Quality Control
3.2. Elaborated Quality
3.3. Designed Quality
- consideration of the product in particular;
- options for improvement;
- validation through variables;
- risk systems;
- improved understanding of the processes.
4. ICH Objectives for a Pharmaceutical Quality System
- Making the product using a system that enables the provision of a product of suitable quality for the patient, healthcare professionals, and authorities.
- Effectively controlling and monitoring processes and product quality and ensuring ongoing suitability. Quality risk management is useful to identify them.
- Continuous improvement in the quality of the product, processes, and pharmaceutical quality system. Reduce variability. To meet this objective, quality risk management is useful to identify and prioritise areas.
4.1. Application of the Objectives to Industrially Manufactured Medicine
4.2. Application of the Objectives to Personalized Preparations
- The main guarantees for fulfilling objective one in the case of a personalized preparation are scientific knowledge and good practices of the prescribing professional and the pharmacist who makes and dispenses the preparation. These professionals take full responsibility for the quality of the preparation process and the use of the medicine [35].
- The quality management system applied in the compounding laboratories from the acquisition of the initial materials to the controls and the dispensing of the product ensures that products with the right quality are made, as described in the legislation. In Spain, RD 175/2001 brought about a change in this regard, since it regulates the rules of proper preparation and quality control of magistral formulas and official formulas. In fact, customer satisfaction with personalized preparations is high [36,37,38]. In addition, satisfaction is very high since this is a medication that is designed, prescribed, and developed for a specific patient to treat a particular pathology. These reasons also make it possible to reduce side effects [39]. Compliance with the first objective is thus ensured.
- Meanwhile, from a quality control perspective, an intrinsic limitation based on the very personalized nature of the preparation has already been described in previous sections: the impossibility of measuring certain attributes that define quality.
- The second objective is partly fulfilled in the case of personalized preparations since some controls can be instituted that offer information about the process and the quality of the product, though there are certain limitations. Process monitoring strategies can be established using protocols that are the result of compound production validations and detailed knowledge of manufacturing operations. There are restrictions at this point: unitary and heterogeneous production means that the possibility of monitoring by means of certain quality controls is reduced.
- Quality risk management will make it possible to identify what is important and what is not, meaning that resources can be usefully applied, thereby obtaining the best possible results. The products and their processes must be fully known and understood and must be analysed to identify any real hazards and risks. Once the risk is known, it should be assessed and accepted or rejected depending on its level and the ways in which the risk may be reduced or avoided [27].
- Detailed knowledge of the product and process management of a personalized preparation is sometimes limited by the resources available for its development and restricted by the variability and time limitations noted elsewhere. Even so, as Minguetti states [3], the authorities agree that the risk associated with the development of personalized preparations is considered acceptable given their added value, even if they are not prepared under the same quality system as at the industrial level.
- In terms of complying with the third objective, when improvements are identified during the magistral formulas compounding process, they are implemented and incorporated into the work protocols. Restrictions are again observed in the detection of such improvements in relation to the previously mentioned peculiarities of personalized preparations. The limitation of not being able to perform certain controls that provide information about processes can be restrictive when identifying areas for improvement. A need for improvement may be found, though the exact processes affected might not be identified if they are not all monitored.
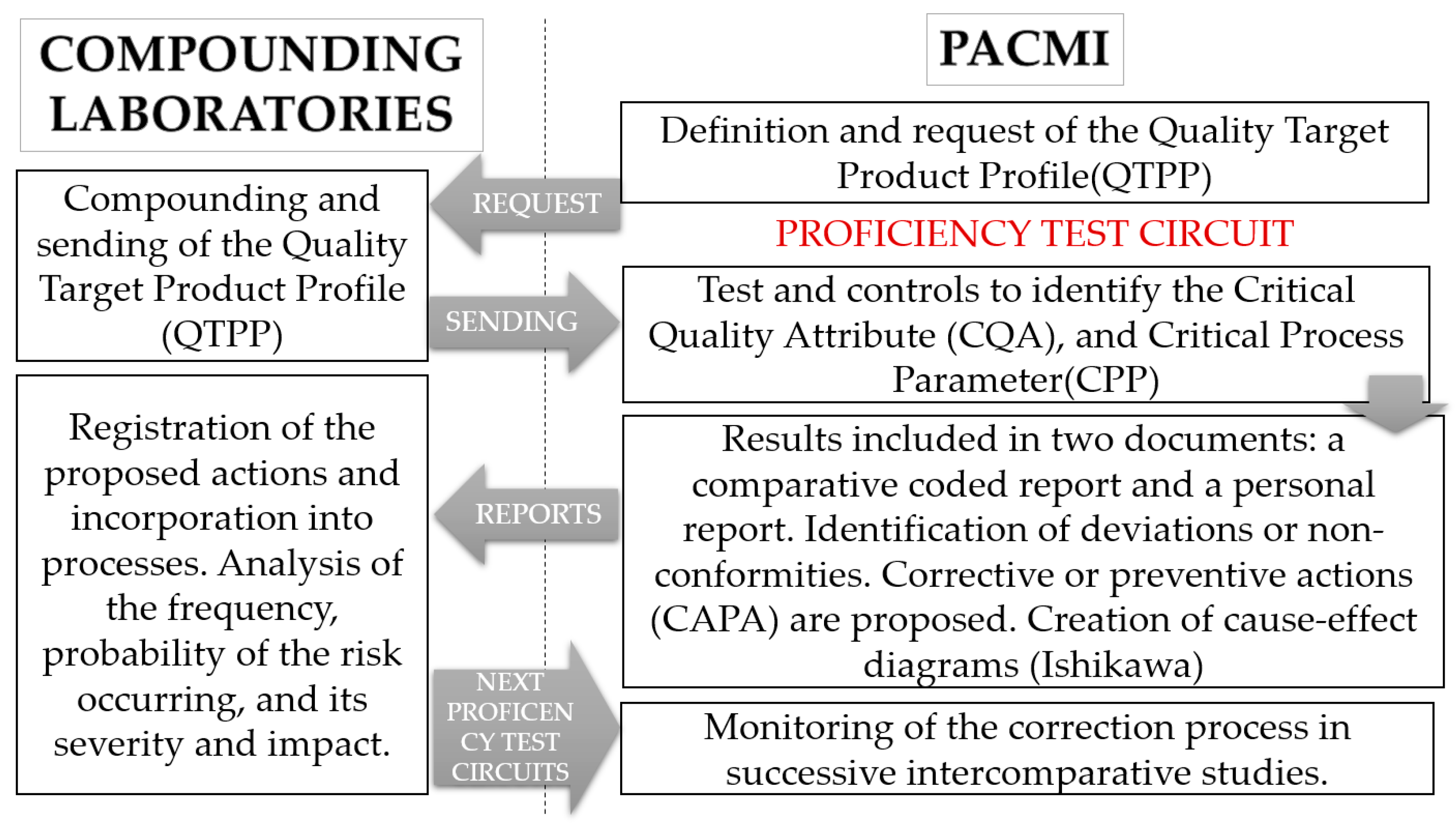
5. Proposal of a Strategy for Overall Improvement in the Personalized Preparation Quality System: Proficiency Testing
- Sampling is impossible as the preparations are single productions (no batches).
- Destructive controls cannot be performed for the same reason as above.
- There is limited availability of the necessary equipment for monitoring and quality control.
- The great variety of medicines produced leads to an increased number of processes and products to be analysed, understood, and mastered.
- Limited resources (financial and time) are available to design and develop the compounding.
- A lack of sampling and analytical control equipment leads to limitations in continuous monitoring; thus, improvement needs may be identified, though the processes or operations that are affected may remain unknown.
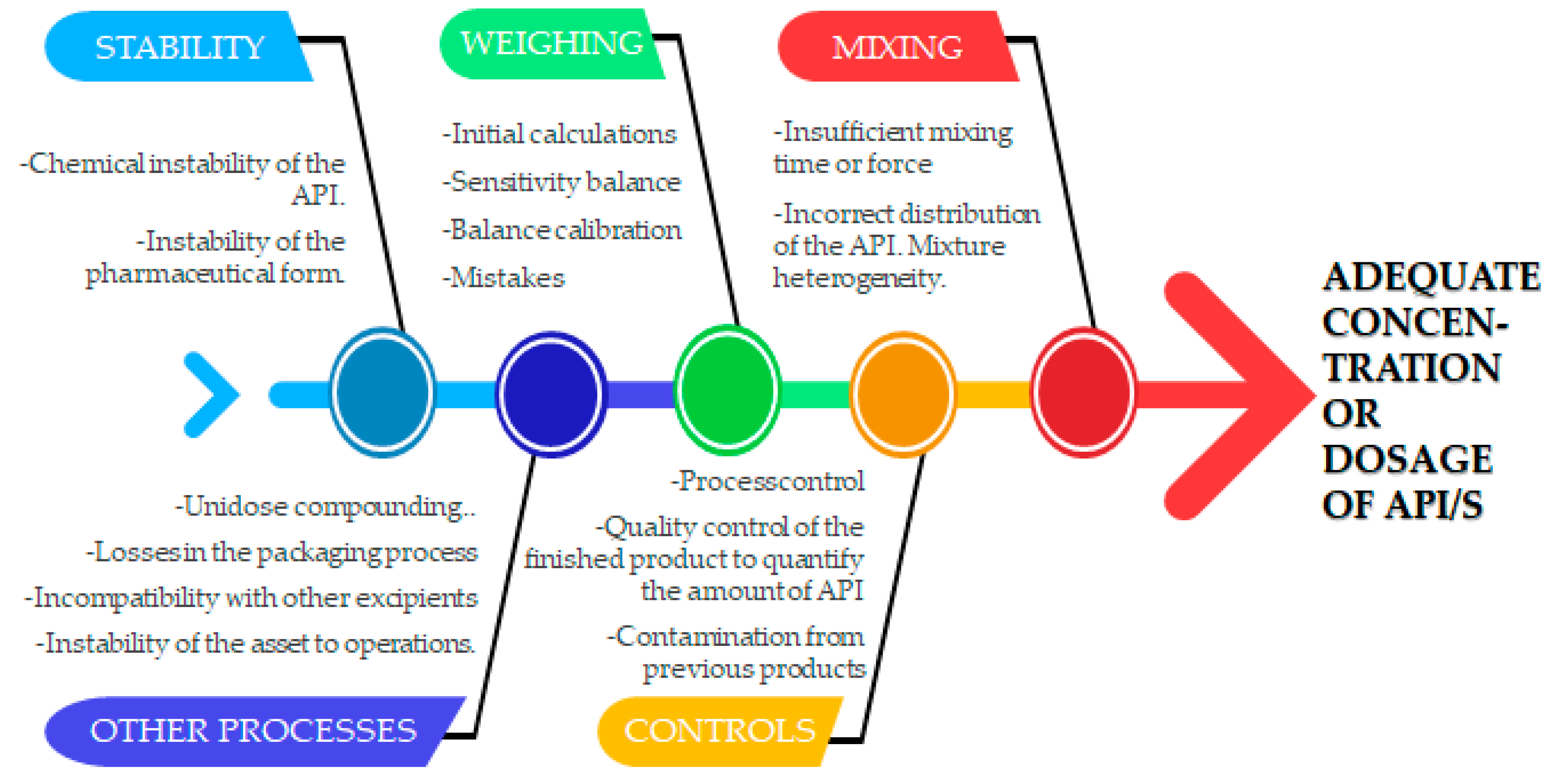
- The percentage of error committed rises when handling small quantities of raw material in the processes, e.g., in weighing, mixing, conditioning, etc. [40].
- The stability studies performed on personalized preparations remain suboptimal.
- Detection of contamination from previous products is a critical issue. Cleaning validation programs form a key component of a quality system.
- Increase the number of samples and thereby ensure sampling and the possibility of destruction.
- Have the infrastructure, equipment, and resources that allow increased knowledge of both products and processes.
- Hence, it is necessary to have a system that allows the maximum number of variables in these products and processes to be compared.
- −
- An individual report with details of the results specific to each participant. The deviations or non-conformities found are detailed and preventive or corrective measures are proposed. The aim is to input improvements into the processes at the compounding laboratory.
- −
- A general report which is duly encoded to safeguard the anonymity of all participants. This contains the comparative results of all the laboratories for all the tests done and a general overview of the incidents or deviations identified related to quality, anonymously identifying the affected samples. These are documented and their root cause is sought. Lastly, corrective or preventive measures are proposed.
- Gathering information to demonstrate to third parties the effective overall quality of personalized preparations.
- Undertaking stability studies and galenic developments.
6. Quality = Homogeneity/Heterogeneity
7. Conclusions
- Allowing destructive testing.
- Increasing the number of samples that facilitate comparative analysis and obtaining conclusions about the impact of some particular factors on the processes.
- Enabling the dedication of more resources: equipment and facilities such as pharmacy technical equipment, sterile environments for microbiological controls, analytical tools, etc.
- Expanding knowledge of the product and processes used in the production of a personalized preparation. In addition to analysing specific quality results, it is possible to broaden the study undertaken by each compounding pharmacist and offer improvement strategies and a risk analysis for the product.
- Pinpointing the deviations or non-conformities found, documenting and identifying their root cause (with the Ishikawa diagram), and proposing preventive or corrective measures (CAPA system). The aim is to input improvements into the processes at the compounding laboratories.
- Contributing to the overall improvement of product quality through increased analysis and knowledge to the benefit of patient health.
- Making galenic developments and stability studies.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Florence, A.T.; Siepmann, J. Dosage Forms for Personalized Medicine: From the Simple to the Complex. In Modern Pharmaceutics, 5th ed.; CRC Press: Boca Raton, FL, USA, 2016; Volume 2, pp. 511–530. [Google Scholar]
- Farmacéuticos. pp. 24–25. Available online: http://publicaciones.portalfarma.com/farmaceuticos/428/files/assets/common/downloads/publication.pdf (accessed on 18 December 2022).
- Minghetti, P.; Pantano, D.; Gennari, C.G.M.; Casiraghi, A. Regulatory framework of pharmaceutical compounding and actual developments of legislation in Europe. Health Policy 2014, 117, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Abrahams, E.; Ginsburg, G.S.; Silver, M. The personalized medicine coalition. Am. J. Pharm. 2005, 5, 345–355. [Google Scholar] [CrossRef] [PubMed]
- ICH. Available online: https://database.ich.org/sites/default/files/Q9_Guideline.pdf (accessed on 5 December 2022).
- ICH. Available online: https://database.ich.org/sites/default/files/Q6A%20Guideline.pdf (accessed on 5 December 2022).
- Agencia Española del Medicamento y Producto Sanitario. Guía de Normas de Correcta Fabricación de la Unión Europea. Available online: https://www.aemps.gob.es/industria-farmaceutica/guia-de-normas-de-correcta-fabricacion/ (accessed on 9 December 2022).
- Eur-lex. European Union Law. Available online: https://eur-lex.europa.eu/eli/dir/1989/341/oj (accessed on 9 December 2022).
- World Health Organization. Available online: https://apps.who.int/iris/handle/10665/43532 (accessed on 9 December 2022).
- Pharmaceutical Preparations European Pharmacopoeia, 7th ed.; Worldwide Book Service: Wickford, UK, 2013; Supplement S7.7.
- United States Pharmacopeia USP 34-NF 29, General Chapter <795>, Pharmaceutical Compounding—Nonsterile Preparations. Available online: https://www.usp.org/compounding/general-chapter-795 (accessed on 9 December 2022).
- United States Pharmacopeia (USP). General Chapter <797> Pharmaceutical Compounding–Sterile Preparations. Available online: https://www.usp.org/compounding/general-chapter-797 (accessed on 9 December 2022).
- Branch, S.K. Guidelines from the international conference on harmonisation (ICH). J. Pharm. Biomed. Anal. 2005, 38, 798–805. [Google Scholar] [CrossRef]
- RED EAMI. Available online: https://www.redeami.net/docs/docs/cooperacion/guias_formulario_iberoamericano/01_Guia_de_buenas_practicas_elaboracion_control_calidad_preparaciones_magistrales_oficinales.pdf (accessed on 10 December 2022).
- PIC/S Guide to Good Practices for the Preparation of Medicinal Products in Healthcare Establishments. Available online: https://www.gmp-compliance.org/files/guidemgr/pe-010-4-guide-to-good-practices-1.pdf (accessed on 7 December 2022).
- Committee of Ministers, Council of Europe. Available online: https://statements.eahp.eu/sites/default/files/resources/resource%20statement%203.3-compunding.pdf (accessed on 1 December 2022).
- Scheepers, H.P.A.; Handlos, V.N.; Walser, S.; Schutjens, M.D.B.; Neef, C. Impact of the Council of Europe Resolution on quality and safety assurance requirements for medicinal products prepared in pharmacies for the special needs of patients. Eur. J. Hosp. Pharm. 2017, 24, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Scheepers, H.P.A.; Busch, G.; Hofbauer, E.; Kalcher, C.; Landgraf, C.; Neelup Handlos, V.; Walser, S. Abridged survey report on quality and safety assurance standards for the preparation of medicinal products in Pharmacies. Pharmeuropa 2010, 22, 405–413. [Google Scholar]
- Scheepers, H.P.; Langedijk, J.; Handlos, V.N.; Walser, S.; Schutjens, M.H.; Neef, C. Legislation on the preparation of medicinal products in European pharmacies and the Council of Europe Resolution. Eur. J. Hosp. Pharm. 2016, 24, 224–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agencia Estatal Boletín Oficial del Estado. Available online: https://www.boe.es/eli/es/rdlg/2015/07/24/1 (accessed on 2 December 2022).
- Agencia Estatal Boletín Oficial del Estado. Available online: https://www.boe.es/eli/es/rd/2001/02/23/175 (accessed on 2 December 2022).
- Agencia Estatal Boletín Oficial del Estado. Available online: https://www.boe.es/eli/es/rd/2003/07/11/905 (accessed on 2 December 2022).
- Agencia Estatal Boletín Oficial del Estado. Formulario Nacional. Available online: https://www.boe.es/biblioteca_juridica/abrir_pdf.php?id=PUB-NT-2019-112 (accessed on 2 December 2022).
- Agencia Estatal Boletín Oficial del Estado. Available online: https://www.boe.es/eli/es/rd/2009/06/19/1015 (accessed on 2 December 2022).
- Agencia Estatal Boletín Oficial del Estado. Available online: https://www.boe.es/eli/es/rd/2010/06/25/824/con (accessed on 2 December 2022).
- Sociedad Española de Farmacia Hospitalaria. Available online: https://www.sefh.es/sefhpdfs/GuiaBPP_JUNIO_2014_VF.pdf (accessed on 2 December 2022).
- Botet, J. The pharmaceutical quality revolution. ScienceRise 2016, 1, 4–15. [Google Scholar] [CrossRef]
- Minghetti, P.; Palmieri, I.; Selmin, F. When authorized medicinal products are not available: Possible alternatives to meet legitimate expectations of patients. J. Pharm. Health Serv. Res. 2010, 1, 107–112. [Google Scholar] [CrossRef]
- ICH. Available online: https://database.ich.org/sites/default/files/Q1A%28R2%29%20Guideline.pdf (accessed on 5 December 2022).
- Trissel, L.A.; Ashworth, L.D.; Ashworth, J. Trissel’s Stability of Compounded Formulations, 6th ed.; American Pharmacists Association: Washington, DC, USA, 2018. [Google Scholar] [CrossRef]
- D’huart, E.; Vigneron, J.; Gindre, I.; Lider, P.; Demoré, B. First international database of research teams in stability and compatibility of medications: An additional function in the Stabilis® database. Ann. Pharm. Françaises 2018, 76, 436–443. [Google Scholar] [CrossRef]
- Buttini, F.; Rozou, S.; Rossi, A.; Zoumpliou, V.; Rekkas, D.M. The application of quality by design framework in the pharmaceutical development of dry powder inhalers. Eur. J. Pharm. Sci. 2018, 113, 64–76. [Google Scholar] [CrossRef]
- ICH. Available online: https://database.ich.org/sites/default/files/Q10%20Guideline.pdf (accessed on 5 December 2022).
- Aaberg, C.; Dahmen, H.; Davies, C.; Sandau, P.L.; Srinivasan, R. ISO 9001: 2015 Versus ICH Q10—A Comparison. PDA J. Pharm. Sci. Technol. 2021, 75, 188–206. [Google Scholar] [CrossRef]
- Ceppi, H.J. Guía Práctica Sobre Recetas Magistrales Para Odontología y Otras Consideraciones Concomitantes; BSG Basago Libros: Córdoba, Argentina, 2003. [Google Scholar]
- Avís, S.; Pérez Higuero, F.L.; Vicente, R.M. Evaluación de la efectividad de la Atención Farmacéutica en pacientes tratados con fórmulas magistrales en el periodo de septiembre 2017–febrero 2018 en Farmacia Magistral de Villanueva de la Serena (Badajoz). FarmaJournal 2018, 3, 43–52. [Google Scholar]
- McPherson, T.; Fontane, P. Patient-centered care in the community-based compounding practice setting. J. Am. Pharm. Assoc. 2010, 50, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Fastø, M.M.; Genina, N.; Kaae, S.; Sporrong, S.K. Perceptions, preferences and acceptability of patient designed 3D printed medicine by polypharmacy patients: A pilot study. Int. J. Clin. Pharm. 2019, 41, 1290–1298. [Google Scholar] [CrossRef]
- Giam, J.A.; McLachlan, A.J.; Krass, I. Community pharmacy compounding–impact on professional status. Int. J. Clin. Pharm. 2011, 33, 177–182. [Google Scholar] [CrossRef]
- KuKanich, B.; Warner, M.; Hahn, K. Analysis of lomustine drug content in FDA-approved and compounded lomustine capsules. J. Am. Vet. Med. 2017, 250, 322–326. [Google Scholar] [CrossRef]
- Watson, C.J.; Whitledge, J.D.; Siani, A.M.; Burns, M.M. Pharmaceutical Compounding: A History, Regulatory Overview, and Systematic Review of Compounding Error. J. Med. Toxicol. 2021, 17, 197–217. [Google Scholar] [CrossRef]
- Staes, C.; Jacobs, J.; Mayer, J.; Allen, J. Description of outbreaks of health-care-associated infections related to compounding pharmacies. Am. J. Health Syst. Pharm. 2013, 70, 1301–1312. [Google Scholar] [CrossRef] [Green Version]
- Puerto Cano, R. Evolución del Medicamento Individualizado en España, Situación Actual y Perspectivas de Future; Academia de Farmacia Santa María de España de la Región de Murcia: Cartagena, España, 2021; pp. 99–110. [Google Scholar]
- Kneip Fleury, M.; Menezes, M.E.; Abol Correa, J. Implementation of the external quality assessment program in Brazil. Biochem Med. 2017, 27, 93–96. [Google Scholar] [CrossRef] [Green Version]
- Costa, A.M.G.; Escott, R.; Garland, S.M.; Byers, D.; Tabrizi, S.N. Development of a pilot proficiency program for human papillomavirus DNA detection. Pathology 2018, 50, 659–664. [Google Scholar] [CrossRef]
- Stavelin, A.; Albe, X.; Meijer, P.; Sarkany, E.; MacKenzie, F. An overview of the European Organization for External Quality Assurance Providers in Laboratory Medicine (EQALM). Biochem Med. 2017, 27, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Corrons, J.L.V.; Albarède, S.; Flandrin, G.; Heller, S.; Horvath, K.; Houwen, B.; Libeer, J.C. Guidelines for blood smear preparation and staining procedure for setting up an external quality assessment scheme for blood smear interpretation. Part I: Control material. Clin. Chem. Lab. Med. 2004, 42, 922–926. [Google Scholar] [CrossRef] [PubMed]
- Bérard, P.; Franck, D. National and international interlaboratories comparisons: A tool for the validation of in vitro and in vivo methods. Radiat. Prot. Dosim. 2011, 144, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Todd, C.A.; Sanchez, A.M.; Garcia, A.; Denny, T.N.; Sarzotti-Kelsoe, M. Implementation of Good Clinical Laboratory Practice (GCLP) guidelines within the external quality assurance program oversight laboratory (EQAPOL). J. Immunol. Methods 2014, 409, 91–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lempers, V.J.C.; Alffenaar, J.W.C.; Touw, D.J.; Burger, D.M.; Uges, D.R.A.; Aarnoutse, R.E.; Brüggemann, R.J.M. Five year results of an international proficiency testing programme for measurement of antifungal drug concentrations. J. Antimicrob. Chemother 2014, 69, 2988–2994. [Google Scholar] [CrossRef] [Green Version]
- Christians, U.; Vinks, A.A.; Langman, L.J.; Clarke, W.; Wallemacq, P.; Van Gelder, T.; Meyer, E.J. Impact of laboratory practices on interlaboratory variability in therapeutic drug monitoring of immunosuppressive drugs. Ther. Drug Monit. 2015, 37, 718–724. [Google Scholar] [CrossRef]
- Burger, D.; Teulen, M.; Eerland, J.; Harteveld, A.; Aarnoutse, R.; Touw, D. The international interlaboratory quality control program for measurement of antiretroviral drugs in plasma: A global proficiency testing program. Ther. Drug Monit. 2011, 33, 239–243. [Google Scholar] [CrossRef]
- ICH. Available online: https://database.ich.org/sites/default/files/Q8%28R2%29%20Guideline.pdf (accessed on 5 December 2022).



{kind=link}
{kind=link}
| Law/Norm | What It Regulates | Observations |
|---|---|---|
| Royal Legislative Decree 1/2015, of 24 July [20]: | Passes the text of the Law on guarantees and rational use of medicines and health products. | It includes a section that states that magistral formulas and official formulas are legally recognized medicines, prepared by or under the direction of a pharmacist, and dispensed from a pharmacy or pharmaceutical service, complete with sufficient information to guarantee they are correctly identified (including the name of the pharmacist who has prepared them), conserved and safely used. |
| Royal Decree (RD) 175/2001, of 23 February [21]: | Passes the norms for proper preparation and quality control of magistral formulas and official formulas. | This is a turning point in legislation on personalized preparations. It introduces regulations for proper production and quality assurance applied to compounding laboratories. They are considered the minimum that every compounding laboratory must meet to ensure the quality of the medicines it manufactures. There are certain “gaps” in them which are detailed in this article. |
| Royal Decree 905/2003, of 11 July [22]: | Modifies the sole transitional provision of Royal Decree 175/2001. | It was published to extend the deadline for the adaptation of laboratories to the requirements of RD175/2001. |
| Order SCO/3262/2003; updates: SCO/3123/2006 and SSI/23/2015 [23] | The National Formulary (and its subsequent updates) and the Royal Spanish Pharmacopoeia are passed. | Currently, 3rd edition of the formulary. It contains 81 monographs on raw material, 57 on official formulas, and 29 typified magistral formulas: standardized compounding approved by the Formulary and Pharmacopoeia Commission (collected in the National Formulary). |
| Royal Decree 1015/2009, of 19 June [24]: | Regulates the availability of medicines in special situations and what can be produced. | There are circumstances in which the clinical data that support a certain therapeutic use for an already authorized drug are not included as an officially approved indication. Very relevant in areas with intense research activity and the pace of evolving scientific knowledge that precedes the procedures to incorporate them as an official indication. There are also conditions of use in clinical practice that are not contemplated in authorization for the medicine, given an absence of commercial interest for undertaking studies pursuant to its authorization. These exceptional uses lie within the wardship of clinical practice and are the responsibility of the prescriber. Authorization is not required on a case-by-case basis. |
| Royal Decree 824/2010, of 25 June [25]: | Pharmaceutical laboratories, manufacturers of active ingredients for pharmaceutical use, and foreign trade in medicinal products and investigational medicinal products | Point 3 of Article 1: non-mandatory authorization as manufacturers of medicines for compounding services that produce magistral and official formulas. |
| Guide to good medicinal product preparation practices in hospital pharmacy services [26]: | Points not observed in RD 175/2001, which are very necessary for hospital pharmacy services: handling, fractionation, and personalized dosage. It covers the preparation of sterile products. | It arose as a result of Royal Decree-Law 16/2012 on urgent measures to ensure the sustainability of the National Health System and improve the quality and safety of its services, which determines the possibility for the Autonomous Regions to certify hospitals for the tasks of handling, fractionation, and personalized dosage, and to guarantee application of the technical guidelines on good practices in hospital pharmacy services in the absence of said text. As it is not legislative in character, merely a recommendation, it is not mandatory to comply with, rather it must be observed. Application and direct reference to the hospital environment, with the same absences in the same spheres, on the matter of compounding in the regional pharmacy. |
| Industrially Manufactured Medicines | Personalized Preparations | |
|---|---|---|
| Batch size | Large batches | Mostly as a unit product (a medicine/prescription). Small batches, only in official formulas. |
| Variability in product/laboratory | A limited number of different medicines/items in each laboratory. Patients adapt to the medicine. The homogeneity of all medicines with the same item number is guaranteed. | Great diversity in medicines; heterogeneity. As many prescriptions as there are patients: subject to changes in pharmaceutical forms and active ingredients; combinations and modification of dosage, excipients, packaging, etc. Great versatility and extensive knowledge are required to be able to pursue development and compounding in a limited timeframe. The medicine is tailored to the patient [16]. |
| Investment of resources in each medicine developed | Each development entails validations and controls, and significant investment of time, money, and personnel. The mean time invested to receive authorization to market a medicine is about 10-12 years with a financial outlay of approximately 800 million Euros [28]. After scaling, production yield is high. | Limited resources and minimal time (from prescription to dispensing: hours or days) are available to design and develop a wide range of medicines. Without these time and resource limitations, it would be unfeasible to be able to respond to the personalized creation of such products at a price that was not exorbitant. As stated in the European resolution on quality assurance and safety requirements for medicines prepared in pharmacies (personalized preparations), the risks of a delay in the supply of a medicine to treat the patient must be assessed, albeit without ignoring the possible risk that could result from an error in preparation. The production is at times singular, making sampling impossible and quality control destructive. |
| Supplies/quantities of raw materials and medicines | The portions of initial, intermediate, and final products are large and it is produced in batches. The yield achieved with high-quantity production makes it possible to invest effort in continuous improvement and process knowledge. | Very small quantities are handled, both in terms of starting materials, in the quantities weighed, and in the number of preparations that are repeated after each design. Handling small quantities involves difficulties. For example, weighing is common to all manufacturing processes, but weighing small quantities generates greater error. (There is a link between the weighed quantity, the sensitivity of the scales, and the error made in this basic operation). |
| Profitability | The initial investment of time and resources to develop a new medicine is high, but once it moves to an industrial scale, the investment is profitable through the high yields achieved with industrial equipment and processes. | For each prescription: development includes a search for information, design, development, specific documentation, purchase of materials from suitable suppliers, validation by creating a production protocol, and lastly, preparation of the final compounding. This is often done for a once-off prescription. As for raw materials acquisition in cases of single preparations, it should be discarded without being used because suppliers do not have small enough sizes. |
| Controls | Production in large batches allows ongoing control. Sampling is not limited, even if the controls performed are “destructive”. Checks can be performed throughout the life cycle of the product. | The total amount produced does not allow for sampling or for destructive quality controls to be performed. |
| Validation and continuous improvement | Time and effort are invested in validation and continuous improvement processes. The opportunity exists to know the details of each process, including personnel and specialized equipment. | A lack of resources is detected that enables increased knowledge regarding some products made at the magistral level |
| Stability | All industrially manufactured medicines have full stability studies. The objective is to know the validity period of use for the medicine. They allow an experimental expiration date to be given, which is obtained by means of testing forced degradation, and stability studies at certain times contiguously when marketing the approved batches. Optimum conservation conditions (conditioning, temperature, and humidity) are assessed [29]. | Not enough information is available on stability since any alteration made to the prescription (change of dose, excipient, or packaging material) will modify the expiration date of the medicine. These changes are at the heart of personalization. Magistral production does not require preparations with such long-life cycles as they are not manufactured, transported, and stored because they are dispensed shortly (hours or days) after they are produced. Personalized preparations are not “in stock”; this only occurs with official formulas. That is why the term extemporaneous preparations is also used to refer to personalized preparations. The Pharmaceutical Inspection Convention (PIC) guide [15] defines an extemporaneous preparation as a product that is dispensed immediately after preparation and not kept in stock. Legislation limits the expiration date of magistral formulas (those that are not typified) to the duration of the prescribed treatment [21]. There is a lack of information when assigning expiration dates to personalized preparations and estimates or decision algorithms must sometimes be used. There are resources that help with this task, such as the manual “Trissel’s stability of compounded formulations” [30] and the “Stabilis” hospital pharmacy website: http://www.stabilis.org/ (accessed on 5 December 2022) [31]. There are pharmacopeias and manuals that compile decision algorithms for the assignment of expiration dates when there is no bibliography, such as United States Pharmacopeia (USP) or the guide for good practices for the preparation of medicines in hospital pharmacy services [26]. |
| Legislation (Spain is used as in the previous section) | Sections that contain Spanish national legislation on the correct preparation and control of medicines at an industrial level, detailed in Royal Decree 824/2010 [25]: Section 1: Pharmaceutical quality system Section 2: Personnel Section 3: Premises and equipment Section 4: Documentation Section 5: Production Section 6: Quality control Section 7: Subcontracted activities Section 8: Complaints, quality defects, and product recalls Section 9: Internal inspections | Sections that contain Spanish national legislation on the correct preparation and control of personalized preparations, detailed in Royal Decree 175/2001 [25]: Section 1: Personnel Section 2: Premises and tools Section 3: Documentation Section 4: Raw materials and packaging material Section 5: Production Section 6: Dispensing Table 1 offers an overview of all the legislation regulating the compounding of personalized preparations in Spain |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uriel, M.; Marro, D.; Gómez Rincón, C. An Adequate Pharmaceutical Quality System for Personalized Preparation. Pharmaceutics 2023, 15, 800. https://doi.org/10.3390/pharmaceutics15030800
Uriel M, Marro D, Gómez Rincón C. An Adequate Pharmaceutical Quality System for Personalized Preparation. Pharmaceutics. 2023; 15(3):800. https://doi.org/10.3390/pharmaceutics15030800
Chicago/Turabian StyleUriel, Marta, Diego Marro, and Carlota Gómez Rincón. 2023. "An Adequate Pharmaceutical Quality System for Personalized Preparation" Pharmaceutics 15, no. 3: 800. https://doi.org/10.3390/pharmaceutics15030800
APA StyleUriel, M., Marro, D., & Gómez Rincón, C. (2023). An Adequate Pharmaceutical Quality System for Personalized Preparation. Pharmaceutics, 15(3), 800. https://doi.org/10.3390/pharmaceutics15030800