

Application of Advanced Technologies—Nanotechnology, Genomics Technology, and 3D Printing Technology—In Precision Anesthesia: A Comprehensive Narrative Review

 , and
, and
Abstract
:1. Introduction
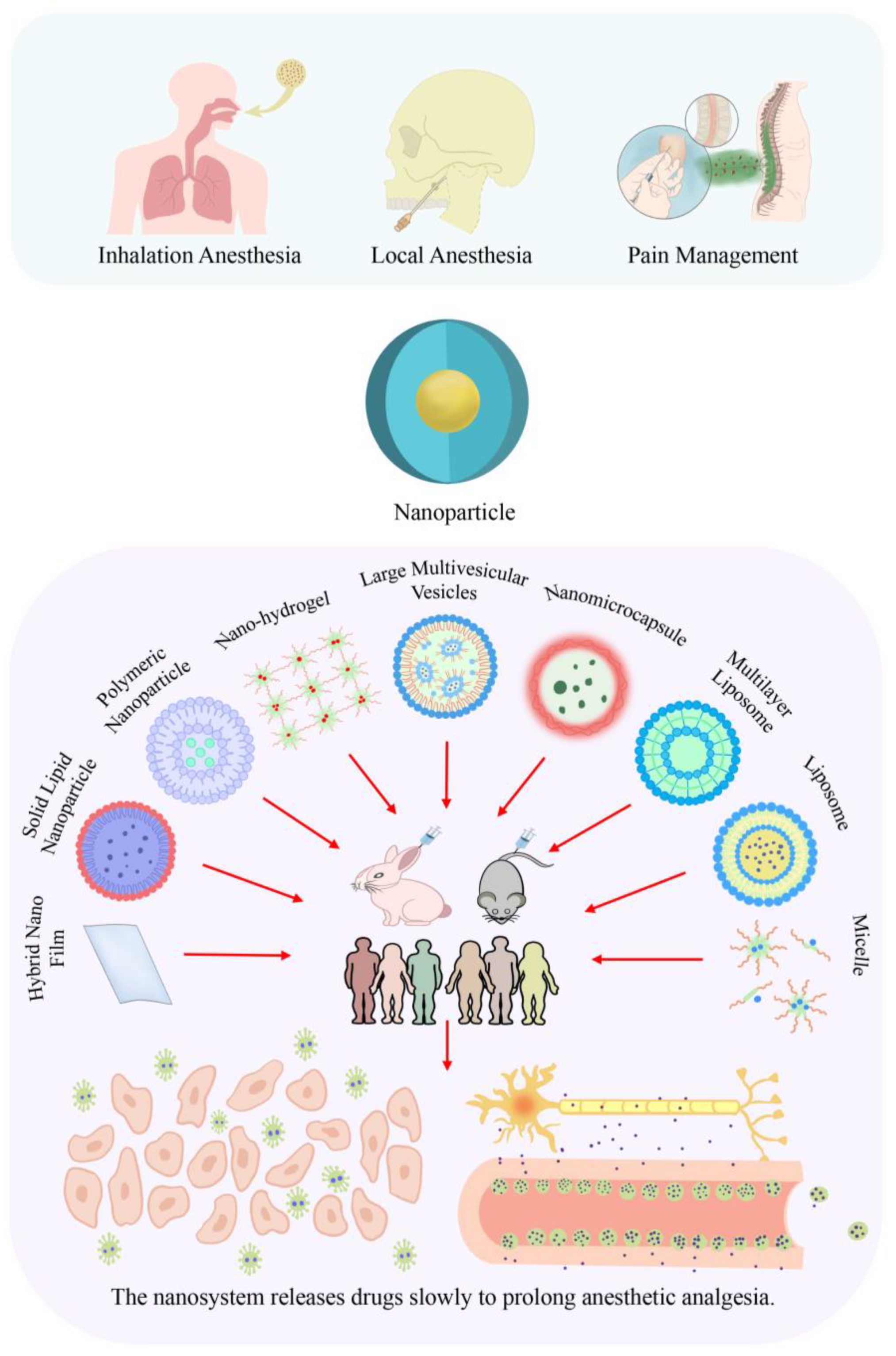
2. Application of Nanotechnology in the Anesthesia Field
2.1. Anesthesia and Nanotechnology
2.1.1. Nanotechnology in Inhalation Anesthesia
2.1.2. Nanotechnology in Local Anesthesia

{kind=link}
{kind=link}
| Local Anesthetic Drugs | Nanoparticle Type | Application Path | Test Method | Results | Duration of Efficacy |
|---|---|---|---|---|---|
| Bupivacaine | 15 nm micellar bupivacaine formulation (M-Bup) and 100 nm liposomal bupivacaine formulation | Local anesthesia | Tail injection in rats [25] | It showed an extended residence time in the local vasculature, with M-Bup showing the most prominent effect; there was also a reduction in systemic drug distribution [25]. | M-Bup provides 4.5 h of local anesthesia [25]. |
| Muhilamellar liposomes | Local anesthesia | Brachial plexus anesthesia in rabbits [28], intravenous drip in rabbits’ ears [29] | There was a prolonged effect of local anesthetics [28], with a significantly reduced drug toxicity to the central nervous system and heart [29]. | In the BP-MLV group, the plasma concentration of bupivacaine was lower within the first 10 min (p < 0.05) and higher after 24 h (p < 0.05). The radiolabeling in the BP group decreased between 4 and 24 h, while in the BP-MLV group, it decreased between 1 and 2 days [28]. | |
| Polymerized alginate nanoparticles [27, 30], large multicapsular liposomes (Bupisome) encapsulated in Ca-alginate cross-linked hydrogels (Bupigel) | Local anesthesia | In vitro and in vivo testing in mice, physicochemical property determination [27], and subcutaneous injection in mice [30] | It has good stability, low cytotoxicity, and a strong intensity of action [27]. There was a prolonged duration of the analgesic effect [27,30], with Bupigel outperforming Bupisome. | BVC (bupivacaine) is completely released in the solution after 350 min (100%), while the complete release of BVC present in the nanoparticle takes a longer time [27]. | |
| Large multivesicular vesicles | Local anesthesia | Healthy volunteers received subcutaneous injections [53] | Delayed elimination and prolonged redistribution of plasma results in prolonged pharmacodynamic effects [53]. | The time to reach the maximum plasma concentration of the liposomal formulation increased by 7-fold (262 +/− 149 min vs. 37.5 +/− 16 min, p < 0.01) [53]. | |
| Liposomal bupivacaine (LEB) | Local anesthesia | Intra-articular soft tissue injection in dogs [54] | Dogs administered with LEB are less likely to require rescue analgesia and receive lower doses of opioid medications compared to dogs administered with 0.5 BH [54]. | In the LEB group, three dogs requiring rescue analgesia were identified at 8 h (n = 2) and 16 h (n = 1) post-extubation, based on a CSU-CAPS pain score ≥ 2. In the 0.5 BH group, among the 10 dogs requiring rescue analgesia, 7 dogs first exhibited these symptoms within 6 (n = 4) to 8 (n = 3) hours post-extubation [54]. | |
| Liposomal suspension of bupivacaine | Local anesthesia | Sciatic nerve blockade in dogs [55] | The blockade characteristics of bupivacaine liposomal suspension are effective and long-lasting [55]. | In the treatment of 10 cases with bupivacaine with dexmedetomidine (BUP-DEX), all functions completely disappeared at 6 h. In all cases, all functions recovered within 96 h and 24 h after administration of bupivacaine liposome suspension (BLS) and BUP-DEX, respectively [55]. | |
| Microcapsules | Local anesthesia | Assessment of catheter microdialysis in healthy volunteers [56] | The extended-release properties of microcapsules allow a prolonged duration of anesthesia [56]. | After injection of microcapsules, the concentration of bupivacaine increased within 24–34 h. After 96 h, 78% of the injection sites with microcapsules still had analgesic effects, significantly longer than the bupivacaine solution (p < 0.001) [56]. | |
| Prilocaine | Liposomes | Local anesthesia for oral cavity | Maxillary infiltration anesthesia in healthy volunteers [31] | Prilocaine does not seem to benefit from liposome encapsulation [31]. | The median (and interquartile range) onset time for all formulations of gingival anesthesia was 2 (0) minutes, with no significant difference between them (p > 0.05) [31]. |
| Liposomes complexed with hydroxypropyl-β-cyclodextrin | Local anesthesia | In vivo assessment of anesthetic effects in guinea pigs [32] | The duration of the anesthetic effect was negatively correlated with the initial lag time of PRL hydrochloride in the core of aqueous vesicles [32]. | Dual-loaded liposomes containing 2% of the total drug dose exhibited optimal therapeutic activity and were significantly superior to the corresponding 2% single-loaded vesicles. They not only showed the shortest onset time (100% blockade of reflexes at 5 min) but also the longest duration of anesthesia effect (100% blockade of reflexes at 35 min) [32]. | |
| Lidocaine | Liposomes | Surface local anesthesia | Skin test on the palmar side of the forearm of volunteers [26] | Lidocaine liposome anesthesia has a longer duration than regular preparation [26]. | The average pain score of 5% liposomal lidocaine was higher than the non-liposomal 5% lidocaine formulation, but the difference reached statistical significance only at 15 min [26]. |
| Lidocaine-Prilocaine | Hybrid Nano Film | Local anesthesia | Permeability test of porcine buccal mucosa, tail-flick test in mice [24] | It is more permeable and has a longer anesthetic effect; it is not cytotoxic to 3T3 and HACAT cell lines [24]. | The obtained material showed a sustained release profile of LDC-PLC for over 8 h, and the permeability of pig buccal mucosa was nearly double that of the control group. Then, the in vivo efficacy of the PCT/NLC formulation was compared to biopolymer films and commercial drugs, demonstrating the longest anesthetic effect (>7 h) in mice through a tail flick test [24]. |
| Mepivacaine | Liposomes | Oral local anesthesia | Oral injection [33], oral maxillary infiltration [34] in healthy volunteers | It extends the duration of anesthesia, reduces injection discomfort [33], and allows systemic absorption similar to that of vasoconstrictor local anesthesia [34]. | Healthy volunteers experienced median ranges of induction latency (LP) (2–8 min), pulpal anesthesia (PA) (20–45 min), and soft tissue anesthesia (STA) (120–180 min) after infiltration anesthesia with the following formulations of lidocaine: MVC 2%EPI, MVC 2%LUV, MVC 3%LUV, and MVC 3% [33]. |
| Ropivacaine | Liposomes | Oral local anesthesia | Maxillary infiltration in healthy volunteers [35] | Liposome formulations lack vasoconstrictors and may be a safer alternative [35]. | They observed a maximum drug concentration (Tmax) of 50 (±14.1) minutes [35]. |
| Tetracaine (TTC) | Polymeric nanoparticles (PLA NPs), solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs) | Local anesthesia | In vitro and in vivo tests in mice [57] | Each system has its advantages, with TTC NLCs being the more promising system for long-term anesthesia [57]. | Free TTC demonstrated complete permeation within 8 h, while TTC NLC showed lower permeation rates than TTC PLA NPs in the first 12 h but higher permeation rates than PLA NPs after 12 to 72 h. TTC SLNs provided the most effective in vitro permeation, with sustained efficiency lasting until the end of 72 h [57]. |
2.1.3. Nanotechnology in Perioperative Pain Management
3. Genomics and Anesthesia
3.1. Pharmacogenomics
3.1.1. CYP1
3.1.2. CYP2
CYP2C9
CYP2C19
CYP2D6
- Opioids
- Antiemetic
- Beta-blockers
3.1.3. CYP3
3.2. Disease Genomics
3.3. Decision Modeling
4. Research and Application of 3D Printing in the Anesthesia Field
4.1. Three-Dimensional Printing Technology
4.2. Three-Dimensional Printing and Anesthesia
4.2.1. Three-Dimensional Printing and Anatomical Models
4.2.2. Three-Dimensional Printing and Anesthesia Equipment
5. Future, Limitations, and Outlook of Precision Anesthesia
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koos, J.A.; Bassett, A. Genetics Home Reference: A Review. Med. Ref. Serv. Q. 2018, 37, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Ciardiello, F.; Ciardiello, D.; Martini, G.; Napolitano, S.; Tabernero, J.; Cervantes, A. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA Cancer J. Clin. 2022, 72, 372–401. [Google Scholar] [CrossRef] [PubMed]
- Hampel, H.; Gao, P.; Cummings, J.; Toschi, N.; Thompson, P.M.; Hu, Y.; Cho, M.; Vergallo, A. The foundation and architecture of precision medicine in neurology and psychiatry. Trends Neurosci. 2023, 46, 176–198. [Google Scholar] [CrossRef] [PubMed]
- Criscione, J.; Rezaei, Z.; Cantu, C.M.H.; Murphy, S.; Shin, S.R.; Kim, D.H. Heart-on-a-chip platforms and biosensor integration for disease modeling and phenotypic drug screening. Biosens. Bioelectron. 2023, 220, 114840. [Google Scholar] [CrossRef]
- Bellini, V.; Valente, M.; Gaddi, A.V.; Pelosi, P.; Bignami, E. Artificial intelligence and telemedicine in anesthesia: Potential and problems. Minerva Anestesiol. 2022, 88, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Booth, B.J.; Nourreddine, S.; Katrekar, D.; Savva, Y.; Bose, D.; Long, T.J.; Huss, D.J.; Mali, P. RNA editing: Expanding the potential of RNA therapeutics. Mol. Ther. 2023, 31, 1533–1549. [Google Scholar] [CrossRef]
- Coughlin, S.S. Toward a road map for global -omics: A primer on -omic technologies. Am. J. Epidemiol. 2014, 180, 1188–1195. [Google Scholar] [CrossRef]
- Collins, F.S.; Varmus, H. A new initiative on precision medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef]
- Botney, R. Improving patient safety in anesthesia: A success story? Int. J. Radiat. Oncol. Biol. Phys. 2008, 71 (Suppl. 1), S182–S186. [Google Scholar] [CrossRef]
- Lanier, W.L. A three-decade perspective on anesthesia safety. Am. Surg. 2006, 72, 985–989; discussion 1021–1030, 1133–1148. [Google Scholar] [CrossRef]
- Ezhevskaya, A.A.; Ovechkin, A.M.; Prusakova, Z.B.; Zagrekov, V.I.; Mlyavykh, S.G.; Anderson, D.G. Relationship among Anesthesia Technique, Surgical Stress, and Cognitive Dysfunction Following Spinal Surgery: A Randomized Trial. J. Neurosurg. Spine 2019, 31, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Ruetzler, K.; Rivas, E.; Cohen, B.; Mosteller, L.; Martin, A.; Keebler, A.; Maheshwari, K.; Steckner, K.; Wang, M.; Praveen, C.; et al. McGrath Video Laryngoscope Versus Macintosh Direct Laryngoscopy for Intubation of Morbidly Obese Patients: A Randomized Trial. Anesth. Analg. 2020, 131, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.; Nicholls, B. Ultrasound in regional anaesthesia. Anaesthesia 2010, 65, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Kantoff, P.W.; Wooster, R.; Farokhzad, O.C. Cancer nanomedicine: Progress, challenges and opportunities. Nat. Rev. Cancer 2017, 17, 20–37. [Google Scholar] [CrossRef]
- Fan, S.; Chan, A.; Au, S.; Leong, M.C.; Chow, M.; Fan, Y.T.; Wong, R.; Chan, S.; Ng, S.K.; Lee, A.P.; et al. Personalised anaesthesia: Three-dimensional printing of facial prosthetic for facial deformity with difficult airway. Br. J. Anaesth. 2018, 121, 675–678. [Google Scholar] [CrossRef]
- Bayda, S.; Adeel, M.; Tuccinardi, T.; Cordani, M.; Rizzolio, F. The History of Nanoscience and Nanotechnology: From Chemical-Physical Applications to Nanomedicine. Molecules 2019, 25, 112. [Google Scholar] [CrossRef]
- Hulla, J.E.; Sahu, S.C.; Hayes, A.W. Nanotechnology: History and future. Hum. Exp. Toxicol. 2015, 34, 1318–1321. [Google Scholar] [CrossRef]
- Desai, C.; Koupenova, M.; Machlus, K.R.; Sen Gupta, A. Beyond the thrombus: Platelet-inspired nanomedicine approaches in inflammation, immune response, and cancer. J. Thromb. Haemost. 2022, 20, 1523–1534. [Google Scholar] [CrossRef]
- Vahabi, S.; Eatemadi, A. Nanoliposome encapsulated anesthetics for local anesthesia application. Biomed. Pharmacother. 2017, 86, 1–7. [Google Scholar] [CrossRef]
- Van der Meel, R.; Sulheim, E.; Shi, Y.; Kiessling, F.; Mulder, W.J.M.; Lammers, T. Smart cancer nanomedicine. Nat. Nanotechnol. 2019, 14, 1007–1017. [Google Scholar] [CrossRef]
- Panyam, J.; Labhasetwar, V. Biodegradable nanoparticles for drug and gene delivery to cells and tissue. Adv. Drug Deliv. Rev. 2003, 55, 329–347. [Google Scholar] [CrossRef] [PubMed]
- Doane, T.L.; Burda, C. The unique role of nanoparticles in nanomedicine: Imaging, drug delivery and therapy. Chem. Soc. Rev. 2012, 41, 2885–2911. [Google Scholar] [CrossRef] [PubMed]
- Bartneck, M. Immunomodulatory Nanomedicine. Macromol. Biosci. 2017, 17, 1700021. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, L.N.M.; Franz-Montan, M.; Alcantara, A.C.S.; Breitkreitz, M.C.; Castro, S.R.; Guilherme, V.A.; Muniz, B.V.; Rodrigues da Silva, G.H.; de Paula, E. Hybrid nanofilms as topical anesthetics for pain-free procedures in dentistry. Sci. Rep. 2020, 10, 11341. [Google Scholar] [CrossRef] [PubMed]
- Weldon, C.; Ji, T.; Nguyen, M.T.; Rwei, A.; Wang, W.; Hao, Y.; Zhao, C.; Mehta, M.; Wang, B.Y.; Tsui, J.; et al. Nanoscale Bupivacaine Formulations To Enhance the Duration and Safety of Intravenous Regional Anesthesia. ACS Nano 2019, 13, 18–25. [Google Scholar] [CrossRef]
- Bucalo, B.D.; Mirikitani, E.J.; Moy, R.L. Comparison of skin anesthetic effect of liposomal lidocaine, nonliposomal lidocaine, and EMLA using 30-minute application time. Dermatol. Surg. 1998, 24, 537–541. [Google Scholar] [CrossRef]
- Grillo, R.; de Melo, N.F.; de Araujo, D.R.; de Paula, E.; Rosa, A.H.; Fraceto, L.F. Polymeric alginate nanoparticles containing the local anesthetic bupivacaine. J. Drug Target. 2010, 18, 688–699. [Google Scholar] [CrossRef]
- Boogaerts, J.G.; Lafont, N.D.; Luo, H.; Legros, F.J. Plasma concentrations of bupivacaine after brachial plexus administration of liposome-associated and plain solutions to rabbits. Can. J. Anaesth. 1993, 40, 1201–1204. [Google Scholar] [CrossRef]
- Boogaerts, J.; Declercq, A.; Lafont, N.; Benameur, H.; Akodad, E.M.; Dupont, J.C.; Legros, F.J. Toxicity of bupivacaine encapsulated into liposomes and injected intravenously: Comparison with plain solutions. Anesth. Analg. 1993, 76, 553–555. [Google Scholar] [CrossRef]
- Cohen, R.; Kanaan, H.; Grant, G.J.; Barenholz, Y. Prolonged analgesia from Bupisome and Bupigel formulations: From design and fabrication to improved stability. J. Control. Release 2012, 160, 346–352. [Google Scholar] [CrossRef]
- Wiziack Zago, P.M.; Baroni, D.B.; Groppo, F.C.; de Paula, E.; Ranali, J.; Volpato, M.C. Anesthetic efficacy of liposomal prilocaine in maxillary infiltration anesthesia. J. Liposome Res. 2011, 21, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Bragagni, M.; Maestrelli, F.; Mennini, N.; Ghelardini, C.; Mura, P. Liposomal formulations of prilocaine: Effect of complexation with hydroxypropyl-ss-cyclodextrin on drug anesthetic efficacy. J. Liposome Res. 2010, 20, 315–322. [Google Scholar] [CrossRef]
- Tofoli, G.R.; Cereda, C.M.; Groppo, F.C.; Volpato, M.C.; Franz-Montan, M.; Ranali, J.; de Araujo, D.R.; de Paula, E. Efficacy of liposome-encapsulated mepivacaine for infiltrative anesthesia in volunteers. J. Liposome Res. 2011, 21, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Tofoli, G.R.; Cereda, C.M.; Araujo, D.R.; Franz-Montan, M.; Groppo, F.C.; Quaglio, D.; Pedrazzoli Junior, J.; Calafatti, S.A.; Barros, F.A.; de Paula, E. Pharmacokinetic study of liposome-encapsulated and plain mepivacaine formulations injected intra-orally in volunteers. J. Pharm. Pharmacol. 2012, 64, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Franz-Montan, M.; Bergamaschi, C.d.C.; de Paula, E.; Groppo, F.C.; Ranali, J.; Fraceto, L.F.; Volpato, M.C. Pharmacokinetic profile of liposome-encapsulated ropivacaine after maxillary infiltration anaesthesia. J. Braz. Chem. Soc. 2010, 21, 1945–1951. [Google Scholar] [CrossRef]
- Schmidt, G.N.; Müller, J.; Bischoff, P. Measurement of the depth of anaesthesia. Anaesthesist 2008, 57, 9–30, 32–36. [Google Scholar] [CrossRef]
- Zhang, Q.; Xia, L.Y.; Liang, W.D.; Rao, D.Y.; Zhu, P.P.; Huang, K.N.; Deng, Z.H.; Zhong, M.L. Intrathecal Dexmedetomidine Combined With Ropivacaine in Cesarean Section: A Prospective Randomized Double-Blind Controlled Study. Front. Med. 2022, 9, 922611. [Google Scholar] [CrossRef]
- Liu, G.L.; Bian, W.C.; Zhao, P.; Sun, L.H. Delivery of Local Anesthesia: Current Strategies, Safety, and Future Prospects. Curr. Drug Metab. 2019, 20, 533–539. [Google Scholar] [CrossRef]
- Duret, C.; Wauthoz, N.; Sebti, T.; Vanderbist, F.; Amighi, K. Solid dispersions of itraconazole for inhalation with enhanced dissolution, solubility and dispersion properties. Int. J. Pharm. 2012, 428, 103–113. [Google Scholar] [CrossRef]
- Strauss, J.M.; Giest, J. Total intravenöse Anästhesie. Auf dem Weg zum Standardverfahren bei Kindern [Total intravenous anesthesia. On the way to standard practice in pediatrics]. Anaesthesist 2003, 52, 763–777. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, L.; Chan, H.K.; Watanabe, W. Formation, characterization, and fate of inhaled drug nanoparticles. Adv. Drug Deliv. Rev. 2011, 63, 441–455. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Peters, J.I.; Williams, R.O., 3rd. Inhaled nanoparticles—A current review. Int. J. Pharm. 2008, 356, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Rogueda, P.G.; Traini, D. The nanoscale in pulmonary delivery. Part 1: Deposition, fate, toxicology and effects. Expert Opin. Drug Deliv. 2007, 4, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Salama, I.E.; Jenkins, C.L.; Davies, A.; Clark, J.N.; Wilkes, A.R.; Hall, J.E.; Paul, A. Volatile fluorinated nanoemulsions: A chemical route to controlled delivery of inhalation anesthesia. J. Colloid Interface Sci. 2015, 440, 78–83. [Google Scholar] [CrossRef]
- Ali, R.; Jain, G.K.; Iqbal, Z.; Talegaonkar, S.; Pandit, P.; Sule, S.; Malhotra, G.; Khar, R.K.; Bhatnagar, A.; Ahmad, F.J. Development and clinical trial of nano-atropine sulfate dry powder inhaler as a novel poisoning antidote. Nanomedicine 2009, 5, 55–63. [Google Scholar] [CrossRef]
- Natalini, C.C.; Krahn, C.L.; Serpa, P.B.S.; Griffith, J.E.; de Almeida, R.M. Intravenous 15% isoflurane lipid nanoemulsion for general anesthesia in dogs. Vet. Anaesth. Analg. 2017, 44, 219–227. [Google Scholar] [CrossRef]
- Wu, Q.; Qin, M.; Zhang, K. Synthesis of sevoflurane loaded reduced graphene oxide nanoparticles system for neuroprotective effects for preconditioning against focal cerebral ischaemia. Artif. Cells Nanomed. Biotechnol. 2019, 47, 3517–3523. [Google Scholar] [CrossRef]
- Sukhani, R.; Garcia, C.J.; Munhall, R.J.; Winnie, A.P.; Rodvold, K.A. Lidocaine disposition following intravenous regional anesthesia with different tourniquet deflation technics. Anesth. Analg. 1989, 68, 633–637. [Google Scholar] [CrossRef]
- Davies, J.A.; Walford, A.J. Intravenous regional anaesthesia for foot surgery. Acta Anaesthesiol. Scand. 1986, 30, 145–147. [Google Scholar] [CrossRef]
- Kim, D.D.; Shuman, C.; Sadr, B. Intravenous regional anesthesia for outpatient foot and ankle surgery: A prospective study. Orthopedics 1993, 16, 1109–1113. [Google Scholar] [CrossRef]
- Hennig, R.; Pollinger, K.; Veser, A.; Breunig, M.; Goepferich, A. Nanoparticle multivalency counterbalances the ligand affinity loss upon PEGylation. J. Control. Release 2014, 194, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Jokerst, J.V.; Lobovkina, T.; Zare, R.N.; Gambhir, S.S. Nanoparticle PEGylation for imaging and therapy. Nanomedicine 2011, 4, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Davidson, E.M.; Barenholz, Y.; Cohen, R.; Haroutiunian, S.; Kagan, L.; Ginosar, Y. High-dose bupivacaine remotely loaded into multivesicular liposomes demonstrates slow drug release without systemic toxic plasma concentrations after subcutaneous administration in humans. Anesth. Analg. 2010, 110, 1018–1023. [Google Scholar] [CrossRef]
- Reader, R.C.; McCarthy, R.J.; Schultz, K.L.; Volturo, A.R.; Barton, B.A.; O’Hara, M.J.; Abelson, A.L. Comparison of liposomal bupivacaine and 0.5% bupivacaine hydrochloride for control of postoperative pain in dogs undergoing tibial plateau leveling osteotomy. J. Am. Vet. Med. Assoc. 2020, 256, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Campoy, L.; Martin-Flores, M.; Gleed, R.D.; Taylor, L.C.; Yant, J.E.; Pavlinac, R. Block duration is substantially longer with a liposomal suspension of bupivacaine than with 0.5% bupivacaine HCl potentiated with dexmedetomidine following an ultrasound-guided sciatic nerve block in Beagles. Am. J. Vet. Res. 2022, 83, ajvr.22.01.0007. [Google Scholar] [CrossRef]
- Kopacz, D.J.; Bernards, C.M.; Allen, H.W.; Landau, C.; Nandy, P.; Wu, D.; Lacouture, P.G. A model to evaluate the pharmacokinetic and pharmacodynamic variables of extended-release products using in vivo tissue microdialysis in humans: Bupivacaine-loaded microcapsules. Anesth. Analg. 2003, 97, 124–131, table of contents. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhao, Q. Long-term anesthetic analgesic effects: Comparison of tetracaine loaded polymeric nanoparticles, solid lipid nanoparticles, and nanostructured lipid carriers in vitro and in vivo. Biomed. Pharmacother. 2019, 117, 109057. [Google Scholar] [CrossRef]
- Altinyazar, H.C.; Ozdemir, H.; Koca, R.; Hosnuter, M.; Demirel, C.B.; Gundogdu, S. Epinephrine in digital block: Color Doppler flow imaging. Dermatol. Surg. 2004, 30, 508–511. [Google Scholar] [CrossRef]
- Negi, P.; Singh, B.; Sharma, G.; Beg, S.; Katare, O.P. Biocompatible lidocaine and prilocaine loaded-nanoemulsion system for enhanced percutaneous absorption: QbD-based optimisation, dermatokinetics and in vivo evaluation. J. Microencapsul. 2015, 32, 419–431. [Google Scholar] [CrossRef]
- Meng, J.; Sturgis, T.F.; Youan, B.B. Engineering tenofovir loaded chitosan nanoparticles to maximize microbicide mucoadhesion. Eur. J. Pharm. Sci. 2011, 44, 57–67. [Google Scholar] [CrossRef]
- Yin, Y.M.; Cui, F.D.; Mu, C.F.; Choi, M.-K.; Kim, J.S.; Chung, S.-J.; Shim, C.-K.; Kim, D.-D. Docetaxel microemulsion for enhanced oral bioavailability: Preparation and in vitro and in vivo evaluation. J. Control. Release 2009, 140, 86–94. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, X.; Gu, Y.; Cheng, Y.; Cao, F. Recent advance of nanoparticle-based topical drug delivery to the posterior segment of the eye. Expert Opin. Drug Deliv. 2018, 15, 687–701. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.G.; Dias, K.; Pereira, T.A.; Bernardi, D.S.; Lopez, R.F. Topical delivery of ocular therapeutics: Carrier systems and physical methods. J. Pharm. Pharmacol. 2014, 66, 507–530. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, P.; Patil, A.; Majumdar, S. Recent advances in topical nano drug-delivery systems for the anterior ocular segment. Ther. Deliv. 2018, 9, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, A.Z.; Eliasen, R.; Oswald, J.; Kempen, P.J.; Melander, F.; Andresen, T.L.; Young, M.; Baranov, P.; Urquhart, A.J. Multifarious Biologic Loaded Liposomes that Stimulate the Mammalian Target of Rapamycin Signaling Pathway Show Retina Neuroprotection after Retina Damage. ACS Nano 2018, 12, 7497–7508. [Google Scholar] [CrossRef]
- Kelly, D.J.; Ahmad, M.; Brull, S.J. Preemptive analgesia I: Physiological pathways and pharmacological modalities. Can. J. Anaesth. 2001, 48, 1000–1010. [Google Scholar] [CrossRef]
- Bell, A. The neurobiology of acute pain. Vet. J. 2018, 237, 55–62. [Google Scholar] [CrossRef]
- Ellison, D.L. Physiology of Pain. Crit. Care Nurs. Clin. N. Am. 2017, 29, 397–406. [Google Scholar] [CrossRef]
- Domínguez-Oliva, A.; Mota-Rojas, D.; Hernández-Avalos, I.; Mora-Medina, P.; Olmos-Hernández, A.; Verduzco-Mendoza, A.; Casas-Alvarado, A.; Whittaker, A.L. The neurobiology of pain and facial movements in rodents: Clinical applications and current research. Front. Vet. Sci. 2022, 9, 1016720. [Google Scholar] [CrossRef]
- Scholl, L.; Seth, P.; Kariisa, M.; Wilson, N.; Baldwin, G. Drug and Opioid-Involved Overdose Deaths—United States, 2013–2017. MMWR Morb. Mortal Wkly Rep. 2018, 67, 1419–1427. [Google Scholar] [CrossRef]
- Mazaleuskaya, L.L.; Muzykantov, V.R.; FitzGerald, G.A. Nanotherapeutic-directed approaches to analgesia. Trends Pharmacol. Sci. 2021, 42, 527–550. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.J.; Aljohani, D.M.; Forget, P. Perioperative opioids: A narrative review contextualising new avenues to improve prescribing. Br. J. Anaesth. 2023, 130, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Babaie, S.; Taghvimi, A.; Hong, J.H.; Hamishehkar, H.; An, S.; Kim, K.H. Recent advances in pain management based on nanoparticle technologies. J. Nanobiotechnol. 2022, 20, 290. [Google Scholar] [CrossRef] [PubMed]
- Kesmati, M.; Torabi, M. Interaction between Analgesic Effect of Nano and Conventional size of Zinc Oxide and Opioidergic System Activity in Animal Model of Acute Pain. Basic Clin. Neurosci. 2014, 5, 80–87. [Google Scholar]
- Nosrati, N.; Hassanpour-Ezzati, M.; Mousavi, S.Z.; Rezagholiyan, S. Comparison of MnO2 nanoparticles and microparticles distribution in CNS and muscle and efect on acute pain threshold in rats. Nanomed. J. 2014, 1, 180–190. [Google Scholar]
- Wu, P.C.; Hsiao, H.T.; Lin, Y.C.; Shieh, D.B.; Liu, Y.C. The analgesia efficiency of ultrasmall magnetic iron oxide nanoparticles in mice chronic inflammatory pain model. Nanomedicine 2017, 13, 1975–1981. [Google Scholar] [CrossRef] [PubMed]
- Ghalandarlaki, N.; Alizadeh, A.M.; Ashkani-Esfahani, S. Nanotechnology-applied curcumin for different diseases therapy. Biomed. Res. Int. 2014, 2014, 394264. [Google Scholar] [CrossRef]
- Shanthanna, H.; Nelson, A.M.; Kissoon, N.; Narouze, S. The COVID-19 pandemic and its consequences for chronic pain: A narrative review. Anaesthesia 2022, 77, 1039–1050. [Google Scholar] [CrossRef]
- Mariano, E.R.; Dickerson, D.M.; Szokol, J.W.; Harned, M.; Mueller, J.T.; Philip, B.K.; Baratta, J.L.; Gulur, P.; Robles, J.; Schroeder, K.M.; et al. A multisociety organizational consensus process to define guiding principles for acute perioperative pain management. Reg. Anesth. Pain Med. 2022, 47, 118–127. [Google Scholar] [CrossRef]
- Wick, E.C.; Grant, M.C.; Wu, C.L. Postoperative Multimodal Analgesia Pain Management With Nonopioid Analgesics and Techniques: A Review. JAMA Surg. 2017, 152, 691–697. [Google Scholar] [CrossRef]
- Beiranvand, S.; Sorori, M.M. Pain management using nanotechnology approaches. Artif. Cells Nanomed. Biotechnol. 2019, 47, 462–468. [Google Scholar] [CrossRef]
- Moradkhani, M.R.; Karimi, A.; Negahdari, B. Nanotechnology application for pain therapy. Artif. Cells Nanomed. Biotechnol. 2018, 46, 368–373. [Google Scholar] [CrossRef]
- Dong, J.; Jiang, D.; Wang, Z.; Wu, G.; Miao, L.; Huang, L. Intra-articular delivery of liposomal celecoxib-hyaluronate combination for the treatment of osteoarthritis in rabbit model. Int. J. Pharm. 2013, 441, 285–290. [Google Scholar]
- Van Boekel, R.L.M.; Warle, M.C.; Nielen, R.G.C.; Vissers, K.C.P.; van der Sande, R.; Bronkhorst, E.M.; Lerou, J.G.C.; Steegers, M.A.H. Relationship Between Postoperative Pain and Overall 30-Day Complications in a Broad Surgical Population: An Observational Study. Ann. Surg. 2019, 269, 856–865. [Google Scholar] [CrossRef]
- Gorfine, S.R.; Onel, E.; Patou, G.; Krivokapic, Z.V. Bupivacaine extended-release liposome injection for prolonged postsurgical analgesia in patients undergoing hemorrhoidectomy: A multicenter, randomized, double-blind, placebo-controlled trial. Dis. Colon. Rectum. 2011, 54, 1552–1559. [Google Scholar] [CrossRef]
- Grant, G.J.; Barenholz, Y.; Bolotin, E.M.; Bansinath, M.; Turndorf, H.; Piskoun, B.; Davidson, E.M. A novel liposomal bupivacaine formulation to produce ultralong-acting analgesia. Anesthesiology 2004, 101, 133–137. [Google Scholar] [CrossRef]
- Jones, C.L.; Gruber, D.D.; Fischer, J.R.; Leonard, K.; Hernandez, S.L. Liposomal bupivacaine efficacy for postoperative pain following posterior vaginal surgery: A randomized, double-blind, placebo-controlled trial. Am. J. Obstet. Gynecol. 2018, 219, 500.E1–500.E8. [Google Scholar] [CrossRef] [PubMed]
- Hergert, M.; Rosolski, T.; Lestin, H.G.; Stranz, G. Postoperative Epiduralanalgesie—Stellenwert, Indikationen und Management [Postoperative epidural analgesia—Current status, indications and management]. Anaesthesiol. Reanim. 2002, 27, 152–159. [Google Scholar] [PubMed]
- Rodriguez, J.; Barcena, M.; Taboada-Muniz, M.; Alvarez, J. Horner syndrome after unintended subdural block. A report of 2 cases. J. Clin. Anesth. 2005, 17, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Ready, L.B. Acute pain: Lessons learned from 25,000 patients. Reg. Anesth. Pain Med. 1999, 24, 499–505. [Google Scholar] [CrossRef]
- Boogaerts, J.G.; Lafont, N.D.; Declercq, A.G.; Luo, H.C.; Gravet, E.T.; Bianchi, J.A.; Legros, F.J. Epidural administration of liposome-associated bupivacaine for the management of postsurgical pain: A first study. J. Clin. Anesth. 1994, 6, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Lafont, N.D.; Legros, F.J.; Boogaerts, J.G. Use of liposome-associated bupivacaine in a cancer pain syndrome. Anaesthesia 1996, 51, 578–579. [Google Scholar] [CrossRef] [PubMed]
- Lafont, N.D.; Boogaerts, J.G.; Legros, F.J. Use of liposome-associated bupivacaine for the management of a chronic pain syndrome. Anesth. Analg. 1994, 79, 818. [Google Scholar] [CrossRef]
- Hernández-Avalos, I.; Mota-Rojas, D.; Mendoza-Flores, J.E.; Casas-Alvarado, A.; Flores-Padilla, K.; Miranda-Cortes, A.E.; Torres-Bernal, F.; Gómez-Prado, J.; Mora-Medina, P. Nociceptive pain and anxiety in equines: Physiological and behavioral alterations. Vet. World. 2021, 14, 2984–2995. [Google Scholar] [CrossRef] [PubMed]
- Helander, E.M.; Menard, B.L.; Harmon, C.M.; Homra, B.K.; Allain, A.V.; Bordelon, G.J.; Wyche, M.Q.; Padnos, I.W.; Lavrova, A.; Kaye, A.D. Multimodal Analgesia, Current Concepts, and Acute Pain Considerations. Curr. Pain Headache Rep. 2017, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- You, P.; Yuan, R.; Chen, C. Design and evaluation of lidocaine- and prilocaine-coloaded nanoparticulate drug delivery systems for topical anesthetic analgesic therapy: A comparison between solid lipid nanoparticles and nanostructured lipid carriers. Drug Des. Devel. Ther. 2017, 11, 2743–2752. [Google Scholar] [CrossRef]
- Yuan, S.; Chen, J.; Feng, S.; Li, M.; Sun, Y.; Liu, Y. Combination anesthetic therapy: Co-delivery of ropivacaine and meloxicam using transcriptional transactivator peptide modified nanostructured lipid carriers in vitro and in vivo. Drug Deliv. 2022, 29, 263–269. [Google Scholar] [CrossRef]
- Yang, Y.; Qiu, D.; Liu, Y.; Chao, L. Topical anesthetic analgesic therapy using the combination of ropivacaine and dexmedetomidine: Hyaluronic acid modified long-acting nanostructured lipid carriers containing a skin penetration enhancer. Drug Des. Devel. Ther. 2019, 13, 3307–3319. [Google Scholar] [CrossRef]
- Khalil, R.M.; Abd-Elbary, A.; Kassem, M.A.; Ghorab, M.M.; Basha, M. Nanostructured lipid carriers (NLCs) versus solid lipid nanoparticles (SLNs) for topical delivery of meloxicam. Pharm. Dev. Technol. 2014, 19, 304–314. [Google Scholar] [CrossRef]
- Tran, T.H.; Shah, A.T.; Loh, M.L. Precision Medicine in Pediatric Oncology: Translating Genomic Discoveries into Optimized Therapies. Clin. Cancer Res. 2017, 23, 5329–5338. [Google Scholar] [CrossRef]
- Williams, J.K.; Feero, W.G.; Leonard, D.G.; Coleman, B. Implementation science, genomic precision medicine, and improved health: A new path forward? Nurs. Outlook 2017, 65, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Kirchheiner, J.; Fuhr, U.; Brockmoller, J. Pharmacogenetics-based therapeutic recommendations--ready for clinical practice? Nat. Rev. Drug Discov. 2005, 4, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Cecchin, E.; Roncato, R.; Guchelaar, H.J.; Toffoli, G.; Ubiquitous Pharmacogenomics, C. Ubiquitous Pharmacogenomics (U-PGx): The Time for Implementation is Now. An Horizon2020 Program to Drive Pharmacogenomics into Clinical Practice. Curr. Pharm. Biotechnol. 2017, 18, 204–209. [Google Scholar] [CrossRef]
- Cacabelos, R.; Naidoo, V.; Corzo, L.; Cacabelos, N.; Carril, J.C. Genophenotypic Factors and Pharmacogenomics in Adverse Drug Reactions. Int. J. Mol. Sci. 2021, 22, 13302. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Ma, J.; Li, M.; Zhang, Y.; Jiang, B.; Zhao, X.; Huai, C.; Shen, L.; Zhang, N.; He, L.; et al. Cytochrome P450 Enzymes and Drug Metabolism in Humans. Int. J. Mol. Sci. 2021, 22, 12808. [Google Scholar] [CrossRef]
- Danielson, P.B. The cytochrome P450 superfamily: Biochemistry, evolution and drug metabolism in humans. Curr. Drug Metab. 2002, 3, 561–597. [Google Scholar] [CrossRef]
- Pinto, N.; Dolan, M.E. Clinically relevant genetic variations in drug metabolizing enzymes. Curr. Drug Metab. 2011, 12, 487–497. [Google Scholar] [CrossRef]
- Anzenbacherova, E.; Spicakova, A.; Jourova, L.; Ulrichova, J.; Adamus, M.; Bachleda, P.; Anzenbacher, P. Interaction of rocuronium with human liver cytochromes P450. J. Pharmacol. Sci. 2015, 127, 190–195. [Google Scholar] [CrossRef]
- Bahar, M.A.; Setiawan, D.; Hak, E.; Wilffert, B. Pharmacogenetics of drug-drug interaction and drug-drug-gene interaction: A systematic review on CYP2C9, CYP2C19 and CYP2D6. Pharmacogenomics 2017, 18, 701–739. [Google Scholar] [CrossRef]
- Kaye, A.D.; Mahakian, T.; Kaye, A.J.; Pham, A.A.; Hart, B.M.; Gennuso, S.; Cornett, E.M.; Gabriel, R.A.; Urman, R.D. Pharmacogenomics, precision medicine, and implications for anesthesia care. Best Pract. Res. Clin. Anaesthesiol. 2018, 32, 61–81. [Google Scholar] [CrossRef]
- Samer, C.F.; Lorenzini, K.I.; Rollason, V.; Daali, Y.; Desmeules, J.A. Applications of CYP450 testing in the clinical setting. Mol. Diagn. Ther. 2013, 17, 165–184. [Google Scholar] [CrossRef] [PubMed]
- Tornio, A.; Backman, J.T. Cytochrome P450 in Pharmacogenetics: An Update. Adv. Pharmacol. 2018, 83, 3–32. [Google Scholar] [CrossRef] [PubMed]
- Bank, P.C.D.; Swen, J.J.; Guchelaar, H.J. Estimated nationwide impact of implementing a preemptive pharmacogenetic panel approach to guide drug prescribing in primary care in The Netherlands. BMC Med. 2019, 17, 110. [Google Scholar] [CrossRef] [PubMed]
- Murayama, N.; Soyama, A.; Saito, Y.; Nakajima, Y.; Komamura, K.; Ueno, K.; Kamakura, S.; Kitakaze, M.; Kimura, H.; Goto, Y.; et al. Six novel nonsynonymous CYP1A2 gene polymorphisms: Catalytic activities of the naturally occurring variant enzymes. J. Pharmacol. Exp. Ther. 2004, 308, 300–306. [Google Scholar] [CrossRef]
- Mei, Y.; Wang, S.Y.; Li, Y.; Yi, S.Q.; Wang, C.Y.; Yang, M.; Duan, K.M. Role of SLCO1B1, ABCB1, and CHRNA1 gene polymorphisms on the efficacy of rocuronium in Chinese patients. J. Clin. Pharmacol. 2015, 55, 261–268. [Google Scholar] [CrossRef]
- Liem, E.B.; Joiner, T.V.; Tsueda, K.; Sessler, D.I. Increased sensitivity to thermal pain and reduced subcutaneous lidocaine efficacy in redheads. Anesthesiology 2005, 102, 509–514. [Google Scholar] [CrossRef]
- Girard, T.; Suhner, M.; Levano, S.; Singer, M.; Zollinger, A.; Hofer, C.K. A fulminant malignant hyperthermia episode in a patient with ryanodine receptor gene mutation p.Tyr522Ser. Anesth. Analg. 2008, 107, 1953–1955. [Google Scholar] [CrossRef]
- Liem, E.B.; Lin, C.M.; Suleman, M.I.; Doufas, A.G.; Gregg, R.G.; Veauthier, J.M.; Loyd, G.; Sessler, D.I. Anesthetic requirement is increased in redheads. Anesthesiology 2004, 101, 279–283. [Google Scholar] [CrossRef]
- Kirchheiner, J.; Schmidt, H.; Tzvetkov, M.; Keulen, J.T.; Lotsch, J.; Roots, I.; Brockmoller, J. Pharmacokinetics of codeine and its metabolite morphine in ultra-rapid metabolizers due to CYP2D6 duplication. Pharmacogenom. J. 2007, 7, 257–265. [Google Scholar] [CrossRef]
- Klees, T.M.; Sheffels, P.; Thummel, K.E.; Kharasch, E.D. Pharmacogenetic determinants of human liver microsomal alfentanil metabolism and the role of cytochrome P450 3A5. Anesthesiology 2005, 102, 550–556. [Google Scholar] [CrossRef]
- Reyes-Gibby, C.C.; Shete, S.; Rakvag, T.; Bhat, S.V.; Skorpen, F.; Bruera, E.; Kaasa, S.; Klepstad, P. Exploring joint effects of genes and the clinical efficacy of morphine for cancer pain: OPRM1 and COMT gene. Pain 2007, 130, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Bastami, S.; Gupta, A.; Zackrisson, A.L.; Ahlner, J.; Osman, A.; Uppugunduri, S. Influence of UGT2B7, OPRM1 and ABCB1 gene polymorphisms on postoperative morphine consumption. Basic Clin. Pharmacol. Toxicol. 2014, 115, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Lv, B.; Zhao, X.; Zhang, Y. Effects of OPRM1 and ABCB1 gene polymorphisms on the analgesic effect and dose of sufentanil after thoracoscopic-assisted radical resection of lung cancer. Biosci. Rep. 2019, 39, BSR20181211. [Google Scholar] [CrossRef] [PubMed]
- Campa, D.; Gioia, A.; Tomei, A.; Poli, P.; Barale, R. Association of ABCB1/MDR1 and OPRM1 gene polymorphisms with morphine pain relief. Clin. Pharmacol. Ther. 2008, 83, 559–566. [Google Scholar] [CrossRef]
- Oliva, A.; Alvarado, A.; Cortés, A.; Avalos, I. Clinical pharmacology of tramadol and tapentadol, and their therapeutic efficacy in different models of acute and chronic pain in dogs and cats. J. Adv. Vet. Anim. Res. 2021, 8, 404–422. [Google Scholar] [CrossRef]
- Perez Jimenez, T.E.; Mealey, K.L.; Schnider, D.; Grubb, T.L.; Greene, S.A.; Court, M.H. Identification of canine cytochrome P-450s (CYPs) metabolizing the tramadol (+)-M1 and (+)-M2 metabolites to the tramadol (+)-M5 metabolite in dog liver microsomes. J. Vet. Pharmacol. Ther. 2018, 41, 815–824. [Google Scholar] [CrossRef]
- Zhong, Q.; Chen, X.; Zhao, Y.; Liu, R.; Yao, S. Association of Polymorphisms in Pharmacogenetic Candidate Genes with Propofol Susceptibility. Sci. Rep. 2017, 7, 3343. [Google Scholar] [CrossRef]
- Kapur, B.M.; Lala, P.K.; Shaw, J.L. Pharmacogenetics of chronic pain management. Clin. Biochem. 2014, 47, 1169–1187. [Google Scholar] [CrossRef]
- Delacour, H.; Lushchekina, S.; Mabboux, I.; Bousquet, A.; Ceppa, F.; Schopfer, L.M.; Lockridge, O.; Masson, P. Characterization of a novel BCHE “silent” allele: Point mutation (p.Val204Asp) causes loss of activity and prolonged apnea with suxamethonium. PLoS ONE 2014, 9, e101552. [Google Scholar] [CrossRef]
- Purohit, P.G.; Tate, R.J.; Pow, E.; Hill, D.; Connolly, J.G. The role of the amino acid residue at alpha1:189 in the binding of neuromuscular blocking agents to mouse and human muscle nicotinic acetylcholine receptors. Br. J. Pharmacol. 2007, 150, 920–931. [Google Scholar] [CrossRef]
- Yuan, H.Y.; Chen, J.J.; Lee, M.T.; Wung, J.C.; Chen, Y.F.; Charng, M.J.; Lu, M.J.; Hung, C.R.; Wei, C.Y.; Chen, C.H.; et al. A novel functional VKORC1 promoter polymorphism is associated with inter-individual and inter-ethnic differences in warfarin sensitivity. Hum. Mol. Genet. 2005, 14, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Huddart, R.; Altman, R.B.; Klein, T.E. PharmGKB summary: Ondansetron and tropisetron pathways, pharmacokinetics and pharmacodynamics. Pharmacogenet Genom. 2019, 29, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.F.; Wang, B.; Yang, L.P.; Liu, J.P. Structure, function, regulation and polymorphism and the clinical significance of human cytochrome P450 1A2. Drug Metab. Rev. 2010, 42, 268–354. [Google Scholar] [CrossRef] [PubMed]
- Koonrungsesomboon, N.; Khatsri, R.; Wongchompoo, P.; Teekachunhatean, S. The impact of genetic polymorphisms on CYP1A2 activity in humans: A systematic review and meta-analysis. Pharmacogenom. J. 2018, 18, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, V.; Huang, N.; Miller, W.L. Pharmacogenetics of P450 oxidoreductase: Effect of sequence variants on activities of CYP1A2 and CYP2C19. Pharmacogenet. Genom. 2008, 18, 569–576. [Google Scholar] [CrossRef]
- Manikandan, P.; Nagini, S. Cytochrome P450 Structure, Function and Clinical Significance: A Review. Curr. Drug Targets 2018, 19, 38–54. [Google Scholar] [CrossRef]
- Waring, R.H. Cytochrome P450: Genotype to phenotype. Xenobiotica 2020, 50, 9–18. [Google Scholar] [CrossRef]
- Baker, W.L.; Johnson, S.G. Pharmacogenetics and oral antithrombotic drugs. Curr. Opin. Pharmacol. 2016, 27, 38–42. [Google Scholar] [CrossRef]
- Yin, T.; Miyata, T. Warfarin dose and the pharmacogenomics of CYP2C9 and VKORC1—Rationale and perspectives. Thromb. Res. 2007, 120, 1–10. [Google Scholar] [CrossRef]
- Inomata, S.; Nagashima, A.; Itagaki, F.; Homma, M.; Nishimura, M.; Osaka, Y.; Okuyama, K.; Tanaka, E.; Nakamura, T.; Kohda, Y.; et al. CYP2C19 genotype affects diazepam pharmacokinetics and emergence from general anesthesia. Clin. Pharmacol. Ther. 2005, 78, 647–655. [Google Scholar] [CrossRef]
- Crews, K.R.; Monte, A.A.; Huddart, R.; Caudle, K.E.; Kharasch, E.D.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Callaghan, J.T.; Samer, C.F.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin. Pharmacol. Ther. 2021, 110, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Bell, G.C.; Caudle, K.E.; Whirl-Carrillo, M.; Gordon, R.J.; Hikino, K.; Prows, C.A.; Gaedigk, A.; Agundez, J.; Sadhasivam, S.; Klein, T.E.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for CYP2D6 genotype and use of ondansetron and tropisetron. Clin. Pharmacol. Ther. 2017, 102, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Meloche, M.; Khazaka, M.; Kassem, I.; Barhdadi, A.; Dube, M.P.; de Denus, S. CYP2D6 polymorphism and its impact on the clinical response to metoprolol: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2020, 86, 1015–1033. [Google Scholar] [CrossRef] [PubMed]
- Al-Eitan, L.N.; Almasri, A.Y.; Khasawneh, R.H. Impact of CYP2C9 and VKORC1 Polymorphisms on Warfarin Sensitivity and Responsiveness in Jordanian Cardiovascular Patients during the Initiation Therapy. Genes 2018, 9, 578. [Google Scholar] [CrossRef]
- Zuo, Q.; Li, L.; Zhong, M.; Chen, G.; Xio, J. Correlation between CYP2C9 gene polymorphism and warfarin dose in Chinese Han population with coronary heart disease. Cell Mol. Biol. 2021, 67, 157–163. [Google Scholar] [CrossRef]
- Kim, H.S.; Cho, D.Y.; Park, B.M.; Bae, S.K.; Yoon, Y.J.; Oh, M.; Ghim, J.L.; Kim, E.Y.; Kim, D.H.; Shin, J.G. The effect of CYP2C19 genotype on the time course of platelet aggregation inhibition after clopidogrel administration. J. Clin. Pharmacol. 2014, 54, 850–857. [Google Scholar] [CrossRef]
- Mega, J.L.; Simon, T.; Collet, J.P.; Anderson, J.L.; Antman, E.M.; Bliden, K.; Cannon, C.P.; Danchin, N.; Giusti, B.; Gurbel, P.; et al. Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with clopidogrel predominantly for PCI: A meta-analysis. JAMA 2010, 304, 1821–1830. [Google Scholar] [CrossRef]
- Zubiaur, P.; Figueiredo-Tor, L.; Villapalos-Garcia, G.; Soria-Chacartegui, P.; Navares-Gomez, M.; Novalbos, J.; Matas, M.; Calleja, S.; Mejia-Abril, G.; Roman, M.; et al. Association between CYP2C19 and CYP2B6 phenotypes and the pharmacokinetics and safety of diazepam. Biomed. Pharmacother. 2022, 155, 113747. [Google Scholar] [CrossRef]
- He, Z.X.; Chen, X.W.; Zhou, Z.W.; Zhou, S.F. Impact of physiological, pathological and environmental factors on the expression and activity of human cytochrome P450 2D6 and implications in precision medicine. Drug Metab. Rev. 2015, 47, 470–519. [Google Scholar] [CrossRef]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Klein, T.E.; Shen, D.D.; Callaghan, J.T.; Kharasch, E.D.; Skaar, T.C.; Clinical Pharmacogenetics Implementation, C. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for codeine therapy in the context of cytochrome P450 2D6 (CYP2D6) genotype. Clin. Pharmacol. Ther. 2012, 91, 321–326. [Google Scholar] [CrossRef]
- Xu, M.; Zheng, L.; Zeng, J.; Xu, W.; Jiang, X.; Wang, L. Physiologically based pharmacokinetic modeling of tramadol to inform dose adjustment and drug-drug interactions according to CYP2D6 phenotypes. Pharmacotherapy 2021, 41, 277–290. [Google Scholar] [CrossRef]
- Anstensrud, A.K.; Molden, E.; Haug, H.J.; Qazi, R.; Muriq, H.; Fosshaug, L.E.; Spigset, O.; Oie, E. Impact of genotype-predicted CYP2D6 metabolism on clinical effects and tolerability of metoprolol in patients after myocardial infarction—A prospective observational study. Eur. J. Clin. Pharmacol. 2020, 76, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Swen, J.J.; Nijenhuis, M.; de Boer, A.; Grandia, L.; Maitland-van der Zee, A.H.; Mulder, H.; Rongen, G.A.; van Schaik, R.H.; Schalekamp, T.; Touw, D.J.; et al. Pharmacogenetics: From bench to byte—An update of guidelines. Clin. Pharmacol. Ther. 2011, 89, 662–673. [Google Scholar] [CrossRef]
- Nieminen, T.; Lehtimaki, T.; Maenpaa, J.; Ropo, A.; Uusitalo, H.; Kahonen, M. Ophthalmic timolol: Plasma concentration and systemic cardiopulmonary effects. Scand. J. Clin. Lab. Investig. 2007, 67, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Rytkonen, J.; Ranta, V.P.; Kokki, M.; Kokki, H.; Hautajarvi, H.; Rinne, V.; Heikkinen, A.T. Physiologically based pharmacokinetic modelling of oxycodone drug-drug interactions. Biopharm. Drug Dispos. 2020, 41, 72–88. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, Y.; Boulieu, R. Contribution of CYP3A4, CYP2B6, and CYP2C9 isoforms to N-demethylation of ketamine in human liver microsomes. Drug Metab. Dispos. 2002, 30, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Eap, C.B.; Buclin, T.; Hustert, E.; Bleiber, G.; Golay, K.P.; Aubert, A.C.; Baumann, P.; Telenti, A.; Kerb, R. Pharmacokinetics of midazolam in CYP3A4- and CYP3A5-genotyped subjects. Eur. J. Clin. Pharmacol. 2004, 60, 231–236. [Google Scholar] [CrossRef] [PubMed]
- He, P.; Court, M.H.; Greenblatt, D.J.; Von Moltke, L.L. Genotype-phenotype associations of cytochrome P450 3A4 and 3A5 polymorphism with midazolam clearance in vivo. Clin. Pharmacol. Ther. 2005, 77, 373–387. [Google Scholar] [CrossRef]
- Elens, L.; Nieuweboer, A.J.; Clarke, S.J.; Charles, K.A.; de Graan, A.J.; Haufroid, V.; van Gelder, T.; Mathijssen, R.H.; van Schaik, R.H. Impact of POR*28 on the clinical pharmacokinetics of CYP3A phenotyping probes midazolam and erythromycin. Pharmacogenet Genom. 2013, 23, 148–155. [Google Scholar] [CrossRef]
- Berger, B.; Kaufmann, P.; Koch, A.; Dingemanse, J. Impact of the Selective Orexin-1 Receptor Antagonist ACT-539313 on the Pharmacokinetics of the CYP3A Probe Drug Midazolam in Healthy Male Subjects. J. Clin. Pharmacol. 2020, 60, 931–941. [Google Scholar] [CrossRef]
- Kaplan, J.C.; Hamroun, D. The 2016 version of the gene table of monogenic neuromuscular disorders (nuclear genome). Neuromuscul. Disord. 2015, 25, 991–1020. [Google Scholar] [CrossRef] [PubMed]
- Ronnblom, A.; Danielsson, A. Hereditary muscular diseases and symptoms from the gastrointestinal tract. Scand J. Gastroenterol. 2004, 39, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Van den Bersselaar, L.R.; Heytens, L.; Silva, H.C.A.; Reimann, J.; Tasca, G.; Diaz-Cambronero, O.; Lokken, N.; Hellblom, A.; Hopkins, P.M.; Rueffert, H.; et al. European Neuromuscular Centre consensus statement on anaesthesia in patients with neuromuscular disorders. Eur. J. Neurol. 2022, 29, 3486–3507. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Bonnemann, C.G.; Muntoni, F. Muscular dystrophies. Lancet 2019, 394, 2025–2038. [Google Scholar] [CrossRef] [PubMed]
- Litman, R.S.; Griggs, S.M.; Dowling, J.J.; Riazi, S. Malignant Hyperthermia Susceptibility and Related Diseases. Anesthesiology 2018, 128, 159–167. [Google Scholar] [CrossRef]
- Sheikh, S.; Alvi, U.; Soliven, B.; Rezania, K. Drugs That Induce or Cause Deterioration of Myasthenia Gravis: An Update. J. Clin. Med. 2021, 10, 1537. [Google Scholar] [CrossRef]
- Gummi, R.R.; Kukulka, N.A.; Deroche, C.B.; Govindarajan, R. Factors associated with acute exacerbations of myasthenia gravis. Muscle Nerve 2019, 60, 693–699. [Google Scholar] [CrossRef]
- Sieb, J.P. Fluoroquinolone antibiotics block neuromuscular transmission. Neurology 1998, 50, 804–807. [Google Scholar] [CrossRef]
- Warner, W.A.; Sanders, E. Neuromuscular Blockade Associated With Gentamicin Therapy. JAMA 1971, 215, 1153–1154. [Google Scholar] [CrossRef]
- Hall, D.R.; McGibbon, D.H.; Evans, C.C.; Meadows, G.A. Gentamicin, tubocurarine, lignocaine and neuromuscular blockade. A case report. Br. J. Anaesth. 1972, 44, 1329–1332. [Google Scholar] [CrossRef]
- Smith, H.; Lerner, P.I.; Weinstein, L. Neurotoxicity and “massive” intravenous therapy with penicillin. A study of possible predisposing factors. Arch. Intern. Med. 1967, 120, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Rubbo, J.T.; Gergis, S.D.; Sokoll, M.D. Comparative neuromuscular effects of lincomycin and clindamycin. Anesth. Analg. 1977, 56, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Myint, T.; Evans, M.E.; Burgess, D.R.; Greenberg, R.N. Respiratory Muscle Paralysis Associated With Colistin, Polymyxin B, and Muscle Relaxants Drugs: A Case Report. J. Investig. Med. High Impact. Case Rep. 2016, 4, 2324709616638362. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, F.; Krampfl, K.; Haeseler, G.; Dengler, R.; Bufler, J. Competitive and open channel block of recombinant nAChR channels by different antibiotics. Neuromuscul. Disord. 2004, 14, 307–312. [Google Scholar] [CrossRef]
- Renton, A.E.; Pliner, H.A.; Provenzano, C.; Evoli, A.; Ricciardi, R.; Nalls, M.A.; Marangi, G.; Abramzon, Y.; Arepalli, S.; Chong, S.; et al. A genome-wide association study of myasthenia gravis. JAMA Neurol. 2015, 72, 396–404. [Google Scholar] [CrossRef]
- Truong, T.M.; Apfelbaum, J.; Shahul, S.; Anitescu, M.; Danahey, K.; Knoebel, R.W.; Liebovitz, D.; Karrison, T.; van Wijk, X.M.R.; Yeo, K.J.; et al. The ImPreSS Trial: Implementation of Point-of-Care Pharmacogenomic Decision Support in Perioperative Care. Clin. Pharmacol. Ther. 2019, 106, 1179–1183. [Google Scholar] [CrossRef]
- Mestek-Boukhibar, L.; Clement, E.; Jones, W.D.; Drury, S.; Ocaka, L.; Gagunashvili, A.; Le Quesne Stabej, P.; Bacchelli, C.; Jani, N.; Rahman, S.; et al. Rapid Paediatric Sequencing (RaPS): Comprehensive real-life workflow for rapid diagnosis of critically ill children. J. Med. Genet. 2018, 55, 721–728. [Google Scholar] [CrossRef]
- Lehmann, T.; Rose, D.; Ranjbar, E.; Ghasri-Khouzani, M.; Tavakoli, M.; Henein, H.; Wolfe, T.; Jawad Qureshi, A. Large-scale metal additive manufacturing: A holistic review of the state of the art and challenges. Int. Mater. Rev. 2021, 67, 410–459. [Google Scholar] [CrossRef]
- Ngo, T.D.; Kashani, A.; Imbalzano, G.; Nguyen, K.T.Q.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. Part B Eng. 2018, 143, 172–196. [Google Scholar] [CrossRef]
- Han, M.; Portnova, A.A.; Lester, M.; Johnson, M. A do-it-yourself 3D-printed thoracic spine model for anesthesia resident simulation. PLoS ONE 2020, 15, e0228665. [Google Scholar] [CrossRef]
- Sherwood, J.K.; Riley, S.L.; Palazzolo, R.; Brown, S.C.; Monkhouse, D.C.; Coates, M.; Griffith, L.G.; Landeen, L.K.; Ratcliffe, A. A three-dimensional osteochondral composite scaffold for articular cartilage repair. Biomaterials 2002, 23, 4739–4751. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, D.; Matsumoto, K.; Tsuchiya, T.; Machino, R.; Takeoka, Y.; Elgalad, A.; Gunge, K.; Takagi, K.; Taura, Y.; Hatachi, G.; et al. Scaffold-free trachea regeneration by tissue engineering with bio-3D printing. Interact. Cardiovasc. Thorac. Surg. 2018, 26, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Paunovic, N.; Bao, Y.; Coulter, F.B.; Masania, K.; Geks, A.K.; Klein, K.; Rafsanjani, A.; Cadalbert, J.; Kronen, P.W.; Kleger, N.; et al. Digital light 3D printing of customized bioresorbable airway stents with elastomeric properties. Sci. Adv. 2021, 7, eabe9499. [Google Scholar] [CrossRef]
- Carter, J.C.; Broadbent, J.; Murphy, E.C.; Guy, B.; Baguley, K.E.; Young, J. A three-dimensional (3D) printed paediatric trachea for airway management training. Anaesth. Intensiv. Care 2020, 48, 243–245. [Google Scholar] [CrossRef]
- Russotto, V.; Myatra, S.N.; Laffey, J.G.; Tassistro, E.; Antolini, L.; Bauer, P.; Lascarrou, J.B.; Szuldrzynski, K.; Camporota, L.; Pelosi, P.; et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. JAMA 2021, 325, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Weatherall, A.D.; Rogerson, M.D.; Quayle, M.R.; Cooper, M.G.; McMenamin, P.G.; Adams, J.W. A Novel 3-Dimensional Printing Fabrication Approach for the Production of Pediatric Airway Models. Anesth. Analg. 2021, 133, 1251–1259. [Google Scholar] [CrossRef]
- Park, S.; Ahn, J.; Yoon, S.U.; Choo, K.S.; Kim, H.J.; Chung, M.; Kim, H.Y. Prediction of endotracheal tube size using a printed three-dimensional airway model in pediatric patients with congenital heart disease: A prospective, single-center, single-group study. Korean J. Anesthesiol. 2021, 74, 333–341. [Google Scholar] [CrossRef]
- Chebib, E.; Lemarteleur, V.; Azale, M.; Deneufbourg, L.; Ceccaldi, P.F.; Teissier, N. Step-by-step development and evaluation of a 3D printed home-made low-cost pediatric tracheobronchial tree for foreign body aspiration extractions. Int. J. Pediatr. Otorhinolaryngol. 2022, 153, 111040. [Google Scholar] [CrossRef]
- Ock, J.; Gwon, E.; Kim, D.H.; Kim, S.H.; Kim, N. Patient-specific and hyper-realistic phantom for an intubation simulator with a replaceable difficult airway of a toddler using 3D printing. Sci. Rep. 2020, 10, 10631. [Google Scholar] [CrossRef]
- Gauger, V.T.; Rooney, D.; Kovatch, K.J.; Richey, L.; Powell, A.; Berhe, H.; Zopf, D.A. A multidisciplinary international collaborative implementing low cost, high fidelity 3D printed airway models to enhance Ethiopian anesthesia resident emergency cricothyroidotomy skills. Int. J. Pediatr. Otorhinolaryngol. 2018, 114, 124–128. [Google Scholar] [CrossRef]
- Bortman, J.; Baribeau, Y.; Jeganathan, J.; Amador, Y.; Mahmood, F.; Shnider, M.; Ahmed, M.; Hess, P.; Matyal, R. Improving Clinical Proficiency Using a 3-Dimensionally Printed and Patient-Specific Thoracic Spine Model as a Haptic Task Trainer. Reg. Anesth. Pain Med. 2018, 43, 819–824. [Google Scholar] [CrossRef]
- Pang, G.; Futter, C.; Pincus, J.; Dhanani, J.; Laupland, K.B. Development and testing of a low cost simulation manikin for extracorporeal cardiopulmonary resuscitation (ECPR) using 3-dimensional printing. Resuscitation 2020, 149, 24–29. [Google Scholar] [CrossRef]
- Shaylor, R.; Verenkin, V.; Golden, E.; Matot, I. The use of three-dimensional printing and virtual reality to develop a personalised airway plan in a 7.5-year-old child: A case report. Eur. J. Anaesthesiol. 2020, 37, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Jundt, J.S.; Chow, C.C.; Couey, M. Computed tomography-guided 3D printed patient-specific regional anesthesia. J. Dent. Anesth. Pain Med. 2020, 20, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Long, D.R.; Doney, A.; Bartels, D.L.; Tan, C.E.; Sayal, P.K.; Anderson, T.A.; Agarwala, A.V. Anesthesia Workspace Cleanliness and Safety: Implementation of a Novel Syringe Bracket Using 3D Printing Techniques. Anesthesiol. Res. Pract. 2019, 2019, 2673781. [Google Scholar] [CrossRef] [PubMed]
- Dinsmore, M.; Doshi, S.; Sin, V.; Matava, C. Design and evaluation of a novel and sustainable human-powered low-cost 3D printed thermal laryngoscope. J. Med. Syst. 2019, 43, 143. [Google Scholar] [CrossRef]
- Clarke, A.L. 3D printed circuit splitter and flow restriction devices for multiple patient lung ventilation using one anaesthesia workstation or ventilator. Anaesthesia 2020, 75, 819–820. [Google Scholar] [CrossRef]


| Drug Classification | Representative Drugs | CYP450 Metabolizing Enzymes [108,109,110,111,112,113] | Other Special Genes | |
|---|---|---|---|---|
| Related Genes | Related Variant Subtypes | |||
| Local anesthetics | Lidocaine Ropivacaine | CYP1A2 CYP3A4 CYP3A5 | CYP1A2 a: Thr83Met, lu168Gln, Phe186Leu, Ser212Cys, Gly299Ala, hr438Ile [114] | SCN5A b [115] MC1R c [116] |
| Benzodiazepines | Midazolam Diazepam | CYP2C19 CYP3A4 CYP3A5 | CYP2C19 *2/*3/*17 CYP3A4 *1B CYP3A5 *1/*3/*6/*7 | - |
| Inhalation of narcotics | Halothane Sevoflurane Isoflurane | CYP2E1 | CYP2E1 *1A/*5B/*6/*7B | RYR1 d [117] MC1R [118] |
| Opioid analgesics | Fentanyl | CYP2D6 | CYP2D6 1/*2/*3/*4/*5/*6/*10/*17/*35/*41 [119] CYP3A4 *1/*1G CYP3A5 *1/*3 [120] CYP2B6 *6 | COMTb e [121] UGTb f [122] ABCB1b g OPRM1b h [123] OPRK1b i MDR1 [124] |
| Codeine | CYP2B6 | |||
| Morphine | CYP3A4 | |||
| Tramadol | CYP3A5 CYP1C2 CYP1D2 CYP2B11 CYP2C41 CYP2D2 CYP2D15 [125,126] | |||
| Intravenous anesthetics | Propofol | CYP2B6 CYP2C9 | CYP2B6 *4/*6 CYP2C9 *2 | UGT1A9 [111] GABA [127] |
| Non-steroidal anti-inflammatory drugs | Aspirin Celecoxib | CYP2C8 CYP2C9 | CYP2C8 *1/*2/*3 CYP2C9 *1/*2/*3 | PTGS1 PTGS2 j [128] |
| Neuromuscular blocking drugs | Succinylcholine Vecuronium-Bromide Rocuronium | CYP3A4 CYP2C19 | - | BCHE k [129] SLCO1B1 ABCB1 [115] RYR1 nAChR l [130] |
| Anticoagulants | Warfarin Clopidogrel | CYP2C9 CYP2C19 | CYP2C9 *1/*2/*3 CYP2C19 *1/*2/*3/*9/*12/*14/*17 [130] | VKORC1 m [131] |
| Antiemetic | Tropisetron Granisetron | CYP2D6 CYP3A4 | CYP2D6 *1/*2/*3/*4/*5/*6/*9/*41 | 5-HT3B [132] ABCB1 SLC22A1 n |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, S.; Luo, Q.; Wen, C.; Zhang, Y.; Liu, L.; Liu, L.; Liu, S.; Chen, C.; Lei, Q.; Zeng, S. Application of Advanced Technologies—Nanotechnology, Genomics Technology, and 3D Printing Technology—In Precision Anesthesia: A Comprehensive Narrative Review. Pharmaceutics 2023, 15, 2289. https://doi.org/10.3390/pharmaceutics15092289
Gu S, Luo Q, Wen C, Zhang Y, Liu L, Liu L, Liu S, Chen C, Lei Q, Zeng S. Application of Advanced Technologies—Nanotechnology, Genomics Technology, and 3D Printing Technology—In Precision Anesthesia: A Comprehensive Narrative Review. Pharmaceutics. 2023; 15(9):2289. https://doi.org/10.3390/pharmaceutics15092289
Chicago/Turabian StyleGu, Shiyao, Qingyong Luo, Cen Wen, Yu Zhang, Li Liu, Liu Liu, Su Liu, Chunhua Chen, Qian Lei, and Si Zeng. 2023. "Application of Advanced Technologies—Nanotechnology, Genomics Technology, and 3D Printing Technology—In Precision Anesthesia: A Comprehensive Narrative Review" Pharmaceutics 15, no. 9: 2289. https://doi.org/10.3390/pharmaceutics15092289
APA StyleGu, S., Luo, Q., Wen, C., Zhang, Y., Liu, L., Liu, L., Liu, S., Chen, C., Lei, Q., & Zeng, S. (2023). Application of Advanced Technologies—Nanotechnology, Genomics Technology, and 3D Printing Technology—In Precision Anesthesia: A Comprehensive Narrative Review. Pharmaceutics, 15(9), 2289. https://doi.org/10.3390/pharmaceutics15092289