
Spatial and Temporal Gait Characteristics in Patients Admitted to a Neuro-Rehabilitation Department with Age-Related White Matter Changes: A Gait Analysis and Clinical Study

 ,
,  ,
,
Abstract
:1. Introduction
Aims of the Study
2. Materials and Methods
2.1. Patients and Controls
2.2. Neuroimaging Data
2.3. Clinical and Functional Assessments
2.4. Gait Analysis
2.5. Statistical Analysis
3. Results
3.1. Sociodemographic Data
3.2. Clinical and Functional Data
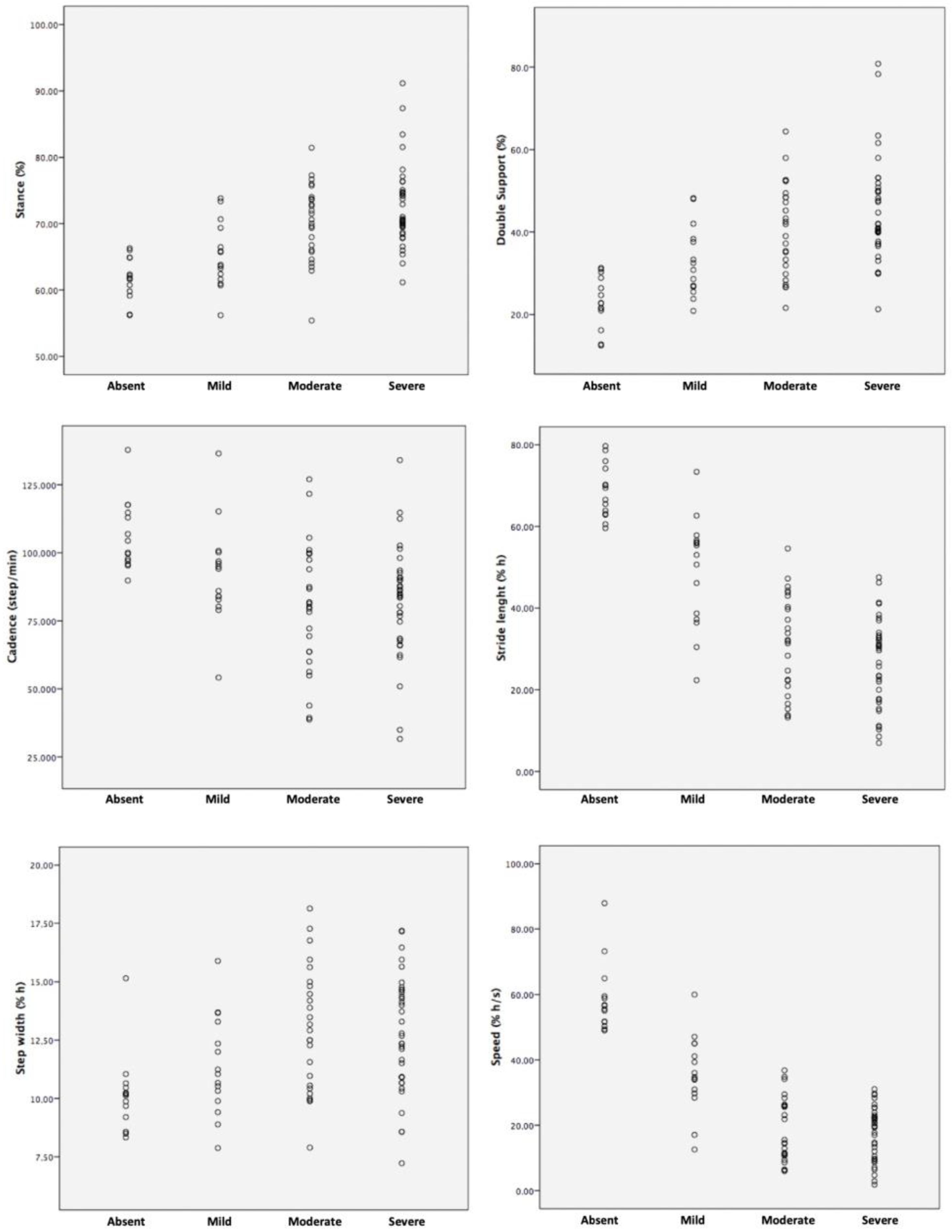
3.3. Gait Analysis Data
3.4. Correlation and Regression Model of the Gait with the Clinical-Radiological Data
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bloem, B.R.; Haan, J.; Lagaay, A.M.; Van Beek, W.; Wintzen, A.R.; Roos, R.A.C. Investigation of gait in elderly subjects over 88 years of age. J. Geriatr. Psychiatry Neurol. 1992, 5, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Sudarsky, L. Gait disorders: Prevalence, morbidity, and etiology. Adv. Neurol. 2001, 87, 111–117. [Google Scholar] [PubMed]
- Verghese, J.; LeValley, A.; Hall, C.B.; Katz, M.J.; Ambrose, A.F.; Lipton, R.B. Epidemiology of gait disorders in community-residing older adults. J. Am. Geriatr. Soc. 2006, 54, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Brach, J.S.; VanSwearingen, J.M. Interventions to Improve Walking in Older Adults. Curr. Transl. Geriatr. Exp. Gerontol. Rep. 2013, 2, 230–238. [Google Scholar] [CrossRef]
- Oh-Park, M. Interplay Between Cognition and Mobility in Older Adults. Ann. Geriatr. Med. Res. 2017, 21, 2–9. [Google Scholar] [CrossRef]
- Inzitari, D.; Carlucci, G.; Pantoni, L. White matter changes: The clinical consequences in the aging population. J. Neural. Transm. Suppl. 2000, 59, 1–8. [Google Scholar]
- Erkinjuntti, T.; Pantoni, L.; Scheltens, P. Cooperation and networking on white matter disorders: The European Task Force on Age-Related White Matter Changes. Dement. Geriatr. Cogn. Disord. 1998, 9 (Suppl. S1), 44–45. [Google Scholar] [CrossRef]
- Pugh, K.G.; Lipsitz, L.A. The microvascular frontal-subcortical syndrome of aging. Neurobiol. Aging. 2002, 23, 421–431. [Google Scholar] [CrossRef]
- Guerini, F.; Frisoni, G.B.; Marrè, A.; Turco, R.; Bellelli, G.; Trabucchi, M. Subcortical vascular lesions predict falls at 12 months in elderly patients discharged from a rehabilitation ward. Arch. Phys. Med. Rehabil. 2008, 89, 1522–1527. [Google Scholar] [CrossRef]
- Gillain, S.; Petermans, J. Contribution of new techniques to study the gait in old populations. Ann. Phys. Rehabil. Med. 2013, 56, 384–395. [Google Scholar] [CrossRef]
- Kohama, S.G.; Rosene, D.L.; Sherman, L.S. Age-related changes in human and non-human primate white matter: From myelination disturbances to cognitive decline. Age 2012, 34, 1093–1110. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Yang, Y.; Xia, Y.; Zhu, W.; Leak, R.K.; Wei, Z.; Wang, J.; Hu, X. Aging of cerebral white matter. Ageing Res. Rev. 2017, 34, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Masdeu, J.C.; Wolfson, L.; Lantos, G.; Tobin, J.N.; Grober, E.; Whipple, R.; Amerman, P. Brain white-matter changes in the elderly prone to falling. Arch. Neurol. 1989, 46, 1292–1296. [Google Scholar] [CrossRef]
- Baloh, R.W.; Yue, Q.; Socotch, T.M.; Jacobson, K.M. White matter lesions and disequilibrium in older people. I. Case-control comparison. Arch. Neurol. 1995, 52, 970–974. [Google Scholar] [CrossRef] [PubMed]
- Mortaza, N.; Abu Osman, N.A.; Mehdikhani, N. Are the spatio-temporal parameters of gait capable of distinguishing a faller from a non-faller elderly? Eur. J. Phys. Rehabil. Med. 2014, 50, 677–691. [Google Scholar]
- Mehmet, H.; Robinson, S.R.; Yang, A.W.H. Assessment of Gait Speed in Older Adults. J. Geriatr. Phys. Ther. 2020, 43, 42–52. [Google Scholar] [CrossRef]
- Bäzner, H.; Oster, M.; Daffertshofer, M.; Hennerici, M. Assessment of gait in subcortical vascular encephalopathy by computerized analysis: A cross-sectional and longitudinal study. J. Neurol. 2000, 247, 841–849. [Google Scholar] [CrossRef]
- Rosano, C.; Brach, J.; Longstreth, W.T.; Newman, A.B. Quantitative measures of gait characteristics indicate prevalence of underlying subclinical structural brain abnormalities in high-functioning older adults. Neuroepidemiology 2006, 26, 52–60. [Google Scholar] [CrossRef]
- Iseki, K.; Hanakawa, T.; Hashikawa, K.; Tomimoto, H.; Nankaku, M.; Yamauchi, H.; Hallett, M.; Fukuyama, H. Gait disturbance associated with white matter changes: A gait analysis and blood flow study. Neuroimage 2010, 49, 1659–1666. [Google Scholar] [CrossRef]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Brink, T.L.; Yesavage, J.A.; Lum, O.; Heersema, P.H.; Adey, M.; Rose, T.L. Screening Tests for Geriatric Depression. Clin. Gerontol. 2008, 1, 37–43. [Google Scholar] [CrossRef]
- WorldCat.org. Guide for the Uniform Data Set for Medical Rehabilitation: (Including the FIM Instrument), Version 5.1. Available online: https://www.worldcat.org/it/title/guide-for-the-uniform-data-set-for-medical-rehabilitation-including-the-fim-instrument-version-51/oclc/855362391 (accessed on 15 May 2023).
- Nevitt, M.C.; Cummings, S.R.; Hudes, E.S. Risk factors for injurious falls: A prospective study. J. Gerontol. 1991, 46, M164–M170. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 2009, 41, 304–311. [Google Scholar] [CrossRef]
- Berg, K.O.; Maki, B.E.; Williams, J.I.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar]
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Onen, F.; Henry Feugeas, M.C.; De Marco, G.; Baron, G.; Ravaud, P.; Legrain, S.; Moretti, J.; Claeys, E.S.; Peretti, I.I. Cerebrospinal fluid MR dynamics and risk of falls in the elderly. J. Neuroradiol. 2005, 32, 3–9. [Google Scholar] [CrossRef]
- Onen, F.; Henry-Feugeas, M.C.; Roy, C.; Baron, G.; Ravaud, P. Mobility decline of unknown origin in mild cognitive impairment: An MRI-based clinical study of the pathogenesis. Brain Res. 2008, 1222, 79–86. [Google Scholar] [CrossRef]
- Hase, Y.; Horsburgh, K.; Ihara, M.; Kalaria, R.N. White matter degeneration in vascular and other ageing-related dementias. J. Neurochem. 2018, 144, 617–633. [Google Scholar] [CrossRef]
- Macellari, V.; Giacomozzi, C.; Saggini, R. Spatial-temporal parameters of gait: Reference data and a statistical method for normality assessment. Gait Posture 1999, 10, 171–181. [Google Scholar] [CrossRef]
- Blanc, Y.; Balmer, C.; Landis, T.; Vingerhoets, F. Temporal parameters and patterns of the foot roll over during walking: Normative data for healthy adults. Gait Posture 1999, 10, 97–108. [Google Scholar] [CrossRef]
- Baezner, H.; Blahak, C.; Poggesi, A.; Pantoni, L.; Inzitari, D.; Chabriat, H.; Erkinjuntti, T.; Fazekas, F.; Ferro, J.M.; Langhorne, P.; et al. Association of gait and balance disorders with age-related white matter changes: The LADIS study. Neurology 2008, 70, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Blahak, C.; Baezner, H.; Pantoni, L.; Poggesi, A.; Chabriat, H.; Erkinjuntti, T.; Fazekas, F.; Ferro, J.M.; Langhorne, P.; O’Brien, J.; et al. Deep frontal and periventricular age related white matter changes but not basal ganglia and infratentorial hyperintensities are associated with falls: Cross sectional results from the LADIS study. J. Neurol. Neurosurg. Psychiatry 2009, 80, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Inzitari, D.; Simoni, M.; Pracucci, G.; Poggesi, A.; Basile, A.M.; Chabriat, H.; Erkinjuntti, T.; Fazekas, F.; Ferro, J.M.; Hennerici, M.; et al. Risk of rapid global functional decline in elderly patients with severe cerebral age-related white matter changes: The LADIS study. Arch. Intern. Med. 2007, 167, 81–88. [Google Scholar] [CrossRef]
- Inzitari, D.; Pracucci, G.; Poggesi, A.; Carlucci, G.; Barkhof, F.; Chabriat, H.; Erkinjuntti, T.; Fazekas, F.; Ferro, J.M.; Hennerici, M.; et al. Changes in white matter as determinant of global functional decline in older independent outpatients: Three year follow-up of LADIS (leukoaraiosis and disability) study cohort. BMJ 2009, 339, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.W.; Chao, W.H.; Lin, S.H.; Chen, Y.Y. A vision-based analysis system for gait recognition in patients with Parkinson’s disease. Expert Syst. Appl. 2009, 36, 7033–7039. [Google Scholar] [CrossRef]
- Tzallas, A.T.; Tsipouras, M.G.; Rigas, G.; Tsalikakis, D.G.; Karvounis, E.C.; Chondrogiorgi, M.; Psomadellis, F.; Cancela, J.; Pastorino, M.; Waldmeyer, M.T.A.; et al. PERFORM: A system for monitoring, assessment and management of patients with Parkinson’s disease. Sensors 2014, 14, 21329–21357. [Google Scholar] [CrossRef] [PubMed]
- Lauraitis, A.; Maskeliunas, R.; Damasevicius, R.; Polap, D.; Wozniak, M. A Smartphone Application for Automated Decision Support in Cognitive Task Based Evaluation of Central Nervous System Motor Disorders. IEEE J. Biomed. Health Inform. 2019, 23, 1865–1876. [Google Scholar] [CrossRef] [PubMed]
- Lauraitis, A.; Maskeliūnas, R.; Damaševičius, R.; Krilavičius, T. A Mobile Application for Smart Computer-Aided Self-Administered Testing of Cognition, Speech, and Motor Impairment. Sensors 2020, 20, 3236. [Google Scholar] [CrossRef] [PubMed]
- Lauraitis, A.; Maskeliunas, R.; Damaševičius, R. ANN and Fuzzy Logic Based Model to Evaluate Huntington Disease Symptoms. J. Healthc. Eng. 2018, 2018, 4581272. [Google Scholar] [CrossRef]
- Priya, S.J.; Rani, A.J.; Subathra, M.S.P.; Mohammed, M.A.; Damaševičius, R.; Ubendran, N. Local Pattern Transformation Based Feature Extraction for Recognition of Parkinson’s Disease Based on Gait Signals. Diagnostics 2021, 11, 1395. [Google Scholar] [CrossRef]
- Rudisch, J.; Jöllenbeck, T.; Vogt, L.; Cordes, T.; Klotzbier, T.J.; Vogel, O.; Wollesen, B. Agreement and consistency of five different clinical gait analysis systems in the assessment of spatiotemporal gait parameters. Gait Posture 2021, 85, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Klöpfer-Krämer, I.; Brand, A.; Wackerle, H.; Müßig, J.; Kröger, I.; Augat, P. Gait analysis-Available platforms for outcome assessment. Injury 2020, 51 (Suppl. S2), S90–S96. [Google Scholar] [CrossRef]
- Sharif, M.I.; Khan, M.A.; Alqahtani, A.; Nazir, M.; Alsubai, S.; Binbusayyis, A.; Damaševičius, R. Deep Learning and Kurtosis-Controlled, Entropy-Based Framework for Human Gait Recognition Using Video Sequences. Electronics 2022, 11, 334. [Google Scholar] [CrossRef]
- Khan, M.A.; Arshad, H.; Damaševičius, R.; Alqahtani, A.; Alsubai, S.; Binbusayyis, A.; Nam, Y.; Kang, B.-G. Human Gait Analysis: A Sequential Framework of Lightweight Deep Learning and Improved Moth-Flame Optimization Algorithm. Comput. Intell. Neurosci. 2022, 2022, 8238375. [Google Scholar] [CrossRef]
- Sethi, D.; Bharti, S.; Prakash, C. A comprehensive survey on gait analysis: History, parameters, approaches, pose estimation, and future work. Artif. Intell. Med. 2022, 129, 102314. [Google Scholar] [CrossRef] [PubMed]
- Mündermann, L.; Corazza, S.; Andriacchi, T.P. The evolution of methods for the capture of human movement leading to markerless motion capture for biomechanical applications. J. Neuroeng. Rehabil. 2006, 3, 6. [Google Scholar] [CrossRef]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis. Expert Rev. Med. Devices 2016, 13, 641–659. [Google Scholar] [CrossRef] [PubMed]
- Sang, V.N.T.; Yano, S.; Kondo, T. On-Body Sensor Positions Hierarchical Classification. Sensors 2018, 18, 3612. [Google Scholar] [CrossRef]
- Ormel, J.; Rijsdijk, F.V.; Sullivan, M.; Van Sonderen, E.; Kempen, G.I.J.M. Temporal and reciprocal relationship between IADL/ADL disability and depressive symptoms in late life. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, P338–P347. [Google Scholar] [CrossRef]
- Teodorczuk, A.; Firbank, M.J.; Pantoni, L.; Poggesi, A.; Erkinjuntti, T.; Wallin, A.; Wahlund, L.-O.; Scheltens, P.; Waldemar, G.; Schrotter, G.; et al. Relationship between baseline white-matter changes and development of late-life depressive symptoms: 3-year results from the LADIS study. Psychol. Med. 2010, 40, 603–610. [Google Scholar] [CrossRef]
- Jellinger, K.A. The enigma of vascular depression in old age: A critical update. J. Neural. Transm. 2022, 129, 961–976. [Google Scholar] [CrossRef]
- Camicioli, R.; Howieson, D.; Oken, B.; Sexton, G.; Kaye, J. Motor slowing precedes cognitive impairment in the oldest old. Neurology 1998, 50, 1496–1498. [Google Scholar] [CrossRef] [PubMed]
- Inzitari, M.; Newman, A.B.; Yaffe, K.; Boudreau, R.; de Rekeneire, N.; Shorr, R.; Harris, T.B.; Rosano, C. Gait speed predicts decline in attention and psychomotor speed in older adults: The health aging and body composition study. Neuroepidemiology 2007, 29, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; Lipton, R.B.; Hall, C.B.; Kuslansky, G.; Katz, M.J.; Buschke, H. Abnormality of gait as a predictor of non-Alzheimer’s dementia. N. Engl. J. Med. 2002, 347, 1761–1768. [Google Scholar] [CrossRef]
- Swanson, R.; Robinson, K.M. Geriatric Rehabilitation: Gait in the Elderly, Fall Prevention and Parkinson Disease. Med. Clin. N. Am. 2020, 104, 327–343. [Google Scholar] [CrossRef]
- Keating, C.J.; Cabrera-Linares, J.C.; Párraga-Montilla, J.A.; Latorre-Román, P.A.; del Castillo, R.M.; García-Pinillos, F. Influence of Resistance Training on Gait & Balance Parameters in Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1759. [Google Scholar]
- Zhong, H.H.; Yu, B.; Luo, D.; Yang, L.Y.; Zhang, J.; Jiang, S.S.; Hu, S.J.; Luo, Y.Y.; Yang, M.W.; Hong, F.F.; et al. Roles of aging in sleep. Neurosci. Biobehav. Rev. 2019, 98, 177–184. [Google Scholar] [CrossRef]
- Yaffe, K.; Nasrallah, I.; Hoang, T.D.; Lauderdale, D.S.; Knutson, K.L.; Carnethon, M.R.; Launer, L.J.; Lewis, C.E.; Sidney, S. Sleep Duration and White Matter Quality in Middle-Aged Adults. Sleep 2016, 39, 1743–1747. [Google Scholar] [CrossRef] [PubMed]
- Sexton, C.E.; Zsoldos, E.; Filippini, N.; Griffanti, L.; Winkler, A.; Mahmood, A.; Allan, C.L.; Topiwala, A.; Kyle, S.D.; Spiegelhalder, K.; et al. Associations between self-reported sleep quality and white matter in community-dwelling older adults: A prospective cohort study. Hum. Brain Mapp. 2017, 38, 5465–5473. [Google Scholar] [CrossRef]
- Brown, R.E.; Basheer, R.; McKenna, J.T.; Strecker, R.E.; McCarley, R.W. Control of sleep and wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef]
- Buchmann, A.; Kurth, S.; Ringli, M.; Geiger, A.; Jenni, O.G.; Huber, R. Anatomical markers of sleep slow wave activity derived from structural magnetic resonance images. J. Sleep Res. 2011, 20, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Dubé, J.; Lafortune, M.; Bedetti, C.; Bouchard, M.; Gagnon, J.F.; Doyon, J.; Evans, A.C.; Lina, J.-M.; Carrier, J. Cortical thinning explains changes in sleep slow waves during adulthood. J. Neurosci. 2015, 35, 7795–7807. [Google Scholar] [CrossRef] [PubMed]
- Neske, G.T. The Slow Oscillation in Cortical and Thalamic Networks: Mechanisms and Functions. Front. Neural Circuits 2016, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Bells, S.; Lefebvre, J.; Longoni, G.; Narayanan, S.; Arnold, D.L.; Yeh, E.A.; Mabbott, D.J. White matter plasticity and maturation in human cognition. Glia 2019, 67, 2020–2037. [Google Scholar] [CrossRef]
- Gouw, A.A.; Van Der Flier, W.M.; Van Straaten, E.C.W.; Pantoni, L.; Bastos-Leite, A.J.; Inzitari, D.; Erkinjuntti, T.; Wahlund, L.O.; Ryberg, C.; Schmidt, R.; et al. Reliability and sensitivity of visual scales versus volumetry for evaluating white matter hyperintensity progression. Cerebrovasc. Dis. 2008, 25, 247–253. [Google Scholar] [CrossRef]
- Madureira, S.; Verdelho, A.; Moleiro, C.; Ferro, J.M.; Erkinjuntti, T.; Jokinen, H.; Pantoni, L.; Fazekas, F.; Van der Flier, W.; Visser, M.; et al. Neuropsychological predictors of dementia in a three-year follow-up period: Data from the LADIS study. Dement. Geriatr. Cogn. Disord. 2010, 29, 325–334. [Google Scholar] [CrossRef]


{kind=link}
| Demographic and Anthropometric Data | Controls (n = 14) | Mild ARWMC (n = 15) | Moderate ARWMC (n = 25) | Severe ARWMC (n = 36) | Tot Pat (n = 76) | F | p (ANOVA) |
|---|---|---|---|---|---|---|---|
| Age (years) | 75.8 ±5 | 76.6 ± 5.5 | 79 ± 6.1 | 78 ± 6.6 | 78.3 ± 6.2 | 1.1 | 0.324 |
| Sex (males. females) | 6M, 8F | 9M, 6F | 14M, 11F | 25M, 11 F | 48M, 28F | 1.0 | 0.369 |
| Weight (kg) | 63.8 ± 5.8 | 74.9 ± 15.5 * | 68.1 ± 14.4 | 69.3 ± 15.5 | 70 ± 15.1 | 1.5 | 0.208 |
| Height (cm) | 162.3 ± 7 | 164.8 ± 10.2 | 165 ± 11.2 | 163 ± 10.5 | 164.4 ± 10.6 | 0.2 | 0.876 |
| Gait parameters | |||||||
| Stance (%) | 61.7 ± 3.1 | 65.1 ± 4.9 * | 70.1 ± 5.7 # ° | 72.6 ± 6.2 § | 70.3 ± 6.3 | 16.1 | <0.0001 |
| Double Support (%) | 23.1 ± 6.2 | 32.6 ± 8.5 * | 40.7 ± 11.1 # ° | 45.0 ± 12.4 § | 42.2 ± 12 | 15.8 | <0.0001 |
| Cadence (step/min) | 106.2 ± 12.7 | 92.3 ± 18.3 | 79.3 ± 23.6 ° | 82 ± 20.1 | 83.1 ± 21.2 | 6.6 | <0.0001 |
| Swing speed (m/s) | 2.27 ± 0.41 | 1.55 ± 0.38 * | 0.95 ± 0.36 # ° | 0.93 ± 0.34 § | 1.0 ± 0.4 | 54.0 | <0.0001 |
| Swing speed (%h/s) | 140.2 ± 24.0 | 94.3 ± 22.3 * | 57.8 ± 21.1 # ° | 57.1 ± 20.2 § | 64.7 ± 25.4 | 60.7 | <0.0001 |
| Stride (m) | 1.11 ± 0.11 | 0.8 ± 0.23 * | 0.51 ± 0.21 # ° | 0.43 ± 0.18 § | 0.53 ± 0.24 | 48.5 | <0.0001 |
| Stride (%h) | 68.6 ± 6.5 | 48.8 ± 13.4 * | 30.7 ± 12.1 # ° | 26.7 ± 10.7 § | 32.4 ± 14.3 | 55.5 | <0.0001 |
| Step width (m) | 0.16 ± 0.02 | 0.18 ± 0.03 | 0.21 ± 0.04 # ° | 0.20 ± 0.04 | 0.20 ± 0.04 | 6 | 0.001 |
| Step width (%h) | 10.1 ± 1.6 | 11.3 ± 2.1 | 12.9 ± 2.6 # ° | 12.6 ± 2.4 | 12.5 ± 2.5 | 5.4 | 0.002 |
| Speed (m/s) | 0.95 ± 0.18 | 0.58 ± 0.19 * | 0.30 ± 0.16 # ° | 0.28 ± 0.13 § | 0.35 ± 0.19 | 66.1 | <0.0001 |
| Speed (%h/s) | 58.6 ± 10.6 | 35.6 ± 11.7 * | 18.4 ± 9.7 # ° | 17.6 ± 8 § | 21.4 ± 11.7 | 72.1 | <0.0001 |
| Clinical Scores | |||||||
| MMSE (max = 30) | 28.4 ± 1.3 | 26 ± 3.7 | 24.7 ± 4.2 ° | 21.4 ± 6.1 + § | 23.4 ± 5.4 | 8.6 | <0.0001 |
| GDS (max = 30) | 4.8 ± 2.1 | 14.4 ± 7 * | 13.4 ± 7.7 ° | 14.6 ± 7.1 | 14.2 ± 7.2 | 7.6 | <0.0001 |
| FIM (max = 126) | 125.6 ± 0.8 | 113.2 ± 17.9 | 102.5 ± 19 ° | 91.3 ± 27.4 + § | 99.3 ± 24.5 | 9.8 | <0.0001 |
| FIM (motor scores) | 90.8 ± 0.5 | 81.9 ± 13.6 | 73.7 ± 15.6 ° | 65.8 ± 20.7 § | 74.5 ± 18.6 | 8.8 | <0.0001 |
| FIM (cognitive scores) | 34.8 ± 0.3 | 30.6 ± 5.2 | 28.8 ± 5.0 ° | 25.5 ± 8.1 + § | 28.7 ± 6.9 | 8.0 | <0.0001 |
| NMPS (max = 14) | 13.8 ± 0.5 | 9.6 ± 3.2 * | 6.2 ± 3 # ° | 5.4 ± 3 § | 6.5 ± 3.4 | 33.3 | <0.0001 |
| BBS (max = 56) | 55.8 ± 0.5 | 45.4 ± 11.2 * | 33.1 ± 14 # ° | 29.6 ± 16.2 § | 33.9 ± 15.6 | 15.2 | <0.0001 |
| Gait Parameters and Clinical Scores vs. Gait Parameters | Stance (%) | Swing (%) | Double Support (%) | Stride Time (s) | Cadence (Step/min) | Swing Speed (% h/s) | Stride (% h) | Step Width (% h) | Speed (% h/s) |
|---|---|---|---|---|---|---|---|---|---|
| Stance (%) | 1 | −0.957 ** | 0.954 ** | 0.530 ** | −0.421 ** | −0.652 ** | −0.767 ** | 0.204 | −0.767 ** |
| Swing (%) | −0.957 ** | 1 | −0.980 ** | −0.593 ** | 0.492 ** | 0.643 ** | 0.684 ** | −0.164 | 0.783 ** |
| Double Support (%) | 0.954 ** | −0.980 ** | 1 | 0.580 ** | −0.487 ** | −0.694 ** | −0.727 ** | 0.212 | −0.761 ** |
| Stride time (s) | 0.530 ** | −0.593 ** | 0.580 ** | 1 | −0.907 ** | −0.540 ** | −0.245 * | 0.07 | −0.541 ** |
| Cadence (step/min) | −0.421 ** | 0.492 ** | −0.487 ** | −0.907 ** | 1 | 0.554 ** | 0.189 | 0.023 | 0.539 ** |
| Swing speed (% h/s) | −0.652 ** | 0.643 ** | −0.694 ** | −0.540 ** | 0.554 ** | 1 | 0.853 ** | −0.256 * | 0.956 ** |
| Stride (% h) | −0.767 ** | 0.684 ** | −0.727 ** | −0.245 * | 0.189 | 0.853 ** | 1 | −0.298 ** | 0.886 ** |
| Step width (% h) | 0.204 | −0.164 | 0.212 | 0.07 | 0.023 | −0.256 * | −0.298 ** | 1 | −0.288 * |
| Speed (% h/s) | −0.767 ** | 0.743 ** | −0.783 ** | −0.541 ** | 0.539 ** | 0.956 ** | 0.886 ** | −0.288 * | 1 |
| ARWMC | 0.428 ** | −0.368 ** | 0.378 ** | 0.124 | −0.144 | −0.484 ** | −0.540 ** | 0.158 | −0.516 ** |
| MMSE | −0.269 * | 0.280 * | −0.299 * | −0.191 | 0.117 | 0.349 ** | 0.353 ** | −0.189 | 0.323 ** |
| GDS | 0.384 ** | −0.392 ** | 0.404 ** | 0.303 ** | −0.273 * | −0.334 ** | −0.317 ** | 0.091 | −0.351 ** |
| FIM | −0.350 ** | 0.345 ** | −0.388 ** | −0.201 | 0.124 | 0.452 ** | 0.481 ** | −0.21 | 0.431 ** |
| NMPS | −0.457 ** | 0.436 ** | −0.495 ** | −0.241 * | 0.196 | 0.637 ** | 0.658 ** | −0.321 ** | 0.631 ** |
| BBS | −0.392 ** | 0.391 ** | −0.445 ** | −0.320 ** | 0.272 * | 0.618 ** | 0.565 ** | −0.291 * | 0.592 ** |
| Gait Parameters and Clinical Scores vs. Clinical Scores | ARWMC | MMSE | GDS | FIM | NMPS | BBS |
|---|---|---|---|---|---|---|
| Stance (%) | 0.428 ** | −0.269 * | 0.384 ** | −0.350 ** | −0.457 ** | −0.392 ** |
| Swing (%) | −0.368 ** | 0.280 * | −0.392 ** | 0.345 ** | 0.436 ** | 0.391 ** |
| Double Support (%) | 0.378 ** | −0.299 * | 0.404 ** | −0.388 ** | −0.495 ** | −0.445 ** |
| Stride time (s) | 0.124 | −0.191 | 0.303 ** | −0.201 | −0.241 * | −0.320 ** |
| Cadence (step/min) | −0.144 | 0.117 | −0.273 * | 0.124 | 0.196 | 0.272 * |
| Swing speed (% h/s) | −0.484 ** | 0.349 ** | −0.334 ** | 0.452 ** | 0.637 ** | 0.618 ** |
| Stride (% h) | −0.540 ** | 0.353 ** | −0.317 ** | 0.481 ** | 0.658 ** | 0.565 ** |
| Step width (% h) | 0.158 | −0.189 | 0.091 | −0.21 | −0.321 ** | −0.291 * |
| Speed (% h/s) | −0.516 ** | 0.323 ** | −0.351 ** | 0.431 ** | 0.631 ** | 0.592 ** |
| ARWMC | 1 | −0.351 ** | 0.027 | −0.348 ** | −0.433 ** | −0.358 ** |
| MMSE | −0.351 ** | 1 | −0.176 | 0.602 ** | 0.528 ** | 0.496 ** |
| GDS | 0.027 | −0.176 | 1 | −0.256 * | −0.177 | −0.209 |
| FIM | −0.348 ** | 0.602 ** | −0.256 * | 1 | 0.730 ** | 0.757 ** |
| NMPS | −0.433 ** | 0.528 ** | −0.177 | 0.730 ** | 1 | 0.881 ** |
| BBS | −0.358 ** | 0.496 ** | −0.209 | 0.757 ** | 0.881 ** | 1 |
| Dependent Variables | Model Summary Values | R2 Change | Coefficients of the Independent Variables | Zero-Order Correlations | Partial Correlations |
|---|---|---|---|---|---|
| Stride (% h) Entry | R = 0.572 R2 = 0.327 | dR2 = 0.327 p = 0.000 | ARWMC = −9.28 (Age, Sex, Weight, Height p > 0.05) | −0.54 | −0.51 |
| Forward stepwise | R = 0.740 R2 = 0.547 | dR2 = 0.220 p = 0.000 | ARWMC = −5.31 NMPS = 2.21 | −0.54 0.65 | −0.35 0.57 |
| R = 0.766 R2 = 0.587 | dR2 = 0.039 p = 0.013 | ARWMC = −5.54 NMPS = 1.97 GDS = −0.42 | −0.54 0.65 −0.31 | −0.38 0.53 −0.29 | |
| Speed (%h/s) Entry | R = 0.549 R2 = 0.301 | dR2 = 0.301 p = 0.000 | Intercept = 66.9 ARWMC = −7.72 (Age, Sex, Weight, Height p > 0.05) | −0.51 | −0.51 |
| Forward stepwise | R = 0.729 R2 = 0.532 | dR2 = 0.230 p = 0.000 | Intercept = 52.6 ARWMC = −4.40 NMPS = 1.84 | −0.51 0.63 | −0.35 0.57 |
| R = 0.757 R2 = 0.573 | dR2 = 0.041 p = 0.013 | Intercept = 62.8 ARWMC = −4.59 NMPS = 1.64 GDS = −0.356 | −0.51 0.63 −0.35 | −0.38 0.53 −0.29 | |
| Double supp (%) Entry | R = 0.427 R2 = 0.182 | dR2 = 0.182 p = 0.013 | ARWMC = 6.4 (Age, Sex, Weight, Height p > 0.05) | 0.39 | 0.39 |
| Forward stepwise | R = 0.576 R2 = 0.332 | dR2 = 0.149 p = 0.000 | ARWMC = 3.5 NMPS = −1.5 | 0.39 −0.49 | 0.23 −0.42 |
| R = 0.649 R2 = 0.421 | dR2 = 0.090 p = 0.002 | ARWMC = 3.8 NMPS = −1.2 GDS = 0.55 | 0.39 −0.49 0.40 | 0.27 −0.36 0.36 |
| Dependent Variables | Model Summary Values | R2 Change | Coefficients of the Independent Variables | Zero-Order Correlations | Partial Correlations |
|---|---|---|---|---|---|
| Cadence (Step/min) Entry | R = 0.339 R2 = 0.115 | dR2 = 0.115 p = 0.120 | Intercept = 134.7 ARWMC = −5.7 (Age, Sex, Weight, Height p > 0.05) | −0.14 | −0.21 |
| Forward stepwise | R = 0.421 R2 = 0.177 | dR2 = 0.062 p = 0.026 | Intercept = 124.7 ARWMC = −3.2 BBS = 0.3 | −0.14 0.27 | −0.11 0.26 |
| Step width (%h) Entry | R = 0.332 R2 = 0.110 | dR2 = 0.110 p = 0.137 | Intercept = 25.6 ARWMC = 0.5 (Age, Sex, Weight, Height p > 0.05) | 0.15 | 0.16 |
| Forward stepwise | R = 0.430 R2 = 0.185 | dR2 = 0.114 p = 0.014 | Intercept = 27.4 ARWMC = 0.1 NMPS = −0.2 | 0.15 −0.32 | 0.03 −0.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gagliardo, A.; Grippo, A.; Di Stefano, V.; Carrai, R.; Scarpino, M.; Martini, M.; Falsini, C.; Rimmaudo, G.; Brighina, F. Spatial and Temporal Gait Characteristics in Patients Admitted to a Neuro-Rehabilitation Department with Age-Related White Matter Changes: A Gait Analysis and Clinical Study. Neurol. Int. 2023, 15, 708-724. https://doi.org/10.3390/neurolint15020044
Gagliardo A, Grippo A, Di Stefano V, Carrai R, Scarpino M, Martini M, Falsini C, Rimmaudo G, Brighina F. Spatial and Temporal Gait Characteristics in Patients Admitted to a Neuro-Rehabilitation Department with Age-Related White Matter Changes: A Gait Analysis and Clinical Study. Neurology International. 2023; 15(2):708-724. https://doi.org/10.3390/neurolint15020044
Chicago/Turabian StyleGagliardo, Andrea, Antonello Grippo, Vincenzo Di Stefano, Riccardo Carrai, Maenia Scarpino, Monica Martini, Catiuscia Falsini, Giulia Rimmaudo, and Filippo Brighina. 2023. "Spatial and Temporal Gait Characteristics in Patients Admitted to a Neuro-Rehabilitation Department with Age-Related White Matter Changes: A Gait Analysis and Clinical Study" Neurology International 15, no. 2: 708-724. https://doi.org/10.3390/neurolint15020044
APA StyleGagliardo, A., Grippo, A., Di Stefano, V., Carrai, R., Scarpino, M., Martini, M., Falsini, C., Rimmaudo, G., & Brighina, F. (2023). Spatial and Temporal Gait Characteristics in Patients Admitted to a Neuro-Rehabilitation Department with Age-Related White Matter Changes: A Gait Analysis and Clinical Study. Neurology International, 15(2), 708-724. https://doi.org/10.3390/neurolint15020044