
An Innovative Surgical Technique to Obtain an Adipose-Derived Stromal Cell-Rich Graft for the Treatment of Osteoarthritis: Technical Note

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
Highlights
- Developed a novel technique to isolate adipose-derived stromal cells for grafting;
- Optimized the procedure for minimal invasiveness and reproducibility;
- Established a basis for future clinical applications of cell-rich grafts.
- Potentially improves outcomes for osteoarthritis patients with less invasive treatment;
- Offers a new avenue for regenerative medicine applications;
- Supports future research into adipose-derived cell therapies;
- Lays the groundwork for broader clinical adoption of cell-rich fat grafting techniques.
Abstract
:1. Introduction
2. Preoperative Considerations
3. Surgical Technique
3.1. Equipment
- 500 mL 0.9% saline;
- 5 mL lidocaine 10 mg/mL (per incision);
- 20 mL mepivacaine 10 mg/mL;
- 0.7 mL 0.1% epinephrine;
- Surgical scalpel with blade no. 11;
- Sterile liposuction cannula set;
- Luer Lock 50 mL syringes × 4;
- Luer Lock 20 mL syringes × 1;
- Luer Lock 10 mL syringes × 8;
- Luer Lock 5 mL syringes × 2;
- Luer Lock Combi-stoppers × 8;
- 20-gauge syringe needles × 2;
- 15-gauge intravenous catheter;
- Three-way stopcocks × 2;
- Thermo Scientific™ MediLite™ Centrifuge (Thermo Fisher Scientific, Waltham, MA, USA) or equivalent.
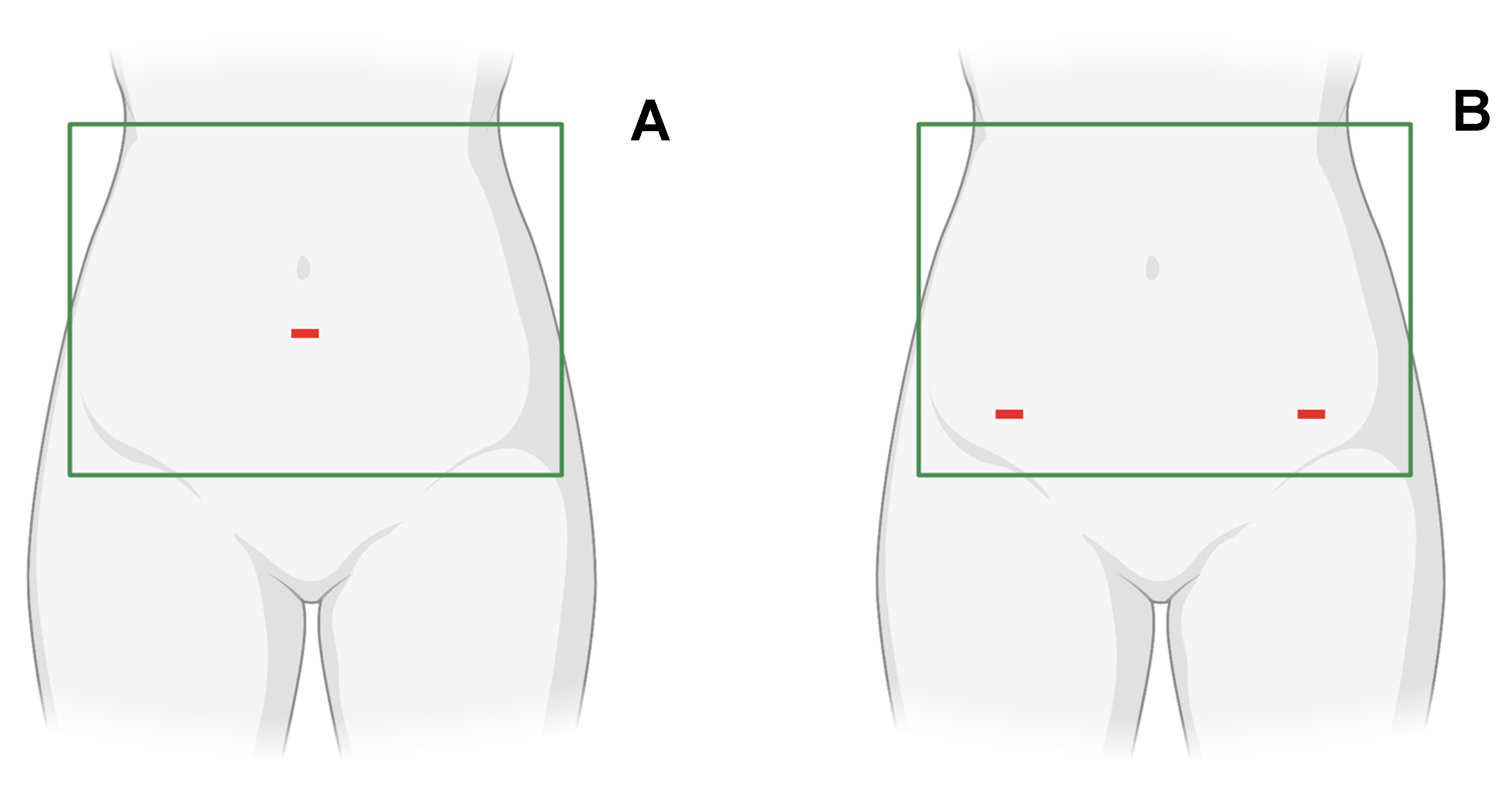
3.2. Patient Positioning and Setup
3.3. Liposuction
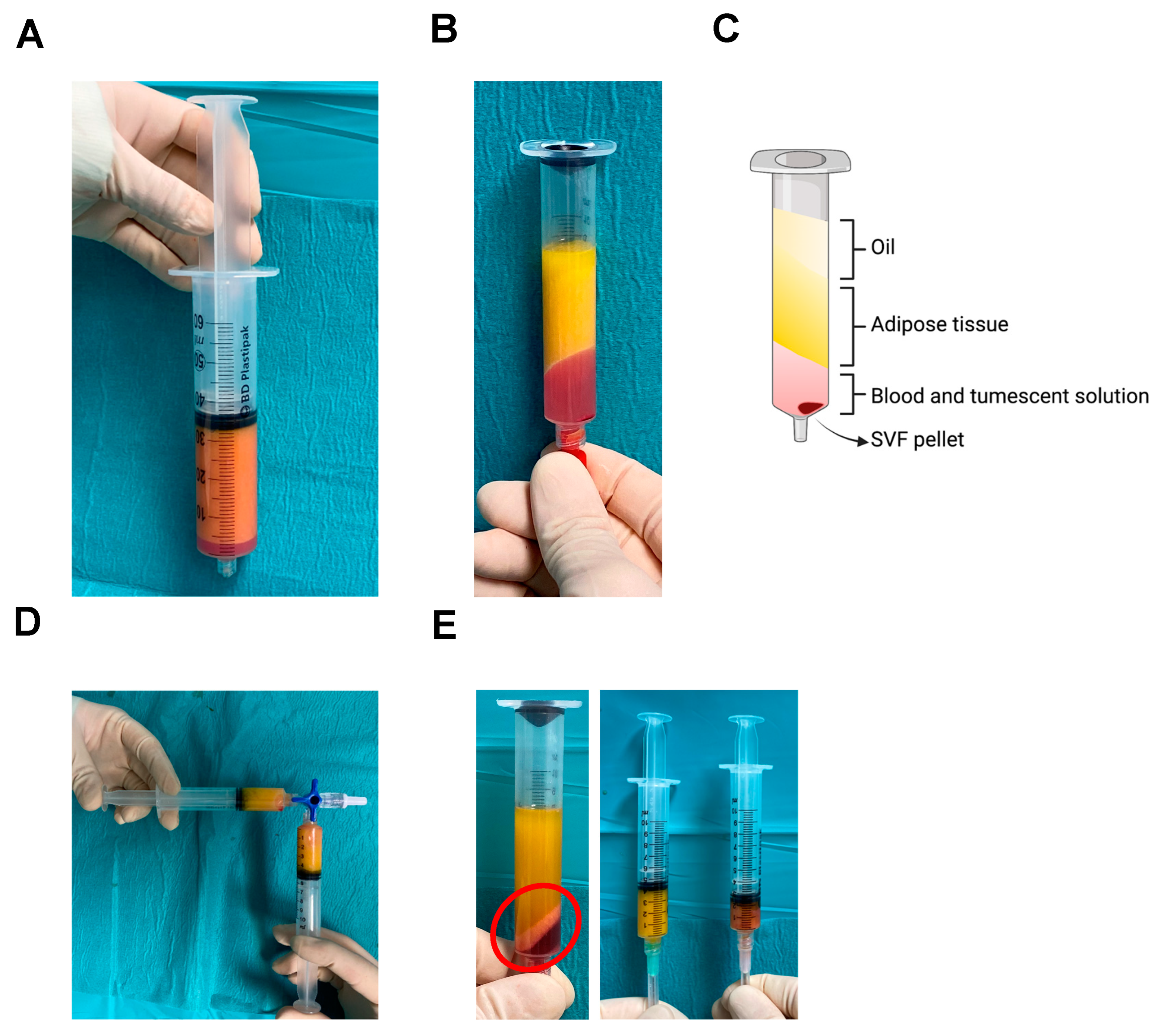
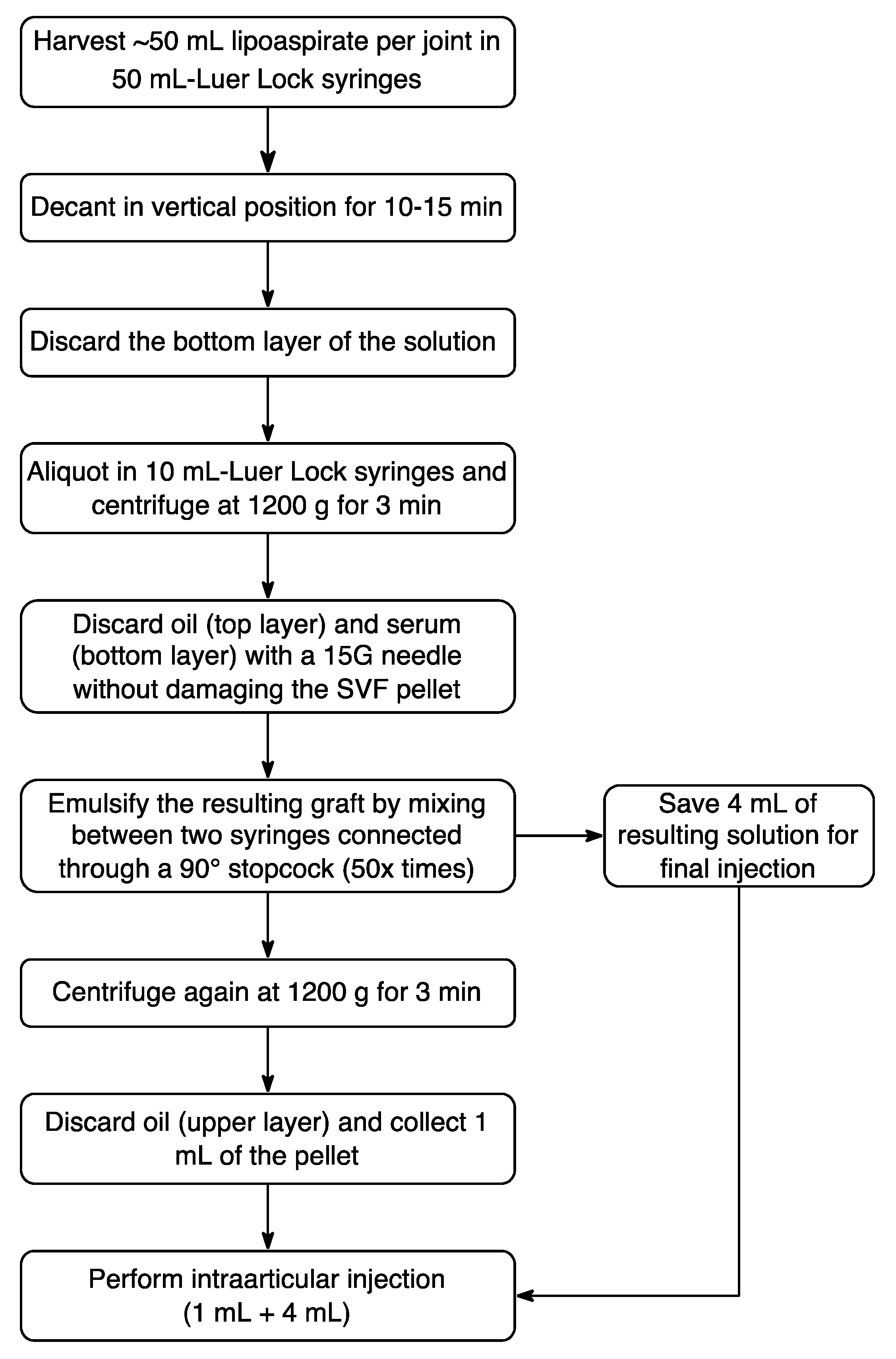
3.4. Graft Preparation
3.5. Intraarticular Injection and Post-Operative Care
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.P. Osteoarthritis. Nat. Rev. Dis. Prim. 2016, 2, 16072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glyn-Jones, S.; Palmer, A.J.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, F.; Gravina, P.; Busato, A.; Farinelli, L.; Soranzo, C.; Vidal, L.; Zingaretti, N.; Zavan, B.; Sbarbati, A.; Riccio, M.; et al. Stem Cells in Autologous Microfragmented Adipose Tissue: Current Perspectives in Osteoarthritis Disease. Int. J. Mol. Sci. 2021, 22, 10197. [Google Scholar] [CrossRef]
- Lopa, S.; Colombini, A.; Moretti, M.; de Girolamo, L. Injective mesenchymal stem cell-based treatments for knee osteoarthritis: From mechanisms of action to current clinical evidences. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 27, 2003–2020. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, A.; Guo, J.; Banyard, D.A.; Fadavi, D.; Toranto, J.D.; Wirth, G.A.; Paydar, K.Z.; Evans, G.R.D.; Widgerow, A.D. Stromal vascular fraction: A regenerative reality? Part 1: Current concepts and review of the literature. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 170–179. [Google Scholar] [CrossRef]
- Persichetti, P.; Marangi, G.F.; Segreto, F.; Pantano, F.; Tirindelli, M.C.; Gregorj, C. Adipose Tissue Purification Technique to Obtain High Concentration of Adipose Stem Cells. Patent IT201700003805A1, 2017. [Google Scholar]
- Cicione, C.; Vadalà, G.; Di Giacomo, G.; Tilotta, V.; Ambrosio, L.; Russo, F.; Zampogna, B.; Cannata, F.; Papalia, R.; Denaro, V. Micro-fragmented and nanofat adipose tissue derivatives: In vitro qualitative and quantitative analysis. Front. Bioeng. Biotechnol. 2023, 11, 911600. [Google Scholar] [CrossRef]
- Beidas, O.E.; Gusenoff, J.A. Update on Liposuction: What All Plastic Surgeons Should Know. Plast. Reconstr. Surg. 2021, 147, 658e–668e. [Google Scholar] [CrossRef]
- Strong, A.L.; Cederna, P.S.; Rubin, J.P.; Coleman, S.R.; Levi, B. The Current State of Fat Grafting. Plast. Reconstr. Surg. 2015, 136, 897–912. [Google Scholar] [CrossRef] [Green Version]
- Kaoutzanis, C.; Gupta, V.; Winocour, J.; Layliev, J.; Ramirez, R.; Grotting, J.C.; Higdon, K. Cosmetic Liposuction: Preoperative Risk Factors, Major Complication Rates, and Safety of Combined Procedures. Aesthetic Surg. J. 2017, 37, 680–694. [Google Scholar] [CrossRef] [PubMed]
- Hunstad, J.P.; Aitken, M.E. Liposuction: Techniques and Guidelines. Clin. Plast. Surg. 2006, 33, 13–25. [Google Scholar] [CrossRef]
- Kucera, I.J.; Lambert, T.J.; Klein, J.A.; Watkins, R.G.; Hoover, J.M.; Kaye, A.D. Liposuction: Contemporary issues for the anesthesiologist. J. Clin. Anesth. 2006, 18, 379–387. [Google Scholar] [CrossRef]
- Boeni, R.; Waechter-Gniadek, P.v. Safety of Tumescent Liposuction Under Local Anesthesia in 9002 Consecutive Patients. Dermatol. Surg. 2021, 47, e184–e187. [Google Scholar] [CrossRef] [PubMed]
- Toledo, L.S. Syringe liposculpture: A two-year experience. Aesthetic Plast. Surg. 1991, 15, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Tevlin, R.; desJardins-Park, H.; Huber, J.; DiIorio, S.E.; Longaker, M.T.; Wan, D.C. Musculoskeletal tissue engineering: Adipose derived stromal cell implementation for the treatment of osteoarthritis. Biomaterials 2022, 286, 121544. [Google Scholar] [CrossRef]
- Doyle, E.C.; Wragg, N.M.; Wilson, S.L. Intraarticular injection of bone marrow-derived mesenchymal stem cells enhances regeneration in knee osteoarthritis. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3827–3842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, C.; Wu, W.; Qu, X. Mesenchymal stem cells in osteoarthritis therapy: A review. Am. J. Transl. Res. 2021, 13, 448–461. [Google Scholar] [PubMed]
- Zhu, Y.; Liu, T.; Song, K.; Fan, X.; Ma, X.; Cui, Z. Adipose-derived stem cell: A better stem cell than BMSC. Cell Biochem. Funct. 2008, 26, 664–675. [Google Scholar] [CrossRef]
- Boada-Pladellorens, A.; Avellanet, M.; Pages-Bolibar, E.; Veiga, A. Stromal vascular fraction therapy for knee osteoarthritis: A systematic review. Ther. Adv. Musculoskelet. Dis. 2022, 14, 1759720X221117879. [Google Scholar] [CrossRef]
- Sharma, S.; Muthu, S.; Jeyaraman, M.; Ranjan, R.; Jha, S.K. Translational products of adipose tissue-derived mesenchymal stem cells: Bench to bedside applications. World J. Stem Cells 2021, 13, 1360–1381. [Google Scholar] [CrossRef]
- Tonnard, P.; Verpaele, A.; Peeters, G.; Hamdi, M.; Cornelissen, M.; Declercq, H. Nanofat grafting: Basic research and clinical applications. Plast Reconstr. Surg. 2013, 132, 1017–1026. [Google Scholar] [CrossRef]
- Mashiko, T.; Wu, S.H.; Feng, J.; Kanayama, K.; Kinoshita, K.; Sunaga, A.; Narushima, M.; Yoshimura, K. Mechanical Micronization of Lipoaspirates: Squeeze and Emulsification Techniques. Plast Reconstr. Surg. 2017, 139, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Jeyaraman, M.; Muthu, S.; Sharma, S.; Ganta, C.; Ranjan, R.; Jha, S.K. Nanofat: A therapeutic paradigm in regenerative medicine. World J. Stem Cells 2021, 13, 1733–1746. [Google Scholar] [CrossRef] [PubMed]
- Michalek, J.; Moster, R.; Lukac, L.; Proefrock, K.; Petrasovic, M.; Rybar, J.; Chaloupka, A.; Darinskas, A.; Michalek, J.; Kristek, J.; et al. Stromal Vascular Fraction Cells of Adipose and Connective Tissue in People with Osteoarthritis: A Case Control Prospective Multi-Centric Non-Randomized Study. Glob. Surg. 2017, 3, 1–9. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ambrosio, L.; Russo, F.; Catapano, S.; Papalia, G.F.; Vadalà, G.; Papalia, R.; Denaro, V. An Innovative Surgical Technique to Obtain an Adipose-Derived Stromal Cell-Rich Graft for the Treatment of Osteoarthritis: Technical Note. Surg. Tech. Dev. 2023, 12, 60-67. https://doi.org/10.3390/std12020005
Ambrosio L, Russo F, Catapano S, Papalia GF, Vadalà G, Papalia R, Denaro V. An Innovative Surgical Technique to Obtain an Adipose-Derived Stromal Cell-Rich Graft for the Treatment of Osteoarthritis: Technical Note. Surgical Techniques Development. 2023; 12(2):60-67. https://doi.org/10.3390/std12020005
Chicago/Turabian StyleAmbrosio, Luca, Fabrizio Russo, Simone Catapano, Giuseppe Francesco Papalia, Gianluca Vadalà, Rocco Papalia, and Vincenzo Denaro. 2023. "An Innovative Surgical Technique to Obtain an Adipose-Derived Stromal Cell-Rich Graft for the Treatment of Osteoarthritis: Technical Note" Surgical Techniques Development 12, no. 2: 60-67. https://doi.org/10.3390/std12020005
APA StyleAmbrosio, L., Russo, F., Catapano, S., Papalia, G. F., Vadalà, G., Papalia, R., & Denaro, V. (2023). An Innovative Surgical Technique to Obtain an Adipose-Derived Stromal Cell-Rich Graft for the Treatment of Osteoarthritis: Technical Note. Surgical Techniques Development, 12(2), 60-67. https://doi.org/10.3390/std12020005