
What Nursing-Sensitive Outcomes Have Been Investigated to Date among Patients with Solid and Hematological Malignancies? A Scoping Review



Abstract
:1. Introduction
- symptom experience: pain, fatigue, insomnia, nausea, constipation, anorexia, breathlessness, diarrhoea, altered skin/mucous membranes, neutropenia;
- functional status: ADL (activities of daily living), IADL (instrumental activities of daily living), role functioning, activity tolerance, ability to carry out usual activities, nutritional status;
- safety (infections, falls, skin ulcers, extravasation incidents, hypersensitive reactions);
- psychological distress (anxiety, depression, spiritual distress); and
- economic (length of stay, unexpected readmissions, emergency visits, out-of-pocket costs, cost per patient day, and cost per episode of care).
2. Materials and Methods
2.1. Research Questions
2.2. Study Design
2.3. Patient, Concept, and Context Framework
- Participants: adult patients with solid tumours or haematological malignancies, at their first diagnosis of cancer or at an advanced stage, in active therapeutic onco-haematological treatments.
- Concept: NSOs identified as any measurable behaviour, condition, or perception of the patient or his/her family that is obtained or is significantly affected by the nursing care received [3].
- Context: onco-haematological care settings, as studies conducted in cancer units/hospitals or outpatient centres, at public or private clinics, including teaching hospitals or at home. Hospice and/or palliative care services were not considered as context given that patients are not subjected to active therapeutic treatments.
2.4. Search Strategy
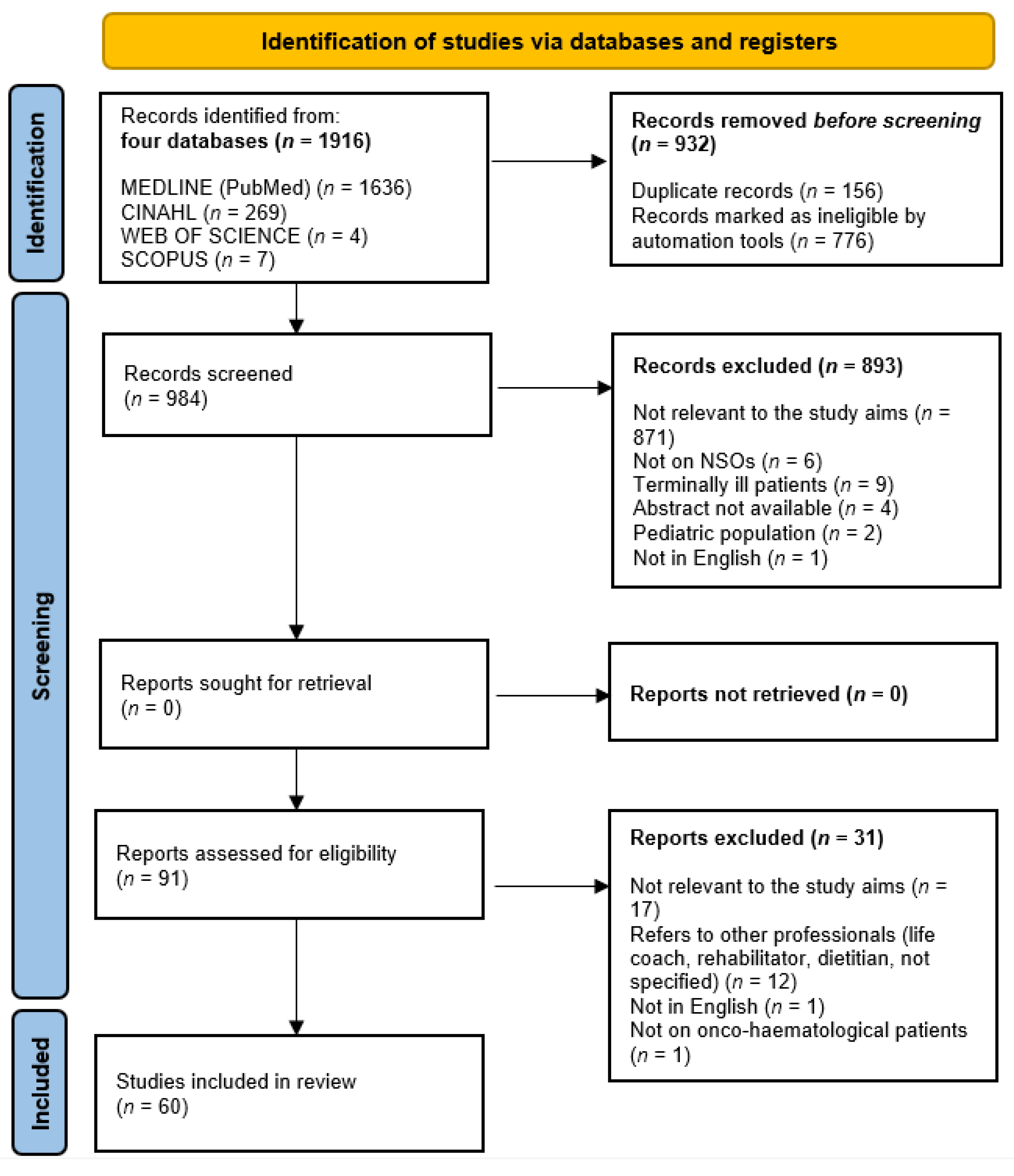
2.5. Study Selection
2.6. Data Collection
2.7. Data Synthesis and Reporting
3. Results
3.1. How Have NSOs Been Investigated in the Field of Oncological Nursing Care?
3.2. What NSOs Have Been Measured to Date and How? The Inductive Approach
3.3. To What Extent Does the NSOs Framework in This Field Reflect the Nursing Outcomes Documented to Date? The Deductive Approach
4. Discussion
4.1. Characteristics of Included Studies
4.2. What NSOs Have Been Measured to Date and How? The Inductive Approach
4.3. To What Extent Does the NSOs Framework in This Nursing Field Reflect the Nursing Outcomes Documented to Date? The Deductive Approach
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Public Involvement Statement
Guidelines and Standards Statement
Conflicts of Interest
References
- Graystone, R. The importance of nurse-sensitive outcome measurements. J. Nurs. Adm. 2018, 48, 533–534. [Google Scholar] [CrossRef]
- Maas, M.L.; Johnson, M.; Moorhead, S. Classifying nursing-sensitive patient outcomes. Image J. Nurs. Sch. 1996, 28, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Moorhead, S.; Johnson, M.; Maas, M. Iowa Outcomes Project. In Nursing Outcomes Classification (NOC)/Iowa Outcomes Project, 3rd ed.; Mosby: St. Louis, MO, USA, 2003. [Google Scholar]
- American Nurses Association. Nursing’s Report Card for Acute Care Settings; American Nurses Publishing: Washington, DC, USA, 1995. [Google Scholar]
- Doran, D.I.; Sidani, S.; Keatings, M.; Doidge, D. An empirical test of the nursing role effectiveness model. J. Adv. Nurs. 2002, 38, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.J.; Brady-Schluttner, K.; Ellenbecker, S.; Johnson, M.; Lassegard, E.; Maas, M.; Stone, J.L.; Westra, B.L. Evaluating physical functional outcomes: One category of the NOC system. Medsurg. Nurs. 1996, 5, 157–162. [Google Scholar] [PubMed]
- Mitchell, P.H.; Lang, N.M. Framing the problem of measuring and improving healthcare quality: Has the Quality Health Outcomes Model been useful? Med. Care 2004, 42, II4–II11. [Google Scholar] [CrossRef]
- Palese, A.; Beltrame, E.R.; Bin, A.; Borghi, G.; Bottacin, M.; Buchini, S.; Buffon, M.L.; Carniel, G.; Dal Bo’, O.; De Caneva, S.; et al. Esiti sensibili alle cure infermieristiche: Analisi critica della letteratura [Nursing sensitive outcomes: A critical appraisal of the literature]. Assist. Inferm. Ric. 2008, 27, 33–42. [Google Scholar] [PubMed]
- Aiken, L.H.; Cimiotti, J.P.; Sloane, D.M.; Smith, H.L.; Flynn, L.; Neff, D.F. Effects of nurse staffing and nurse education on patient deaths in hospitals with different nurse work environments. J. Nurs. Adm. 2012, 42, S10–S16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, P.; Maruotti, A.; Recio Saucedo, A.; Redfern, O.C.; Ball, J.E.; Briggs, J.; Dall’Ora, C.; Schmidt, P.E.; Smith, G.B.; Missed Care Study Group. Nurse staffing, nursing assistants and hospital mortality: Retrospective longitudinal cohort study. BMJ Qual. Saf. 2019, 28, 609–617. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.G.; Kim, J.S. The association between nurse staffing levels and paediatric nursing-sensitive outcomes in tertiary hospitals. J. Nurs. Manag. 2018, 26, 1002–1014. [Google Scholar] [CrossRef]
- Oner, B.; Zengul, F.D.; Oner, N.; Ivankova, N.V.; Karadag, A.; Patrician, P.A. Nursing-sensitive indicators for nursing care: A systematic review (1997–2017). Nurs. Open 2021, 8, 1005–1022. [Google Scholar] [CrossRef]
- Seligardi, M.; Bassi, E.; Mongardi, M. Esiti sensibili alle cure infermieristiche e staffing: Le infezioni correlate all’assistenza. Revisione della letteratura [Nursing sensitive outcomes and staffing: A review on healthcare associated infection]. Assist. Inferm. Ric. 2017, 36, 172–178. [Google Scholar] [PubMed]
- Danielis, M.; Palese, A.; Terzoni, S.; Destrebecq, A. What nursing sensitive outcomes have been studied to-date among patients cared for in intensive care units? Findings from a scoping review. Int. J. Nurs. Stud. 2020, 102, 103491. [Google Scholar] [CrossRef]
- Danielis, M.; Castellano, A.; Mattiussi, E.; Palese, A. Nursing-Sensitive Outcomes among Patients Cared for in Paediatric Intensive Care Units: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 9507. [Google Scholar] [CrossRef]
- Oleske, D.M.; Hauck, W.W. A population-based evaluation of the impact of interventions for improving care to cancer patients in the home setting. Home Health Care Serv. Q. 1988, 9, 45–61. [Google Scholar] [CrossRef]
- Given, B.A.; Sherwood, P.R. Nursing sensitive patient outcomes—A white paper. Oncol. Nurs. Forum 2005, 32, 773–784. [Google Scholar] [CrossRef]
- Williams, S.A. Quality and care: Patients’ perceptions. J. Nurs. Care Qual. 1998, 12, 18–25. [Google Scholar] [PubMed]
- Given, B.; Beck, S.; Etland, C.; Gobel, B.H.; Lamkin, L.; Marsee, V. Oncology Nursing-Sensitive Patient Outcomes. Available online: http://www.ons.org/Research/NursingSensitive/Description (accessed on 12 November 2021).
- Griffiths, P.; Richardson, A.; Blackwell, R. Nurse Sensitive Outcomes & Indicators in Ambulatory Chemotherapy; National Nursing Research Unit, King’s College of London: London, UK, 2009. [Google Scholar]
- Griffiths, P.; Richardson, A.; Blackwell, R. Outcomes sensitive to nursing service quality in ambulatory cancer chemotherapy: Systematic scoping review. Eur. J. Oncol. Nurs. 2012, 16, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Molassiotis, A.; Liu, X.L.; Kwok, S.W. Impact of advanced nursing practice through nurse-led clinics in the care of cancer patients: A scoping review. Eur. J. Cancer Care 2021, 30, e13358. [Google Scholar] [CrossRef]
- Blackburn, L.M.; Abel, S.; Green, L.; Johnson, K.; Panda, S. The Use of comfort kits to optimize adult cancer pain management. Pain Manag. Nurs. 2019, 20, 25–31. [Google Scholar] [CrossRef]
- Yates, P.; Edwards, H.; Nash, R.; Aranda, S.; Purdie, D.; Najman, J.; Skerman, H.; Walsh, A. A randomized controlled trial of a nurse-administered educational intervention for improving cancer pain management in ambulatory settings. Patient Educ. Couns. 2004, 53, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, K.; Beaver, K.; Kitchener, H.; O’Neill, J.; Farrell, C. Women’s experiences of information, psychological distress and worry after treatment for gynaecological cancer. Patient Educ. Couns. 2005, 56, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Musiello, T.; Dixon, G.; O’Connor, M.; Cook, D.; Miller, L.; Petterson, A.; Saunders, C.; Joske, D.; Johnson, C. A pilot study of routine screening for distress by a nurse and psychologist in an outpatient haematological oncology clinic. Appl. Nurs. Res. 2017, 33, 15–18. [Google Scholar] [CrossRef]
- Godino, C.; Jodar, L.; Durán, A.; Martínez, I.; Schiaffino, A. Nursing education as an intervention to decrease fatigue perception in oncology patients. Eur. J. Oncol Nurs. 2006, 10, 150–155. [Google Scholar] [CrossRef]
- Braamse, A.M.; van Meijel, B.; Visser, O.; van Oppen, P.; Boenink, A.D.; Eeltink, C.; Cuijpers, P.; Huijgens, P.C.; Beekman, A.T.; Dekker, J. Distress and quality of life after autologous stem cell transplantation: A randomized clinical trial to evaluate the outcome of a web-based stepped care intervention. BMC Cancer 2010, 10, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, S.; Ogawa, K.; Yamagishi, A. Effectiveness of communication skills training of nurses on the quality of life and satisfaction with healthcare professionals among newly diagnosed cancer patients: A preliminary study. Psycho-Oncology 2011, 20, 1285–1291. [Google Scholar] [CrossRef]
- Coleman, E.A.; Coon, S.K.; Lockhart, K.; Kennedy, R.L.; Montgomery, R.; Copeland, N.; McNatt, P.; Savell, S.; Stewart, C. Effect of certification in oncology nursing on nursing-sensitive outcomes. J. Nurs. Adm. 2010, 40, S35–S42. [Google Scholar] [CrossRef] [Green Version]
- Riese, C.; Weiß, B.; Borges, U.; Beylich, A., Jr.; Dengler, R.; Hermes-Moll, K.; Welslau, M.; Baumann, W. Effectiveness of a standardized patient education program on therapy-related side effects and unplanned therapy interruptions in oral cancer therapy: A cluster-randomized controlled trial. Support. Care Cancer 2017, 25, 3475–3483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayaad, O.; Alloubani, A.; Al-Rafaay, M.; Arideh, A.; Abualeish, M.; Akhu-Zaheya, L. Impact of structured nurse leader rounds on satisfaction with nursing care among patients with cancer. J. Nurs. Sch. 2019, 51, 526–536. [Google Scholar] [CrossRef]
- Gray, R.E.; Goel, V.; Fitch, M.I.; Franssen, E.; Labrecque, M. Supportive care provided by physicians and nurses to women with breast cancer. Results from a population-based survey. Support. Care Cancer 2002, 10, 647–652. [Google Scholar] [CrossRef]
- Jernigan, C.; Johnson, T.; Varghese, S.; Fellman, B. Evaluating the feasibility of a nurse-driven telephone triage intervention for patients with cancer in the ambulatory setting. Oncol. Nurs. Forum 2020, 47, E44–E54. [Google Scholar] [CrossRef]
- Graupner, C.; Kimman, M.L.; Mul, S.; Slok, A.; Claessens, D.; Kleijnen, J.; Dirksen, C.D.; Breukink, S.O. Patient outcomes, patient experiences and process indicators associated with the routine use of patient-reported outcome measures (PROMs) in cancer care: A systematic review. Support. Care Cancer 2021, 29, 573–593. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Peters, M.; Marnie, C.; Colquhoun, H.; Garritty, C.M.; Hempel, S.; Horsley, T.; Langlois, E.V.; Lillie, E.; O’Brien, K.K.; Tunçalp, Ö.; et al. Scoping reviews: Reinforcing and advancing the methodology and application. Syst. Rev. 2021, 10, 263. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; Adelaide, North Adelaide, Australia Joanna Briggs Institute: North Adelaide, Australia, 2020. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiese, M.S. Observational and interventional study design types: An overview. Biochem. Med. 2014, 24, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Gordils-Perez, J.; Schneider, S.M.; Gabel, M.; Trotter, K.J. Oncology nurse navigation: Development and implementation of a program at a comprehensive cancer center. Clin. J. Oncol. Nurs. 2017, 21, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B. Health services research: A working model. N. Eng. J. Med. 1973, 289, 132–136. [Google Scholar] [CrossRef]
- Ekwall, E.; Ternestedt, B.M.; Sorbe, B. Important aspects of health care for women with gynecologic cancer. Oncol. Nurs. Forum 2003, 30, 313–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Doran, D.M.; Sidani, S.; Di Pietro, T. Nursing-sensitive outcomes. In Foundations of Clinical Nurse Specialist Practice; Fulton, J.S., Lyon, B., Goudreau, K., Eds.; Springer: New York, NY, USA, 2010; pp. 35–37. [Google Scholar]
- Scott, C.; Andrews, D.; Bulla, S.; Loerzel, V. Teach-back method: Using a nursing education intervention to improve discharge instructions on an adult oncology unit. Clin. J. Oncol Nurs. 2019, 23, 288–294. [Google Scholar]
- Stacey, D.; Ludwig, C.; Jolicoeur, L.; Carley, M.; Balchin, K.; Jibb, L.; Kelly, F.; Kuziemsky, C.; Madore, S.; Rambout, L.; et al. Quality of telephone-based cancer symptom management by nurses: A quality improvement project. Support. Care Cancer 2021, 29, 841–849. [Google Scholar] [CrossRef]
- Given, B.; Given, C.W.; McCorkle, R.; Kozachik, S.; Cimprich, B.; Rahbar, M.H.; Wojcik, C. Pain and fatigue management: Results of a nursing randomized clinical trial. Oncol. Nurs. Forum 2002, 29, 949–956. [Google Scholar] [CrossRef] [Green Version]
- Kvåle, K.; Synnes, O. Understanding cancer patients’ reflections on good nursing care in light of Antonovsky’s theory. Eur. J. Oncol. Nurs. 2013, 17, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, C. Oral chemotherapy: Patient education and nursing intervention. J. Oncol. Navig. Surviv. 2016, 7, 20–27. [Google Scholar]
- Du Pen, A.R.; Du Pen, S.; Hansberry, J.; Miller-Kraybill, B.; Millen, J.; Everly, R.; Hansen, N.; Syrjala, K. An educational implementation of a cancer pain algorithm for ambulatory care. Pain Manag. Nurs. 2000, 1, 116–128. [Google Scholar] [CrossRef]
- Curcio, K.R.; Lambe, C.; Schneider, S.; Khan, K. Evaluation of a cancer survivorship protocol: Transitioning patients to survivors. Clin. J. Oncol. Nurs. 2012, 16, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Jakobsson, L.; Holmberg, L. Quality from the patient’s perspective: A one-year trial. Int. J. Health Care Qual. Assur. 2012, 25, 177–188. [Google Scholar] [CrossRef]
- Charalambous, A. Variations in patient satisfaction with care for breast, lung, head and neck and prostate cancers in different cancer care settings. Eur. J. Oncol. Nurs. 2013, 17, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Larsson, G.; Widmark Peterson, V.; Lampic, C.; von Essen, L.; Sjödén, P.O. Cancer patient and staff ratings of the importance of caring behaviors and their relations to patient anxiety and depression. J. Adv. Nurs. 1998, 27, 855–864. [Google Scholar] [CrossRef]
- MacLeod, A.; Branch, A.; Cassidy, J.; McDonald, A.; Mohammed, N.; MacDonald, L. A nurse-/pharmacy-led capecitabine clinic for colorectal cancer: Results of a prospective audit and retrospective survey of patient experiences. Eur. J. Oncol. Nurs. 2007, 11, 247–254. [Google Scholar] [CrossRef]
- Halldórsdóttir, S.; Hamrin, E. Caring and uncaring encounters within nursing and health care from the cancer patient’s perspective. Cancer Nurs. 1997, 20, 120–128. [Google Scholar] [CrossRef]
- Ivers, R.; Jackson, B.; Levett, T.; Wallace, K.; Winch, S. Home to health care to hospital: Evaluation of a cancer care team based in Australian Aboriginal primary care. Aust. J. Rural Health 2019, 27, 88–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hargie, O.; Brataas, H.; Thorsnes, S. Cancer patients’ sensemaking of conversations with cancer nurses in outpatient clinics. Aust. J. Adv. Nurs. 2009, 26, 70–78. [Google Scholar]
- Sommer, M.; Frandsen, L.; Jensen, P.; Bøgsted, M.; El-Galaly, T.C.; Grønkjær, M. Hematological cancer survivors’ experiences of participating in a shared care follow-up-an exploratory interview study. J. Cancer Surviv. 2021, 15, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Krishnasamy, M. What do cancer patients identify as supportive and unsupportive behaviour of nurses? A pilot study. Eur. J. Cancer Care 1996, 5, 103–110. [Google Scholar] [CrossRef]
- de Veer, A.; Slev, V.N.; Pasman, H.R.; Verdonck-de Leeuw, I.M.; Francke, A.L.; van Uden-Kraan, C.F. Assessment of a structured self-management support intervention by nurses for patients with incurable cancer. Oncol. Nurs. Forum 2020, 47, 305–317. [Google Scholar] [CrossRef]
- Coolbrandt, A.; Wildiers, H.; Aertgeerts, B.; Dierckx de Casterlé, B.; van Achterberg, T.; Milisen, K. Systematic development of CHEMO-SUPPORT, a nursing intervention to support adult patients with cancer in dealing with chemotherapy-related symptoms at home. BMC Nurs. 2018, 17, 28. [Google Scholar] [CrossRef] [Green Version]
- Zou, J.Y.; Xu, Y.; Wang, X.H.; Jiang, Q.; Zhu, X.M. Improvement of constipation in leukemia patients undergoing chemotherapy using sweet potato. Cancer Nurs. 2016, 39, 181–186. [Google Scholar] [CrossRef]
- Andersson, P.; Persson, L.; Hallberg, I.R.; Renvert, S. Testing an oral assessment guide during chemotherapy treatment in a Swedish care setting: A pilot study. J. Clin. Nurs. 1999, 8, 150–158. [Google Scholar] [CrossRef]
- Panteli, V.; Patistea, E. Assessing patients’ satisfaction and intensity of pain as outcomes in the management of cancer-related pain. Eur. J. Oncol Nurs. 2007, 11, 424–433. [Google Scholar] [CrossRef]
- Mårtensson, G.; Carlsson, M.; Lampic, C. Are cancer patients whose problems are overestimated by nurses less satisfied with their care? Eur. J. Cancer Care 2010, 19, 382–392. [Google Scholar] [CrossRef]
- Egerod, I.; Kaldan, G.; Nordentoft, S.; Larsen, A.; Herling, S.F.; Thomsen, T.; Endacott, R.; INACTIC-group. Skills, competencies, and policies for advanced practice critical care nursing in Europe: A scoping review. Nurse Educ. Pract. 2021, 54, 103142. [Google Scholar] [CrossRef] [PubMed]
- McDonald, G.B.; Sandmaier, B.M.; Mielcarek, M.; Sorror, M.; Pergam, S.A.; Cheng, G.S.; Hingorani, S.; Boeckh, M.; Flowers, M.D.; Lee, S.J.; et al. Survival, Nonrelapse Mortality, and Relapse-Related Mortality After Allogeneic Hematopoietic Cell Transplantation: Comparing 2003–2007 Versus 2013–2017 Cohorts. Ann. Intern. Med. 2020, 172, 229–239. [Google Scholar] [CrossRef]
- Bönte, M.; von dem Knesebeck, O.; Siegrist, J.; Marceau, L.; Link, C.; Arber, S.; Adams, A.; McKinlay, J.B. Women and men with coronary heart disease in three countries: Are they treated differently? Womens Health Issues 2018, 18, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Tognoni, G. Misurare e valutare alle frontiere incerte tra quantità e qualità. Assist. Inferm. Ric. 2022, 41, 182–185. [Google Scholar]
- Valderas, J.M.; Alonso, J. Patient reported outcome measures: A model-based classification system for research and clinical practice. Qual. Life Res. 2008, 17, 1125–1135. [Google Scholar] [CrossRef]
- Ruatti, E.; Danielis, M.; Palese, A. Il programma Productive Ward per migliorare la qualità delle cure infermieristiche: Risultati di una scoping review [The Productive Ward programme to provide high quality care: Findings from a scoping review]. Assist. Inferm. Ric. 2021, 40, 221–232. [Google Scholar] [PubMed]
- Erdoğan Yüce, G.; Döner, A.; Muz, G. Psychological Distress and Its Association with Unmet Needs and Symptom Burden in Outpatient Cancer Patients: A Cross-Sectional Study. Semin. Oncol. Nurs. 2021, 37, 151214. [Google Scholar] [CrossRef]
- Skrutkowski, M.; Saucier, A.; Eades, M.; Swidzinski, M.; Ritchie, J.; Marchionni, C.; Ladouceur, M. Impact of a pivot nurse in oncology on patients with lung or breast cancer: Symptom distress, fatigue, quality of life, and use of healthcare resources. Oncol. Nurs. Forum 2008, 35, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Bevans, M.; El-Jawahri, A.; Tierney, D.K.; Wiener, L.; Wood, W.A.; Hoodin, F.; Kent, E.E.; Jacobsen, P.B.; Lee, S.J.; Hsieh, M.M.; et al. National Institutes of Health Hematopoietic Cell Transplantation Late Effects Initiative: The Patient-Centered Outcomes Working Group Report. Biol. Blood Marrow Transplant. 2017, 23, 538–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palese, A.; Zanini, A.; Carlevaris, E.; Morandin, A.; Carpanelli, I.; Dante, A. Hidden outpatient oncology clinical nursing minimum data set: Findings from an Italian multi-method study. Eur. J. Oncol Nurs. 2013, 17, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Sanson, G.; Alvaro, R.; Cocchieri, A.; Vellone, E.; Welton, J.; Maurici, M.; Zega, M.; D’Agostino, F. Nursing Diagnoses, Interventions, and Activities as Described by a Nursing Minimum Data Set: A Prospective Study in an Oncology Hospital Setting. Cancer Nurs. 2019, 42, E39–E47. [Google Scholar] [CrossRef]
- Tisnasari, I.A.M.A.S.; Nuraini, T.; Afiyanti, Y.; Rudi, R.; Maria, R. Psychological and sexual problems of cancer survivors. Arch. Ital. Urol. Androl. 2003, 95, 11473. [Google Scholar] [CrossRef] [PubMed]
- Martinez, K.A.; Friese, C.; Kershaw, T.; Given, C.W.; Fendrick, A.M.; Northouse, L. Effect of a nurse-led psychoeducational intervention on healthcare service utilization among adults with advanced cancer. Oncol. Nurs. Forum 2015, 42, E310–E318. [Google Scholar] [CrossRef] [Green Version]
- Zaorsky, N.G.; Khunsriraksakul, C.; Acri, S.L.; Liu, D.J.; Ba, D.M.; Lin, J.L.; Liu, G.; Segel, J.E.; Drabick, J.J.; Mackley, H.B.; et al. Medical Service Use and Charges for Cancer Care in 2018 for Privately Insured Patients Younger Than 65 Years in the US. J. Am. Med. Assoc. 2021, 4, e2127784. [Google Scholar] [CrossRef] [PubMed]
- Torstveit, A.H.; Miaskowski, C.; Løyland, B.; Grov, E.K.; Guren, M.G.; Ritchie, C.S.; Paul, S.M.; Kleven, A.G.; Utne, I. Common and distinct characteristics associated with self-reported functional status in older patients with cancer receiving chemotherapy. Eur. J. Oncol. Nurs. 2021, 54, 102033. [Google Scholar] [CrossRef]
- Chang, Y.; Lin, Y.P.; Chang, H.J.; Lin, C.C. Cancer patient and staff ratings of caring behaviours: Relationship to level of pain intensity. Cancer Nurs. 2005, 28, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.I.; Milligan, P.; Cairns, J.; McClelland, D.B.; Parker, A.C. Nurse practitioner support for transfusion in patients with haematological disorders in hospital and at home. Transfus. Med. 1999, 9, 31–36. [Google Scholar] [CrossRef]
- Ferreira, E.; Kamada, I.; Reis, P.E.; Cruz, F.O.; Jesus, C.A.; Pinho, D.L. Telephone contact as a strategy for the promotion of comfort to the patient submitted to chemotherapy. J. Nurs. 2017, 11, 1936–1942. [Google Scholar]
- Keeley, P.; Wolf, Z.; Regul, L.; Jadwin, A. Effectiveness of standard of care protocol on patient satisfaction and perceived staff caring. Clin. J. Oncol. Nurs. 2015, 19, 352–360. [Google Scholar] [CrossRef]
- Kimman, M.L.; Bloebaum, M.M.; Dirksen, C.D.; Houben, R.M.; Lambin, P.; Boersma, L.J. Patient satisfaction with nurse-led telephone follow-up after curative treatment for breast cancer. BMC Cancer 2010, 10, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleeberg, U.R.; Feyer, P.; Günther, W.; Behrens, M. Patient satisfaction in outpatient cancer care: A prospective survey using The PASQOC questionnaire. Support. Care Cancer 2008, 16, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Kousoulou, M.; Suhonen, R.; Charalambous, A. Associations of individualized nursing care and quality oncology nursing care in patients diagnosed with cancer. Eur. J. Oncol. Nurs. 2019, 41, 33–40. [Google Scholar] [CrossRef]
- McCorkle, R.; Strumpf, N.E.; Nuamah, I.F.; Adler, D.C.; Cooley, M.E.; Jepson, C.; Lusk, E.J.; Torosian, M. A specialized home care intervention improves survival among older post-surgical cancer patients. J. Am. Geriatr. Soc. 2000, 48, 1707–1713. [Google Scholar]
- McCorkle, R.; Jeon, S.; Ercolano, E.; Lazenby, M.; Reid, A.; Davies, M.; Viveiros, D.; Gettinger, S. An advanced practice nurse coordinated multidisciplinary intervention for patients with late-stage cancer: A cluster randomized trial. J. Palliat. Med. 2015, 18, 962–969. [Google Scholar] [CrossRef] [Green Version]
- McGrath, P. Taking control: Findings of a prospective study of an educational course for patients with leukaemia. Support. Care Cancer 2000, 8, 377–384. [Google Scholar] [CrossRef]
- Milani, A.; Mauri, S.; Gandini, S.; Magon, G. Oncology Nursing Minimum Data Set (ONMDS): Can we hypothesize a set of prevalent Nursing Sensitive Outcomes (NSO) in cancer patients? Ecancermedicalscience 2013, 7, 345. [Google Scholar]
- Møller, T.; Borregaard, N.; Tvede, M.; Adamsen, L. Patient education--a strategy for prevention of infections caused by permanent central venous catheters in patients with haematological malignancies: A randomized clinical trial. J. Hosp. Infect. 2005, 61, 330–341. [Google Scholar] [CrossRef]
- Muñoz, R.; Farshidpour, L.; Chaudhary, U.B.; Fathi, A.H. Multidisciplinary cancer care model: A positive association between oncology nurse navigation and improved outcomes for patients with cancer. Clin. J. Oncol. Nurs. 2018, 22, E141–E145. [Google Scholar] [CrossRef] [PubMed]
- Naveh, P.; Leshem, R.; Dror, Y.F.; Musgrave, C.F. Pain severity, satisfaction with pain management, and patient-related barriers to pain management in patients with cancer in Israel. Oncol. Nurs. Forum 2011, 38, E305–E313. [Google Scholar] [CrossRef] [Green Version]
- Predeger, E.J.; O’Malley, M.; Hendrix, T.; Parker, N.M. Oncology rehabilitation outcomes over time: A mixed-methods approach. Oncol. Nurs. Forum 2014, 41, E56–E63. [Google Scholar] [CrossRef] [PubMed]
- Stuart, T.A.; Stutzman, S.E.; Hicks, A.D.; Olson, D.M. Patient education: A comparison of teaching strategies for patients with brain neoplasms. Clin. J. Oncol. Nurs. 2019, 23, E81–E86. [Google Scholar] [CrossRef] [PubMed]
- Tseng, H.; Moorhead, S. The use of standardized terminology to represent nursing knowledge: Nursing interventions relevant to safety for patients with cancer. Stud. Health Technol. Inform. 2014, 201, 298–303. [Google Scholar]
- Westman, B.; Ullgren, H.; Olofsson, A.; Sharp, L. Patient-reported perceptions of care after the introduction of a new advanced cancer nursing role in Sweden. Eur. J. Oncol. Nurs. 2019, 41, 41–48. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| NSOs: Categories (n, %) | NSOs: Sub-Categories (n, %) * | Metrics of the NSOs: Data Collection Tool and Language * (n of Studies) |
|---|---|---|
| Satisfaction and perception of nursing care received (32, 21.2%) | Satisfaction (19, 12.6%) * | PSNCQQ, validated questionnaire, Arabic (1) GGZ-thermometer, validated questionnaire, Dutch (1) PSS, self-report validated questionnaire, Greek (1) PGI, validated questionnaire, English (2) Non-declared tool, English (1), NA (1) Ranking questionnaire, 5-point scale, not validated, English (1) Satisfaction survey, English (1) 5 A’s model’, self-report questionnaire + 11-point Likert-type scale, self-report questionnaire, Dutch (1) VAS tool, Japanese (1), NA (1) 7 questions from the PGO, not validated self-report questionnaire, English (1) PSCC, validated scale, English (1) Satisfaction questionnaire, previously piloted self-report questionnaire, Spanish (1) HCAHPS, self-report questionnaire, English (1) PSQ III, validated questionnaire, Dutch (1), English (1) PASQOC, validated self-report questionnaire, German (1) * NSC, validated self-report questionnaire, Swedish (1) CASC, validated self-report questionnaire, Swedish, and two open questions (1) APS POQ, validated tool, Greek (1) * Open questions and semi-structured interviews (1) |
| Experiences and perceptions of care (11, 7.2%) * | Non-declared tool, English (1) 7 single questions adapted by the 10-care dimension by NCSR, not validated, Greek (1) Survey questionnaire, non-validated, English (1) * Non-validated self-report questionnaire with Likert scales and open-ended comments, English (1) * 6-items of study specific questionnaire, Swedish (1) Semi-structured interview analysed using a qualitative content analysis (1) * Semi-structured interviews analysed by thematic analysis (1) * NA (1) | |
| Quality of the relationship with nurses (2, 1.3%) * | Deep-probe semi-structured “sensemaking” interviews (1) Not highly structured interview using an hermeneutical approach (1) * | |
| Nursing care process quality (18, 11.9%) | Quality of care received (5, 3.3%) | In-depth dialogues analysed by thematic analysis (1) CBI-24, validated self-report questionnaire, English (1) QPP, validated self-report questionnaire, Swedish (1) ICS, self-report validated questionnaire, Greek (1) QONCS, self-report validated questionnaire, Greek (1) SMAT, 8 item tool to analyse audio-recorded calls and documentation, English and French (1) |
| Timing (5, 3.3%) | Time from diagnosis to treatment (1) Waiting time from admission to transfusion (1) Length of patient stay (1) Time conducting the screening in the ambulatory (1) Time from the first health nurse visit to the last home health nurse visit (1) | |
| Caring and uncaring behaviours (4, 2.6%) * | CARE-Q, validated assessment tool, Chinese (1) and Norwegian (1) Semi-structured interview analysed by thematic analysis (1) * HCI, validated questionnaire, English (1) | |
| Access to care (2, 1.3%) | Time for the first patient call to first oncology provider consultation (1) 7-items of study specific questionnaire for access to resources (1) | |
| Acceptability and accessibility of cancer service (1, 0.6%) * | Semi-structured interviews analysed by grounded theory (1) * | |
| Disposition at discharge (1, 0.6%) | Disposition at discharge (1) | |
| Psychological distress (11, 7.3%) | General (7, 4.6%) | HADS, self-report validated questionnaire, English (2), Dutch (1), Swedish (2), NA (1) PHQ-9, self-report questionnaire, Dutch (1), English (1) * POMS, validated, NA (1) NCCN DT, self-report validated questionnaire, English (1) The Problem List, self-report validated questionnaire, English (1) |
| Depression (2, 1.3%) * | CES-D, self-report questionnaire, English (1), NA (1) | |
| Anxiety (2, 1.3%) | STAI-state adapted, self-report validated questionnaire, Dutch (1), NA (1) GAD-7, validated self-report questionnaire, English (1) | |
| Experiences with therapy-related side effects (11, 7.3%) | General symptoms (8, 5.3%) * | SES, 5-point scale, English, and telephone-based interview (1) MDASI, validated self-report questionnaire, English (1) MDASI-NH, self-report questionnaire, English (1) FACT-HNSI, validated, NA (1) CSAS, validated, NA (1) MSAS, validated questionnaire, English (1) * NA (1) NRS, validated, NA (1) Checklist format using based on scientific literature, Portuguese (1) Frequencies from the patients’ diaries (1) |
| Symptom distress (3, 2.0%) | SDS, self-report questionnaire, English (3) * | |
| Health care system utilization (10, 6.6%) | Emergency department visits (4, 2.6%) | N of emergency department visits (4) |
| Hospital admissions/hospitalizations (2, 1.3%) | N of hospital admissions/hospitalizations (2) | |
| Referrals (1, 0.6%) | Referral rate (1) | |
| Clinical appointments/visits (3, 2.0%) | N of appointments (1) N of home visits (1) N of missed appointments (1) | |
| Pain (9, 6.0%) | Resolution/reduction (7, 4.6%) * | BPI-C, self-report questionnaire, Chinese (1) and English (2) * VAS, self-report validated tool (1) * 10 degree not-declared scale, English (1) NA (1) |
| Satisfaction with pain management (2, 1.3%) | Non-declared scale for ambulatory patients and two statements for inpatients (1) RPS-POQ, validated self-report questionnaire, Hebrew (1) | |
| Health-related quality of life (8, 5.2%) | - | EORTC QLQ-C30, validated questionnaire, Dutch (1), NA (1) SF-8, validated questionnaire, Japanese (1) SF-36, validated questionnaire, Dutch (1), English (1) * EORTC QLQ-C15-PAL, validated questionnaire, Dutch (1) FACIT-Sp, validated self-report questionnaire, Swedish (1) FACT-G, validated questionnaire, English (2), NA (1) FACT-HN, validated, NA (1) FACT B/ES, validated, NA (1) QLQ-BR23, validated, NA (1) |
| Barriers and facilitators to intervention adherence/symptoms (5, 3.3%) * | - | ASK-12, validated tool, English (1) PBS, validated questionnaire, English (1) * BQ-SF, validated self-report questionnaire, Hebrew (1) Checklist and open-ended questions, English (1) * Self-report questionnaire developed for the study, English (1) |
| Role functioning (4, 2.6%) | Functional status (3, 2.0%) * | Two subscales from the SF-36, validated questionnaire, English, and telephone-based interview (1) ESDS, self-report questionnaire, validated, English (2) * |
| Ability to function independently (1, 0.6%) | DGSS, validated questionnaire, Dutch (1) | |
| Knowledge in (4, 2.6%) | Understanding diagnosis and disease management (2, 1.3%) | Developed survey, English (1) Knowledge questionnaire derived from Miller (2008), English (1) |
| Managing chronic cancer pain (1, 0.6%) | PPQ, validated questionnaire, English (1) | |
| Medications and side effects (1, 0.6%) | Two items of study questionnaire, English (1) | |
| Self-efficacy (4, 2.6%) | - | NA (1) PAM, validated self-report questionnaire, Dutch (1) SEMCD 6, validated questionnaire, English (1) Two subscales of the study questionnaire (1) |
| Fatigue (3, 2.0%) | - | FACT-F, validated scale, Spanish (1) BFI-I, validated, English (1), French (1) |
| Health status (3, 2.0%) * | - | SF-12, validated questionnaire, English (1) 28-item retrospective survey, not validated, English (1) * HADS, validated questionnaire, English (1) EORTC QLQ-C30, validated questionnaire, English (1) |
| Activation (2, 1.3%) | - | 5-items of study specific questionnaire, Swedish (1) PAM, validated self-report questionnaire, Dutch (1) |
| Awareness of the importance of received intervention (2, 1.3%) | - | 11-point Likert-type scale, self-report questionnaire, Dutch (1) Ranking questionnaire, non-validated, English (1) |
| Clinical effectiveness of intervention delivered (2, 1.3%) | Capecitabine management (1, 0.6%) | Capecitabine dosing schedule, N of treatment modifications, N of response to treatment, N of adverse events, N of need for consultations with general practitioners (1) |
| Incidence of CRIs (1, 0.6%) | Clinical criteria and laboratory data of CRI (1) | |
| Oral care (2, 1.3%) | Oral situation (1, 0.6%) * | OAG, non-validated assessment tool, Swedish (1) * |
| Mucositis (1, 0.6%) | NA (1) | |
| Nausea and vomiting (2, 1.3%) | - | INVR, self-report validated instrument, English (1) NA (1) |
| Comfort (1, 0.6%) | - | Interview based on Katherine Kolcaba’s Theory of Comfort, analysed by content analysis |
| Concerns (1, 0.6%) | - | Semi-structured interview |
| Constipation and satisfaction with bowel movements (1, 0.6%) | - | Constipation and defecation, Roma III validated criteria, Chinese (1) Satisfaction with bowel movements, 3-degree score, Chinese (1) |
| Coping (1, 0.6%) | - | CBI, self-report validated questionnaire, Swedish |
| Cost (1, 0.6%) | - | Mean time to complete and review the protocol |
| Diarrhoea (1, 0.6%) | - | NA |
| Fall prevention (1, 0.6%) | - | Behaviour, NOC 3, classification, English |
| Nutrition (1, 0.6%) | - | NA |
| Patients’ assessment and care (1, 0.6%) | - | Standard JCI (nursing care is planned within 24 h from admittance, nursing care is tailored using the collected data, nursing plan is updated and modified based on patient reassessment) Standard JCI (patients’ needs are identified based on nursing and medical assessment and they are registered; all patients underwent a screening of pain; the patient is subjected to revaluation in order to determine the response to treatment; the patient is subjected to revaluation in order to plan for continuity of care; the patient is subjected to revaluation at appropriate intervals depending on the treatment plan and identified needs) |
| Perception of health-related information (1, 0.6%) | - | EORTC QLQ-INFO25, validated questionnaire, Swedish |
| Physiologic complications (1, 0.6%) | - | Presence of urinary tract infection, respiratory tract infection, skin/mucocutaneous infection, bleeding, febrile state, thrombophlebitis, or pulmonary embolus |
| Problem solving ability (1, 0.6%) | - | SPSI-R, validated questionnaire, Dutch |
| Safe medication administration (1, 0.6%) | - | NA |
| Sleep disturbance (1, 0.6%) | - | NA |
| Social support (1, 0.6%) | - | SSL, validated questionnaire, Dutch |
| Survival (1, 0.6%) | - | Time in days from enrolment in the study until death or last date known alive (1) |
| Tissue integrity (1, 0.6%) | - | Skin and mucous membrane, NOC 3, classification, English |
| Uncertainty (1, 0.6%) | - | MUIS-C, validated questionnaire, English (1) |
| Unplanned therapy interruption (1, 0.6%) | - | N of therapy interruptions from the patients’ diary and nurses’ records (1) |
| Use of sources of information (1, 0.6%) | - | Semi-structured interview (1) |
| ONS Outcomes Classification Exemplars | NSOs from Our Scoping Review (N, %) | Detailed ONS Outcomes from Our Scoping Review (n, %) |
|---|---|---|
| Symptom control and management | 44 (29.1) | |
| Pain | 10 (6.6) | Resolution/reduction of pain (7, 4.6%), Satisfaction with pain management (2, 1.3%), Knowledge in managing chronic cancer pain (1, 0.6%) |
| Altered skin or mucous membrane | 1 (0.6) | Tissue integrity (1, 0.6%) |
| Constipation | 1 (0.6) | Constipation and satisfaction with bowel movements (1, 0.6%) |
| Diarrhoea | 1 (0.6) | Diarrhoea (1, 0.6%) |
| Fatigue | 3 (2.0) | Fatigue (3, 2.0%) |
| Insomnia | 1 (0.6) | Sleep disturbance (1, 0.6%) |
| Nausea | 2 (1.3) | Nausea and vomiting (2, 1.3%) |
| Peripheral neuropathy | - | - |
| Anorexia | - | - |
| Breathlessness | - | - |
| Neutropenia | - | - |
| Other | 27 (17.9) | General therapy-related symptoms (8, 5.3%), Barriers and facilitators to intervention adherence/symptoms (5, 3.3%), Therapy-related symptom distress (3, 2.0%), Knowledge in understanding diagnosis and disease management (2, 1.3%), Clinical effectiveness of capecitabine management (1, 0.6%), Comfort (1, 0.6%), Mucositis (1, 0.6%), Oral care situation (1, 0.6%), Health status (3, 2.0%), Physiologic complications (1, 0.6%), Knowledge in medications and side effects (1, 0.6%) |
| Economic | 20 (13.2) | |
| Emergency room visits | 4 (2.6) | Emergency department visits (4, 2.6%) |
| Unexpected readmissions | 2 (1.3) | Readmissions/hospitalizations (2, 1.3%) |
| Length of stay | 1 (0.6) | Length of stay (1, 0.6%) |
| Out-of-pocket costs (family) | - | - |
| Homecare visits | 1 (0.6) | Homecare visits (1, 0.6%) |
| Costs per day per episode | 1 (0.6) | Costs (1, 0.6%) |
| Other | 11 (7.3) | Access to care (2, 1.3%), Timing of care process (4, 2.6%), Clinical appointments (2, 1.3%), Acceptability and accessibility of cancer services (1, 0.6%), Patient disposition at discharge (1, 0.6%), Referrals (1, 0.6%) |
| Functional status | 20 (13.2) | |
| Role functioning | 3 (2.0) | Functional status (3, 2.0%) |
| Ability to carry out usual activities | 1 (0.6) | Ability to function independently (1, 0.6%) |
| Nutritional status | 1 (0.6) | Nutrition (1, 0.6%) |
| Activities of daily living | - | - |
| Activity tolerance | - | - |
| Instrumental activities of daily living | - | - |
| Other | 15 (10.0) | Health-related quality of life (8, 5.3%), Self-efficacy (4, 2.6%), Activation (2, 1.3%), Self-care (1, 0.6%) |
| Psychological health status | 13 (8.6) | |
| Anxiety | 2 (1.3) | Anxiety (2, 1.3%) |
| Depression | 2 (1.3) | Depression (2, 1.3%) |
| Spiritual distress | - | - |
| Coping | 1 (0.6) | Coping (1, 0.6%) |
| Other | 8 (5.3) | Psychological distress in general (7, 4.6%), concerns (1, 0.6%) |
| Safety (preventable adverse events) | 4 (2.6) | |
| Infections | 1 (0.6) | CRIs (1, 0.6%), Urinary tract infection (1, 0.6%), Respiratory tract infection (1, 0.6%), Skin/mucocutaneous infection (1, 0.6%), Bleeding (1, 0.6%), Febrile state (1, 0.6%), Thrombophlebitis (1, 0.6%), or Pulmonary embolus (1, 0.6%) |
| Falls | 1 (0.6) | Fall prevention (1, 0.6%) |
| Skin ulcers | - | - |
| Extravasation incidents | 1 (0.6) | Safe medication administration (1, 0.6%) |
| Hypersensitive reactions | - | - |
| Other | 1 (0.6) | Unplanned therapy interruptions (1, 0.6%) |
| - | ||
| Other * | 50 (33.1) | Satisfaction with care received (19, 12.6%), Experiences and perceptions of care received (11, 7.2%), Quality of relationship with nurses (2, 1.3%), Quality of care received (5, 3.3%), Caring and uncaring behaviours (4, 2.6%), Awareness of the importance of received intervention (2, 1.3%), Patients’ assessment and care (1, 0.6%), Perception of health-related information (1, 0.6%), Problem solving ability (1, 0.6%), Social support (1, 0.6%), Survival (1, 0.6%), Uncertainty (1, 0.6%), Use of sources of information (1, 0.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visintini, C.; Palese, A. What Nursing-Sensitive Outcomes Have Been Investigated to Date among Patients with Solid and Hematological Malignancies? A Scoping Review. Nurs. Rep. 2023, 13, 1101-1125. https://doi.org/10.3390/nursrep13030096
Visintini C, Palese A. What Nursing-Sensitive Outcomes Have Been Investigated to Date among Patients with Solid and Hematological Malignancies? A Scoping Review. Nursing Reports. 2023; 13(3):1101-1125. https://doi.org/10.3390/nursrep13030096
Chicago/Turabian StyleVisintini, Chiara, and Alvisa Palese. 2023. "What Nursing-Sensitive Outcomes Have Been Investigated to Date among Patients with Solid and Hematological Malignancies? A Scoping Review" Nursing Reports 13, no. 3: 1101-1125. https://doi.org/10.3390/nursrep13030096
APA StyleVisintini, C., & Palese, A. (2023). What Nursing-Sensitive Outcomes Have Been Investigated to Date among Patients with Solid and Hematological Malignancies? A Scoping Review. Nursing Reports, 13(3), 1101-1125. https://doi.org/10.3390/nursrep13030096