Pursuing Sustainability for Healthcare through Digital Platforms




Abstract
:1. Introduction
2. Theoretical Background
2.1. A Systemic Approach to Healthcare Sustainability
2.2. The Role of ICTs and Digital Platforms for Healthcare Sustainability
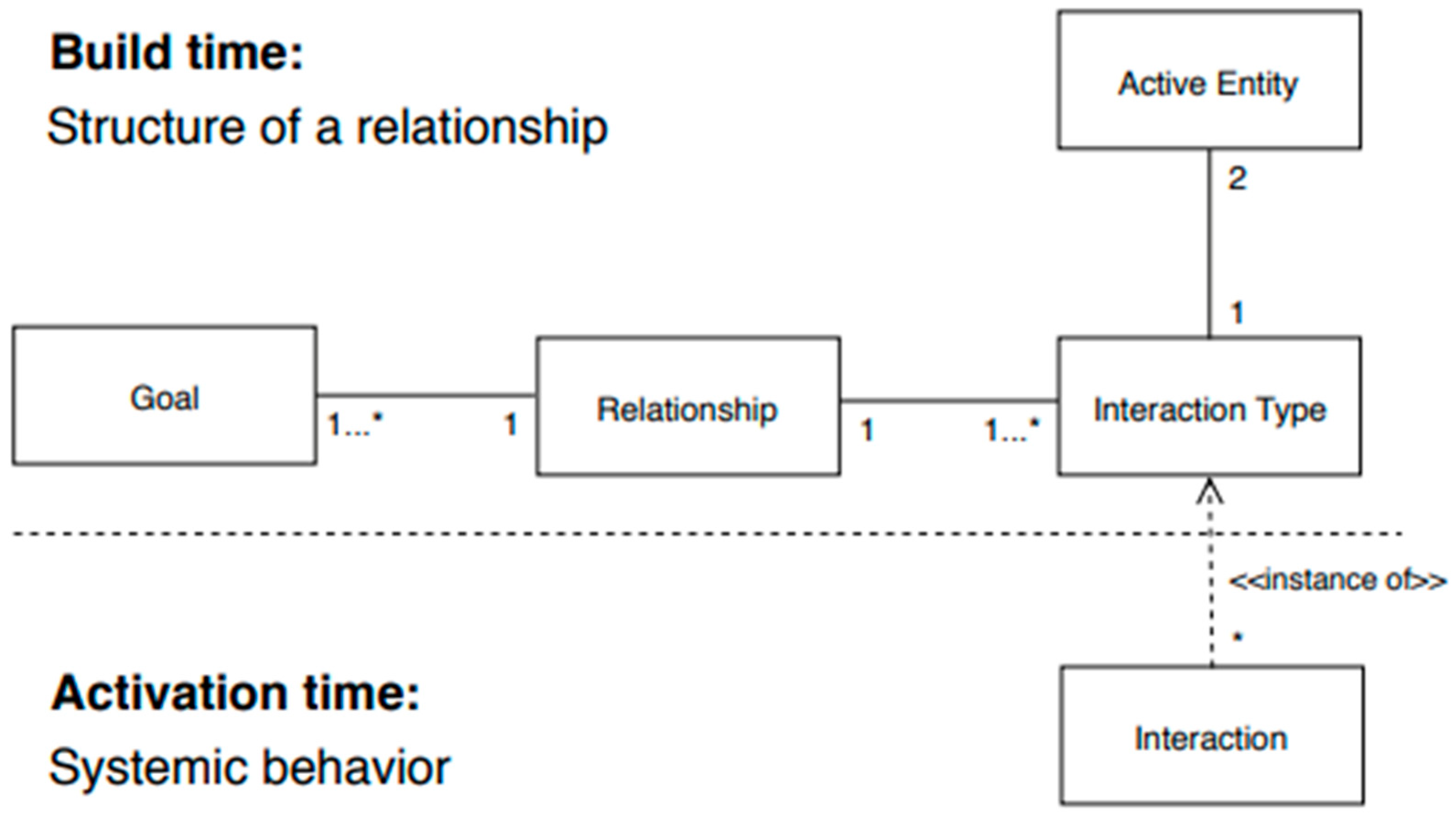
3. The Interaction Type as a Bridge between Relationship and Interaction: A Proposed Model
- Goal—something that individuals or organization try to do or to achieve;
- Active entity—an organization, an individual or even an automated component able to assume a specific behaviour when interacting with other active entities;
- Relationship—a logical or physical connection between the components of a structure or those relationships; thus, relationships, facilitating communication, make it possible to boost the interaction between active entities;
- Interaction—a concrete action involving at least two active entities and aiming to reach a specific and shared goal;
- Interaction type—the structural element that shapes a specific kind of interaction and which qualifies one or more interactions, offering them an external shape or configuration.
| appointment booking = {patient, doctor, to get an appointment, |
| “message for the appointment request”, |
| “to be in touch”}. |
| i1 = {mr. Brown, dr. White, to get an appointment, |
| “I have a stomach ache, please book me an appointment” |
| “mr. Brown and dr. White are in touch”}, |
| i2 = {mr. Brown, dr. White, to get an appointment, |
| “I feel sick, please book me an appointment” |
| “mr. Brown and dr. White are in touch”}. |
| aitName = {activeEntity1, activeEntity2, goal, setOfInteractionTypes, constraints} |
| medical examination = {patient, doctor, to solve a health problem, |
| {appointment booking, take a physical, medical report, payment} |
| select all}. |
| follow up = {patient, doctor, to monitor the patient health status, |
| “information about the progress of the therapeutic plan” |
| “to be in touch”}. |
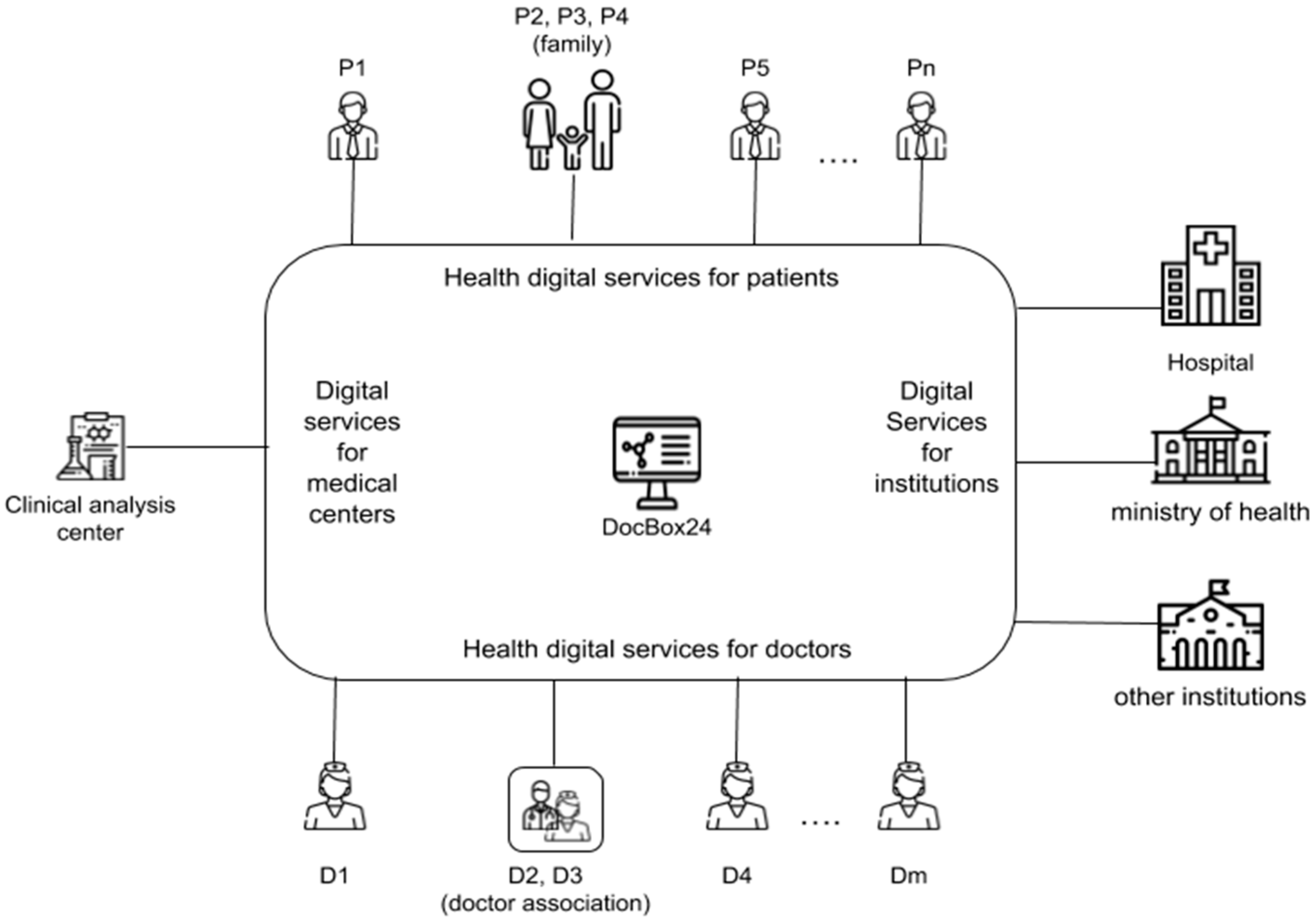
4. Designing and Implementing A Digital Platform for Healthcare Services Sustainability: A Prototype
- connecting physicians who work as freelancers with patients in a single application context;
- offering a complete set of digital services (e.g., booking, visit/report, follow up, etc.);
- provide an authorized access to health-related data to patients, physicians, public institutions and private health organizations;
- maintaining a single database, which can be used for predictive analysis through machine learning algorithms;
- integrating the existing or future digital, and even wearable, devices for data recording and analysis.
- -
- active entity 1—healthcare digital platform;
- -
- healthcare digital platform—active entity 2.
- patient-DocBox24, for appointment booking, initiator: patient
- DocBox24-doctor, for appointment request, initiator: DocBox24
- doctor-DocBox24, for appointment scheduling, initiator: doctor
- DocBox24-patient, to confirm the appointment, initiator: DocBox24
- (a)
- asynchronous interactions, which no longer need the simultaneous presence of all the active entities who participate in the interaction;
- (b)
- the ongoing improvement of the interaction, for example in terms of interactions’ number reduction, process efficiency and effectiveness, service cost reduction and similar;
- (c)
- (d)
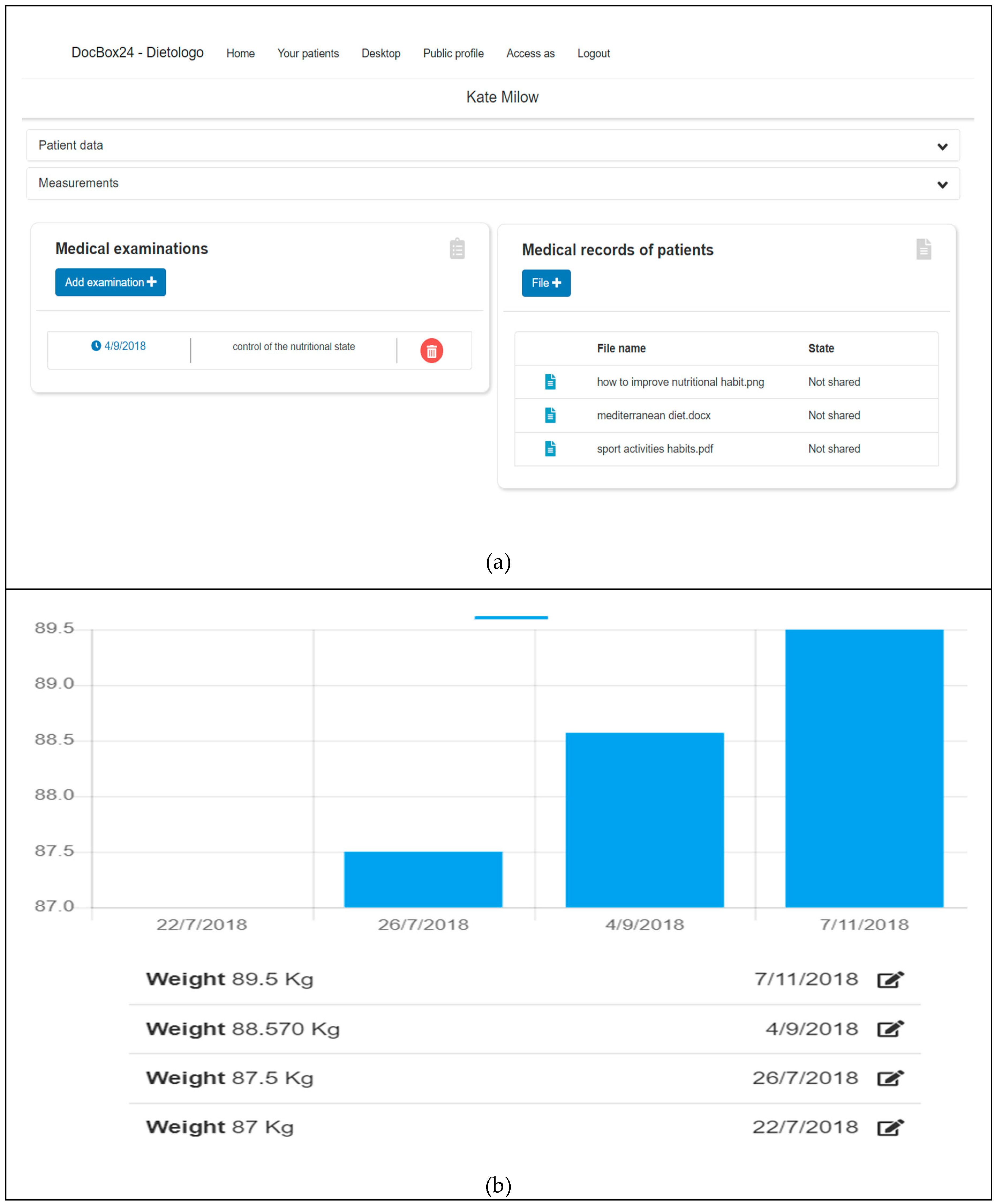
- the provision of new services, such as the cloud management of an electronic health record (EHR), based on ubiquitous, always available, but protected access;
- (e)
- the data collection and the subsequent statistical analysis and data mining.
| publish timetable = {doctor, DocBox24, |
| to publish the timetable for appointments in the next period, |
| “timetable” |
| “the doctor is registered in DocBox24 and can access its services”}. |
| appointment booking = {patient, DocBox24, |
| “select a free slot in the doctor timetable” |
| “the patient is connected to DocBox24”}. |
5. Discussions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brundtland, G. Our Common Future: Report of the 1987 World Commission on Environment and Development; United Nations: Oslo, Norway, 1987; pp. 1–59. [Google Scholar]
- Komiyama, H.; Takeuchi, K. Sustainability science: Building a new discipline. Sustain. Sci. 2006, 1, 1–6. [Google Scholar] [CrossRef]
- Pearce, D.W.; Markandya, A.; Barbier, E.B. Blueprint for a Green Economy; Earthscan: London, UK, 1989. [Google Scholar]
- Burger, P. Why any substantial definition of sustainability must fail–and why this is a good, not a bad story. In Proceedings of the 12th Annual International Sustainable Development Research Conference, Hong Kong, China, 6–8 April 2006. [Google Scholar]
- Armitage, D.R.; Plummer, R.; Berkes, F.; Arthur, R.I.; Charles, A.T.; Davidson-Hunt, I.J.; McConney, P. Adaptive co-management for social–ecological complexity. Front. Ecol. Environ. 2009, 7, 95–102. [Google Scholar] [CrossRef]
- Byrne, D. Complexity Theory and the Social Sciences: An Introduction; Routledge: London, UK, 2002. [Google Scholar]
- Barth, M.; Michelsen, G. Learning for change: An educational contribution to sustainability science. Sustain. Sci. 2013, 8, 103–119. [Google Scholar] [CrossRef]
- Bogdanov, A.A. Theory of Organization, or Tektology, 1996 ed.; Dudley P. Centre for: Castlegate, UK, 1913. [Google Scholar]
- Von Bertalanffy, L. General System Theory; Wiley: New York, NY, USA, 1968. [Google Scholar]
- Golinelli, G.M. Viable Systems Approach (VSA): Governing Business Dynamics; Cedam: Padova, Italy, 2010. [Google Scholar]
- Barile, S.; Saviano, M. Foundations of Systems Thinking: The Structure-System Paradigm. In Various Authors, Contributions to Theoretical and Practical Advances in Management. A Viable Systems Approach (VSA). ASVSA, Associazione per la Ricerca sui Sistemi Vitali; International Printing: Avellino, Italy, 2011; pp. 1–24. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2044579 (accessed on 21 December 2018).
- Saviano, M.; Barile, S.; Spohrer, J.C.; Caputo, F. A service research contribution to the global challenge of sustainability. J. Serv. Theory Pract. 2017, 27, 951–976. [Google Scholar] [CrossRef]
- Palumbo, R. The Bright Side and the Dark Side of Patient Empowerment: Co-Creation and Co-Destruction of Value in the Healthcare Environment; Springer: London, UK, 2017. [Google Scholar]
- Nota, G.; Aiello, R. The interaction type approach to relationships management. J. Ambient Intell. Hum. Comput. 2017, 1–15. [Google Scholar] [CrossRef]
- Chaudhry, B.; Wang, J.; Wu, S.; Maglione, M.; Mojica, W.; Roth, E.; Shekelle, P.G. Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care. Ann. Internal Med. 2006, 144, 742–752. [Google Scholar] [CrossRef]
- Seiffert, M.E.B.; Loch, C. Systemic thinking in environmental management: Support for sustainable development. J. Clean. Prod. 2005, 13, 1197–1202. [Google Scholar] [CrossRef]
- Valente, T.W. Network interventions. Science 2012, 337, 49–53. [Google Scholar] [CrossRef]
- Begun, J.W.; Zimmerman, B.; Dooley, K. Health care organizations as complex adaptive systems. Adv. Health Care Organ. Theory 2003, 253, 288. [Google Scholar]
- World Health Organization (WHO). The World Health Report 2000. Health Systems: Improving Performance; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Navarro-Espigares, J.L.; Martín-Segura, J.A.; Hernández-Torres, E. The role of the service sector in regional economic resilience. Serv. Ind. J. 2012, 32, 571–590. [Google Scholar] [CrossRef] [Green Version]
- Ioannou, I.; Serafeim, G. The Consequences of Mandatory Corporate Sustainability Reporting; Harvard Business School Research, Working Paper No. 11-100; Harvard Business School Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Christopher, W.F. Holistic Management: Managing What Matters for Company Success; John Wiley & Sons: New York, NY, USA, 2007; Volume 46. [Google Scholar]
- Espinosa, A.; Porter, T. Sustainability, complexity and learning: Insights from complex systems approaches. Learn. Organ. 2011, 18, 54–72. [Google Scholar] [CrossRef]
- Barile, S.; Saviano, M. Complexity and sustainability in management: Insights from a systems perspective. In Social Dynamics in a Systems Perspective; Springer: Cham, Switzerland, 2018; pp. 39–63. [Google Scholar]
- Fiksel, J. Sustainability and resilience: Toward a systems approach. Sustain. Sci. Pract. Policy 2006, 2, 14–21. [Google Scholar] [CrossRef]
- Beer, S. Brain of the Firm: A Development in Management Cybernetics; Herder and Herder: New York, NY, USA, 1972. [Google Scholar]
- Aquino, R.P.; Barile, S.; Grasso, A.; Saviano, M. Envisioning smart and sustainable healthcare: 3D Printing technologies for personalized medication. Futures 2018. [Google Scholar] [CrossRef]
- Golinelli, G.M.; Gatti, M. The Firm as a Viable System. Symphonya Emerg. Issue Mang 2001, 2, 38–63. [Google Scholar] [CrossRef]
- Barile, S.; Lusch, R.; Reynoso, J.; Saviano, M.; Spohrer, J. Systems, networks, and ecosystems in service research. J. Serv. Manag. 2016, 27, 652–674. [Google Scholar] [CrossRef]
- IFM, IBM. Succeeding Through Service Innovation: A Service Perspective for Education, Research, Business and Government; University of Cambridge Institute for Manufacturing: Cambridge, UK, 2008. [Google Scholar]
- Reynoso, J.; Barile, S.; Saviano, M.; Spohrer, J. Service Systems, Networks, and Ecosystems: Connecting the Dots Concisely from a Systems Perspective1; The SAGE Handbook of Service-Dominant Logic; SAGE: Thousand Oaks, CA, USA, 2018; p. 241. [Google Scholar]
- Polese, F.; Capunzo, M. The determinants of translational medicine success—A managerial contribution. Transl. Med. 2013, 6, 29. [Google Scholar]
- Saviano, M.; Bassano, C.; Calabrese, M. A VSA-SS approach to healthcare service systems the triple target of efficiency, effectiveness and sustainability. Serv. Sci. 2010, 2, 41–61. [Google Scholar] [CrossRef]
- Lipsitz, L.A. Understanding health care as a complex system: The foundation for unintended consequences. JAMA 2012, 308, 243–244. [Google Scholar] [CrossRef]
- Oudshoorn, A. Client-Provider Relationships in a Community Health Clinic for People Experiencing Homelessness: A Critical Ethnography. Ph.D. Thesis, University of Western Ontario, London, ON, Canada, 2011; p. 107. [Google Scholar]
- Rathert, C.; Wyrwich, M.D.; Boren, S.A. Patient-centered care and outcomes: A systematic review of the literature. Med. Care Res. Rev. 2013, 70, 351–379. [Google Scholar] [CrossRef]
- Prigge, J.K.; Dietz, B.; Homburg, C.; Hoyer, W.D.; Burton, J.L. Patient empowerment: A cross-disease exploration of antecedents and consequences. Int. J. Res. Mark. 2015, 32, 375–386. [Google Scholar] [CrossRef]
- Barile, S.; Saviano, M.; Polese, F. Information asymmetry and co-creation in health care services. AMJ 2014, 22, 205–217. [Google Scholar] [CrossRef]
- Naaranoja, M.; Uden, L. Why Co-creation of Value May Not Work? In International Conference on Knowledge Management in Organizations; Springer: Cham, Switzerland, 2014; pp. 362–372. [Google Scholar]
- Polese, F.; Mele, C.; Gummesson, E. Value co-creation as a complex adaptive process. J. Serv. Theory Pract. 2017, 27, 926–929. [Google Scholar] [CrossRef]
- Carlsson, L.; Berkes, F. Co-management: Concepts and methodological implications. J. Environ. Manag. 2005, 75, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Caputo, F.; Buhnova, B.; Walletzký, L. Investigating the role of smartness for sustainability: Insights from the Smart Grid domain. Sustain. Sci. 2018, 1–11. [Google Scholar] [CrossRef]
- Berry, L.L.; Bendapudi, N. Health care: A fertile field for service research. J. Serv. Res. 2007, 10, 111–122. [Google Scholar] [CrossRef]
- Holmes, M.V.; Shah, T.; Vickery, C.; Smeeth, L.; Hingorani, A.D.; Casas, J.P. Fulfilling the promise of personalized medicine? Systematic review and field synopsis of pharmacogenetic studies. PLoS ONE 2009, 4, e7960. [Google Scholar] [CrossRef] [PubMed]
- Walczak, M. Models of the emergence and diffusion of mass customization. Procedia Soc. Behav. Sci. 2014, 110, 812–821. [Google Scholar]
- Skinner, R.I. The value of information technology in healthcare/reply. Front. Health Serv. Manag. 2003, 19, 3–15. [Google Scholar] [CrossRef]
- Realpe, A.; Wallace, L.M. What Is Co-Production; The Health Foundation: London, UK, 2010; pp. 1–11. [Google Scholar]
- Grunwald, A. Technology Assessment and Policy Advice in the Field of Sustainable Development. In Technology, Society and Sustainability; Springer: Cham, Switzerland, 2017; pp. 203–221. [Google Scholar]
- Spohrer, J.; Maglio, P.P.; Bailey, J.; Gruhl, D. Steps toward a science of service systems. Computer 2007, 40. [Google Scholar] [CrossRef]
- Rumbaugh, J.; Jacobson, I.; Booch, G. Unified Modeling Language Reference Manual; Pearson Higher Education: New York, NY, USA, 2004. [Google Scholar]
- Barile, S.; Polese, F. Smart service systems and viable service systems: Applying systems theory to service science. Serv. Sci. 2010, 2, 21–40. [Google Scholar] [CrossRef]
- Breidbach, C.F.; Maglio, P.P. Technology-enabled value co-creation: An empirical analysis of actors, resources, and practices. Ind. Mark. Manag. 2016, 56, 73–85. [Google Scholar] [CrossRef]
- Lusch, R.F.; Nambisan, S. Service innovation: A service-dominant logic perspective. MIS Q. 2015, 39, 155–176. [Google Scholar] [CrossRef]
- Yoo, Y.; Boland, R.J., Jr.; Lyytinen, K.; Majchrzak, A. Organizing for innovation in the digitized world. Organ. Sci. 2012, 23, 1398–1408. [Google Scholar] [CrossRef]
- Beirão da Veiga, L.; Brezzi, F.; Marini, L.D.; Russo, A. Virtual element method for general second-order elliptic problems on polygonal meshes. Math. Models Meth. Appl. Sci. 2016, 26, 729–750. [Google Scholar] [CrossRef]
- Barrett, M.; Davidson, E.; Prabhu, J.; Vargo, S.L. Service innovation in the digital age: Key contributions and future directions. MIS Q. 2015, 39, 135–154. [Google Scholar] [CrossRef]
- Patrício, L.; de Pinho, N.F.; Teixeira, J.G.; Fisk, R.P. Service Design for Value Networks: Enabling Value Cocreation Interactions in Healthcare. Serv. Sci. 2018, 10, 76–97. [Google Scholar] [CrossRef]
- Vargo, S.L.; Maglio, P.P.; Akaka, M.A. On value and value co-creation: A service systems and service logic perspective. Eur. Mang. J. 2008, 26, 145–152. [Google Scholar] [CrossRef]
- Kongstvedt, P.R. (Ed.) The Managed Health Care Handbook; Jones & Bartlett Learning: London, UK, 2001. [Google Scholar]
- Storbacka, K.; Brodie, R.J.; Böhmann, T.; Maglio, P.P.; Nenonen, S. Actor engagement as a micro foundation for value co-creation. J. Bus. Res. 2016, 69, 3008–3017. [Google Scholar] [CrossRef]
- Palumbo, R.; Cosimato, S.; Tommasetti, A. Dream or reality? A recipe for sustainable and innovative health care ecosystems. TQM J. 2017, 29, 847–862. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Aggregate Interaction Types | |||||
|---|---|---|---|---|---|
| Relationship | Interaction Type Name | Goal | Set of Interaction Types | Constraint | Initiator |
| patient-doctor | medical examination | solve a health problem | appointment booking take a physical medical report payment | select all | patient |
| patient-analysis centre | clinical analysis | to get clinical examination | appointment booking payment clinical examination clinical report | select all | patient |
| hospital-family | vaccination | vaccination campaign | call for vaccination make a vaccine | a family member is responsible for the hospital-family relationship, select all | hospital |
| doctor1-doctor2 | consultation | to get an appointment for a further specialist examination | appointment booking clinical history clinical examination clinical report | select all | doctor 1 |
| Simple Interaction Types | |||||
|---|---|---|---|---|---|
| Relationship | Interaction Type Name | Goal | Message | Constraint | Initiator |
| patient-doctor | appointment booking | to get an appointment | message for appointment request | to be in touch | patient |
| patient-doctor | symptoms | to describe the health status | message for the description of symptoms | to be in touch | patient |
| patient-doctor | medical report | to produce a medical report for the patient | message that describes the health problem and the therapeutic plan | to be in touch | doctor |
| patien1-patient2 | information sharing | provide mutual assistance to face everyday diseases problems | message with experience sharing | patien1 and patient2 wish to share information | patient1 or patient2 |
| doctor-Department of Health | data transmission | sending data about the provided treatments | data sending | select all | doctor |
| Simple Interaction Types for the Management of an EHR in a Cloud Environment | |||||
|---|---|---|---|---|---|
| Relationship | Interaction Type Name | Goal | Message | Constraint | Initiator |
| patient-DocBox24 | Electronic Health Record1 | The patient manages his online health data and medical reports | data to manage the EHR | the patient is connected to DocBox24 | patient |
| doctor-DocBox24 | Electronic Health Record2 | The doctor manages online data and medical reports for his patients | data to manage the patient EHR | the doctor is connected to DocBox24 | doctor |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faggini, M.; Cosimato, S.; Nota, F.D.; Nota, G. Pursuing Sustainability for Healthcare through Digital Platforms. Sustainability 2019, 11, 165. https://doi.org/10.3390/su11010165
Faggini M, Cosimato S, Nota FD, Nota G. Pursuing Sustainability for Healthcare through Digital Platforms. Sustainability. 2019; 11(1):165. https://doi.org/10.3390/su11010165
Chicago/Turabian StyleFaggini, Marisa, Silvia Cosimato, Francesco David Nota, and Giancarlo Nota. 2019. "Pursuing Sustainability for Healthcare through Digital Platforms" Sustainability 11, no. 1: 165. https://doi.org/10.3390/su11010165
APA StyleFaggini, M., Cosimato, S., Nota, F. D., & Nota, G. (2019). Pursuing Sustainability for Healthcare through Digital Platforms. Sustainability, 11(1), 165. https://doi.org/10.3390/su11010165