Sex Differences and Psychological Factors Associated with General Health Examinations Participation: Results from a Vietnamese Cross-Section Dataset

 ,
, 
 , , and
, , and
Abstract
:1. Introduction
1.1. On General Health Examinations
1.2. Sex and Psychological Differences Involved in Health Behaviors
1.3. Psychological Factors and GHEs Participation
2. Materials and Methods
2.1. Sample
2.2. Procedures
2.3. Measures
- (i)
- The probability of a person hesitant to take periodic general health examination due to fear of discovering one’s disease (coded as “DiscDisease”) against sex (“Sex”) and whether their friends or family have gone through long-term treatment (“AcqTrmt”);
- (ii)
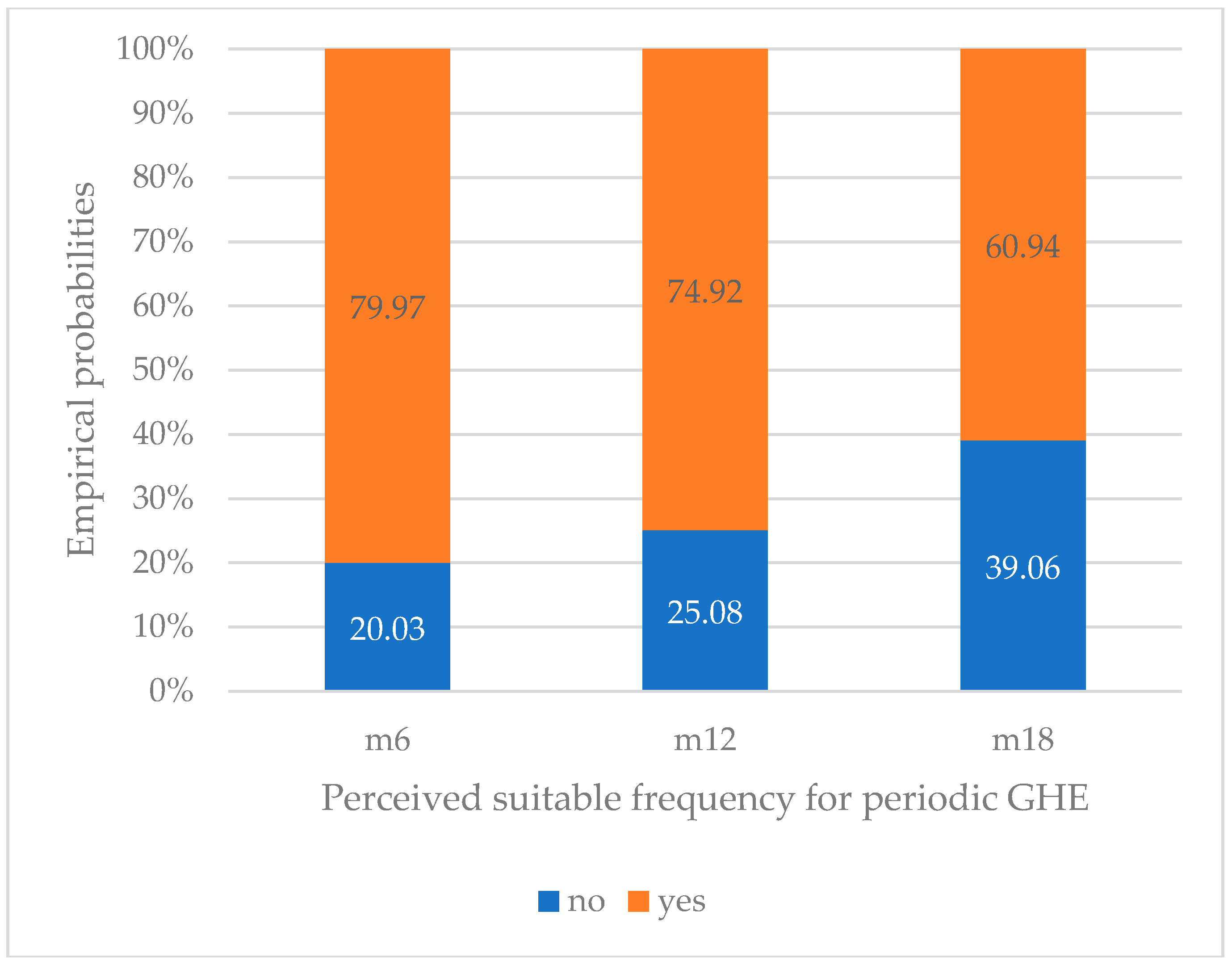
- The probability of perceived appropriate periodic GHE frequency (6 months, 12 months, ≥18 months) (“SuitFreq”) against the time since their last visit to a doctor (“RecExam”) and the fear of diseases detection (“DiscDisease”).
2.4. Analysis
− 1.085 × unknown.RecExam − 0.838 × yes.DiscDisease
− 1.553 × unknown.RecExam − 0.594 × yes.DiscDisease
3. Results
3.1. Fear of Disease Detection in GHE Decisions
3.2. Correlates of Perception on the Appropriate GHE Frequencies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data availability
References
- Holland, W. Periodic health examination: History and critical assessment. EuroHealth 2009, 15, 16–20. [Google Scholar]
- Roberts, N.T. The values and limitations of periodic health examinations. J. Chronic Dis. 1959, 9, 95–116. [Google Scholar] [CrossRef]
- Dobell, H. Lectures on the Germs and Vestiges of Disease, and on the Prevention of the Invasion and Fatality of Disease by Periodical Examinations. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5180312/pdf/brforeignmcrev72757-0171.pdf (accessed on 18 January 2018).
- Emerson, H. Periodic medical examinations of apparently healthy persons. JAMA J. Am. Med. Assoc. 1923, 80, 1376. [Google Scholar] [CrossRef]
- Han, P.K.J. Historical Changes in the Objectives of the Periodic Health Examination. Ann. Intern. Med. 1997, 127, 910. [Google Scholar] [CrossRef]
- Oboler, S.K.; Prochazka, A.V.; Gonzales, R.; Xu, S.; Anderson, R.J. Public Expectations and Attitudes for Annual Physical Examinations and Testing. Ann. Intern. Med. 2002, 136, 652. [Google Scholar] [CrossRef]
- Zielhuis, G.A. Are periodic school health examinations worthwhile? Health Policy 1985, 5, 241–253. [Google Scholar] [CrossRef]
- Wu, H.-Y.; Yang, L.-L.; Zhou, S. Impact of periodic health examination on surgical treatment for uterine fibroids in Beijing: A case-control study. BMC Health Serv. Res. 2010, 10. [Google Scholar] [CrossRef]
- Burton, L.C.; Steinwachs, D.M.; German, P.S.; Shapiro, S.; Brant, L.J.; Richards, T.M.; Clark, R.D. Preventive services for the elderly: Would coverage affect utilization and costs under Medicare? Am. J. Public Health 1995, 85, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, N.; Tatara, K.; Fujiwara, H. Do preventive health services reduce eventual demand for medical care? Soc. Sci. Med. 1996, 43, 999–1005. [Google Scholar] [CrossRef]
- Vuong, Q. The financial economy of Viet Nam in an age of reform, 1986–2016. In Routledge Handbook of Banking and Finance in Asia; Volz, U., Morgan, P., Yoshino, N., Eds.; Routledge T&F: London, UK, 2019. [Google Scholar]
- Vuong, Q.-H.; Vu, Q.-H.; Vuong, T.-T. What makes Vietnamese (not) attend periodic general health examinations? A 2016 cross-sectional study. Osong Public Health Res. Perspect. 2017, 8, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Vuong, Q.H. Be rich or don’t be sick: Estimating Vietnamese patients’ risk of falling into destitution. SpringerPlus 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Fineberg, H.V. A Successful and Sustainable Health System—How to Get There from Here. N. Engl. J. Med. 2012, 366, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- International Cooperation Department. Labour Codes, General Labour and Employment Acts; Ministry of Labour, Official Gazette: Hanoi, Vietnam, 2012; Volume 2012, pp. 48–78. [Google Scholar]
- LĐO. Kham Suc Khoe Dinh Ky Cho Vui [Periordic Health Check-Ups for Fun]. Available online: https://laodong.vn/suc-khoe/kham-suc-khoe-dinh-ky-cho-vui-584383.ldo (accessed on 25 December 2018).
- Nupponen, R. Client views on periodic health examinations: Opinions and personal experience. J. Adv. Nurs. 1996, 23, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Liang, W. A population-based study of age and gender differences in patterns of health-related behaviors. Am. J. Prev. Med. 1999, 17, 8–17. [Google Scholar] [CrossRef]
- Pinkhasov, R.M.; Wong, J.; Kashanian, J.; Lee, M.; Samadi, D.B.; Pinkhasov, M.M.; Shabsigh, R. Are men shortchanged on health? Perspective on health care utilization and health risk behavior in men and women in the United States. Int. J. Clin. Pract. 2010, 64, 475–487. [Google Scholar] [CrossRef]
- Waldron, I. Sex differences in illness incidence, prognosis and mortality: Issues and evidence. Soc. Sci. Med. 1983, 17, 1107–1123. [Google Scholar] [CrossRef]
- Cleary, P.D.; Mechanic, D.; Greenley, J.R. Sex Differences in Medical Care Utilization: An Empirical Investigation. J. Health Soc. Behav. 1982, 23, 106. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, J.H.; Pope, C.R. Gender roles, illness orientation and use of medical services. Soc. Sci. Med. 1983, 17, 129–137. [Google Scholar] [CrossRef]
- Verbrugge, L.M.; Wingard, D.L.; Features Submission, H.C. Sex Differentials in Health and Mortality. Women Health 1987, 12, 103–145. [Google Scholar] [CrossRef]
- Courtenay, W.H. Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Soc. Sci. Med. 2000, 50, 1385–1401. [Google Scholar] [CrossRef]
- Woodwell, D. National Ambulatory Medical Care Survey, 1996. In ICPSR Data Holdings; Inter-University Consortium for Political and Social Research (ICPSR): California, CA, USA, 1998. [Google Scholar]
- United Nations Statistics Division. Demographic Yearbook 2003. Available online: https://unstats.un.org/unsd/demographic-social/products/dyb/dybsets/2003%20DYB.pdf (accessed on 18 January 2019).
- Kung, H.-C.; Hoyert, D.L.; Xu, J.; Murphy, S.L. Deaths: Final data for 2005. Natl. Vital. Stat. Rep. 2008, 56, 1–120. [Google Scholar] [PubMed]
- Publications S.S.O.A. Actuarial Studies. Available online: http://www.ssa.gov/OACT/NOTES/actstud.html (accessed on 24 May 2018).
- Davies, J.; McCrae, B.P.; Frank, J.; Dochnahl, A.; Pickering, T.; Harrison, B.; Zakrzewski, M.; Wilson, K. Identifying Male College Students’ Perceived Health Needs, Barriers to Seeking Help, and Recommendations to Help Men Adopt Healthier Lifestyles. J. Am. Coll. Health 2000, 48, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Dawson, K.A.; Schneider, M.A.; Fletcher, P.C.; Bryden, P.J. Examining gender differences in the health behaviors of Canadian university students. J. R. Soc. Promot. Health 2007, 127, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Jepson, R.; Clegg, A.; Forbes, C.; Lewis, R.; Sowden, A.; Kleijnen, J. The determinants of screening uptake and interventions for increasing uptake: A systematic review. Health Technol. Assess 2000, 4, 1–133. [Google Scholar]
- Van Wijk, C.M.T.G.; Kolk, A.M. Sex differences in physical symptoms: The contribution of symptom perception theory. Soc. Sci. Med. 1997, 45, 231–246. [Google Scholar] [CrossRef]
- Franks, P.; Clancy, C.M.; Gold, M.R.; Nutting, P.A. Health insurance and subjective health status: Data from the 1987 National Medical Expenditure survey. Am. J. Public Health 1993, 83, 1295–1299. [Google Scholar] [CrossRef]
- Sullivan, T.J.; Andersen, R.; Lion, J.; Anderson, O.W. Two Decades of Health Services: Social Survey Trends in Use and Expenditure. Soc. Forces 1978, 56, 970. [Google Scholar] [CrossRef]
- Addis, M.E.; Mahalik, J.R. Men, masculinity, and the contexts of help seeking. Am. Psychol. 2003, 58, 5–14. [Google Scholar] [CrossRef]
- Mahedy, L.; Todaro-Luck, F.; Bunting, B.; Murphy, S.; Kirby, K. Risk factors for psychological distress in Northern Ireland. Int. J. Soc. Psychiatry 2012, 59, 646–654. [Google Scholar] [CrossRef]
- Vuong, Q.-H.; Vuong, T.-T.; Ho, T.; Nguyen, H. Psychological and Socio-Economic Factors Affecting Social Sustainability through Impacts on Perceived Health Care Quality and Public Health: The Case of Vietnam. Sustainability 2017, 9, 1456. [Google Scholar] [CrossRef]
- Ladwig, K.-H.; Marten-Mittag, B.; Formanek, B.; Dammann, G. Gender differences of symptom reporting and medical health care utilization in the German population. Eur. J. Epidemiol. 2000, 16, 511–518. [Google Scholar] [CrossRef]
- Jianakoplos, N.A.; Bernasek, A. Are women more risk averse? Econ. Inq. 1998, 36, 620–630. [Google Scholar] [CrossRef]
- Croson, R.; Gneezy, U. Gender Differences in Preferences. J. Econ. Lit. 2009, 47, 448–474. [Google Scholar] [CrossRef] [Green Version]
- Donna, R. Women Are Better Retirement Savers than Men, But Still Have a Lot Less Money. Available online: http://time.com/money/3911377/retirement-401ks-women-men/ (accessed on 18 January 2019).
- Lucy, B. The Truth about Our Economy’s Gender Divide? Women Are Saving More Money—But They Won’t Invest. Available online: http://www.independent.co.uk/voices/the-truth-about-our-economys-gender-divide-women-save-more-money-but-they-wont-invest-a6942596.html (accessed on 21 May 2018).
- Wennman-Larsen, A.; Tishelman, C. Advanced home care for cancer patients at the end of life: A qualitative study of hopes and expectations of family caregivers. Scand. J. Caring Sci. 2002, 16, 240–247. [Google Scholar] [CrossRef]
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Skinner, C.; Tiro, J.; Champion, V. The health belief model. In Health Behavior: Theory, Research, and Practice, 5th ed.; Glanz, K., Rimer, B., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015. [Google Scholar]
- Wall, M.; Teeland, L. Non-participants in a preventive health examination for cardiovascular disease: Characteristics, reasons for non-participation, and willingness to participate in the future. Scand. J. Prim. Health Care 2004, 22, 248–251. [Google Scholar] [CrossRef]
- Dryden, R.; Williams, B.; McCowan, C.; Themessl-Huber, M. What do we know about who does and does not attend general health checks? Findings from a narrative scoping review. BMC Public Health 2012, 12. [Google Scholar] [CrossRef]
- Burton, L.C.; German, P.S.; Shapiro, S. A Preventive Services Demonstration. Med. Care 1997, 35, 1149–1157. [Google Scholar] [CrossRef]
- Boland, B.J.; Wollan, P.C.; Silverstein, M.D. Yield of laboratory tests for case-finding in the ambulatory general medical examination. Am. J. Med. 1996, 101, 142–152. [Google Scholar] [CrossRef]
- Vuong, Q.-H. Survey data on Vietnamese propensity to attend periodic general health examinations. Sci. Data 2017, 4, 170142. [Google Scholar] [CrossRef] [Green Version]
- Vuong, Q.-H.; Ho, T.-M.; Nguyen, H.-K.; Vuong, T.-T. Healthcare consumers’ sensitivity to costs: A reflection on behavioural economics from an emerging market. Palgrave Commun. 2018, 4. [Google Scholar] [CrossRef]
- Vuong, Q.-H.; La, V.-P.; Vuong, T.-T.; Ho, M.-T.; Nguyen, H.-K.T.; Nguyen, V.-H.; Pham, H.-H.; Ho, M.-T. An open database of productivity in Vietnam’s social sciences and humanities for public use. Sci. Data 2018, 5, 180188. [Google Scholar] [CrossRef] [PubMed]
- Agresti, A. Categorical Data Analysis; John Wiley & Sons, Inc.: New York, NY, USA, 2002. [Google Scholar]
- Vuong, Q.; Nguyen, T. Vietnamese patients’ choice of healthcare provider: In search of quality information. Int. J. Behav. Healthcare Res. 2015, 5, 184–212. [Google Scholar] [CrossRef]
- Kuo, R.N.; Lai, M.-S. The influence of socio-economic status and multimorbidity patterns on healthcare costs: A six-year follow-up under a universal healthcare system. Int. J. Equity Health 2013, 12, 69. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Chen, Y.; Tong, X.; Feng, Z.; Wei, L.; Zhou, D.; Tian, M.; Lv, B.; Feng, D. The use of annual physical examinations among the elderly in rural China: A cross-sectional study. BMC Health Serv. Res. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Horner, S.D.; Ambrogne, J.; Coleman, M.A.; Hanson, C.; Hodnicki, D.; Lopez, S.A.; Talmadge, M.C. Traveling for Care: Factors Influencing Health Care Access for Rural Dwellers. Public Health Nurs. 1994, 11, 145–149. [Google Scholar] [CrossRef]
- Vuong, Q.-H.; Bui, Q.-K.; La, V.-P.; Vuong, T.-T.; Nguyen, V.-H.T.; Ho, M.-T.; Nguyen, H.-K.T.; Ho, M.-T. Cultural additivity: Behavioural insights from the interaction of Confucianism, Buddhism and Taoism in folktales. Palgrave Commun. 2018, 4, 143. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N | Percentage (%) |
|---|---|---|
| Age | ||
| <30 | 1306 | 63.15 |
| 30–49 | 643 | 31.09 |
| ≥50 | 119 | 5.76 |
| Sex (“Sex”) | ||
| Male | 728 | 35.2 |
| Female | 1340 | 64.8 |
| Hesitation due to possible discovery of diseases (“DiscDisease”) | ||
| Yes | 483 | 23.36 |
| No | 1585 | 76.64 |
| Time since the most recent visit to doctor (“RecExam”) | ||
| Less than 12 months | 1373 | 66.39 |
| From 12 to 24 months | 200 | 9.67 |
| Above 24 months | 125 | 6.05 |
| Unknown | 370 | 17.89 |
| Having friends under long-term treatments (“AcqTrmt”) | ||
| Yes | 917 | 44.34 |
| Never | 1151 | 55.66 |
| Perceived suitable periodic GHE frequency (“SuitFreq”) | ||
| Every 6 months | 1238 | 59.86 |
| Every 12 months | 638 | 30.85 |
| ≥18 months | 192 | 9.28 |
| Intercept | “Sex” | “AcqTrmt” | |
|---|---|---|---|
| “Male” | “Yes” | ||
| β0 | β1 | β2 | |
| logit(yes|no) | −1.155 *** (−14.573) | −0.409 *** (−3.602) | 0.221 * (2.110) |
| “RecExam” | “DiscDisease” | ||||
|---|---|---|---|---|---|
| Intercept | “less12” | “g24” | “unknown” | “Yes” | |
| β0 | β1 | β2 | β3 | β4 | |
| logit(m6|m18) | 2.026 *** (7.495) | 0.854 ** (2.937) | −0.588 (−1.620) | −1.085 *** (−3.741) | −0.838 *** (−4.862) |
| logit(m12|m18) | 1.793 *** (6.540) | 0.277 (0.937) | −0.865 * (−2.307) | −1.553 *** (−5.170) | −0.594 ** (−3.276) |
| “DiscDisease” | “Yes” | “No” | ||
|---|---|---|---|---|
| “AcqTrmt”|”Sex” | “Male” | “Female” | “Male” | “Female” |
| “Yes” | 0.207 | 0.282 | 0.793 | 0.718 |
| “Never” | 0.173 | 0.240 | 0.827 | 0.760 |
| “SuitFreq” | “m6” | |||
| “DiscDisease”| “RecExam” | “less12” | “b1224” | “g24” | “unknown” |
| “yes” | 0.589 | 0.432 | 0.432 | 0.394 |
| “no” | 0.666 | 0.520 | 0.544 | 0.530 |
| “SuitFreq” | “m12” | |||
| “DiscDisease”| “RecExam” | “less12” | “b1224” | “g24” | “unknown” |
| “yes” | 0.334 | 0.437 | 0.331 | 0.250 |
| “no” | 0.296 | 0.412 | 0.327 | 0.263 |
| “SuitFreq” | “m18” | |||
| “DiscDisease”| “RecExam” | “less12” | “b1224” | “g24” | “unknown” |
| “yes” | 0.077 | 0.131 | 0.237 | 0.356 |
| “no” | 0.038 | 0.068 | 0.129 | 0.207 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vuong, Q.-H.; Nghiem, K.-C.P.; La, V.-P.; Vuong, T.-T.; Nguyen, H.-K.T.; Ho, M.-T.; Tran, K.; Khuat, T.-H.; Ho, M.-T. Sex Differences and Psychological Factors Associated with General Health Examinations Participation: Results from a Vietnamese Cross-Section Dataset. Sustainability 2019, 11, 514. https://doi.org/10.3390/su11020514
Vuong Q-H, Nghiem K-CP, La V-P, Vuong T-T, Nguyen H-KT, Ho M-T, Tran K, Khuat T-H, Ho M-T. Sex Differences and Psychological Factors Associated with General Health Examinations Participation: Results from a Vietnamese Cross-Section Dataset. Sustainability. 2019; 11(2):514. https://doi.org/10.3390/su11020514
Chicago/Turabian StyleVuong, Quan-Hoang, Kien-Cuong P. Nghiem, Viet-Phuong La, Thu-Trang Vuong, Hong-Kong T. Nguyen, Manh-Toan Ho, Kien Tran, Thu-Hong Khuat, and Manh-Tung Ho. 2019. "Sex Differences and Psychological Factors Associated with General Health Examinations Participation: Results from a Vietnamese Cross-Section Dataset" Sustainability 11, no. 2: 514. https://doi.org/10.3390/su11020514
APA StyleVuong, Q. -H., Nghiem, K. -C. P., La, V. -P., Vuong, T. -T., Nguyen, H. -K. T., Ho, M. -T., Tran, K., Khuat, T. -H., & Ho, M. -T. (2019). Sex Differences and Psychological Factors Associated with General Health Examinations Participation: Results from a Vietnamese Cross-Section Dataset. Sustainability, 11(2), 514. https://doi.org/10.3390/su11020514