
Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea


Abstract
:1. Introduction
2. Background and Literature Review
2.1. Concerns on Games and Media Panic
2.2. Gaming Disorder
2.3. Contingent Valuation Model
3. Materials and Method
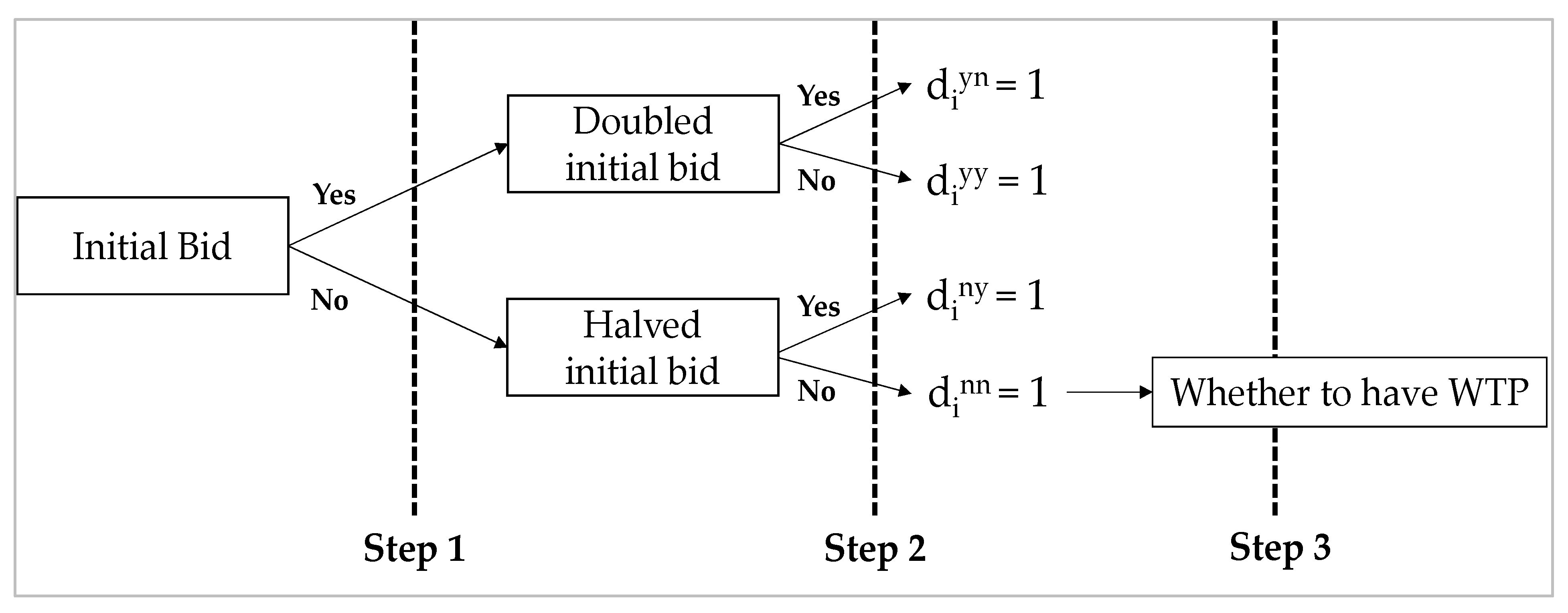
3.1. Analysis Method: DBDC Model
3.2. Questionnaire Design and Procedure
3.3. Participants
4. Results
4.1. Demographic Profile of the Participants
4.2. WTP Estimation Results
4.3. Evaluation of Social Cost
5. Discussions and Conclusions
6. Limitation of the Study
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Drotner, K. Dangerous media? Panic discourses and dilemmas of modernity. Paedagog. Hist. 1999, 35, 593–619. [Google Scholar] [CrossRef]
- Critcher, C. Screen savers. Case histories of social reaction to mass media, children and violence. Rech. et Anthropol. 2012, 43, 59–78. [Google Scholar] [CrossRef]
- Critcher, C. Making waves: Historical aspects of public debates about children and mass media. In The International Handbook of Children, Media and Culture; Sage: London, UK, 2008; pp. 91–104. [Google Scholar]
- Barker, M. A Haunt of Fears: The Strange History of the British Horror Comics Campaign; University Press of Mississippi: Jackson, MS, USA, 1984. [Google Scholar]
- Jensen, H.S. Why Batman was bad: A Scandinavian Debate about Children’s Consumption of Comics and Literature in the 1950s. Barn 2010, 3, 47–70. [Google Scholar]
- Buckingham, D.; Whiteman, N.; Willett, R.; Burn, A.N. The Impact of the Media on Children and Young People with a Particular Focus on Computer Games and the Internet; Prepared for the Byron Review on Children and New Technology; Department for Children, Schools and Families: London, UK, 2007.
- Buckingham, D.; Strandgaard Jensen, H. Beyond “media panics”: Reconceptualising public debates about children and media. J. Child. Media 2012, 6, 413–429. [Google Scholar] [CrossRef]
- Mentzoni, R.A.; Brunborg, G.S.; Molde, H.; Myrseth, H.; Skouverøe, K.J.M.; Hetland, J.; Pallesen, S. Problematic video game use: Estimated prevalence and associations with mental and physical health. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.A.; Shibuya, A.; Ihori, N.; Swing, E.L.; Bushman, B.J.; Sakamoto, A.; Rothstein, H.R.; Saleem, M. Violent video game effects on aggression, empathy, and prosocial behavior in eastern and western countries: A meta-analytic review. Psychol. Bull. 2010, 136, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.J.; Namkoong, K.; Ku, T.; Kim, S.J. The relationship between online game addiction and aggression, self-control and narcissistic personality traits. Eur. Psychiatry 2008, 23, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Király, O.; Griffiths, M.D.; King, D.L.; Lee, H.-K.; Lee, S.-Y.; Bányai, F.; Zsila, Á.; Takacs, Z.K.; Demetrovics, Z. Policy responses to problematic video game use: A systematic review of current measures and future possibilities. J. Behav. Addict. 2018, 7, 503–517. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, C.J. Evidence for publication bias in video game violence effects literature: A meta-analytic review. Aggress. Violent Behav. 2007, 12, 470–482. [Google Scholar] [CrossRef]
- Ferguson, C.J. Do angry birds make for angry children? A meta-analysis of video game influences on children’s and adolescents’ aggression, mental health, prosocial behavior, and academic performance. Perspect. Psychol. Sci. 2015, 10, 646–666. [Google Scholar] [CrossRef]
- Szycik, G.R.; Mohammadi, B.; Hake, M.; Kneer, J.; Samii, A.; Münte, T.F.; te Wildt, B.T. Excessive users of violent video games do not show emotional desensitization: An fMRI study. Brain Imaging Behav. 2017, 11, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Kühn, S.; Kugler, D.T.; Schmalen, K.; Weichenberger, M.; Witt, C.; Gallinat, J. Does playing violent video games cause aggression? A longitudinal intervention study. Mol. Psychiatry 2019, 24, 1220–1234. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.-h.S. Korea to classify gaming addiction as a disease. Business Korea, 27 May 2019. [Google Scholar]
- Aarseth, E.; Bean, A.M.; Boonen, H.; Colder Carras, M.; Coulson, M.; Das, D.; Deleuze, J.; Dunkels, E.; Edman, J.; Ferguson, C.J. Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal. J. Behav. Addict. 2017, 6, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, S.; Nakayama, H.; Mihara, S.; Maezono, M.; Kitayuguchi, T.; Hashimoto, T. Inclusion of gaming disorder criteria in ICD-11: A clinical perspective in favor: Commentary on: Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal (AARSETH ET AL.). J. Behav. Addict. 2017, 6, 293–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Király, O.; Demetrovics, Z. Inclusion of Gaming Disorder in ICD has more advantages than disadvantages: Commentary on: Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal (Aarseth et al.). J. Behav. Addict. 2017, 6, 280–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Brink, W. ICD-11 Gaming Disorder: Needed and just in time or dangerous and much too early? Commentary on: Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal (Aarseth et al.). J. Behav. Addict. 2017, 6, 290–292. [Google Scholar] [CrossRef] [Green Version]
- Van Rooij, A.J.; Ferguson, C.J.; Colder Carras, M.; Kardefelt-Winther, D.; Shi, J.; Aarseth, E.; Bean, A.M.; Bergmark, K.H.; Brus, A.; Coulson, M. A weak scientific basis for gaming disorder: Let us err on the side of caution. J. Behav. Addict. 2018, 7, 1–9. [Google Scholar] [CrossRef]
- Stevens, M.W.; Dorstyn, D.; Delfabbro, P.H.; King, D.L. Global prevalence of gaming disorder: A systematic review and meta-analysis. Aust. N. Z. J. Psychiatry 2020, 55, 553–568. [Google Scholar] [CrossRef]
- Anderson, C.A.; Gentile, D.A.; Buckley, K.E. Violent Video Game Effects on Children and Adolescents: Theory, Research, and Public Policy; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Allen, J.J.; Anderson, C.A. General aggression model. In The International Encyclopedia of Media Effects; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 1–15. [Google Scholar]
- DeWall, C.N.; Anderson, C.A.; Bushman, B.J. The general aggression model: Theoretical extensions to violence. Psychol. Violence 2011, 1, 245–258. [Google Scholar] [CrossRef] [Green Version]
- Greitemeyer, T.; Mügge, D.O. Video games do affect social outcomes: A meta-analytic review of the effects of violent and prosocial video game play. Personal. Soc. Psychol. Bull. 2014, 40, 578–589. [Google Scholar] [CrossRef]
- Ward, M.R. Video games and crime. Contemp. Econ. Policy 2011, 29, 261–273. [Google Scholar] [CrossRef]
- Cunningham, S.; Engelstätter, B.; Ward, M.R. Understanding the effects of violent video games on violent crime. ZEW Cent. Eur. Econ. Res. Discuss. Pap. 2011. [Google Scholar] [CrossRef]
- Markey, P.M.; Markey, C.N.; French, J.E. Violent video games and real-world violence: Rhetoric versus data. Psychol. Pop. Media Cult. 2015, 4, 277–295. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, S.; Engelstätter, B.; Ward, M.R. Violent video games and violent crime. South. Econ. J. 2016, 82, 1247–1265. [Google Scholar] [CrossRef]
- Lee, C.; Kim, H.; Hong, A. Ex-post evaluation of illegalizing juvenile online game after midnight: A case of shutdown policy in South Korea. Telemat. Inform. 2017, 34, 1597–1606. [Google Scholar] [CrossRef]
- Choi, J.; Cho, H.; Lee, S.; Kim, J.; Park, E.-C. Effect of the online game shutdown policy on internet use, internet addiction, and sleeping hours in Korean adolescents. J. Adolesc. Health 2018, 62, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Hunt, A. The great masturbation panic and the discourses of moral regulation in nineteenth-and early twentieth-century Britain. J. Hist. Sex. 1998, 8, 575–615. [Google Scholar]
- Hier, S.P.; Lett, D.; Walby, K.; Smith, A. Beyond folk devil resistance: Linking moral panic and moral regulation. Criminol. Crim. Justice 2011, 11, 259–276. [Google Scholar] [CrossRef]
- Hunt, A. Moral regulation and making-up the new person: Putting Gramsci to work. Theor. Criminol. 1997, 1, 275–301. [Google Scholar] [CrossRef]
- Critcher, C. Widening the focus: Moral panics as moral regulation. Br. J. Criminol. 2009, 49, 17–34. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Petry, N.M.; Rehbein, F.; Ko, C.-H.; O’Brien, C.P. Internet gaming disorder in the DSM-5. Curr. Psychiatry Rep. 2015, 17, 72. [Google Scholar] [CrossRef]
- Stein, D.J.; Reed, G.M. ICD-11: The importance of a science of psychiatric nosology. Lancet Psychiatry 2019, 6, 6–7. [Google Scholar] [CrossRef]
- Shadloo, B.; Farnam, R.; Amin-Esmaeili, M.; Hamzehzadeh, M.; Rafiemanesh, H.; Jobehdar, M.M.; Ghani, K.; Charkhgard, N.; Rahimi-Movaghar, A. Inclusion of gaming disorder in the diagnostic classifications and promotion of public health response: Commentary to the “scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal”: A perspective from Iran. J. Behav. Addict. 2017, 6, 310–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zastrow, M. News Feature: Is video game addiction really an addiction? Proc. Natl. Acad. Sci. USA 2017, 114, 4268–4272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bean, A.M.; Nielsen, R.K.; Van Rooij, A.J.; Ferguson, C.J. Video game addiction: The push to pathologize video games. Prof. Psychol. Res. Pract. 2017, 48, 378–389. [Google Scholar] [CrossRef] [Green Version]
- Dullur, P.; Starcevic, V. Internet gaming disorder does not qualify as a mental disorder. Aust. N. Z. J. Psychiatry 2018, 52, 110–111. [Google Scholar] [CrossRef] [PubMed]
- Frances, A. The past, present and future of psychiatric diagnosis. World Psychiatry 2013, 12, 111–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakefield, J. DSM-5, psychiatric epidemiology and the false positives problem. Epidemiol. Psychiatr. Sci. 2015, 24, 188–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciriacy-Wantrup, S.V. Capital returns from soil-conservation practices. J. Farm Econ. 1947, 29, 1181–1196. [Google Scholar] [CrossRef]
- Carson, R.T. Contingent valuation: A user’s guide. Environ. Sci. Technol. 2000, 34, 1413–1418. [Google Scholar] [CrossRef] [Green Version]
- Haab, T.C.; McConnell, K.E. Valuing Environmental and Natural Resources: The Econometrics of Non-Market Valuation; Edward Elgar Publishing: Cheltenham, UK, 2002. [Google Scholar]
- Arrow, K.; Solow, R.; Portney, P.R.; Leamer, E.E.; Radner, R.; Schuman, H. Report of the NOAA panel on contingent valuation. Fed. Regist. 1993, 58, 4601–4614. [Google Scholar]
- Jin, J.; Wan, X.; Lin, Y.; Kuang, F.; Ning, J. Public willingness to pay for the research and development of solar energy in Beijing, China. Energy Policy 2019, 134, 110962. [Google Scholar] [CrossRef]
- Zhu, L.; Song, Q.; Sheng, N.; Zhou, X. Exploring the determinants of consumer’s WTB and WTP for electric motorcycles using CVM method in Macau. Energy Policy 2019, 127, 64–72. [Google Scholar] [CrossRef]
- Woo, J.; Lim, S.; Lee, Y.-G.; Huh, S.-Y. Financial feasibility and social acceptance for reducing nuclear power plants: A contingent valuation study. Sustainability 2018, 10, 3833. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Chung, N.; Lee, W.S. Preserving the culture of Jeju Haenyeo (Women Divers) as a sustainable tourism resource. Sustainability 2020, 12, 564. [Google Scholar] [CrossRef]
- Zhao, F.; Huang, M. Exploring the Non-Use Value of Important Agricultural Heritage System: Case of Lingnan Litchi Cultivation System (Zengcheng) in Guangdong, China. Sustainability 2020, 12, 3638. [Google Scholar] [CrossRef]
- Jung, J.; Lee, W.S. Estimating the preservation value of the Confucianism symbol tree: Application of the contingent valuation method. Anatolia 2021, 1–13. [Google Scholar] [CrossRef]
- Humphreys, B.R.; Johnson, B.K.; Mason, D.S.; Whitehead, J.C. Estimating the value of medal success in the Olympic Games. J. Sports Econ. 2018, 19, 398–416. [Google Scholar] [CrossRef]
- Vinnicombe, T.; Sou, J.P.U. How can we correct for contingent valuation bias? A case study of the Macau Orchestra. Econ. Aff. 2019, 39, 346–362. [Google Scholar] [CrossRef]
- Shin, J.; Kim, Y.; Nam, H.; Cho, Y. Economic evaluation of healthcare technology improving the quality of social life: The case of assistive technology for the disabled and elderly. Appl. Econ. 2016, 48, 1361–1371. [Google Scholar] [CrossRef]
- Frew, E.; Wolstenholme, J.; Whynes, D. Willingness-to-pay for colorectal cancer screening. Eur. J. Cancer 2001, 37, 1746–1751. [Google Scholar] [CrossRef]
- Yasunaga, H.; Ide, H.; Imamura, T.; Ohe, K. Benefit evaluation of mass screening for prostate cancer: Willingness-to-pay measurement using contingent valuation. Urology 2006, 68, 1046–1050. [Google Scholar] [CrossRef]
- Shono, A.; Kondo, M.; Ohmae, H.; Okubo, I. Willingness to pay for public health services in rural Central Java, Indonesia: Methodological considerations when using the contingent valuation method. Soc. Sci. Med. 2014, 110, 31–40. [Google Scholar] [CrossRef]
- Tambor, M.; Pavlova, M.; Rechel, B.; Golinowska, S.; Sowada, C.; Groot, W. Willingness to pay for publicly financed health care services in Central and Eastern Europe: Evidence from six countries based on a contingent valuation method. Soc. Sci. Med. 2014, 116, 193–201. [Google Scholar] [CrossRef]
- Milligan, M.A.; Bohara, A.K.; Pagán, J.A. Assessing willingness to pay for cancer prevention. Int. J. Health Care Financ. Econ. 2010, 10, 301–314. [Google Scholar] [CrossRef]
- Asgary, A.; Willis, K.; Taghvaei, A.A.; Rafeian, M. Estimating rural households’ willingness to pay for health insurance. Eur. J. Health Econ. 2004, 5, 209–215. [Google Scholar] [CrossRef]
- Catma, S.; Varol, S. Willingness to pay for a hypothetical COVID-19 vaccine in the United States: A contingent valuation approach. Vaccines 2021, 9, 318. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Juan, Y.; Choi, Y.; Lee, C.-K. Estimating the preservation value of world heritage site using contingent valuation method: The case of the Li River, China. Sustainability 2019, 11, 1100. [Google Scholar] [CrossRef] [Green Version]
- Hanemann, M.; Loomis, J.; Kanninen, B. Statistical efficiency of double-bounded dichotomous choice contingent valuation. Am. J. Agric. Econ. 1991, 73, 1255–1263. [Google Scholar] [CrossRef]
- Bateman, I.J.; Langford, I.H.; Jones, A.P.; Kerr, G.N. Bound and path effects in double and triple bounded dichotomous choice contingent valuation. Resour. Energy Econ. 2001, 23, 191–213. [Google Scholar] [CrossRef]
- Bateman, I.J.; Carson, R.T.; Day, B.; Hanemann, M.; Hanley, N.; Hett, T.; Jones-Lee, M.; Loomes, G.; Mourato, S.; Pearce, D.W. Economic Valuation with Stated Preference Techniques: A Manual; Edward Elgar: Cheltenham, UK, 2002. [Google Scholar]
- Teng, C.-I. How do challenges increase customer loyalty to online games? Cyberpsychol. Behav. Soc. Netw. 2013, 16, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.-I. Look to the future: Enhancing online gamer loyalty from the perspective of the theory of consumption values. Decis. Support Syst. 2018, 114, 49–60. [Google Scholar] [CrossRef]
- Lopez-Feldman, A. Introduction to Contingent Valuation Using Stata; MPRA Paper No. 41018; MPRA: Munich, Germany, 2012. [Google Scholar]
- Feng, W.; Ramo, D.; Chan, S.; Bourgeois, J. Internet gaming disorder: Trends in prevalence 1998–2016. Addict. Behav. 2017, 75, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, B.-N.; Cho, S.-C.; Kim, J.-W.; Shin, M.-S.; Yoo, H.-J. Prevalence, correlates, and comorbidities of DSM-IV psychiatric disorders in children in Seoul, Korea. Asia Pac. J. Public Health 2015, 27, NP1942–NP1951. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, I.; Lim, M.H.; Paik, K.C.; Cho, S.; Kwon, H.-J.; Lee, S.G.; Yoo, S.-J.; Ha, M. Prevalence of attention-deficit/hyperactivity disorder and its comorbidity among Korean children in a community population. J. Korean Med. Sci. 2017, 32, 401–406. [Google Scholar] [CrossRef]
- Korean Statistics. Estimation of the Population; Korean Statistics: Seoul, Korea, 2020. [Google Scholar]
- Hong, M.; Park, B.; Lee, S.M.; Bahn, G.H.; Kim, M.J.; Park, S.; Oh, I.-H.; Park, H. Economic burden and disability-adjusted life years (DALYs) of attention deficit/hyperactivity disorder. J. Atten. Disord. 2020, 24, 823–829. [Google Scholar] [CrossRef]


{kind=link}
| Bid (GD Diagnosis Test Price: KRW) | Number of Surveys |
|---|---|
| 100,000 | 171 |
| 140,000 | 170 |
| 180,000 | 170 |
| 220,000 | 170 |
| 260,000 | 170 |
| 300,000 | 170 |
| Total | 1021 |
| Number of Respondent (%) | ||
|---|---|---|
| Gender | Male | 512 (50.15%) |
| Female | 509 (49.85%) | |
| Age | 20s | 200 (19.59%) |
| 30s | 207 (20.27%) | |
| 40s | 248 (24.29%) | |
| 50s | 258 (25.27%) | |
| Over 60 | 108 (10.58%) | |
| Marriage | Yes | 654 (64.05%) |
| No | 367 (35.95%) | |
| Education | Less than high school | 216 (21.16%) |
| Attending/Graduated College | 142 (13.91%) | |
| Attending/Graduated University | 495 (48.48%) | |
| Attending/Graduated Graduate school | 168 (16.45%) | |
| Monthly income | Less than 2 M (KRW) | 121 (11.85%) |
| 2 M ~less than 3 M (KRW) | 180 (17.63%) | |
| 3 M ~ less than 4 M (KRW) | 205 (20.08%) | |
| 4 M ~ less than 5 M (KRW) | 183 (17.92%) | |
| 5 M ~ less than 6 M (KRW) | 142 (13.91%) | |
| More than 6 M (KRW) | 190 (18.61%) |
| Bid Amount (KRW) | Number of Samples | Respond | |||||
|---|---|---|---|---|---|---|---|
| Initial | Higher | Lower | Yes-Yes | Yes-No | No-Yes | No-No | |
| 100,000 | 200,000 | 50,000 | 171 | 49 | 43 | 38 | 41 |
| 140,000 | 280,000 | 70,000 | 170 | 32 | 29 | 44 | 65 |
| 180,000 | 360,000 | 90,000 | 170 | 37 | 28 | 32 | 73 |
| 220,000 | 440,000 | 110,000 | 170 | 21 | 28 | 41 | 80 |
| 260,000 | 520,000 | 130,000 | 170 | 27 | 23 | 33 | 87 |
| 300,000 | 600,000 | 150,000 | 170 | 20 | 27 | 27 | 96 |
| Total | 1021 | 186 | 178 | 215 | 442 | ||
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |||
| Constant | 179.40 | *** | 0.000 | −21.57 | 0.805 | |
| Age | - | 3.98 | *** | 0.000 | ||
| Gender (Male) | - | 1.11 | 0.952 | |||
| Education | - | 5.27 | 0.577 | |||
| Income | - | 17.90 | ** | 0.002 | ||
| Marriage | - | −0.01 | 1.000 | |||
| Prior knowledge | - | −21.04 | 0.162 | |||
| Attitude | - | −4.39 | 0.657 | |||
| Agree | - | 10.73 | 0.054 | |||
| Suspicion of GD | - | −71.42 | *** | 0.007 | ||
| Interest on game | - | −5.33 | 0.470 | |||
| Log likelihood | −1244.08 | −1212.59 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, C.; Kim, Y.; Sohn, J.H. Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea. Sustainability 2021, 13, 8106. https://doi.org/10.3390/su13148106
Yoo C, Kim Y, Sohn JH. Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea. Sustainability. 2021; 13(14):8106. https://doi.org/10.3390/su13148106
Chicago/Turabian StyleYoo, Changsok, Yelim Kim, and Jee Hoon Sohn. 2021. "Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea" Sustainability 13, no. 14: 8106. https://doi.org/10.3390/su13148106
APA StyleYoo, C., Kim, Y., & Sohn, J. H. (2021). Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea. Sustainability, 13(14), 8106. https://doi.org/10.3390/su13148106