
The Psychological and Social Impacts of Curfew during the COVID-19 Outbreak in Kuwait: A Cross-Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
- Measuring residents’ perceptions related to the COVID-19 pandemic.
- Assessing residents’ mental health changes before and during the COVID-19 curfew.
- Describing the changes in health behaviors from before and during the COVID-19 curfew.
- Identifying risks related to negative psychological impacts of the COVID-19 curfew.
2. Materials and Methods
2.1. Survey Method and Target Population
2.2. Questionnaire Design and Tools
2.3. Research Ethics
2.4. Method of Analysis
3. Results
3.1. General Characteristics
3.2. Working Conditions at Home
3.3. Health Conditions
3.4. Perception of COVID-19
3.5. Mental Health
3.6. Family Relationship
3.7. Correlations between Mental Health and Health Behaviors
3.8. Predictors of Mental Health Status
3.8.1. Predictor Variables Associated with Depression and Extremely Severe Depression
3.8.2. Predicting Variables to Depression and Extremely Severe Depression
3.8.3. Predicting Variables to Stress and Severe or Extremely Severe Stress
3.8.4. Predicting Variables to Psychological Distress and Severe or Extremely Severe Psychological Distress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Novel Coronavirus (2019-nCoV): Situation Report-1; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. WHO Timeline-COVID-19. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (accessed on 13 May 2021).
- The Central Agency for Information. Technology COVID 19 Updates: Sate of Kuwait-Live. Available online: https://corona.e.gov.kw/En/ (accessed on 30 April 2021).
- Salman, A.; Sigodo, K.O.; Al-Ghadban, F.; Al-Lahou, B.; Alnashmi, M.; Hermassi, S.; Chun, S. Effects of COVID-19 Lockdown on Physical Activity and Dietary Behaviors in Kuwait: A Cross-Sectional Study. Nutrients 2021, 13, 2252. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and Anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef]
- Hyland, P.; Shevlin, M.; McBride, O.; Murphy, J.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr. Scand. 2020, 142, 249–256. [Google Scholar] [CrossRef]
- Brown, S.M.; Doom, J.R.; Lechuga-Peña, S.; Watamura, S.E.; Koppels, T. Stress and parenting during the global COVID-19 pandemic. Child Abus. Negl. J. 2020, 110, 104699. [Google Scholar] [CrossRef] [PubMed]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological Outcomes Associated with Stay-at-Home Orders and the Perceived Impact of COVID-19 on Daily Life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef] [PubMed]
- Alasousi, L.; al Hammouri, S.; Al-abdulhadi, S. al Anxiety and media exposure during COVID-19 outbreak in Kuwait. medRxiv 2020, 24, 745. [Google Scholar]
- Sifat, R.I. Impact of the COVID-19 pandemic on domestic violence in Bangladesh. Asian J. Psychiatry J. 2020, 53, 102393. [Google Scholar] [CrossRef] [PubMed]
- Brailovskaia, J.; Margraf, J. Predicting adaptive and maladaptive responses to the Coronavirus (COVID-19) outbreak: A prospective longitudinal study. Int. J. Clin. Heal. Psychol. 2020, 20, 183–191. [Google Scholar] [CrossRef]
- Abbas, J.; Wang, D.; Su, Z.; Ziapour, A. The Role of Social Media in the Advent of COVID-19 Pandemic: Crisis Management, Mental Health Challenges and Implications. Risk Manag. Healthc. Policy 2021, 14, 1917–1932. [Google Scholar] [CrossRef] [PubMed]
- Sukeri, S.; Zahiruddin, W.M.; Shafei, M.N.; Hamat, R.A.; Osman, M.; Jamaluddin, T.Z.M.T.; Daud, A.B. Perceived severity and susceptibility towards leptospirosis infection in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 6362. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Infodemic. Available online: https://www.who.int/health-topics/infodemic#tab=tab_1 (accessed on 12 May 2021).
- Young, M.E.; Norman, G.R.; Humphreys, K.R. Medicine in the Popular Press: The Influence of the Media on Perceptions of Disease. PLoS ONE 2008, 3, e3552. [Google Scholar] [CrossRef]
- Chan, E.Y.Y.; Huang, Z.; Lo, E.S.K.; Hung, K.K.C.; Wong, E.L.Y.; Wong, S.Y.S. Sociodemographic predictors of health risk perception, attitude and behavior practices associated with health-emergency disaster risk management for biological hazards: The case of COVID-19 pandemic in Hong Kong, SAR China. Int. J. Environ. Res. Public Health 2020, 17, 3869. [Google Scholar] [CrossRef]
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Heal. Educ. Behav. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrie, K.J.; Weinman, J. Why illness perceptions matter. Clin. Med. Northfield. 2006, 6, 536–539. [Google Scholar] [CrossRef]
- Kim, C.W.; Song, H.R. Structural Relationships among Public’s Risk Characteristics, Trust, Risk Perception and Preventive Behavioral Intention-The Case of MERS in Korea. Crisisonomy 2017, 13, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Survey Tool and Guidance: Rapid, Simple, Flexible Behavioral Insights on COVID-19; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- United Nations. Policy Brief: COVID-19 and the Need for Action on Mental Health; United Nations: New York, NY, USA, 2020. [Google Scholar]
- Shahnazi, H.; Ahmadi-Livani, M.; Pahlavanzadeh, B.; Rajabi, A.; Hamrah, M.S.; Charkazi, A. Assessing preventive health behaviors from COVID-19: A cross sectional study with health belief model in Golestan Province, Northern of Iran. Infect. Dis. Poverty 2020, 9, 157. [Google Scholar] [CrossRef]
- Yusoff, M.S.B. Psychometric properties of the depression anxiety stress scale in a sample of medical degree applicants. Int. Med. J. 2013, 20, 295–300. [Google Scholar]
- The International Physical Activity Questionnaire Guidelines for Data Processing and Analysis of the International Physical Activity (IPAQ). Available online: http://www.ipaq.ki.se/ (accessed on 30 April 2021).
- American Association for Public Opinion Research the Code of Professional Ethics and Practices. Available online: https://www.aapor.org/Standards-Ethics/AAPOR-Code-of-Ethics.aspx (accessed on 21 June 2020).
- Salman, A.; Tolma, E.; Chun, S.; Sigodo, K.O.; Al-Hunayan, A. Health Promotion Programs to Reduce Noncommunicable Diseases: A Call for Action in Kuwait. Healthcare 2020, 8, 251. [Google Scholar] [CrossRef]
- Salman, A.; Fakhraldeen, S.A.; Chun, S.; Jamil, K.; Gasana, J.; Al-Hunayan, A. Enhancing Research and Development in the Health Sciences as a Strategy to Establish a Knowledge-Based Economy in the State of Kuwait: A Call for Action. Healthcare 2020, 8, 264. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.; Salman, A. Policy Paper for the Health Pillar: Overview of Gaps, Challenges, and Way Forward in Kuwait National Development Plan 2015–2020; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019. [Google Scholar]
- Chun, S.; Salman, A. White Paper for the Health Pillar National Health Policy Framework: Ensuring Healthy Lives and Wellbeing; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019. [Google Scholar]
- Chun, S.; Salman, A. Research Agenda for the Health Pillar; Kuwait Public Policy Center, General Secretariat of the Supreme Council for Planning and Development: Kuwait City, Kuwait, 2019. [Google Scholar]
- Pfefferbaum, B.; North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Hermassi, S.; Sellami, M.; Salman, A.; Al-Mohannadi, A.S.; Bouhafs, E.G.; Hayes, L.D.; Schwesig, R. Effects of COVID-19 Lockdown on Physical Activity, Sedentary Behavior, and Satisfaction with Life in Qatar: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 3093. [Google Scholar] [CrossRef]
- Costanza, A.; Amerio, A.; Odone, A.; Baertschi, M.; Richard-Lepouriel, H.; Weber, K.; Di Marco, S.; Prelati, M.; Aguglia, A.; Escelsior, A.; et al. Suicide prevention from a public health perspective. What makes life meaningful? The opinion of some suicidal patients. Acta Biomed 2020, 91, 128–134. [Google Scholar] [PubMed]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the COVID-19 pandemic. QJM An. Int. J. Med. 2020, 113, 311–312. [Google Scholar] [CrossRef]
- Sediri, S.; Zgueb, Y.; Ouanes, S.; Ouali, U.; Bourgou, S.; Jomli, R.; Nacef, F. Women’s mental health: Acute impact of COVID-19 pandemic on domestic violence. Arch. Womens. Ment. Health 2020, 23, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Thibaut, F.; van Wijngaarden-Cremers, P.J.M. Women’s Mental Health in the Time of Covid-19 Pandemic. Front. Glob. Women Heal. 2020, 1, 588372. [Google Scholar] [CrossRef]
- Costanza, A.; Rothen, S.; Achab, S.; Thorens, G.; Baertschi, M.; Weber, K.; Canuto, A.; Richard-Lepouriel, H.; Perroud, N.; Zullino, D. Impulsivity and Impulsivity-Related Endophenotypes in Suicidal Patients with Substance Use Disorders: An Exploratory Study. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [Green Version]
- Guadagni, V.; Umilta’, A.; Iaria, G. Sleep Quality, Empathy, and Mood During the Isolation Period of the COVID-19 Pandemic in the Canadian Population: Females and Women Suffered the Most. Front. Glob. Women Heal. 2020, 1, 585938. [Google Scholar] [CrossRef]
- Liu, S.; Yang, L.; Zhang, C.; Xu, Y.; Cai, L.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; et al. Gender differences in mental health problems of healthcare workers during the coronavirus disease 2019 outbreak. J. Psychiatr. Res. 2021, 137, 393–400. [Google Scholar] [CrossRef]
- Yan, S.; Xu, R.; Stratton, T.D.; Kavcic, V.; Luo, D.; Hou, F.; Bi, F.; Jiao, R.; Song, K.; Jiang, Y. Sex differences and psychological stress: Responses to the COVID-19 pandemic in China. BMC Public Health 2021, 21, 79. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, H.G. Gender Differences in Mental Health and Beliefs about Covid-19 among Elderly Internet Users. Paidéia 2021, 31, e3110. [Google Scholar] [CrossRef]
- Prowse, R.; Sherratt, F.; Abizaid, A.; Gabrys, R.L.; Hellemans, K.G.C.; Patterson, Z.R.; McQuaid, R.J. Coping With the COVID-19 Pandemic: Examining Gender Differences in Stress and Mental Health Among University Students. Front. Psychiatry 2021, 12, 650759. [Google Scholar] [CrossRef]
- García-Fernández, L.; Romero-Ferreiro, V.; Padilla, S.; David López-Roldán, P.; Monzó-García, M.; Rodriguez-Jimenez, R. Gender differences in emotional response to the COVID-19 outbreak in Spain. Brain Behav. 2021, 11, e01934. [Google Scholar] [CrossRef] [PubMed]
- Ambrosetti, J.; Macheret, L.; Folliet, A.; Wullschleger, A.; Amerio, A.; Aguglia, A.; Serafini, G.; Prada, P.; Kaiser, S.; Bondolfi, G.; et al. Impact of the COVID-19 Pandemic on Psychiatric Admissions to a Large Swiss Emergency Department: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 1174. [Google Scholar] [CrossRef] [PubMed]
- Bhugra, D.; Tasman, A.; Pathare, S.; Priebe, S.; Smith, S.; Torous, J.; Arbuckle, M.R.; Langford, A.; Alarcón, R.D.; Chiu, H.F.K.; et al. The WPA-Lancet Psychiatry Commission on the Future of Psychiatry. The Lancet Psychiatry 2017, 4, 775–818. [Google Scholar] [CrossRef]
- Costanza, A.; Ambrosetti, J.; Wyss, K.; Bondolfi, G.; Sarasin, F.; Khan, R. Preventing suicide in emergencies: From “Interpersonal Suicide Theory” to connectedness. Rev. Med. Suisse 2018, 4, 335–338. [Google Scholar]
- Deslich, S.; Stec, B.; Tomblin, S.; Coustasse, A. Telepsychiatry in the 21st century: Transforming healthcare with technology. Perspect. Heal. Inf. Manag. 2013, 10, 1. Available online: https://www.researchgate.net/publication/249967520_Telepsychiatry_in_the_21st_Century_Transforming_Healthcare_with_Technology (accessed on 21 June 2020).
- Costanza, A.; Mazzola, V.; Radomska, M.; Amerio, A.; Aguglia, A.; Prada, P.; Bondolfi, G.; Sarasin, F.; Ambrosetti, J. Who Consults an Adult Psychiatric Emergency Department? Pertinence of Admissions and Opportunities for Telepsychiatry. Med. B Aires 2020, 56, 295. [Google Scholar] [CrossRef]
- Salum, G.A.; Rehmenklau, J.F.; Csordas, M.C.; Pereira, F.P.; Castan, J.U.; Ferreira, A.B.; Delgado, V.B.; de Bolzan, L.M.; de Lima, M.A.; Blauth, J.H.; et al. Supporting people with severe mental health conditions during the COVID-19 pandemic: Considerations for low- and middle-income countries using telehealth case management. Braz. J. Psychiatry 2020, 42, 451. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | % |
|---|---|
| Gender | |
| Female | 57.9 |
| Male | 42.1 |
| Age | |
| 21~29 | 28.7 |
| 30~39 | 29.3 |
| 40~49 | 23.0 |
| 50~59 | 15.2 |
| 60 and above | 3.8 |
| Nationality | |
| Kuwaiti | 67.7 |
| Non-Kuwaiti | 32.3 |
| Marital status | |
| Married | 63.8 |
| Single (never married) | 29.7 |
| Divorced/spouse deceased | 6.5 |
| Education | |
| High school/intermediate school/primary school/less than primary school | 13.3 |
| Diploma | 16.5 |
| College/University | 47.6 |
| Postgraduate | 22.7 |
| Variables | % |
|---|---|
| Employment type | |
| Salaried employee | 63.9 |
| Retired | 8.2 |
| Unemployed | 6.0 |
| Business Owner | 5.0 |
| Student | 13.1 |
| Homemaker | 3.7 |
| Do you work for a job at home, even under Curfew (for students: are you continuing to study) during the COVID-19 outbreak? | |
| No | 64.5 |
| Yes | 35.5 |
| How much time and effort did you spend on housework during the COVID-19 outbreak? | |
| Rather reduced | 10.9 |
| Same as usual | 25.8 |
| Slightly increased | 37.0 |
| Very much increased | 26.4 |
| Variables | % |
|---|---|
| Do you have any conditions or diseases? (selected all that apply) | |
| High blood pressure | 11.5 |
| Diabetes | 10.5 |
| Cardiovascular disease | 3.8 |
| Chronic bronchitis | 5.4 |
| Hereditary conditions | 3.2 |
| Mental illness | 1.5 |
| Cancer | 0.9 |
| Physical disability | 1.2 |
| None of the diseases | 66.9 |
| Are you, or have you been, infected with the novel coronavirus? | |
| Yes, tested and the result was positive | 2.2 |
| Yes, suspected but not confirmed by a test | 2.2 |
| No, tested and the result was negative | 8.1 |
| No | 72.9 |
| Don’t know | 14.6 |
| Do you know people in your immediate social environment who are or have been infected with the novel coronavirus? | |
| Yes, confirmed | 50.4 |
| Yes, suspected but not confirmed by a test | 3.4 |
| No, tested and the result was negative | 4.3 |
| No | 36.4 |
| Don’t know | 5.4 |
| Variables | Female (n = 393) | Male (n = 286) | x2-or t-, and (p-Value) |
|---|---|---|---|
| %, Mean (SD) | |||
| Do you consider yourself to be? | |||
| Risk Averse | 66.9 | 67.5 | 7.651 (0.022) |
| Risk Takers | 3.8 | 8.4 | |
| Neutral | 29.3 | 24.1 | |
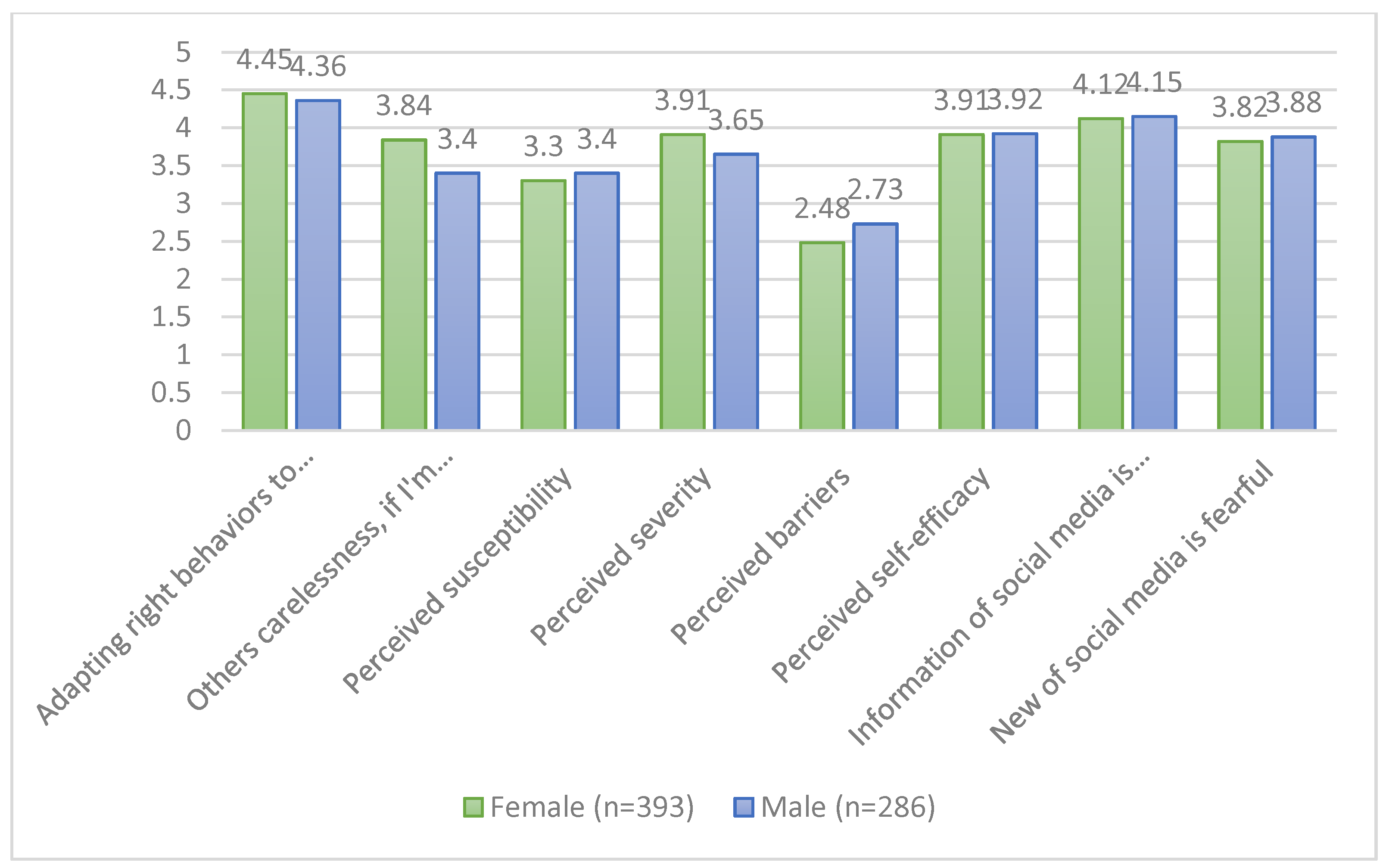
| Do you consider yourself adapting the right behaviors and measurements to prevent the infection? | |||
| (Mal adaptation ①-②-③-④-⑤ Adaptation) | 4.45 (0.89) | 4.36 (1.00) | 1.225 (0.221) |
| If I’m infected with coronavirus, it will come with~ | |||
| (My carelessness ①-②-③-④-⑤ Carelessness from other community people) | 3.84 (1.44) | 3.40 (1.61) | 3.774 (0.000) |
| Perceived susceptibility 1 | 3.30 (1.18) | 3.40 (1.00) | −1.136 (0.256) |
| Perceived severity 1 | 3.91 (0.82) | 3.65 (0.96) | 3.795 (0.000) |
| Perceived barriers 1 | 2.48 (0.91) | 2.73 (0.91) | −3.666 (0.000) |
| Perceived self-efficacy 1 | 3.91 (0.83) | 3.92 (0.78) | −0.212 (0.832) |
| TV, radio, SMS, and Internet information about the disease have been helpful 1 | 4.12 (1.14) | 4.15 (1.05) | −0.389 (0.698) |
| Is the news on Social Media and the Internet and TV induce fear and feeling of threat? 1 | 3.82 (1.09) | 3.88 (1.09) | −0.656 (0.512) |
| Mental Health | Total (n = 679) | Female (n = 393) | Male (n = 286) | x2-and (p-Value) |
|---|---|---|---|---|
| % | ||||
| Depression | ||||
| Normal | 43.9 | 40.2 | 49.0 | 8.980 (0.030) |
| Mild | 19.9 | 21.6 | 17.5 | |
| Moderate | 18.7 | 17.8 | 19.9 | |
| Extremely severe | 17.5 | 20.4 | 13.6 | |
| Anxiety | ||||
| Normal | 87.9 | 85.5 | 91.3 | |
| Moderate | 6.5 | 7.9 | 4.5 | 5.961 (0.114) |
| Severe | 2.9 | 3.8 | 1.7 | |
| Extremely severe | 2.7 | 2.8 | 2.4 | |
| Stress | ||||
| Normal | 83.2 | 81.7 | 85.3 | |
| Moderate | 8.2 | 8.9 | 7.3 | 1.907 (0.592) |
| Severe | 5.3 | 6.1 | 4.2 | |
| Extremely severe | 3.2 | 3.3 | 3.1 | |
| General psychological distress | ||||
| Normal | 62.3 | 58.0 | 68.2 | |
| Mild | 14.1 | 15.5 | 12.2 | |
| Moderate | 11.0 | 11.5 | 10.5 | 8.876 (0.064) |
| Severe | 7.4 | 8.7 | 4.9 | |
| Extremely severe | 5.4 | 6.4 | 4.2 | |
| Health Behaviors | Total (n = 679) | Female (n = 393) | Male (n = 286) | χ2-and (p-Value) |
|---|---|---|---|---|
| % | ||||
| Have tensions or even violent behavior increased in the relationships with any of your family members (husband/wife, parents, children) compared to before the outbreak of COVID-19? | ||||
| Yes | 31.3 | 34.9 | 26.4 | 5.717 (0.057) |
| No | 65.4 | 62.3 | 68.7 | |
| I refuse to answer | 3.2 | 2.8 | 3.9 | |
| Have these tensions in your relationships with any of your family members (husband/wife, parents, children) resulted in physical or verbal abuse? | ||||
| Verbal abuse | 14.1 | 17.8 | 9.1 | 14.888 (0.005) |
| Physical abuse | 0.9 | 0.5 | 1.4 | |
| Verbal and physical abuse | 2.9 | 3.8 | 1.7 | |
| No | 78.5 | 74.3 | 84.3 | |
| I refuse to answer | 3.5 | 3.6 | 3.5 | |
| In your view, what are the factors affecting the mental wellbeing of yourself and any of your family members, leading to tensions or even violent acts in the relationship during the COVID-19 outbreak? (Please select all that apply) | ||||
| Physical proximity | 26.5 | 26.7 | 26.2 | 0.021 (0.930) |
| Increased demands at the job | 10.3 | 11.2 | 9.1 | 0.793 (0.443) |
| Increased household work | 18.4 | 23.4 | 11.5 | 15.531 (0.000) |
| Increased tasks to guide children’s learning | 15.9 | 18.1 | 12.9 | 3.256 (0.089) |
| Financial anxieties | 25.3 | 24.4 | 26.6 | 0.403 (0.533) |
| Fear about the future prospects | 36.8 | 34.4 | 40.2 | 2.442 (0.126) |
| Lack of common interest and/or hobbies | 20.6 | 23.7 | 16.4 | 5.288 (0.022) |
| Lack of physical exercise and sport | 17.1 | 15.0 | 19.9 | 2.826 (0.099) |
| Lack of sleep and rest | 21.2 | 23.2 | 18.5 | 2.118 (0.155) |
| Increased negative health symptoms | 11.0 | 12.5 | 9.1 | 1.922 (0.175) |
| Others | 25.3 | 24.7 | 26.2 | 0.208 (0.656) |
| Depression | Anxiety | Stress | General Psychological Distress | |
|---|---|---|---|---|
| Days of physical activities | −0.061 | −0.037 | −0.085 * | −0.074 |
| Daily amount of smoking cigarette | 0.084 * | 0.013 | 0.020 | 0.049 |
| Daily amount of smoking shisha | 0.041 | 0.033 | 0.059 | 0.054 |
| Sleep hours | 0.047 | 0.013 | 0.014 | 0.031 |
| Quality of sleep | −0.139 ** | −0.181 ** | 0.158 ** | −0.194 ** |
| Variables | Adjusted Odds Ratio (95% CI) | |
|---|---|---|
| Normal vs. Depression | Normal vs. Extremely Severe Depression | |
| Gender Male Female | - | 1 2.00 (1.13, 3.55) |
| Age 50 and above 21~49 | 1 2.18 (1.14, 3.35) | 1 4.56 (1.86, 11.22) |
| Have tensions or even violent behavior increased in the relationships with any of your family members? No Yes | 1 2.07 (1.41, 3.35) | 1 2.88 (1.75, 4.76) |
| Comparing with the eating habits before the COVID-19 outbreak in Kuwait, what is your current amount of ‘sweets and snacks’? I eat the same as before or less I eat more | 1 1.52 (1.07, 2.17) | - |
| In the past week, how many days have you done a total of 30 min or more of physical activity? More than 1 day None | - | 1 1.64 (1.00, 2.71) |
| How many cigarettes do you usually smoke a day? (include electric cigarettes) None Smoke every day | 1 1.63 (1.08, 2.48) | 1 3.02 (1.58, 5.79) |
| How many hours do you usually sleep a day? (include naps) 8–9 h Less than 8 h or more than 9 h | 1 1.55 (1.11, 2.16) | - |
| How do you think about the quality of your sleep to compared to what you had before the COVID-19 outbreak? Very good/good Poor/very poor | - | 1 (1.07, 2.86) |
| Variables | Final Odds Ratio (95% CI) | |
|---|---|---|
| Normal vs. Anxiety | Normal vs. Severe or Extremely Severe Anxiety | |
| Marital status Married Single/divorced/widowed | - | 1 2.54 (1.24, 5.20) |
| Do you have any conditions or diseases? No Yes | - | 1 2.11 (1.03, 4.32) |
| Have tensions or even violent behavior increased in the relationships with any of your family members? No Yes | 1 2.52 (1.54, 4.11) | 1 3.24 (1.57, 6.65) |
| How do you think about the quality of your sleep to compared to what you had before the COVID-19 outbreak? Very good/good Poor/very poor | 1 2.07 (1.26, 3.38) | 1 2.79 (1.35, 5.80) |
| Variables | Final Odds Ratio (95% CI) | |
|---|---|---|
| Normal vs. Stress | Normal vs. Severe or Extremely Severe Stress | |
| Marital status Married Single/divorced/widowed | 1 1.63 (1.05, 2.54) | 1 1.83 (1.01, 3.29) |
| Have tensions or even violent behavior increased in the relationships with any of your family members? No Yes | 1 3.07 (1.985, 4.76) | 1 3.52 (1.94, 6.39) |
| How many cigarettes do you usually smoke a day? (include electric cigarettes) None Smoke every day | 1 1.70 (1.03, 2.83) | - |
| How do you think about the quality of your sleep to compared to what you had before the COVID-19 outbreak? Very good/good Poor/very poor | 1 1.94 (1.25, 3.01) | 1 (1.10, 3.61) |
| Variables | Final Odds Ratio (95% CI) | |
|---|---|---|
| Normal vs. Distress | Normal vs. Severe or Extremely Severe Distress | |
| Gender Male Female | - | 1 3.09 (1.54, 6.19) |
| Age 50 and above 21~49 | 1 2.43 (1.46, 4.04) | 1 3.68 (1.37, 9.92) |
| Do you have any conditions or diseases? No Yes | 1 1.55 (1.07, 2.25) | 1 1.83 (1.07, 3.32) |
| Have tensions or even violent behavior increased in the relationships with any of your family members? No Yes | 1 1.68 (1.10, 2.57) | 1 3.56 (2.08, 6.09) |
| Have these tensions in your relationships with any of your family members? No Verbal or physical abuse | 1 1.66 (1.01, 2.73) | - |
| Comparing with the eating habits before the COVID-19 outbreak in Kuwait, what is your current amount of ‘sweets and snacks’? I eat the same as before or less I eat more | 1 1.46 (1.02, 2.07) | - |
| How many cigarettes do you usually smoke a day? (include electric cigarettes) None Smoke every day | - | 1 3.06 (1.47, 6.36) |
| How do you think about the quality of your sleep compared to what you had before the COVID-19 outbreak? Very good/good Poor/very poor | 1 1.61 (1.14, 2.28) | 1 2.20 (1.28, 3.78) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salman, A.; Al-Ghadban, F.; Sigodo, K.O.; Taher, A.K.; Chun, S. The Psychological and Social Impacts of Curfew during the COVID-19 Outbreak in Kuwait: A Cross-Sectional Study. Sustainability 2021, 13, 8464. https://doi.org/10.3390/su13158464
Salman A, Al-Ghadban F, Sigodo KO, Taher AK, Chun S. The Psychological and Social Impacts of Curfew during the COVID-19 Outbreak in Kuwait: A Cross-Sectional Study. Sustainability. 2021; 13(15):8464. https://doi.org/10.3390/su13158464
Chicago/Turabian StyleSalman, Ahmad, Fatima Al-Ghadban, Kennedy Ouma Sigodo, Ayyoub K. Taher, and Sungsoo Chun. 2021. "The Psychological and Social Impacts of Curfew during the COVID-19 Outbreak in Kuwait: A Cross-Sectional Study" Sustainability 13, no. 15: 8464. https://doi.org/10.3390/su13158464
APA StyleSalman, A., Al-Ghadban, F., Sigodo, K. O., Taher, A. K., & Chun, S. (2021). The Psychological and Social Impacts of Curfew during the COVID-19 Outbreak in Kuwait: A Cross-Sectional Study. Sustainability, 13(15), 8464. https://doi.org/10.3390/su13158464