
Facilitators and Barriers of Teachers’ Use of Effective Classroom Management Strategies for Students with ADHD: A Model Analysis Based on Teachers’ Perspectives

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
- 1.
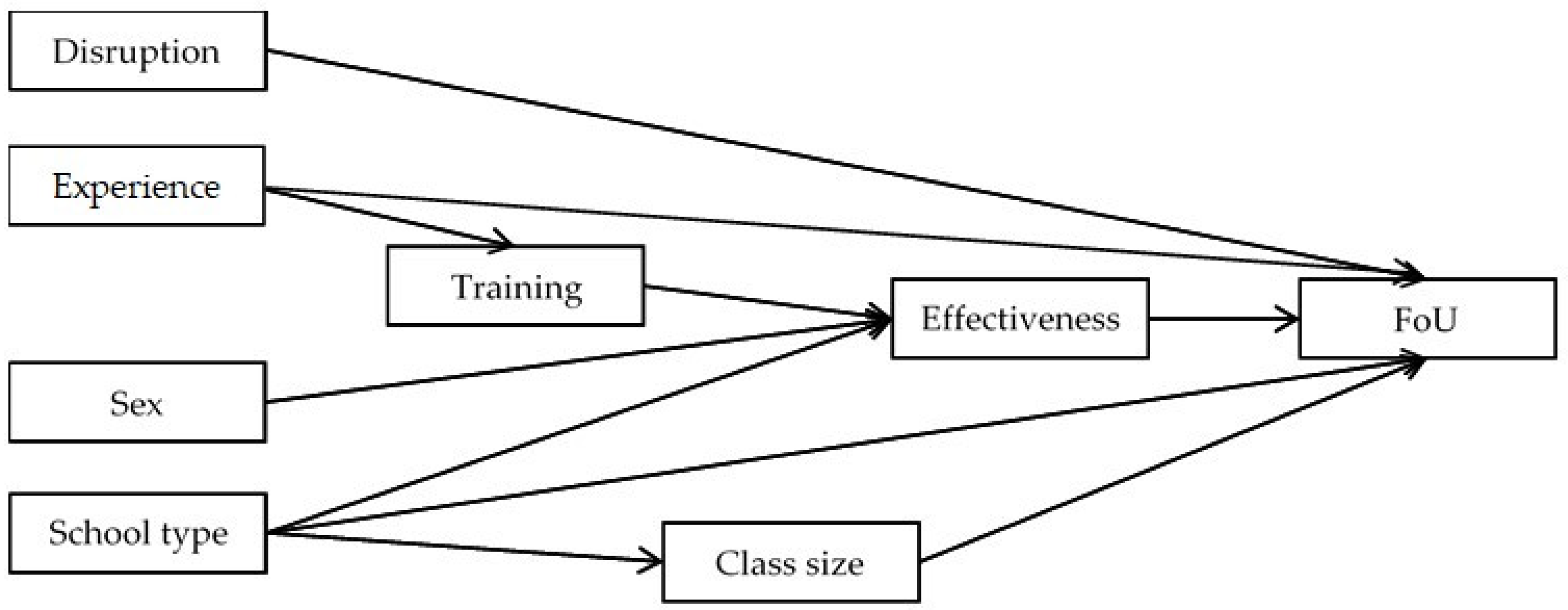
- Can the theory-driven path model of relevant factors associated with implementing effective CMS (i.e., perceived effectiveness of CMS, perceived disruption induced by specific behavioral problems associated with students with ADHD, formal or informal training in ADHD, school type, and sex) developed by Strelow et al. [14] via top-down methods be replicated utilizing bottom-up, open innovation methods?
- 2.
- Does the inclusion of the variables class size and experience, measured by the number of children with ADHD currently instructed by the teacher improve the model fit compared to the original model?
- 3.
- What are the main barriers to implementing effective CMS according to in-service teachers, and do primary/SEN and secondary school teachers differ in how frequently they report them?
2. Materials and Methods
2.1. Sample
2.2. Study Design
2.3. Procedure
2.4. Measures
2.4.1. Sociodemographic Data
2.4.2. Frequency of Use (FoU) and Perceived Effectiveness of CMS (Perceived Effectiveness)
2.4.3. Perceived Disruption Induced by Specific Behavioral Problems Associated with Students with ADHD (Perceived Disruption)
2.4.4. Teachers’ Participation in Formal or Informal Training (Training)
2.4.5. Barriers of CMS Implementation and Support Needs
2.4.6. Influence of the Special Conditions Due to the SARS-CoV-2 Pandemic
2.5. Statistical Analyses
2.5.1. Missing Data Analysis
2.5.2. Path Model Analysis
2.5.3. Exploratory Analyses
3. Results
3.1. Path Analysis of the Replication Model
3.2. Path Analysis of the Extended Model
3.3. Exploratory Analyses
4. Discussion
4.1. General Discussion
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- Frazier, T.W.; Youngstrom, E.A.; Glutting, J.J.; Watkins, M.W. ADHD and achievement: Meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. J. Learn. Disabil. 2007, 40, 49–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loe, I.M.; Feldman, H.M. Academic and educational outcomes of children with ADHD. J. Pediatr. Psychol. 2007, 32, 643–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Oord, S.; Prins, P.J.M.; Oosterlaan, J.; Emmelkamp, P.M.G. Efficacy of methylphenidate, psychosocial treatments and their combination in school-aged children with ADHD: A meta-analysis. Clin. Psychol. Rev. 2008, 28, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Gaastra, G.F.; Groen, Y.; Tucha, L.; Tucha, O. The Effects of Classroom Interventions on Off-Task and Disruptive Classroom Behavior in Children with Symptoms of Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. PLoS ONE 2016, 11, e0148841. [Google Scholar] [CrossRef] [Green Version]
- DuPaul, G.J.; Eckert, T.L.; Vilardo, B. The Effects of School-Based Interventions for Attention Deficit Hyperactivity Disorder: A Meta-Analysis 1996–2010. Sch. Psych. Rev. 2012, 41, 387–412. [Google Scholar] [CrossRef]
- United Nations Sustainable Development Goals Home Page. Available online: https://www.un.org/sustainabledevelopment/education/ (accessed on 10 November 2021).
- DuPaul, G.J.; Chronis-Tuscano, A.; Danielson, M.L.; Visser, S.N. Predictors of Receipt of School Services in a National Sample of Youth with ADHD. J. Atten. Disord. 2019, 23, 1303–1319. [Google Scholar] [CrossRef]
- Ruhmland, M.; Christiansen, H. Konzepte zu Grundlagen von ADHS und Interventionen im Unterricht bei Grundschullehrkräften. Psychol. Erzieh. Unterr. 2017, 64, 109–122. [Google Scholar] [CrossRef]
- Ajzen, I. Attitudes, Personality and Behaviour, 2nd ed.; Open University Press: Berkshire, UK, 2005; ISBN 978-0335217038. [Google Scholar]
- Gollwitzer, M.; Thorwart, A.; Meissner, K. Editorial: Psychological Responses to Violations of Expectations. Front. Psychol. 2017, 8, 2357. [Google Scholar] [CrossRef] [Green Version]
- Rief, W.; Glombiewski, J.A.; Gollwitzer, M.; Schubö, A.; Schwarting, R.; Thorwart, A. Expectancies as core features of mental disorders. Curr. Opin. Psychiatry 2015, 28, 378–385. [Google Scholar] [CrossRef]
- Strelow, A.E.; Dort, M.; Schwinger, M.; Christiansen, H. Influences on pre-service teachers’ intention to use classroom management strategies for students with ADHD: A model analysis. Int. J. Educ. Res. 2020, 103, 101627. [Google Scholar] [CrossRef]
- Strelow, A.E.; Dort, M.; Schwinger, M.; Christiansen, H. Influences on Teachers’ Intention to Apply Classroom Management Strategies for Students with ADHD: A Model Analysis. Sustainability 2021, 13, 2558. [Google Scholar] [CrossRef]
- Zemp, M.; Hehlke, L.; Strelow, A.E.; Dort, M.; Christiansen, H. Empirische Arbeit: Einstellung und Intention zum Einsatz (in)effektiver Klassenmanagement-Interventionen von Lehrpersonen und Lehramtsstudierenden bei Schüler*Innen mit ADHS: Eine Replikationsstudie. Psychol. Erzieh. Unterr. 2021, 68. [Google Scholar] [CrossRef]
- Kaff, M.S.; Zabel, R.H.; Milham, M. Revisiting Cost-Benefit Relationships of Behavior Management Strategies: What Special Educators Say About Usefulness, Intensity, and Effectiveness. Prev. Sch. Fail. 2007, 51, 35–45. [Google Scholar] [CrossRef]
- Mulligan, S. Classroom Strategies Used by Teachers of Students with Attention Deficit Hyperactivity Disorder. Phys. Occup. Ther. Pediatr. 2001, 20, 25–44. [Google Scholar] [CrossRef]
- Gaastra, G.F.; Groen, Y.; Tucha, L.; Tucha, O. Unknown, Unloved? Teachers’ Reported Use and Effectiveness of Classroom Management Strategies for Students with Symptoms of ADHD. Child Youth Care Forum 2020, 49, 1–22. [Google Scholar] [CrossRef] [Green Version]
- DuPaul, G.J.; Jimerson, S.R. Assessing, understanding, and supporting students with ADHD at school: Contemporary science, practice, and policy. Sch. Psychol. Q. 2014, 29, 379–384. [Google Scholar] [CrossRef] [Green Version]
- Harazni, L.; Alkaissi, A. The Experience of Mothers and Teachers of Attention Deficit/Hyperactivity Disorder Children, and Their Management Practices for the Behaviors of the Child a Descriptive Phenomenological Study. J. Educ. Pract. 2016, 7, 1–21. [Google Scholar]
- Greene, R.W.; Beszterczey, S.K.; Katzenstein, T.; Park, K.; Goring, J. Are Students with ADHD More Stressful to Teach? J. Emot. Behav. Disord. 2002, 10, 79–89. [Google Scholar] [CrossRef]
- Ward, R.J.; Bristow, S.J.; Kovshoff, H.; Cortese, S.; Kreppner, J. The Effects of ADHD Teacher Training Programs on Teachers and Pupils: A Systematic Review and Meta-Analysis. J. Atten. Disord. 2020. [Google Scholar] [CrossRef]
- Latouche, A.P.; Gascoigne, M. In-Service Training for Increasing Teachers’ ADHD Knowledge and Self-Efficacy. J. Atten. Disord. 2019, 23, 270–281. [Google Scholar] [CrossRef]
- Vereb, R.L.; DiPerna, J.C. Teachers’ Knowledge of ADHD, Treatments for ADHD, and Treatment Acceptability: An Initial Investigation. Sch. Psych. Rev. 2004, 33, 421–428. [Google Scholar] [CrossRef]
- Aguiar, A.P.; Kieling, R.R.; Costa, A.C.; Chardosim, N.; Dorneles, B.V.; Almeida, M.R.; Mazzuca, A.C.; Kieling, C.; Rohde, L.A. Increasing teachers’ knowledge about ADHD and learning disorders: An investigation on the role of a psychoeducational intervention. J. Atten. Disord. 2014, 18, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Hart, K.C.; Fabiano, G.A.; Evans, S.W.; Manos, M.J.; Hannah, J.N.; Vujnovic, R.K. Elementary and Middle School Teachers’ Self-Reported Use of Positive Behavioral Supports for Children with ADHD: A National Survey. J. Emot. Behav. Disord. 2017, 25, 246–256. [Google Scholar] [CrossRef]
- Mohr-Jensen, C.; Steen-Jensen, T.; Bang-Schnack, M.; Thingvad, H. What Do Primary and Secondary School Teachers Know About ADHD in Children? Findings from a Systematic Review and a Representative, Nationwide Sample of Danish Teachers. J. Atten. Disord. 2019, 23, 206–219. [Google Scholar] [CrossRef]
- West, J.; Taylor, M.; Houghton, S.; Hudyma, S. A Comparison of Teachers’ and Parents’ Knowledge and Beliefs About Attention-Deficit/Hyperactivity Disorder (ADHD). Sch. Psychol. Int. 2005, 26, 192–208. [Google Scholar] [CrossRef]
- Martinussen, R.; Tannock, R.; Chaban, P. Teachers’ Reported Use of Instructional and Behavior Management Practices for Students with Behavior Problems: Relationship to Role and Level of Training in ADHD. Child Youth Care Forum 2011, 40, 193–210. [Google Scholar] [CrossRef]
- Bussing, R.; Gary, F.A.; Leon, C.E.; Garvan, C.W.; Reid, R. General Classroom Teachers’ Information and Perceptions of Attention Deficit Hyperactivity Disorder. Behav. Disord. 2002, 27, 327–339. [Google Scholar] [CrossRef]
- OECD. Education at a Glance 2014: OECD Indicators; OECD Publishing: Paris, France, 2014; ISBN 978-92-64-21505-4. [Google Scholar]
- Kos, J.M.; Richdale, A.L.; Jackson, M.S. Knowledge about Attention-Deficit/Hyperactivity Disorder: A comparison of in-service and preservice teachers. Psychol. Sch. 2004, 41, 517–526. [Google Scholar] [CrossRef]
- Sniehotta, F.F.; Schwarzer, R.; Scholz, U.; Schüz, B. Action planning and coping planning for long-term lifestyle change: Theory and assessment. Eur. J. Soc. Psychol. 2005, 35, 565–576. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling Health Behavior Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Dort, M.; Strelow, A.E.; French, B.; Groom, M.; Luman, M.; Thorell, L.B.; Biele, G.; Christiansen, H. Bibliometric Review: Classroom Management in ADHD—Is There a Communication Gap Concerning Knowledge between the Scientific Fields Psychiatry/Psychology and Education? Sustainability 2020, 12, 6826. [Google Scholar] [CrossRef]
- Long, A.C.J.; Hagermoser Sanetti, L.M.; Collier-Meek, M.A.; Gallucci, J.; Altschaefl, M.; Kratochwill, T.R. An exploratory investigation of teachers’ intervention planning and perceived implementation barriers. J. Sch. Psychol. 2016, 55, 1–26. [Google Scholar] [CrossRef]
- Bussing, R.; Koro-Ljungberg, M.; Gagnon, J.C.; Mason, D.M.; Ellison, A.; Noguchi, K.; Garvan, C.W.; Albarracin, D. Feasibility of School-Based ADHD Interventions: A Mixed-Methods Study of Perceptions of Adolescents and Adults. J. Atten. Disord. 2016, 20, 400–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, D.A.; Gwernan-Jones, R.; Richardson, M.; Racey, D.; Rogers, M.; Stein, K.; Thompson-Coon, J.; Ford, T.J.; Garside, R. The experiences of and attitudes toward non-pharmacological interventions for attention-deficit/hyperactivity disorder used in school settings: A systematic review and synthesis of qualitative research. Emot. Behav. Diffic. 2016, 21, 61–82. [Google Scholar] [CrossRef]
- Durlak, J.A.; DuPre, E.P. Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Budge, E.J.; Tsoti, S.M.; Howgate, D.J.; Sivakumar, S.; Jalali, M. Collective intelligence for translational medicine: Crowdsourcing insights and innovation from an interdisciplinary biomedical research community. Ann. Med. 2015, 47, 570–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Han, L.; Stein, G.; Day, S.; Bien-Gund, C.; Mathews, A.; Ong, J.J.; Zhao, P.-Z.; Wei, S.-F.; Walker, J.; et al. Crowdsourcing in health and medical research: A systematic review. Infect. Dis. Poverty 2020, 9, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, S.; Bergenholtz, C.; Bogers, M.; Brasseur, T.-M.; Conradsen, M.L.; Di Marco, D.; Distel, A.P.; Dobusch, L.; Dörler, D.; Effert, A.; et al. The Open Innovation in Science research field: A Collaborative Conceptualisation Approach. Ind. Innov. 2020, 1–50. [Google Scholar] [CrossRef]
- Blackburn, S.; McLachlan, S.; Jowett, S.; Kinghorn, P.; Gill, P.; Higginbottom, A.; Rhodes, C.; Stevenson, F.; Jinks, C. The extent, quality and impact of patient and public involvement in primary care research: A mixed methods study. Res. Involv. Engagem. 2018, 4, 16. [Google Scholar] [CrossRef]
- Brett, J.; Staniszewska, S.; Mockford, C.; Herron-Marx, S.; Hughes, J.; Tysall, C.; Suleman, R. Mapping the impact of patient and public involvement on health and social care research: A systematic review. Health Expect. 2014, 17, 637–650. [Google Scholar] [CrossRef]
- Sherman, J.; Rasmussen, C.; Baydala, L. The impact of teacher factors on achievement and behavioural outcomes of children with Attention Deficit/Hyperactivity Disorder (ADHD): A review of the literature. Educ. Res. 2008, 50, 347–360. [Google Scholar] [CrossRef]
- Statista. Frauenanteil unter den Lehrkräften nach Schulart. 2021. Available online: https://de.statista.com/statistik/daten/studie/1129852/umfrage/frauenanteil-unter-den-lehrkraeften-in-deutschland-nach-schulart/ (accessed on 27 October 2021).
- Leiner, D. SoSci Survey, Version 3.1. 06; SoSci Survey GmbH: München, Germany, 2019. [Google Scholar]
- Kos, J.M.; Richdale, A.L.; Hay, D.A. Children with Attention Deficit Hyperactivity Disorder and Their Teachers: A Review of the Literature. Intl. J. Disabil. Dev. Educ. 2006, 53, 147–160. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 25; IBM SPSS Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Muthén, L.K.; Muthén, B. Mplus User’s Guide: Statistical Analysis with Latent Variables, User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Leiner, D.J. Too Fast, Too Straight, Too Weird: Non-Reactive Indicators for Meaningless Data in Internet Surveys. Surv. Res. Methods 2019, 13, 229–248. [Google Scholar] [CrossRef]
- Enders, C.K. The Performance of the Full Information Maximum Likelihood Estimator in Multiple Regression Models with Missing Data. Educ. Psychol. Meas. 2001, 61, 713–740. [Google Scholar] [CrossRef]
- Barbeau, K.; Boileau, K.; Sarr, F.; Smith, K. Path analysis in Mplus: A tutorial using a conceptual model of psychological and behavioral antecedents of bulimic symptoms in young adults. Quant. Methods Psychol. 2019, 15, 38–53. [Google Scholar] [CrossRef]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Automat. Contr. 1974, 19, 716–723. [Google Scholar] [CrossRef]
- Schwarz, G. Estimating the Dimension of a Model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Huang, P.-H. Asymptotics of AIC, BIC, and RMSEA for Model Selection in Structural Equation Modeling. Psychometrika 2017, 82, 407–426. [Google Scholar] [CrossRef] [PubMed]
- Alkahtani, K.D.F. Teachers’ Knowledge and Misconceptions of Attention Deficit/Hyperactivity Disorder. Psychology 2013, 4, 963–969. [Google Scholar] [CrossRef] [Green Version]
- Falk, C.F.; Muthukrishna, M. Parsimony in model selection: Tools for assessing fit propensity. Psychol. Methods 2021. Advance online publication. [Google Scholar] [CrossRef]
- Epstein, M.; Atkins, M.; Cullinan, D.; Kutash, K.; Weaver, R. Reducing Behavior Problems in the Elementary School Classroom: A Practice Guide (NCEE #2008-012); Institute of Education Sciences: Washington, DC, USA, 2008.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Md | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. FoU | 344 | 759.35 | 144.00 | - | |||||||
| 2. Effectiveness | 349 | 772.47 | 160.32 | 0.54 ** | - | ||||||
| 3. Disruption | 347 | 483.06 | 104.49 | 0.15 ** | −0.02 | - | |||||
| 4. Sex a,e | 354 | 0 | - | −0.17 ** | −0.08 | −0.09 | - | ||||
| 5. School type b,e | 349 | 0 | - | −0.26 ** | −0.14 * | −0.14 * | 0.27 ** | - | |||
| 6. Training c,e | 354 | 1 | - | 0.30 ** | 0.14 ** | −0.02 | −0.11* | −0.07 | - | ||
| 7. Age | 354 | 42.01 | 11.44 | 0.11 ** | 0.07 | −0.06 | 0.01 | −0.02 | 0.26 ** | - | |
| 8. Experience | 338 | 1.67 | 2.27 | 0.12 * | 0.09 | −0.01 | 0.15 ** | 0.16 ** | 0.23 ** | 0.11 * | - |
| 9. Class size | 351 | 20.68 | 4.70 | −0.16 ** | 0.17 | −0.04 | 0.15 ** | 0.43 ** | −0.08 | −0.07 | 0.04 |
| Barriers to Effective CMS Implementation | Primary/SEN School Teachers | Secondary School Teachers | χ2 | df | BF01 |
|---|---|---|---|---|---|
| Too many different teachers for one class | 23.8% | 30.3% | 1.76 | 1 | 0.41 |
| Missing joint arrangements with other teachers about classroom management | 11.0% | 24.6% | 11.02 ** | 1 | 27.78 |
| Lack of time | 37.4% | 44.3% | 1.54 | 1 | 0.40 |
| Class size, too many students in one class | 57.7% | 57.4% | 0.01 | 1 | 0.19 |
| Lack of cooperation with caregivers | 4.8% | 3.3% | 0.47 | 1 | 0.09 |
| Poor cooperation with caregivers | 15.9% | 8.2% | 4.07 * | 1 | 0.99 |
| No flexibility in everyday teaching | 18.1% | 22.1% | 0.84 | 1 | 0.23 |
| Too many students with disabilities in one class | 50.7% | 35.2% | 7.61 ** | 1 | 8.55 |
| Group dynamics in the class make individual support difficult | 15.9% | 13.1% | 0.47 | 1 | 0.17 |
| Lack of knowledge about interventions | 7.9% | 9.0% | 0.12 | 1 | 0.11 |
| Insufficient knowledge transfer during undergraduate studies | 6.6% | 7.4% | 0.73 | 1 | 0.10 |
| Too few teachers in the educational system | 6.6% | 5.7% | 0.10 | 1 | 0.09 |
| No consent from caregivers | 3.5% | 1.6% | 1.01 | 1 | 0.10 |
| (Work)overload of teachers | 23.3% | 22.1% | 0.07 | 1 | 0.16 |
| Lack of practical tools | 12.3% | 9.8% | 0.49 | 1 | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szép, A.; Dantchev, S.; Zemp, M.; Schwinger, M.; Chavanon, M.-L.; Christiansen, H. Facilitators and Barriers of Teachers’ Use of Effective Classroom Management Strategies for Students with ADHD: A Model Analysis Based on Teachers’ Perspectives. Sustainability 2021, 13, 12843. https://doi.org/10.3390/su132212843
Szép A, Dantchev S, Zemp M, Schwinger M, Chavanon M-L, Christiansen H. Facilitators and Barriers of Teachers’ Use of Effective Classroom Management Strategies for Students with ADHD: A Model Analysis Based on Teachers’ Perspectives. Sustainability. 2021; 13(22):12843. https://doi.org/10.3390/su132212843
Chicago/Turabian StyleSzép, Anna, Slava Dantchev, Martina Zemp, Malte Schwinger, Mira-Lynn Chavanon, and Hanna Christiansen. 2021. "Facilitators and Barriers of Teachers’ Use of Effective Classroom Management Strategies for Students with ADHD: A Model Analysis Based on Teachers’ Perspectives" Sustainability 13, no. 22: 12843. https://doi.org/10.3390/su132212843
APA StyleSzép, A., Dantchev, S., Zemp, M., Schwinger, M., Chavanon, M. -L., & Christiansen, H. (2021). Facilitators and Barriers of Teachers’ Use of Effective Classroom Management Strategies for Students with ADHD: A Model Analysis Based on Teachers’ Perspectives. Sustainability, 13(22), 12843. https://doi.org/10.3390/su132212843