
Design and Development of an Instrument on Knowledge of Food Safety, Practices, and Risk Perception Addressed to Children and Adolescents from Low-Income Families

 ,
, 
 , ,
, ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
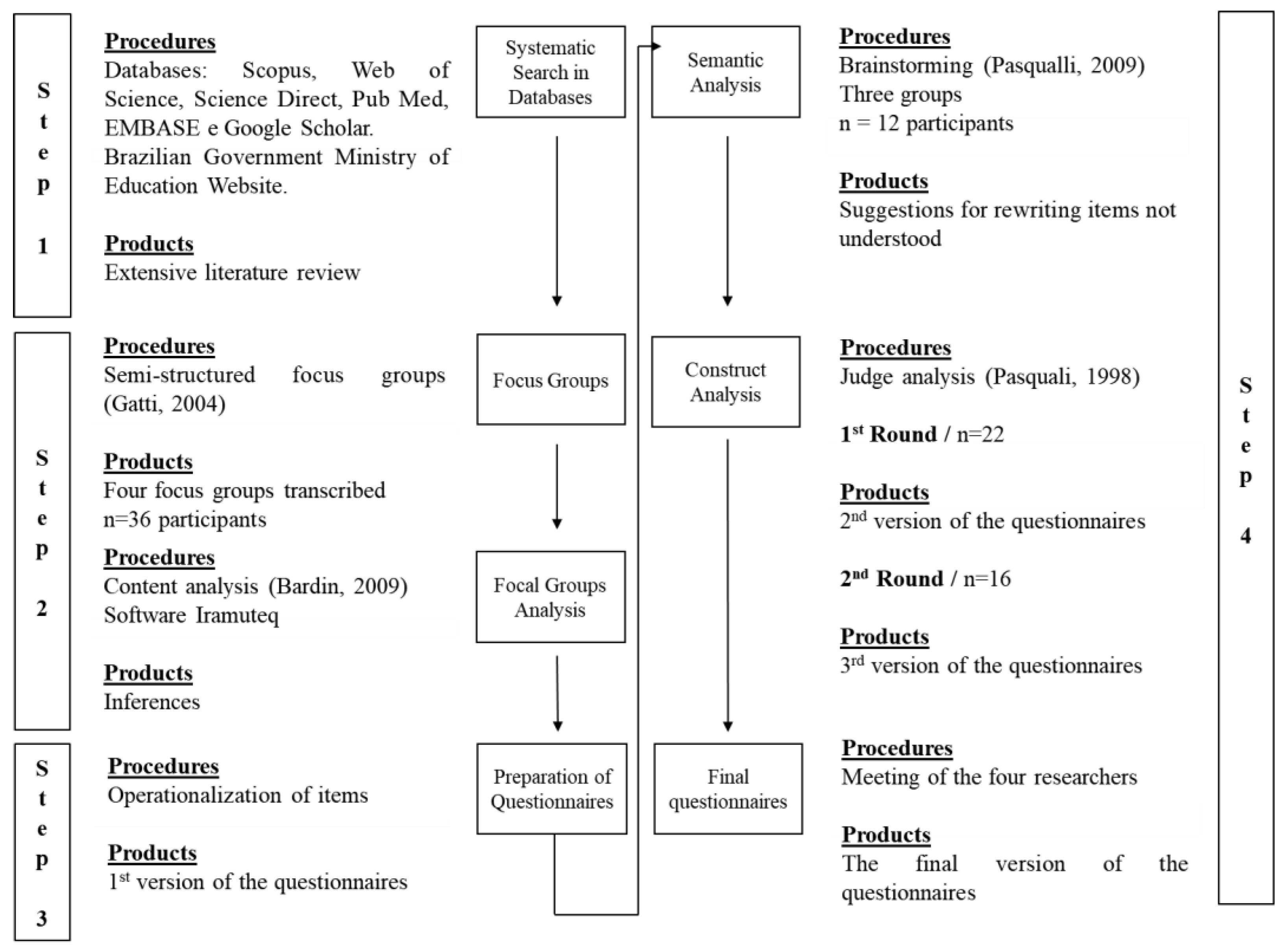
2. Materials and Methods
2.1. Systematic Search in Databases
2.2. Focus Groups (FG) Development and Analysis
2.3. Questionnaires Development
2.4. Questionnaires Analysis
2.4.1. Semantic Analysis
2.4.2. Construct Analysis (Round 1 and 2)
2.4.3. Elaboration of the Final Questionnaires
3. Results and Discussion
3.1. Search in Databases
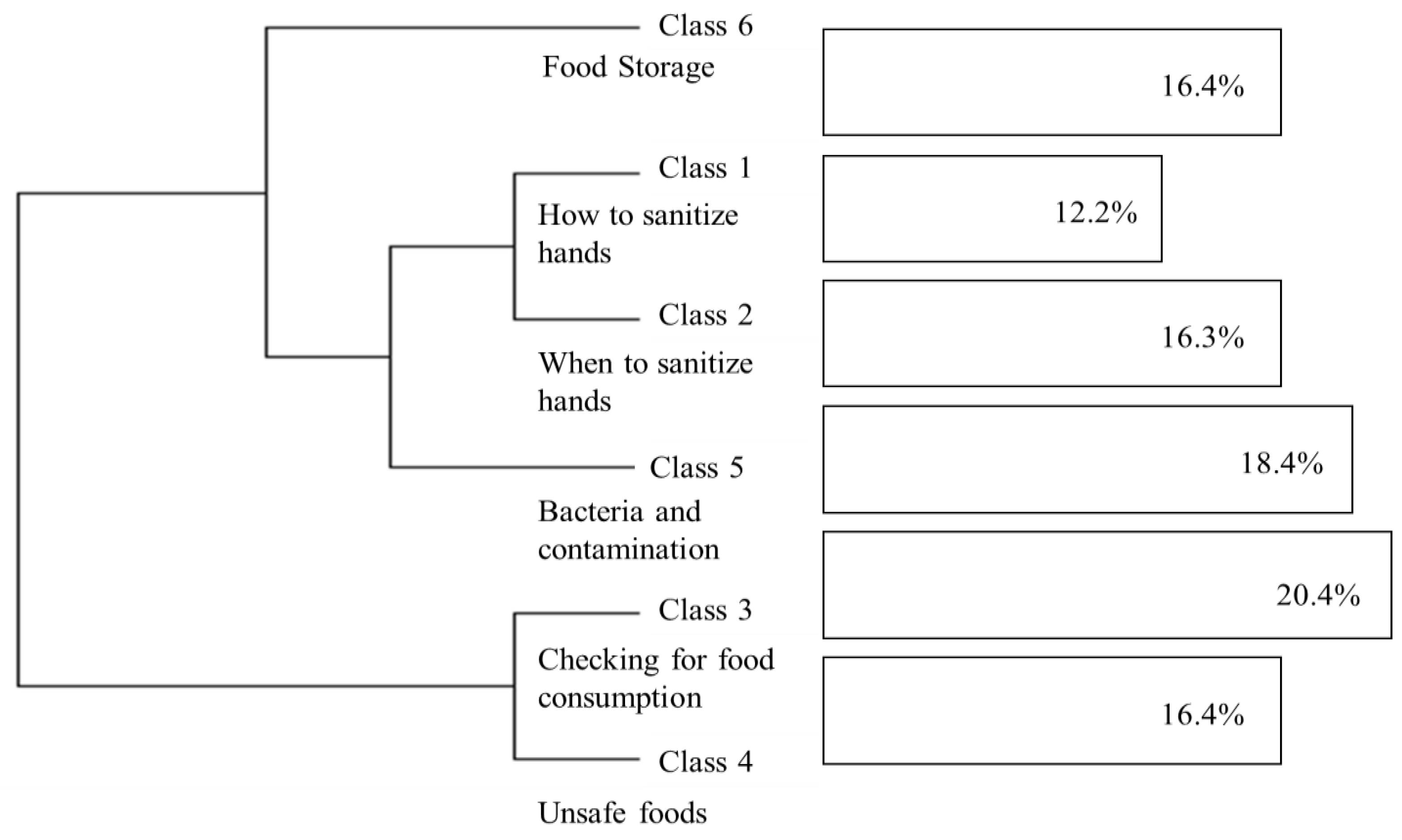
3.2. Conducting and Analyzing Focus Groups (FG)
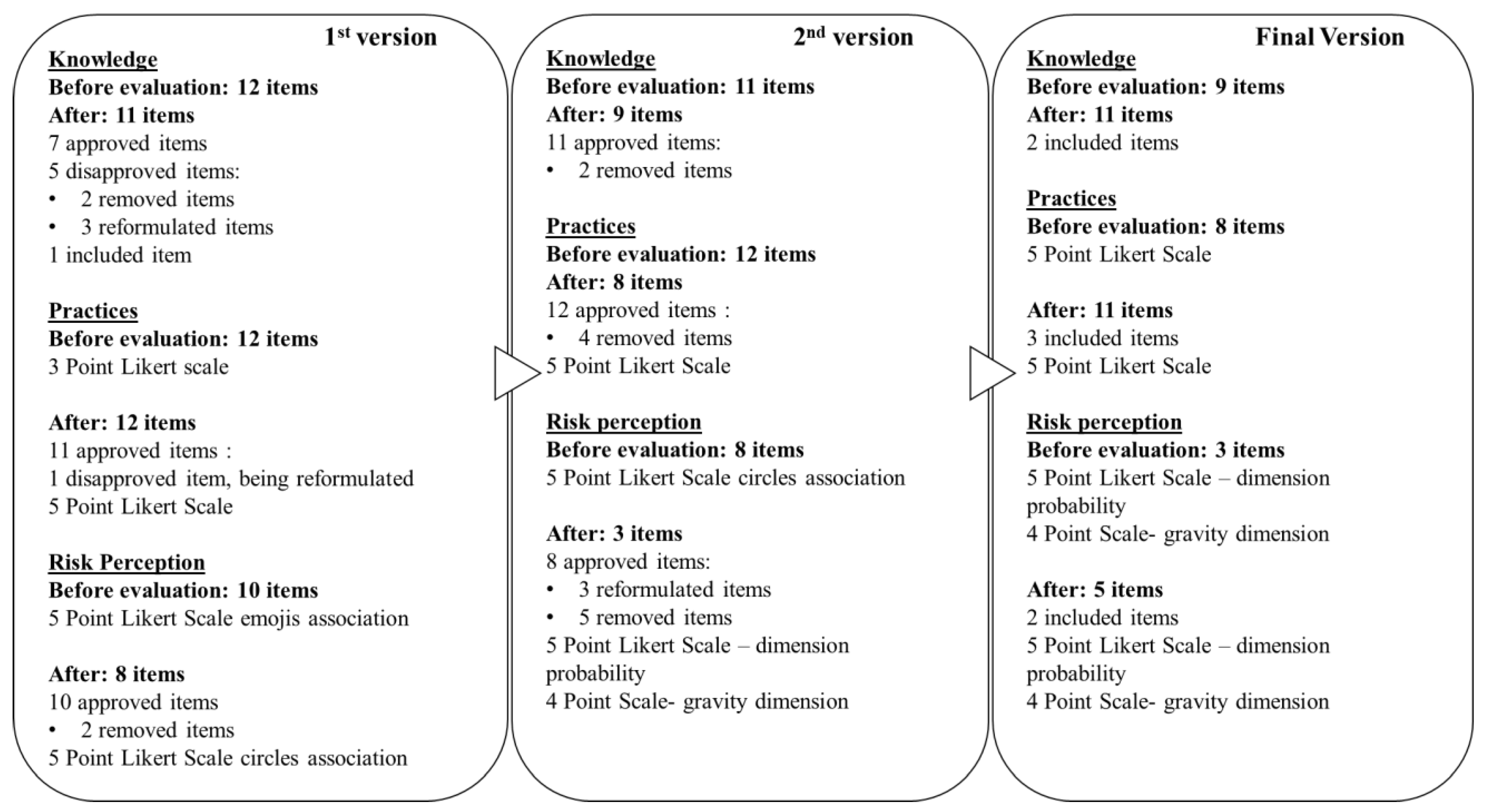
3.3. Questionnaires Development (Questionnaires Analysis)
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Instrument Addressed for Low-Income Children and Adolescents on Food Safety Knowledge, Practices, and Risk Perception
- School__________________________________ Code________ (filled in by the researcher)
- Series __________ Age: ________ years old Area where you live: ( ) Urban ( ) Rural
- Gender: ( ) Female ( ) Male Date: ____ / ____ / 202___
| Make an X ONLY A RECTANGLE that matches your answer. | |
| ATTENTION: GETTING SICK = having stomach pain and/or diarrhea and/or vomiting and/or headache and/or fever because you ate contaminated food. | |
| 1. What is the chance that YOU will get sick from eating food served at your school? | 1.1 If YOU get sick from eating food served at the school you study, how serious could it be? |
 |  |
| 2. What is the chance that a COLLEAGUE who studies with you will get sick from having eaten the same food served at your school? | 2.1 If YOUR COLLEAGUE gets sick from eating food served at the school you study, how serious could it be? |
 |  |
| 3. What is the chance that a person will die from eating contaminated food? | |
 | |
| Examples of how food can be contaminated: | |
- The presence of animal feces in the area where fruits and vegetables are planted;
- The use of pesticides to produce and grow food (fruits, vegetables, cereals such as corn, etc.);
- Due to people’s lack of hygiene when preparing food.
| Code ________ (filled in by the researcher) | |
| Make an X ONLY A RECTANGLE that matches your answer. | |
| ATTENTION: GETTING SICK = having stomach pain and/or diarrhea and/or vomiting and/or headache and/or fever because you ate contaminated food. | |
(1) Do you always need to use soap/soap/detergent to wash your hands correctly? (2) Is using a paper towel to clean a dirty board of raw meat enough to be able to use this board to cut bread? Enough: when you don’t need to do anything else. (3) Should raw meats be kept in the refrigerator on shelves below ready-to-eat foods? Examples of ready-to-eat foods: cake, cooked rice, baked beans. (4) Eating a raw egg or soft yolk can make you sick? (5) Eating food that was out of the fridge for a long time after it was done can make you sick? Ex: Food prepared for lunch that stayed until dinner time on the stove. | (6) Eating foods with a bad smell, bad taste, different texture than usual or moldy, can make you sick? (7) Removing the moldy part of bread before eating reduces or eliminates the chance of you becoming ill? (8) Eating food made in a kitchen that contains flies and other insects can make you sick? (9) To eat raw fruits and vegetables, do you need to wash them using bleach? (10) Can eat fruits and vegetables that have been grown with pesticides make you sick? (11) Does unsafe food to eat always smell foul, look strange, and have a different texture? Unsafe food: food that can make you sick. |
| Code ________ (filled in by the researcher) | |
| Make an X ONLY A RECTANGLE that matches your answer. | |
|
| Examples of fruit: apple, grape, orange. |
 |
|
| IF YOU SCORE IN THE PREVIOUS QUESTION, THE OPTIONS RARELY, SOMETIMES, OFTEN OR ALWAYS OR ALWAYS, ANSWER THE NEXT QUESTIONS: |
|
Thank you!  |
References
- Riesute, R.; Salomskiene, J.; Moreno, D.S.; Gustiene, S. Effect of yeasts on food quality and safety and possibilities of their inhibition. Trends Food Sci. Technol. 2021, 108, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. WHO Estimates of the Global Burden of Foodborne Diseases, 1st ed.; WHO Library Cataloguing-in-Publication Data; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-156516-5. [Google Scholar]
- Hadler, J.L.; Clogher, P.; Libby, T.; Wilson, E.; Oosmanally, N.; Ryan, P.; Magnuson, L.; Lathrop, S.; Mcguire, S.; Cieslak, P.; et al. Relationship Between Census Tract–Level Poverty and Domestically Acquired Salmonella Incidence: Analysis of Foodborne Diseases Active Surveillance Network Data, 2010–2016. J. Infect. Dis. 2019, 222, 1405–1412. [Google Scholar] [CrossRef]
- EFSA; ECDC. The European Union Summary Report on Trends and Sources of Zoonoses, Zoonotic Agents and Food-Borne Outbreaks in 2017; Wiley-Blackwell Publishing Ltd.: Hoboken, NJ, USA, 2018; Volume 16. [Google Scholar]
- Draeger, C.; Akutsu, R.; Zandonadi, R.; da Silva, I.; Botelho, R.; Araújo, W. Brazilian Foodborne Disease National Survey: Evaluating the Landscape after 11 Years of Implementation to Advance Research, Policy, and Practice in Public Health. Nutrients 2019, 11, 40. [Google Scholar] [CrossRef] [Green Version]
- Dubugras, M.T.B.; Pérez-Gutiérrez, E. Perspectiva Sobre a Análise de Risco na Segurança dos Alimentos; PAHO: Rio de Janeiro, Brazil, 2008. [Google Scholar]
- WHO. A Guide to Healthy Food Markets; WHO: Geneva, Switzerland, 2006; ISBN 0201398257. [Google Scholar]
- De Andrade, M.L.; Rodrigues, R.R.; Antongiovanni, N.; da Cunha, D.T. Knowledge and risk perceptions of foodborne disease by consumers and food handlers at restaurants with different food safety profiles. Food Res. Int. 2019, 121, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Zhang, Y.; Ma, J.; Zhan, S. Food safety knowledge, attitude and self-reported practice of secondary school students in Beijing, China: A cross-sectional study. PLoS ONE 2017, 12, e0187208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Freitas, R.S.G.; da Cunha, D.T.; Stedefeldt, E. Food safety knowledge as gateway to cognitive illusions of food handlers and the different degrees of risk perception. Food Res. Int. 2019, 116, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Xu, X.; Chen, H.; Bai, R.; Zhang, Y.Y.; Hou, X.; Zhang, F.; Zhang, Y.Y.; Sharma, M.; Zeng, H.; et al. Food safety related knowledge, attitudes, and practices (KAP) among the students from nursing, education and medical college in Chongqing, China. Food Control 2019, 95, 181–188. [Google Scholar] [CrossRef]
- Marklinder, I.; Ahlgren, R.; Blücher, A.; Ehn Börjesson, S.M.; Hellkvist, F.; Moazzami, M.; Schelin, J.; Zetterström, E.; Eskhult, G.; Danielsson-Tham, M.L. Food safety knowledge, sources thereof and self-reported behaviour among university students in Sweden. Food Control 2020, 113, 107130. [Google Scholar] [CrossRef]
- Ovca, A.; Jevšnik, M.; Kavčič, M.; Raspor, P. Food safety knowledge and attitudes among future professional food handlers. Food Control 2018, 84, 345–353. [Google Scholar] [CrossRef]
- Rossi, M.d.S.C.; Stedefeldt, E.; da Cunha, D.T.; de Rosso, V.V. Food safety knowledge, optimistic bias and risk perception among food handlers in institutional food services. Food Control 2017, 73, 681–688. [Google Scholar] [CrossRef]
- Baptista, R.C.; Rodrigues, H.; Sant’Ana, A.S. Consumption, knowledge, and food safety practices of Brazilian seafood consumers. Food Res. Int. 2020, 132, 109084. [Google Scholar] [CrossRef]
- Da Cunha, D.T.; Stedefeldt, E.; de Rosso, V.V. The role of theoretical food safety training on Brazilian food handlers’ knowledge, attitude and practice. Food Control 2014, 43, 167–174. [Google Scholar] [CrossRef]
- Haapala, I.; Probart, C. Food safety knowledge, perceptions, and behaviors among middle school students. J. Nutr. Educ. Behav. 2004, 36, 71–76. [Google Scholar] [CrossRef]
- Meysenburg, R.; Albrecht, J.A.; Litchfield, R.; Ritter-Gooder, P.K. Food safety knowledge, practices and beliefs of primary food preparers in families with young children. A mixed methods study. Appetite 2014, 73, 121–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osei Tutu, B.; Hushie, C.; Asante, R.; Egyakwa-Amusah, J.A. Food safety knowledge and self-reported practices among school children in the Ga West Municipality in Ghana. Food Control 2019, 110, 107012. [Google Scholar] [CrossRef]
- Teh, N.S.A.; Hamid, M.R.A.; Asmawi, U.M.M.; Nor, N.M. Food Hygiene’s Knowledge, Attitudes and Practices between Urban and Suburban Adolescents. Procedia—Soc. Behav. Sci. 2016, 234, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Tabile, A.F.; Jacometo, M.C.D. Fatores influenciadores no processo de aprendizagem: Um estudo de caso. Rev. Psicopedag. 2017, 34, 75–86. [Google Scholar]
- Byrd-Bredbenner, C.; Abbot, J.M.; Quick, V. Food safety knowledge and beliefs of middle school children: Implications for food safety educators: Research in food science education. J. Food Sci. Educ. 2010, 9, 19–30. [Google Scholar] [CrossRef]
- Eves, A.; Bielby, G.; Egan, B.; Lumbers, M.; Raats, M.; Adams, M. Food hygiene knowledge and self-reported behaviours of UK school children (4–14 years). Br. Food J. 2006, 108, 706–720. [Google Scholar] [CrossRef]
- Young, V.L.; Brown, C.L.; Hayes, C.; McNulty, C.A.M. Review of risk communication and education strategies around food hygiene and safety for children and young people. Trends Food Sci. Technol. 2018, 84, 64–67. [Google Scholar] [CrossRef]
- Martin Romero, M.Y.; Francis, L.A. Youth involvement in food preparation practices at home: A multi-method exploration of Latinx youth experiences and perspectives. Appetite 2020, 144, 104439. [Google Scholar] [CrossRef]
- Berge, J.M.; MacLehose, R.F.; Larson, N.; Laska, M.; Neumark-Sztainer, D. Family Food Preparation and Its Effects on Adolescent Dietary Quality and Eating Patterns. J. Adolesc. Health 2016, 59, 530–536. [Google Scholar] [CrossRef] [Green Version]
- Chu, Y.L.; Storey, K.E.; Veugelers, P.J. Involvement in Meal Preparation at Home Is Associated With Better Diet Quality Among Canadian Children. J. Nutr. Educ. Behav. 2014, 46, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Ovca, A.; Jevšnik, M.; Raspor, P. Food safety awareness, knowledge and practices among students in Slovenia. Food Control 2014, 42, 144–151. [Google Scholar] [CrossRef]
- Sattler, M.; Hopkins, L.; Anderson Steeves, E.; Cristello, A.; Mccloskey, M.; Gittelsohn, J.; Hurley, K. Characteristics of Youth Food Preparation in Low-Income, African American Homes: Associations with Healthy Eating Index Scores. Ecol. Food Nutr. 2015, 54, 380–396. [Google Scholar] [CrossRef] [Green Version]
- Mullan, B.A.; Wong, C.; Kothe, E.J. Predicting adolescents ’ safe food handling using an extended theory of planned behavior. Food Control 2013, 31, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde. Surtos de Doenças Transmitidas por alimentos no Brasil; Ministério da Saúde: Brasília, Brazil, 2019. [Google Scholar]
- Marchi, D.M.; Baggio, N.; Teo, C.R.P.A.; Busato, M.A. Ocorrência de surtos de doenças transmitidas por alimentos no Município de Chapecó, Estado de Santa Catarina, Brasil, no período de 1995 a 2007. Epidemiologia e Serviços Saúde 2011, 20, 401–407. [Google Scholar] [CrossRef]
- Moreb, N.A.; Priyadarshini, A.; Jaiswal, A.K. Knowledge of food safety and food handling practices amongst food handlers in the Republic of Ireland. Food Control 2017, 80, 341–349. [Google Scholar] [CrossRef] [Green Version]
- Kuo, S.C.; Weng, Y.M. Food safety knowledge, attitude, and practice among elementary schoolchildren in southern Taiwan. Food Control 2021, 122, 107818. [Google Scholar] [CrossRef]
- Gautam, O.P.; Schmidt, W.P.; Cairncross, S.; Cavill, S.; Curtis, V. Trial of a novel intervention to improve multiple food hygiene behaviors in Nepal. Am. J. Trop. Med. Hyg. 2017, 96, 1415–1426. [Google Scholar] [CrossRef]
- Hoffmann, V.; Moser, C.; Saak, A. Food safety in low and middle-income countries: The evidence through an economic lens. World Dev. 2019, 123, 104611. [Google Scholar] [CrossRef]
- Nizame, F.A.; Leontsini, E.; Luby, S.P.; Nuruzzaman, M.; Parveen, S.; Winch, P.J.; Ram, P.K.; Unicomb, L. Hygiene practices during food preparation in Rural Bangladesh: Opportunities to improve the impact of handwashing interventions. Am. J. Trop. Med. Hyg. 2016, 95, 288–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, M.; Göranzon, H.; Marklinder, I. “Teaching Young Consumers”—Food safety in home and consumer studies from a teacher’s perspective. Int. J. Consum. Stud. 2014, 38, 357–366. [Google Scholar] [CrossRef]
- Pawlowski, J.; Trentini, C.M.; Bandeira, D.R. Discutindo procedimentos psicométricos a partir da análise de um instrumento de avaliação neuropsicológica breve. Psico-USF 2007, 12, 211–219. [Google Scholar] [CrossRef]
- OPAS. Segurança dos Alimentos é Responsabilidade de Todos. Available online: https://www.paho.org/bra/index.php?option=com_content&view=article&id=5960:seguranca-dos-alimentos-e-responsabilidade-de-todos&Itemid=875 (accessed on 13 January 2020).
- Ministério da Educação. Brasil no PISA 2015: Análises e Reflexões Sobre o Desempenho dos Estudantes Brasileiros; Câmara Brasileira do Livro: São Paulo, Brazil, 2016; p. 273. [Google Scholar]
- Alexandre, N.M.C.; Coluci, M.Z.O. Validade de conteúdo nos processos de construção e adaptação de instrumentos de medidas. Ciência e Saúde Coletiva 2011, 16, 3061–3068. [Google Scholar] [CrossRef] [PubMed]
- Pasquali, L. Princípios de elaboração de escalas psicológicas. Rev. Psiquiatr. Clínica 1998, 25, 206–2013. [Google Scholar]
- Recommended international code of practice general principles of food hygiene. In Codex Alimentarius; CAC/RCP: Vienna, Austria, 2003.
- Ministry of Health of Brazil. Brazil Resolução RDC n° 216, de 15 de Setembro de 2004; Ministry of Health of Brazil: Brasília, Brazil, 2004; pp. 1–14. [Google Scholar]
- Ministry of Health of Brazil. Brazil Instrução Normativa DIVISA/SVS No 16, de 23 de maio de 2017; Ministry of Health of Brazil: Brasília, Brazil, 2017; pp. 1–23. [Google Scholar]
- Ministério da Educação. Base Nacional Comum Curricular: Educação é a base; Ministério da Educação: Brasília, Brazil, 2018. [Google Scholar]
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change1. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef]
- WHO. Five Keys to Safer Food Manual; WHO: Geneva, Switzerland, 2006; ISBN 978-972-8643-34-8. [Google Scholar]
- Da Cunha, D.T.; Stedefeldt, E.; de Rosso, V.V. He is worse than I am: The positive outlook of food handlers about foodborne disease. Food Qual. Prefer. 2014, 35, 95–97. [Google Scholar] [CrossRef]
- Gatti, B.A. Grupo Focal na Pesquisa em Ciência Sociais e Humanas; Líber Livro: Brasília, Brazil, 2005. [Google Scholar]
- Gavaravarapu, S.R.M.; Vemula, S.R.; Rao, P.; Mendu, V.V.R.; Polasa, K. Focus Group Studies on Food Safety Knowledge, Perceptions, and Practices of School-going Adolescent Girls in South India. J. Nutr. Educ. Behav. 2009, 41, 340–346. [Google Scholar] [CrossRef]
- Ratinaud, P. Iramuteq—IRaMuTeQ 2014. Available online: http://www.iramuteq.org (accessed on 13 March 2020).
- Bardin, L. Análise de Conteúdo; Edições 70: São Paulo, Brazil, 2011. [Google Scholar]
- Camargo, B.V.; Justo, A.M. Tutorial Para Uso do Software de Análise Textual IRAMUTEQ; Universidade Federal de Santa Catarina: Florianópolis, Santa Catarina, Brasil, 2013. [Google Scholar]
- De Andrade, M.L.; Stedefeldt, E.; Zanin, L.M.; da Cunha, D.T. Food safety culture in food services with different degrees of risk for foodborne diseases in Brazil. Food Control 2020, 112, 107152. [Google Scholar] [CrossRef]
- Slovic, P. Perception of Risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, N.D. Why it won’t happen to me: Perceptions of risk factors and susceptibility. Health Psychol. 1984, 3, 431–457. [Google Scholar] [CrossRef]
- Da Cunha, D.T. Viés Otimista, Percepção de Risco e Ilusão de Controle de Manipuladores de Alimentos: Discutindo Conhecimentos, Atitudes e Práticas; Universidade Federal de São Paulo: São Paulo, Brazil, 2014. [Google Scholar]
- Whalen, C.K.; Henker, B.; O’Neil, R.; Hollingshead, J.; Holman, A.; Moore, B. Optimism in Children’s Judgments of Health and Environmental Risks. Health Psychol. 1994, 13, 319–325. [Google Scholar] [CrossRef]
- Swaney-Stueve, M.; Jepsen, T.; Deubler, G. The emoji scale: A facial scale for the 21st century. Food Qual. Prefer. 2018, 68, 183–190. [Google Scholar] [CrossRef]
- Medeiros, R.K.d.S.; Ferreira Júnior, M.A.; Torres, G.d.V.; Vitor, A.F.; Santos, V.E.P.; Barichello, E. Validação de conteúdo de instrumento sobre a habilidade em sondagem nasogástrica. Rev. Eletrônica Enferm. 2015, 17, 278–289. [Google Scholar] [CrossRef] [Green Version]
- Nauta, M.J.; Fischer, A.R.H.; Van Asselt, E.D.; De Jong, A.E.I.; Frewer, L.J.; De Jonge, R. Food safety in the domestic environment: The effect of consumer risk information on human disease risks. Risk Anal. 2008, 28, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Kreimeier, S.; Greiner, W. EQ-5D-Y as a Health-Related Quality of Life Instrument for Children and Adolescents: The Instrument’s Characteristics, Development, Current Use, and Challenges of Developing Its Value Set. Value Health 2019, 22, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Wille, N.; Badia, X.; Bonsel, G.; Burström, K.; Cavrini, G.; Devlin, N.; Egmar, A.; Greiner, W.; Gusi, N.; Herdman, M.; et al. Development of the EQ-5D-Y: A child-friendly version of the EQ-5D. Qual. Life Res. 2010, 19, 875–886. [Google Scholar] [CrossRef] [Green Version]
- Ohara, K.; Nakamura, H.; Kouda, K.; Fujita, Y.; Momoi, K.; Mase, T.; Carroll, C.; Iki, M. Psychometric properties of the Japanese version of the Dutch Eating Behavior Questionnaire for Children. Appetite 2020, 151, 104690. [Google Scholar] [CrossRef]
- WHO. Quantitative Microbial Risk Assessment: Application for water safety management. In Routledge Handbook of Water and Health; CRC: Boca Raton, FL, USA, 2016; pp. 558–569. [Google Scholar] [CrossRef]
- ISO. Risk management—Principles and guidelines; NBR ISO 31000; ISO: Geneva, Switzerland.
- Joshi, M.S.; Maclean, M.; Stevens, C. Accident frequency and unrealistic optimism: Children ’ s assessment of risk. Accid. Anal. Prev. 2018, 111, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Instituto de Pesquisa Econômica Aplicada. Agenda 2030: Objetivos do Desenvolvimento Sustentável—Metas Brasileiras; Instituto de Pesquisa Econômica Aplicada: Brasília, Distrito Federal, Brazil, 2018. [Google Scholar]
- Ministério da Saúde. Guia Alimentar Para a População Brasileira; Ministério da Saúde: Brasília, Brasil, 2014; Volume 2, p. 158. [Google Scholar]
- Aldanondo-Ochoa, A.M.; Almansa-Sáez, C. The private provision of public environment: Consumer preferences for organic production systems. Land Use Policy 2009, 26, 669–682. [Google Scholar] [CrossRef]
- Feil, A.A.; Cyrne, C.C.d.S.; Sindelar, F.C.W.; Barden, J.E.; Dalmoro, M. Profiles of sustainable food consumption: Consumer behavior toward organic food in southern region of Brazil. J. Clean. Prod. 2020, 258, 120690. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Contexts of child rearing: Problems and prospects. Am. Psychol. 1979, 34, 844–850. [Google Scholar] [CrossRef]
- Cala, V.C.; Soriano, E. Health Education from an Ecological Perspective. Adaptation of the Bronfenbrenner Model from an Experience with Adolescents. Procedia—Soc. Behav. Sci. 2014, 132, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Sirasa, F.; Mitchell, L.; Silva, R.; Harris, N. Factors influencing the food choices of urban Sri Lankan preschool children: Focus groups with parents and caregivers. Appetite 2020, 150, 104649. [Google Scholar] [CrossRef] [PubMed]
- Brazil Pesquisa Nacional por Amostra de Domicílios (PNAD): Segurança Alimentar; IBGE: Rio de Janeiro, Brazil, 2004; p. 140.
- Brazil Pesquisa Nacional por Amostra de Domicílios—Segurança Alimentar 2004/2009; IBGE: Rio de Janeiro, Brazil, 2010; Volume 41, p. 188.
- Brazil Pesquisa Nacional por Amostra de Domicílios (PNAD): Segurança Alimentar; IBGE: Rio de Janeiro, Brazil, 2014; Volume 39, pp. 1–63.
- Brazil Pesquisa Nacional de Demografia e Saúde da Mulher e da Criança—PNDS 2006; CEBRAP: São Paulo, Brazil, 2009.
- Morais, D.d.C.; Dutra, L.V.; Franceschini, S.d.C.C.; Priore, S.E. Insegurança alimentar e indicadores antropométricos, dietéticos e sociais em estudos brasileiros: Uma revisão sistemática. Ciencia e Saude Coletiva 2014, 19, 1475–1488. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Doenças Transmissíveis Pela Comida Matam 420 mil Pessoas por ano no Mundo; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Pinto, V.R.A.; Teixeira, C.G.; Lima, T.S.; De Almeida Prata, E.R.B.; Vidigal, M.C.T.R.; Martins, E.; Perrone, Í.T.; de Carvalho, A.F. Health beliefs towards kefir correlate with emotion and attitude: A study using an emoji scale in Brazil. Food Res. Int. 2020, 129, 108833. [Google Scholar] [CrossRef]
- Dalmoro, M.; Vieira, K.M. Dilemas na Construção de Escalas Tipo Likert: O Número de Itens e a Disposição Influenciam nos Resultados? Rev. Gestão Organ. 2013, 6, 161–174. [Google Scholar] [CrossRef]
- Gordis, L. Epidemiologia, 4th ed.; Revinter: Rio de Janeiro, Brazil, 2010. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Themes—Keys to Safer Food | Units of Record | FG1 | FG2 | FG3 | FG4 | Total by UR | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| F | % | F | % | F | % | F | % | F | % | ||
| Keep it clean | Hand hygiene/Bacterial contamination | 17 | 26 | 23 | 36 | 11 | 17 | 12 | 21 | 63 | 39 |
| Separate raw and cooked foods | Cross-contamination | 1 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| Cook the food well | Proper cooking | 0 | 0 | 1 | 100 | 0 | 0 | 0 | 0 | 1 | 0 |
| Keep food at safe temperatures | Food storage | 2 | 20 | 2 | 20 | 1 | 10 | 5 | 50 | 10 | 6 |
| Use safe water and safe raw materials | Sanitation of fruits and vegetables | 0 | 0 | 2 | 8 | 15 | 62 | 7 | 30 | 24 | 15 |
| Safe/unsafe food | 15 | 25 | 13 | 21 | 22 | 36 | 10 | 18 | 60 | 40 | |
| Keys to Safer Food | Evocations |
|---|---|
| Keep it clean | Hand hygiene/Bacterial contamination |
| “If we do not wash our hands, we can infect the food, and we will eat the infected food, and the bacteria will infect us from the inside. It is always good to wash your hands if you touch the floor or something dirty.” | |
| “Bacteria are tiny animals. If I touch the floor, it is full of bacteria there. Bacteria are everywhere.” | |
| “You put the soap in your hand. We have to wash our hands up to the elbow. ” | |
| Separate raw and cooked foods | Cross-contamination |
| “If you combine the moldy food with other foods, the clean one can get mold from the one that you put together.” | |
| Keep food at safe temperatures | Food Storage |
| “You can keep the whole papaya in a warm place; when opened, you can store it in the refrigerator.” | |
| “If we are going to save food to eat today or tomorrow, we will store it in the refrigerator. If we are going to save it for a week or later, it is better to save it in the freezer.” | |
| Use safe water and safe raw materials | Checking food for consumption |
| “From the smell of fish if it is spoiled fish. Auntie, if it is food that comes in the bag, you can see the date on the label when it expires or because of the smell like beans.” | |
| “There are some rotten. Others get softer sometimes.” | |
| “When it expires. When it does not smell good. When the fly is climbing on top of that bad smell. Like milk. It stinks. The egg stinks when it gets rotten.” | |
| “Expiration of food is when you want to eat something, and it has been in your cabinet for a long time, and you hardly eat it, and it has passed its expiration date, and if you eat it can give you a stomach ache or even kill the person.” | |
| Safe/unsafe food | |
| “Unsafe food is fried, soda, fats, sweets, snacks.” | |
| “Unsafe foods are those that have pesticides. If we eat food that has pesticides for several years, we will die. Get stomach pain and diarrhea.” | |
| “Safe food is that there is no poison, that there is no animal.” | |
| “Safe foods for me are those that do not have pesticides and those that we grow.” | |
| “There are things that smell bad, but it is good to eat. Some look bad, but they are good. Some are bad, but they are good.” | |
| Sanitation of fruits and vegetables | |
| “Some foods have to put on bleach, like lettuce and tomatoes. And there are some foods that we have to boil.” | |
| “You have to soak the fruit, and then put a little bleach in it, then let it soak, to remove most of the microbes.” | |
| “I do not eat a thing with bleach in my food.” | |
| “Bleach? That is crazy, dude?” |
| Items | I-CVI | |||||
|---|---|---|---|---|---|---|
| Risk Perception | Knowledge | Practices | ||||
| V1 | V2 | V1 | V2 | V1 | V2 | |
| 1 | 0.93 | 0.99 | 0.84 | 1 | 0.93 | 0.98 |
| 2 | 0.84 | 0.95 | 0.77 | 0.9 | 0.93 | 0.96 |
| 3 | 0.86 | 0.98 | 0.79 | 0.88 | 0.88 | 0.86 |
| 4 | 0.86 | 0.93 | 0.85 | 0.99 | 0.85 | 0.98 |
| 5 | 0.88 | 0.94 | 0.76 | 0.89 | 0.89 | 0.99 |
| 6 | 0.87 | 1 | 0.82 | 1 | 0.85 | 0.9 |
| 7 | 0.91 | 1 | 0.79 | 1 | 0.92 | 0.98 |
| 8 | 0.84 | 1 | 0.9 | 0.9 | 0.95 | 1 |
| 9 | 0.94 | - | 0.86 | 0.93 | 0.88 | 0.96 |
| 10 | 0.88 | - | 0.79 | 0.95 | 0.84 | 0.99 |
| 11 | - | - | 0.84 | 0.93 | 0.78 | 0.96 |
| 12 | - | - | 0.93 | - | 0.87 | 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batista, S.A.; Stedefeldt, E.; Nakano, E.Y.; Cortes, M.d.O.; Botelho, R.B.A.; Zandonadi, R.P.; Raposo, A.; Han, H.; Ginani, V.C. Design and Development of an Instrument on Knowledge of Food Safety, Practices, and Risk Perception Addressed to Children and Adolescents from Low-Income Families. Sustainability 2021, 13, 2324. https://doi.org/10.3390/su13042324
Batista SA, Stedefeldt E, Nakano EY, Cortes MdO, Botelho RBA, Zandonadi RP, Raposo A, Han H, Ginani VC. Design and Development of an Instrument on Knowledge of Food Safety, Practices, and Risk Perception Addressed to Children and Adolescents from Low-Income Families. Sustainability. 2021; 13(4):2324. https://doi.org/10.3390/su13042324
Chicago/Turabian StyleBatista, Sueny Andrade, Elke Stedefeldt, Eduardo Yoshio Nakano, Mariana de Oliveira Cortes, Raquel Braz Assunção Botelho, Renata Puppin Zandonadi, António Raposo, Heesup Han, and Verônica Cortez Ginani. 2021. "Design and Development of an Instrument on Knowledge of Food Safety, Practices, and Risk Perception Addressed to Children and Adolescents from Low-Income Families" Sustainability 13, no. 4: 2324. https://doi.org/10.3390/su13042324
APA StyleBatista, S. A., Stedefeldt, E., Nakano, E. Y., Cortes, M. d. O., Botelho, R. B. A., Zandonadi, R. P., Raposo, A., Han, H., & Ginani, V. C. (2021). Design and Development of an Instrument on Knowledge of Food Safety, Practices, and Risk Perception Addressed to Children and Adolescents from Low-Income Families. Sustainability, 13(4), 2324. https://doi.org/10.3390/su13042324