Bovine Colostrum Supplementation During Running Training Increases Intestinal Permeability


Abstract
:1. Introduction
2. Results and Discussion
2.1. Age, Height and Mass
2.2. Exercise Parameters
Peak oxygen uptake ( ![Nutrients 01 00224 i001]() )
)

{kind=link}
 ) between groups at Week 0 (BC 52.8 ± 1.6 mL·kg-1·min-1, WP 53.1 ± 2.0 mL·kg-1·min-1, CON 57.3 ± 3.0 mL·kg-1·min-1; P = 0.15). While peak tended to increase in all groups (BC 0.6 ± 1.3 mL·kg-1·min-1, WP 0.2 ± 1.6 ml·kg-1·min-1, CON 2.2 ± 1.0 mL·kg-1·min-1), this did not reach statistical significance (P = 0.22).
) between groups at Week 0 (BC 52.8 ± 1.6 mL·kg-1·min-1, WP 53.1 ± 2.0 mL·kg-1·min-1, CON 57.3 ± 3.0 mL·kg-1·min-1; P = 0.15). While peak tended to increase in all groups (BC 0.6 ± 1.3 mL·kg-1·min-1, WP 0.2 ± 1.6 ml·kg-1·min-1, CON 2.2 ± 1.0 mL·kg-1·min-1), this did not reach statistical significance (P = 0.22). Exercise duration
Peak Heart Rate (HR)
HR at lactate threshold (i.e. training HR [HRt])
2.3. Dietary Intake
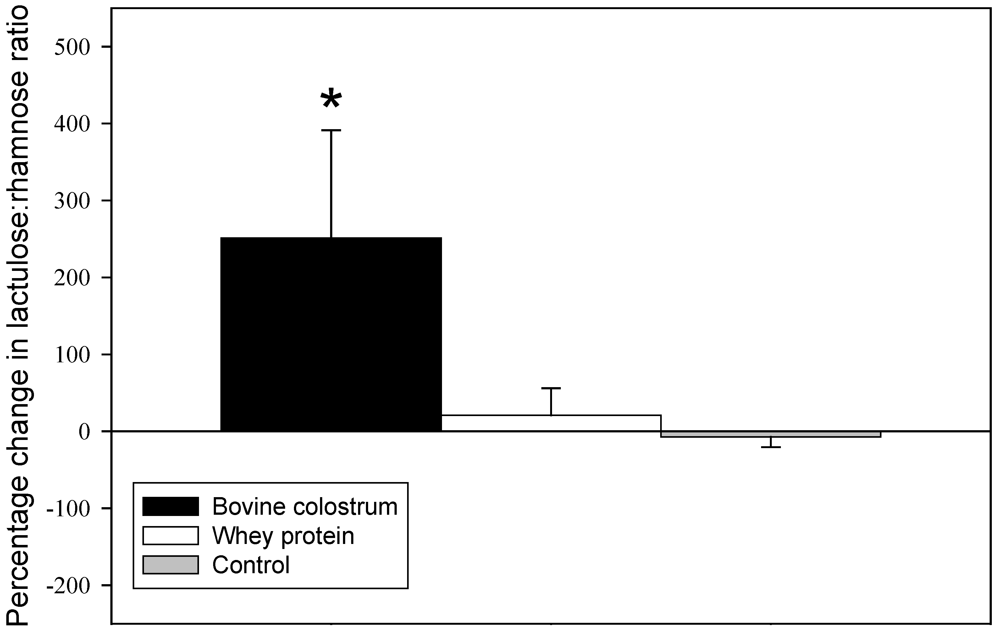
2.4. Intestinal Permeability
 . Nevertheless, the increase in intestinal permeability with BC supplementation was a somewhat unexpected finding given that BC has been shown to attenuate the intestinal hyperpermeability induced by non-steroidal anti-inflammatory drugs (NSAIDs) [11]. The finding of an increase in permeability suggests that in healthy adult gut BC might induce an opposite effect and increase the leakiness of tight junctions between enterocytes, although no participants reported any adverse gastrointestinal symptoms. Alternatively, this finding could be interpreted as indicating that BC increased the intestinal transport of larger molecules. Colostrum contains components which facilitate intestinal macromolecular transport in neonates prior to gut closure [12,13], with the increased transport being ascribed to colostral proteinase inhibitors protecting against molecular digestion and bioactive components stimulating transport pathways [12,13]. The lactulose/rhamnose test of intestinal permeability employed in the current study is based on the assumption that rhamnose, a relatively small monosaccharide (164 Da), will permeate the epithelia transcellulary, while the larger lactulose disaccharide molecule (342 Da) will only be absorbed paracellulary through the tight junctions between the epithelial cells [14]. The test is not able to specifically determine the pathway by which lactulose is transported across the intestinal epithelium and it is possible that BC increased paracellular transport by increasing the gaps between the tight junctions of enteroendocytes, but it also cannot be ruled out that BC may have increased intestinal transport by endocytosis or some other mechanism, as it does in neonatal animals. If this were the case then some of the bioactive components in BC which promote macromolecular transport in the neonatal gut [12] might also facilitate the transport of larger molecules in the adult human gut.
. Nevertheless, the increase in intestinal permeability with BC supplementation was a somewhat unexpected finding given that BC has been shown to attenuate the intestinal hyperpermeability induced by non-steroidal anti-inflammatory drugs (NSAIDs) [11]. The finding of an increase in permeability suggests that in healthy adult gut BC might induce an opposite effect and increase the leakiness of tight junctions between enterocytes, although no participants reported any adverse gastrointestinal symptoms. Alternatively, this finding could be interpreted as indicating that BC increased the intestinal transport of larger molecules. Colostrum contains components which facilitate intestinal macromolecular transport in neonates prior to gut closure [12,13], with the increased transport being ascribed to colostral proteinase inhibitors protecting against molecular digestion and bioactive components stimulating transport pathways [12,13]. The lactulose/rhamnose test of intestinal permeability employed in the current study is based on the assumption that rhamnose, a relatively small monosaccharide (164 Da), will permeate the epithelia transcellulary, while the larger lactulose disaccharide molecule (342 Da) will only be absorbed paracellulary through the tight junctions between the epithelial cells [14]. The test is not able to specifically determine the pathway by which lactulose is transported across the intestinal epithelium and it is possible that BC increased paracellular transport by increasing the gaps between the tight junctions of enteroendocytes, but it also cannot be ruled out that BC may have increased intestinal transport by endocytosis or some other mechanism, as it does in neonatal animals. If this were the case then some of the bioactive components in BC which promote macromolecular transport in the neonatal gut [12] might also facilitate the transport of larger molecules in the adult human gut.3. Experimental Section
3.1. Participants
3.2. Experimental Protocol
3.3. Body Mass and Height
3.4. Treadmill Running Test
3.5. Cardiorespiratory Assessment
3.6. Blood Collection and Analysis
3.7. Lactate Threshold
and the blood lactate concentrations during the treadmill run were used to determine the corresponding to the lactate threshold. Linear regression analysis of the HR vs response during exercise was then used to determine the HR corresponding to the at the lactate threshold. This HR was used as the training HR (HRt) for the running training program.3.8. Running Training Program
3.9. Intestinal Permeability
3.10. Nutrition
3.11. Statistical Procedures
4. Conclusions
Acknowledgements
References and Notes
- Coombes, J.; Conacher, M.; Austen, S.; Marshall, P. Dose effects of oral bovine colostrum supplementation on physical work capacity in cyclists. Med. Sci. Sport. Exercise 2002, 34, 1184–1188. [Google Scholar]
- Buckley, J.; Brinkworth, G.; Abbott, M. Effect of bovine colostrum on anaerobic exercise performance and plasma insulin-like growth factor I. J. Sport. Sci. 2003, 21, 577–588. [Google Scholar]
- Hofman, Z.; Smeets, R.; Verlaan, G.; v.d. Lugt, R.; Verstappen, P.A. The effect of bovine colostrum supplementation on exercise performance in elite field hockey players. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 461–479. [Google Scholar]
- Buckley, J.; Abbott, M.; Brinkworth, G.; Whyte, P. Bovine colostrum supplementation during endurance running training improves recovery, but not performance. J. Sci. Med. Sport 2002, 5, 65–79. [Google Scholar] [PubMed]
- Brinkworth, G.D.; Buckley, J.D.; Bourdon, P.C.; Gulbin, J.P.; David, A.Z. Oral bovine colostrum supplementation enhances buffer capacity but not rowing performance in elite female rowers. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 349–363. [Google Scholar]
- Brinkworth, G.; Buckley, J. Concentrated bovine colostrum protein supplementation reduces the incidence of self-reported symptoms of upper respiratory infection in adult males. Eur. J. Nutr. 2003, 42, 228–232. [Google Scholar]
- Øktedalen, O.; Lunde, O.C.; Opstad, P.K.; Aabakken, L.; Kvernebo, K. Changes in the gastrointestinal mucosa after long-distance running. Scand. J. Gastroenterol. 1992, 27, 270–273. [Google Scholar]
- Pals, K.L.; Chang, R.-T.; Ryan, A.J.; Gisolfi, C.V. Effect of running intensity on intestinal permeability. J. Appl. Physiol. 1997, 82, 571–576. [Google Scholar]
- van Nieuwenhoven, M.; Brouns, F.; Brummer, R.-J. Gastrointestinal profile of symptomatic athletes at rest and during physical exercise. Eur. J. Appl. Physiol. 2004, 91, 429–434. [Google Scholar]
- Playford, R.; MacDonald, C.; Calnan, D.; Floyd, D.; Podas, T.; Johnson, W.; Wicks, A.; Bashir, O.; Marchbank, T. Co-administration of the health food supplement, bovine colostrum, reduces the acute non-steroidal anti-inflammatory drug-induced increase in intestinal permeability. Clin. Sci. 2001, 100, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Playford, R.J.; MacDonald, C.E.; Calnan, D.P.; Floyd, D.N.; Podas, T.; Johnson, W.; Wicks, A.C.; Bashir, O.; Marchbank, T. Co-administration of the health food supplement, bovine colostrum, reduces the acute non-steroidal anti-inflammatory drug-induced increase in intestinal permeability. Clin. Sci. 2001, 100, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.R.; Elnif, J.; Burrin, D.G.; Sanglid, P.T. Development of intestinal immunoglobulin absorption and enzyme activities in neonatal pigs is diet dependent. J. Nutr. 2001, 131, 3259–3265. [Google Scholar]
- Westrom, B.; Ohlsson, B.; Svendsen, J.; Tagesson, C.; Karlsson, B. Intestinal transmission of macromolecules (BSA and FITC-labelled dextrans) in the neonatal pig: enhancing effect of colostrum, proteins, and protease inhibitors. Biol. Neonate 1985, 47, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason, I.; MacPherson, A.; Hollander, D. Intestinal permeability: An overview. Gastroenterology 1995, 108, 1566–1581. [Google Scholar]
- Mero, A.; Kähkönen, J.; Nykänen, T.; Parviainen, T.; Jokinen, I.; Takala, T.; Nikula, T.; Rasi, S.; Leppäluoto, J. IGF-1, IgA, and IgG responses to bovine colostrum supplementation during training. J. Appl. Physiol. 2002, 93, 732–739. [Google Scholar] [PubMed]
- Pakkanen, R.; Aalto, J. Growth factors and antimicrobial factors of bovine colostrum. Int. Dairy J. 1997, 7, 285–297. [Google Scholar]
- Brinkworth, G.; Buckley, J. Bovine colostrum supplementation does not affect nutrient absorptive capacity in healthy young men. Nutr. Res. 2003, 23, 1619–1629. [Google Scholar]
- Mero, A.; Miikkulainen, H.; Riski, J.; Pakkanen, R.; Aalto, J.; Takala, T. Effects of bovine colostrum supplementation on serum IGF-1, IgG, hormone, and saliva IgA during training. J. Appl. Physiol. 1997, 83, 1144–1151. [Google Scholar]
- Olds, T.; Norton, K. Pre-exercise Health Screening Guide; Human Kinetics: Champaign, IL, USA, 1999; p. 81. [Google Scholar]
- Norton, K.I.; Olds, T.S. Anthropometrica; New South Wales Press: Sydney, Austrilia, 1996. [Google Scholar]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. Improved detection of lactate threshold during exercise using a log-log transformation. J. Appl. Physiol. 1985, 59, 1936–1940. [Google Scholar]
- Miki, K.; Butler, R.; Moore, D.; Davidson, G. Rapid and simultaneous quantification of rhamnose, mannitol, and lactulose in urine by HPLC for estimating intestinal permeability in pediatric practice. Clin. Chem. 1996, 42, 71–75. [Google Scholar] [PubMed]
- Jackson, M. The 12345+ Food and Nutrition Plan; Anti Cancer Foundation of South Australia: Adelaide, Australia, 1991; p. 15. [Google Scholar]
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Buckley, J.D.; Butler, R.N.; Southcott, E.; Brinkworth, G.D. Bovine Colostrum Supplementation During Running Training Increases Intestinal Permeability. Nutrients 2009, 1, 224-234. https://doi.org/10.3390/nu1020224
Buckley JD, Butler RN, Southcott E, Brinkworth GD. Bovine Colostrum Supplementation During Running Training Increases Intestinal Permeability. Nutrients. 2009; 1(2):224-234. https://doi.org/10.3390/nu1020224
Chicago/Turabian StyleBuckley, Jonathan D., Ross N. Butler, Emma Southcott, and Grant D. Brinkworth. 2009. "Bovine Colostrum Supplementation During Running Training Increases Intestinal Permeability" Nutrients 1, no. 2: 224-234. https://doi.org/10.3390/nu1020224
APA StyleBuckley, J. D., Butler, R. N., Southcott, E., & Brinkworth, G. D. (2009). Bovine Colostrum Supplementation During Running Training Increases Intestinal Permeability. Nutrients, 1(2), 224-234. https://doi.org/10.3390/nu1020224