Evaluation of Pictorial Dietary Assessment Tool for Hospitalized Patients with Diabetes: Cost, Accuracy, and User Satisfaction Analysis

 ,
, 
Abstract
:1. Introduction
2. Method
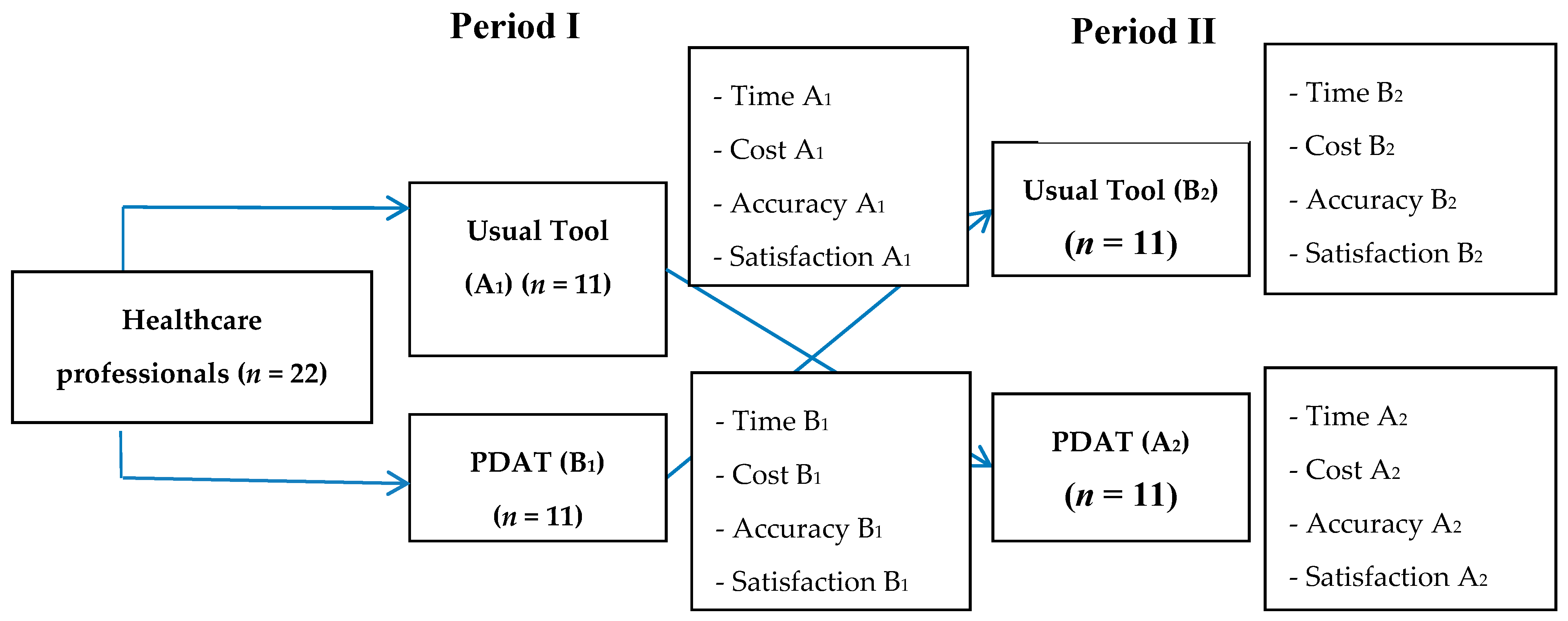
2.1. Study Design
2.2. Study Setting and Time Scale
2.3. Ethical Approval
2.4. Subjects
2.5. Assessors
2.6. Dietary Intake Measurement Methods
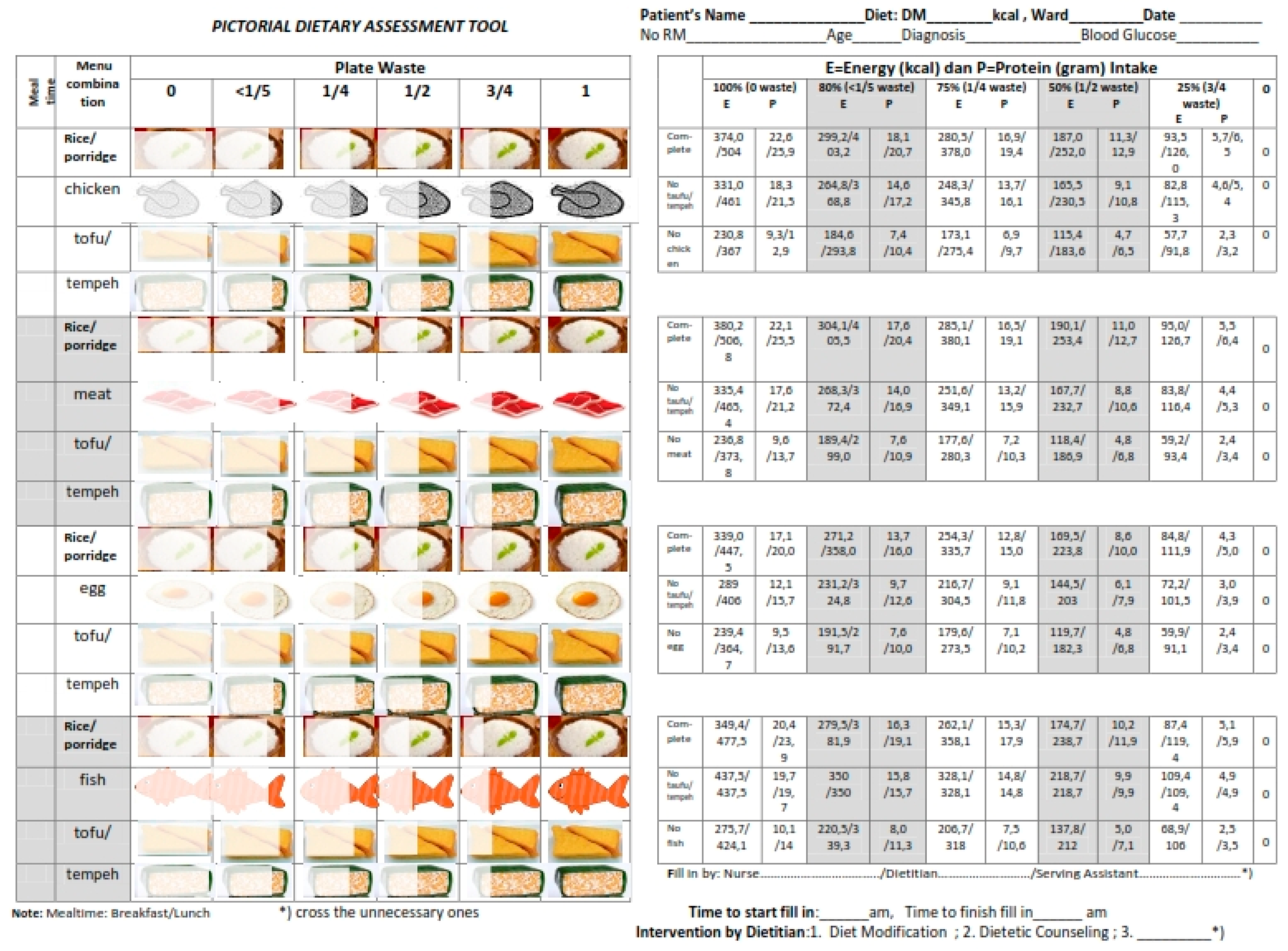
2.6.1. Pictorial Dietary Assessment Tool (PDAT)
2.6.2. Food Weighing Method
2.7. Cost Estimation Approach
2.8. User Satisfaction Assessment
2.9. Data Analysis
3. Results
3.1. Characteristics of Assessors and Patients
3.2. Cost Estimation
3.3. The Accuracy of Nutrient Intake Estimation
3.4. Satisfaction of Healthcare Staff
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Mueller, C.; Compher, C.; Ellen, D.M.; A.S.P.E.N.; Board of Directors. A.S.P.E.N. Clinical Guidelines: Nutrition screening, assessment, and intervention in adults. J. Parenter. Enter. Nutr. 2011, 35, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of Republic of Indonesia. Guidance of Nutrition Services of Hospitals; Government of Republic of Indonesia: Jakarta, Indonesia, 2013. Available online: http://gizi.depkes.go.id/download/Pedoman Gizi/COVER PGRS_PGRS Final.pdf (accessed on 12 July 2015). (In Indonesian)
- Mowe, M.; Bosaeus, I.; Rasmussen, H.H.; Kondrup, J.; Unosson, M.; Irtun, Ø. Nutritional routines and attitudes among doctors and nurses in Scandinavia: A questionnaire based survey. Clin. Nutr. 2006, 25, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Palmer, M.; Miller, K.; Noble, S. The accuracy of food intake charts completed by nursing staff as part of usual care when no additional training in completing intake tools is provided. Clin. Nutr. 2014, 34, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Bjornsdottir, R.; Oskarsdottir, E.S.; Thordardottir, F.R.; Ramel, A.; Thorsdottir, I.; Gunnarsdottir, I. Validation of a plate diagram sheet for estimation of energy and protein intake in hospitalized patients. Clin. Nutr. 2013, 32, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Schrader, E. Dietary assessment methods for older persons: what is the best approach? Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Comstock, E.M.; St Pierre, R.G.; Mackiernan, Y.D. Measuring individual plate waste in school lunches. Visual estimation and children’s ratings vs. actual weighing of plate waste. J. Am. Diet. Assoc. 1981, 79, 290–296. [Google Scholar] [PubMed]
- Castellanos, V.H.; Andrews, Y.N. Inherent flaws in a method of estimating meal intake commonly used in long-term-care facilities. J. Am. Diet. Assoc. 2002, 102, 826–830. [Google Scholar] [CrossRef]
- Berrut, G.; Favreau, A.M.; Dizo, E.; Tharreau, B.; Poupin, C.; Gueringuili, M.; Fressinaud, P.; Ritz, P. Estimation of calorie and protein intake in aged patients: Validation of a method based on meal portions consumed. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M52–M56. [Google Scholar] [CrossRef] [PubMed]
- Scognamiglio, U.; Salvia, A.; Paolucci, S.; Garbagnati, F.; Caltagirone, C.; Musicco, M. Validity of a questionnaire for the semi-quantitative evaluation of dietary intake of hospitalised patients compared to weighed records. J. Hum. Nutr. Diet. 2012, 25, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Thibault, R.; Goujon, N.; Le Gallic, E.; Clairand, R.; Sébille, V.; Vibert, J.; Schneider, M.; Darmaun, D. Use of 10-point analogue scales to estimate dietary intake: A prospective study in patients nutritionally at-risk. Clin. Nutr. 2009, 28, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Andrews, Y.N.; Castellanos, V.H. Development of a method for estimation of food and fluid intakes by nursing assistants in long-term care facilities: A pilot study. J. Am. Diet. Assoc. 2003, 103, 873–877. [Google Scholar] [CrossRef]
- Lorefalt, B.; Unosson, M. Estimation of energy intake in clinical practice: A comparison between a food record protocol and a precoded food record book. J. Clin. Nurs. 2002, 11, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Budiningsari, D.; Shahar, S.; Abdul Manaf, Z.; Susetyowati, S. Needs assessment for patients food intake monitoring among Indonesian healthcare professionals. Int. Nurs. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Susyani, S.; Prawirohartono, E.P.; Sudargo, T. Accuracy of staff to determine plate waste of hospitalised patients using Visual Comstock 6 point. Indones. J. Clin. Nutr. 2005, 2, 37–43. (In Indonesian) [Google Scholar]
- Simmons, S.F.; Reuben, D. Nutritional intake monitoring for Nursing home residents: A comparison of staff documentation, direct observation, and photography methods. J. Am. Geriatr. Soc. 2000, 48, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Budiningsari, D.; Shahar, S.; Manaf, Z.A.; Susetyowati, S. A simple dietary assessment tool to monitor food intake of hospitalized adult patients. J. Multidiscip. Healthc. 2016, 9, 311–322. [Google Scholar] [PubMed]
- Smith, P.E.; Smith, A.E. High-quality nutritional interventions reduce costs. J. Healthc. Financ. Manag. Assoc. 1997, 51, 66–69. [Google Scholar]
- Kruizenga, H.M.; Van Tulder, M.W.; Seidell, J.C.; Thijs, A.; Ader, H.J.; Van Bokhorst-de van der Schueren, M.A.E. Effectiveness and cost-effectiveness of early screening and treatment of malnourished patients. Am. J. Clin. Nutr. 2005, 82, 1082–1089. [Google Scholar] [PubMed]
- Franz, M.J.; Powers, M.A.; Leontos, C.; Holzmeister, L.A.; Kulkarni, K.; Monk, A.; Wedel, N.; Gradwell, E. The Evidence for Medical Nutrition Therapy for Type 1 and Type 2 Diabetes in Adults. J. Am. Diet. Assoc. 2010, 110, 1852–1889. [Google Scholar] [CrossRef] [PubMed]
- Sallé, A.; Ryan, M.; Ritz, P. Underreporting of Food Intake in Obese Diabetic and Nondiabetic Patients. Diabetes Care 2006, 29, 2726–2727. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, Y.; Yokoyama, T.; Homma, T.; Tanaka, H.; Kawahara, K. Relationship between the ability to recognize energy intake and expenditure, and blood sugar control in type 2 diabetes mellitus patients. Diabetes Res. Clin. Pract. 2005, 67, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Baker, J. Activity-Based Costing and Activity-Based Management for Health Care; Aspen Publishers: Gaithersburg, MD, USA, 1998. [Google Scholar]
- Susetyowati, S.; Hadi, H.; Asdie, A.H.; Hakimi, M. Implementation of standardized nutrition care process algorithm nutritional screening-based. Indones. J. Clin. Nutr. 2014, 11, 20–30. (In Indonesian) [Google Scholar]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Association of Indonesian Endocrinology. Consensus of Management and Prevention of Diabetes Melitus Type 2 in Indonesia; Perkeni: Jakarta, Indonesia, 2011; Available online: http://dokumen.tips/documents/revisi-final-konsensus-dm-tipe-2-indonesia-2011.html (accessed on 5 October 2016). (In Indonesian)
- Sullivan, S.C.; Bopp, M.M.; Roberson, P.K.; Lensing, S.; Sullivan, D.H. Evaluation of an Innovative Method for Calculating Energy Intake of Hospitalized Patients. Nutrients 2016, 8, 557. [Google Scholar] [CrossRef] [PubMed]
- Shahar, S.; Chee, K.Y.; Chak, W.; Wan, P. Food intakes and preferences of hospitalised geriatric patients. BMC Geriatr. 2002, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Kawasaki, Y.; Sakai, M.; Nishimura, K.; Fujiwara, K.; Fujisaki, K.; Shimpo, M.; Akamatsu, R. Criterion validity of the visual estimation method for determining patients’ meal intake in a community hospital. Clin. Nutr. 2016, 35, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Wang, P.; Laville, M.; Boissel, J.P. Low protein diets delay end-stage renal disease in non-diabetic adults with chronic renal failure. Nephrol. Dial. Transplant. 2000, 15, 1986–1992. [Google Scholar] [CrossRef] [PubMed]
- Boden, G.; Sargrad, K.; Homko, C.; Mozzoli, M.; Stein, T.P. Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. Ann. Intern. Med. 2005, 142, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, F.Q.; Gannon, M.C. The metabolic response to a high-protein, low-carbohydrate diet in men with type 2 diabetes mellitus. Metabolism 2006, 55, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Scott, D.; Hodge, A.M.; English, D.R.; Giles, G.G.; Ebeling, P.R.; Sander, K.M. Dietary protein intake and risk of type 2 diabetes: Results from the Melbourne Collaborative Cohort Study and a meta-analysis of prospective studies. Am. J. Clin. Nutr. 2016, 104, 1352–1365. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F.; Loria, C.M.; Reedy, J.L.; Baranowski, T. Need for Technological Innovation in Dietary Assessment. J. Am. Diet. Assoc. 2010, 110, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Duerksen, D.R.; Keller, H.H.; Vesnaver, E.; Laporte, M.; Jeejeebhoy, K.; Payette, H.; Gramlich, L.; Bernier, P.; Allard, J.P. Nurses’ perceptions regarding the prevalence, detection, and causes of malnutrition in Canadian hospitals: Results of a Canadian Malnutrition Task Force Survey. J. Parenter. Enter. Nutr. 2014, 40, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; McCutcheon, H. Mealtimes in hospital—Who does what ? J. Clin. Nurs. 2006, 15, 1221–1227. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Step | Analysis | Description | Elaboration |
|---|---|---|---|
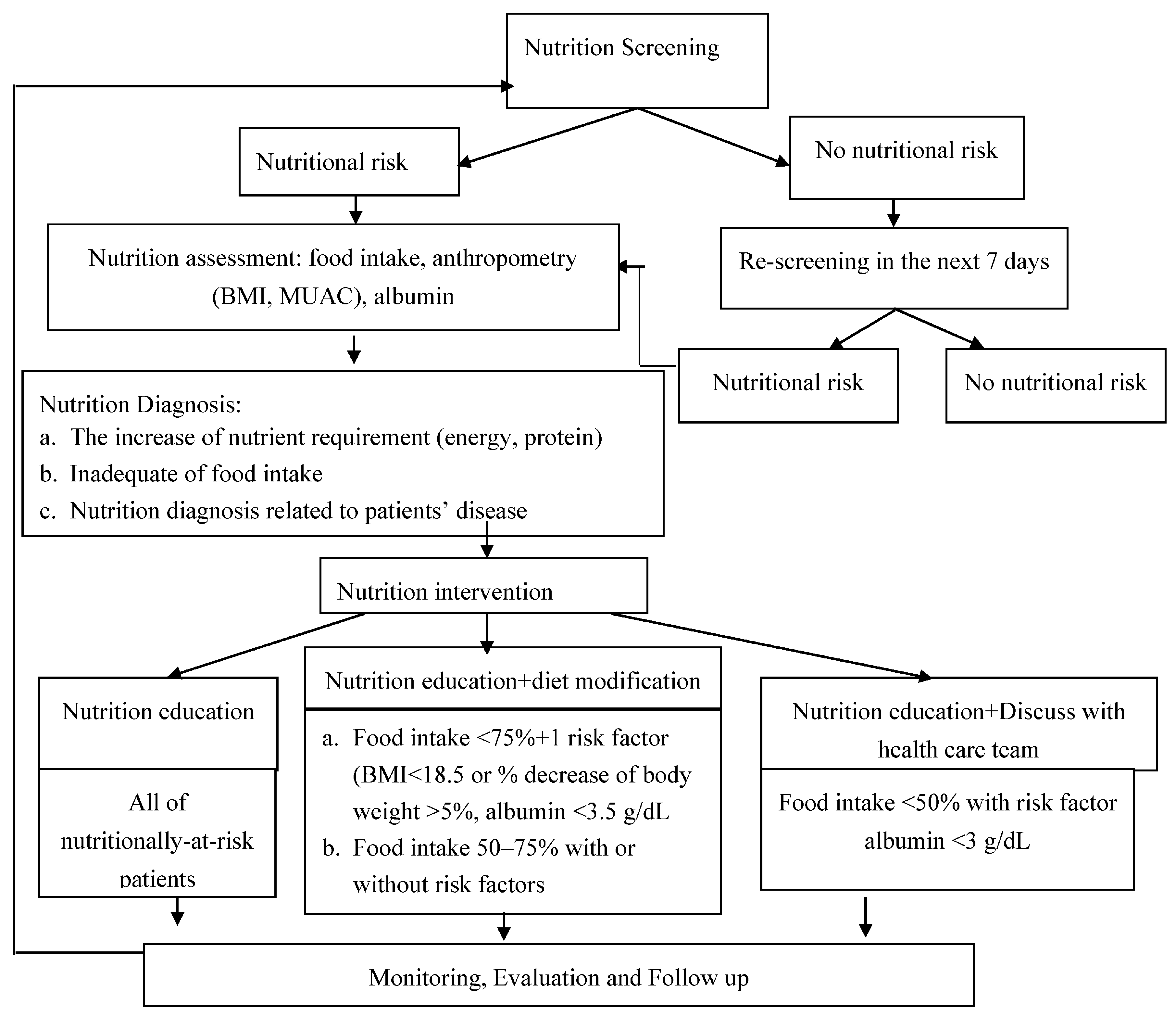
| 1 | Process Analysis | We described the overall process from the admission of hospitalized patients to the practices to monitor food intake of patients | Refer to Figure 3 |
| 2 | Activity Analysis | We presented an activity analysis for each relevant activity performed by the healthcare staff to complete the task for food intake recording. It was based on: the process analysis, direct observation, and time measurements. Cost driver was defined as activities consuming cost (labor hour, patient per minute). |
|
| 3 | Activity Costs | In order to determine the costs of activities previously identified, we assigned the cost of the resources to the activities using resource drivers. Resources were defined as people, equipment, supplies, etc. that allow activities necessary for the food intake recording of patients. | Cost of resources consist of nurses, dietitians, and serving assistant salaries (USD 267.2/month, USD 229/month, and USD 114.5/month, respectively) |
| 4 | Costs of Different Tools to Record Food Intake of Patients | We calculated the cost of the different methods of recording food intake (modified Comstock as the usual tool vs. PDAT). | Refer to The Results Section |
| Characteristics | Healthcare Staff (n = 22) |
|---|---|
| Age (years), mean ± SD | 40 ± 9.3 |
| Gender, n (%) | |
| Women | 17 (77.3) |
| Men | 5 (22.7) |
| Background of Healthcare Staff, n (%) | |
| Nurses | 6 (27.2) |
| Dietitians | 8 (36.4) |
| Serving Assistants | 8 (36.4) |
| Education level, n (%) | |
| Middle (high school) | 7 (31.8) |
| High (diploma, bachelor) | 15 (68.2) |
| Years of working, mean ± SD | 19 ± 11.6 |
| PDAT | Modified Comstock | Total | p (Chi Square) | |
|---|---|---|---|---|
| (n = 66) | (n = 66) | (n = 132) | ||
| Age (years), mean ± SD | 56.4 ± 10.5 | 56.1 ± 10.5 | ||
| Gender, n (%) | ||||
| Women | 31 (48.4) | 33 (51.6) | 64 (48.5) | 0.728 |
| Men | 35 (51.5) | 33 (48.5) | 68 (51.5) | |
| Type of Diet | ||||
| Normal textured diet | 37 (53.6) | 32 (46.4) | 69 (52.3) | 0.384 |
| Soft textured diet | 29 (46) | 34 (54) | 63 (47.7) | |
| Diabetic Diet (kcal/day) | ||||
| 1500 | 17 (56.7) | 13 (43.3) | 30 (22.7) | 0.836 |
| 1700 | 35 (49.3) | 36 (50.7) | 71 (53.8) | |
| 1900 | 11 (45.8) | 13 (54.2) | 24 (18.2) | |
| 2100 | 3 (42.9) | 4 (57.1) | 7 (5.3) | |
| Adequacy of energy intake (breakfast) | ||||
| <RDA a | 42 (51.2) | 40 (48.8) | 82 (62.1) | 0.720 |
| ≥RDA a | 24 (48) | 26 (52) | 50 (37.9) | |
| Adequacy of energy intake (lunch) | ||||
| <RDA a | 44 (49.4) | 45 (50.6) | 89 (67.4) | 0.853 |
| ≥RDA a | 22 (51.2) | 21 (48.8) | 43 (32.6) | |
| Nutrition screening, n (%) | ||||
| Not at risk | 44 (50.6) | 43 (49.4) | 87 (65.9) | 0.854 |
| At risk | 22 (48.9) | 23 (51.1) | 45 (34.1) | |
| Accompanying diagnosis with diabetes | ||||
| Renal disorders | 9 (47.4) | 10 (52.6) | 19 (14.4) | 0.259 |
| Hepatic disorders | 3 (100) | 0 (0) | 3 (2.3) | |
| Malignancy | 24 (61.5) | 15 (38.5) | 39 (29.5) | |
| Fracture/surgery | 4 (44.4) | 5 (55.8) | 9 (6.8) | |
| Ulcer | 10 (52.6) | 9 (47.4) | 19 (14.4) | |
| Coronary heart disease/ischemia | 9 (45) | 11 (55) | 20 (15.2) | |
| Pulmonary disorders | 2 (66.7) | 1 (33.3) | 3 (2.3) | |
| Cataract | 4 (28.6) | 10 (71.4) | 14 (10.6) | |
| Hypoglycemia | 1 (50) | 1 (50) | 2 (1.5) | |
| Hyperglycemia | 0 (0) | 1 (100) | 1 (0.8) | |
| Digestive disorders | 0 (0) | 3 (100) | 3 (2.3) |
| No. | Resources | Cost Drivers | PDAT | Modified Comstock | p Value |
|---|---|---|---|---|---|
| Staff | |||||
| 1 | Number of staff involved | 6 nurses | 18 patients | 18 patients | |
| 8 dietitians | 24 patients | 24 patients | |||
| 8 serving assistants | 24 patients | 24 patients | |||
| total | 66 patients | 66 patients | |||
| 2 | Staff (grade) × salary (USD) | Labor hours (in minutes) mean ± SD | 0.02 ± 0.01 | 0.02 ± 0.01 | 0.960 |
| Nurses | 0.03/min | 0.03/min | |||
| Dietitians | 0.02/min | 0.02/min | |||
| Serving assistants | 0.01/min | 0.01/min | |||
| 3 | Time spent by the staff to complete the tool (minutes) | Minute per patient (Mean ± SD) | 2.3 ± 0.7 | 3.5 ± 1.3 | 0.000 * |
| 4 | Staff cost for time spent | (Mean ± SD) | 0.05 ± 0.02 | 0.08 ± 0.04 | 0.000 * |
| Time saved (minute) | 1.2 | ||||
| Cost saved for the time saved | 0.08 − 0.05 = 0.03 | ||||
| Time saving gain (total cost/time spent) | USD/minutes | 0.03/1.2 = 0.025 | |||
| Equipment | |||||
| 1 | One set of forms | Set per patient | 0.07 | 0.03 | |
| 2 | Stationary | Set per patient | 0.15 | 0.15 | |
| Total cost | USD | 0.22 | 0.18 | 0.000 * | |
| Total overall cost | (Mean ± SD) | 0.27 ± 0.02 | 0.26 ± 0.04 | 0.013 * |
| Accuracy | ||
|---|---|---|
| Breakfast | P10 a | P15 b |
| Energy | ||
| PDAT | 98.5 | 98.5 |
| Modified Comstock | 89.4 | 92.4 |
| Protein | ||
| PDAT | 98.5 | 86.4 * |
| Modified Comstock | 28.8 * | 63.6 * |
| Lunch | ||
| Energy | ||
| PDAT | 84.8 | 98.5 |
| Modified Comstock | 77.3 | 93.9 * |
| Protein | ||
| PDAT | 71.2 * | 87.9 |
| Modified Comstock | 39.4 * | 71.2 * |
| No. | Satisfaction Aspects | Minimum–Maximum | Median | Mean ± SD | p Value | |||
|---|---|---|---|---|---|---|---|---|
| PDAT | Modified Comstock | PDAT | Modified Comstock | PDAT | Modified Comstock | |||
| 1 | It is practical enough | 4–5 | 3–5 | 4 | 4 | 4.4 ± 0.49 | 4.4 ± 0.58 | 0.477 |
| 2 | It can be used for all kind of diet (per oral) of patients | 2–5 | 4–5 | 4 | 4 | 4.3 ± 0.69 | 4.4 ± 0.50 | 0.403 |
| 3 | Time needed to complete this tool is short enough | 4–5 | 3–5 | 4 | 4 | 4.1 ± 0.35 | 4.4 ± 0.57 | 0.004 * |
| 4 | It is easy to use (user-friendly) even with minimal training | 3–5 | 3–5 | 4 | 5 | 4.2 ± 0.50 | 4.5 ± 0.66 | 0.003 * |
| 5 | It helps for recording food intake of patients | 4–5 | 3–5 | 5 | 4 | 4.6 ± 0.50 | 4.2 ± 0.72 | 0.004 * |
| 6 | It helps to provide more information on plate waste according to type of food | 4–5 | 2–4 | 5 | 2.5 | 4.7 ± 0.45 | 2.9 ± 0.96 | <0.001 * |
| 7 | It helps to obtain the more accurate food intake data | 4–5 | 2–4 | 5 | 3 | 4.7 ± 0.45 | 2.9 ± 0.88 | <0.001 * |
| 8 | It facilitates the calculation of energy and protein intake | 4–5 | 2–4 | 4 | 2 | 4.4 ± 0.49 | 2.7 ± 0.87 | <0.001 * |
| 9 | It gives more information in decision making for further nutrition management to improve management of diabetic care | 4–5 | 2–5 | 4 | 2 | 4.2 ± 0.39 | 3.0 ± 0.96 | <0.001 * |
| 10 | Overall, I would recommend to use PDAT (or Comstock) in other hospitals. | 4–5 | 2–4 | 4 | 3 | 4.2 ± 0.39 | 3.0 ± 0.80 | <0.001 * |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budiningsari, D.; Shahar, S.; Abdul Manaf, Z.; Mohd Nordin, N.A.; Susetyowati, S. Evaluation of Pictorial Dietary Assessment Tool for Hospitalized Patients with Diabetes: Cost, Accuracy, and User Satisfaction Analysis. Nutrients 2018, 10, 27. https://doi.org/10.3390/nu10010027
Budiningsari D, Shahar S, Abdul Manaf Z, Mohd Nordin NA, Susetyowati S. Evaluation of Pictorial Dietary Assessment Tool for Hospitalized Patients with Diabetes: Cost, Accuracy, and User Satisfaction Analysis. Nutrients. 2018; 10(1):27. https://doi.org/10.3390/nu10010027
Chicago/Turabian StyleBudiningsari, Dwi, Suzana Shahar, Zahara Abdul Manaf, Nor Azlin Mohd Nordin, and Susetyowati Susetyowati. 2018. "Evaluation of Pictorial Dietary Assessment Tool for Hospitalized Patients with Diabetes: Cost, Accuracy, and User Satisfaction Analysis" Nutrients 10, no. 1: 27. https://doi.org/10.3390/nu10010027
APA StyleBudiningsari, D., Shahar, S., Abdul Manaf, Z., Mohd Nordin, N. A., & Susetyowati, S. (2018). Evaluation of Pictorial Dietary Assessment Tool for Hospitalized Patients with Diabetes: Cost, Accuracy, and User Satisfaction Analysis. Nutrients, 10(1), 27. https://doi.org/10.3390/nu10010027