The Relationship between Body Composition and a Gluten Free Diet in Children with Celiac Disease

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
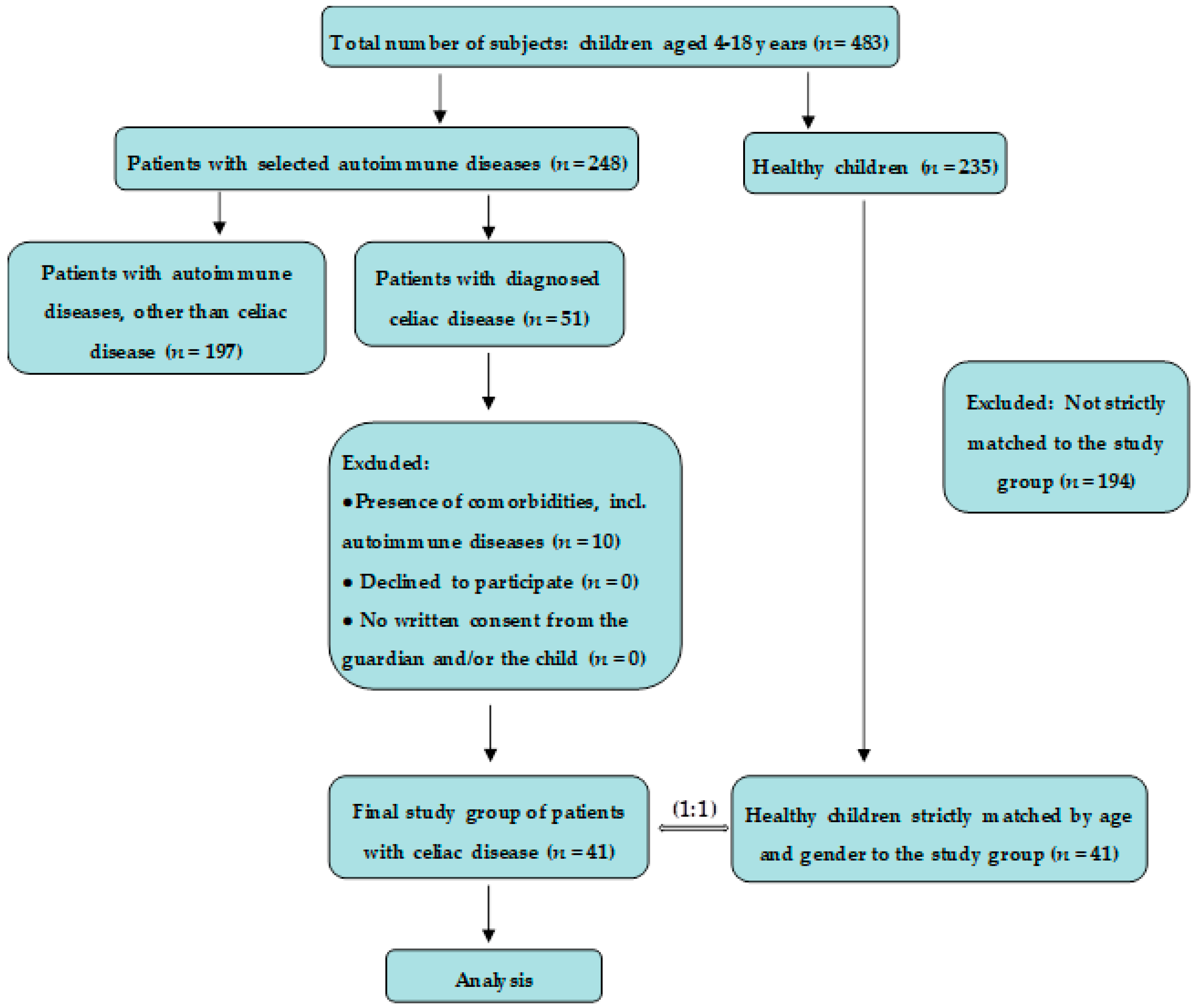
2.2. Subjects
2.3. Assessments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European society for pediatric gastroenterology, hepatology, and nutrition guidelines for the diagnosis of coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef] [PubMed]
- Ivarsson, A.; Myléus, A.; Norström, F.; van der Pals, M.; Rosén, A.; Högberg, L.; Danielsson, L.; Halvarsson, B.; Hammarroth, S.; Hernell, O.; et al. Prev–alence of childhood celiac disease and changes in infant feeding. Pediatrics 2013, 131, e687–e694. [Google Scholar] [CrossRef] [PubMed]
- Almazán, M.V.; Ortega, E.; Moreno Torres, R.; Tovar, M.; Romero, J.; López-Casado, M.Á.; Jáimez, L.; Jiménez-Jáimez, J.; Ballesteros, A.; Caballero-Villarraso, J.; et al. Diagnostic screening for subclinical celiac disease using a rapid test in children aged 2–4. Pediatr. Res. 2015, 78, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Bascuñán, K.A.; Roncoroni, L.; Branchi, F.; Doneda, L.; Scricciolo, A.; Ferretti, F.; Araya, M.; Elli, L. The 5 Ws of a gluten challenge for gluten-related disorders. Nutr. Rev. 2018, 76, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Mustalahti, K.; Catassi, C.; Reunanen, A.; Fabiani, E.; Heier, M.; McMillan, S.; Murray, L.; Metzger, M.H.; Gasparin, M.; Bravi, E.; et al. The prevalence of celiac disease in Europe: Results of a centralized, international mass screening project. Ann. Med. 2010, 42, 587–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obtułowicz, K.; Waga, J.; Dyga, W. Gluten-mechanisms of intolerance, symptoms and treatment possibilities of IgE-related allergy for gluten in the light of actual clinical and immunological studies. Przegl. Lek. 2015, 72, 747–753. [Google Scholar] [PubMed]
- Fasano, A.; Catassi, C. Clinical practice. Celiac disease. N. Engl. J. Med. 2012, 367, 2419–2426. [Google Scholar] [CrossRef] [PubMed]
- Parzanese, I.; Qehajaj, D.; Patrinicola, F.; Aralica, M.; Chiriva-Internati, M.; Stifter, S.; Elli, L.; Grizzi, F. Celiac disease: From pathophysiology to treatment. World J. Gastrointest. Pathophysiol. 2017, 8, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Pulido, O.; Zarkadas, M.; Dubois, S.; Macisaac, K.; Cantin, I.; La Vieille, S.; Godefroy, S.; Rashid, M. Clinical features and symptom recovery on a gluten-free diet in Canadian adults with celiac disease. Can. J. Gastroenterol. 2013, 27, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Alzaben, A.S.; Turner, J.; Shirton, L.; Samuel, T.M.; Persad, R.; Mager, D. Assessing nutritional quality and adherence to the gluten-free diet in children and adolescents with celiac disease. Can. J. Diet. Pract. Res. 2015, 76, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Laurikka, P.; Salmi, T.; Collin, P.; Huhtala, H.; Mäki, M.; Kaukinen, K.; Kurppa, K. Gastrointestinal symptoms in celiac disease patients on a long-term gluten-free diet. Nutrients 2016, 8, E429. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, S.J.; Gibson, P.R. Nutritional inadequacies of the gluten-free diet in both recently-diagnosed and long-term patients with coeliac disease. J. Hum. Nutr. Diet. 2013, 26, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, P.; Picca, M.; Dilillo, D.; Meneghin, F.; Cravidi, C.; Tischer, M.C.; Vivaldo, T.; Bedogni, G.; Zuccotti, G.V. Changes of body mass index in celiac children on a gluten-free diet. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Anania, C.; Pacifico, L.; Olivero, F.; Perla, F.M.; Chiesa, C. Cardiometabolic risk factors in children with celiac disease on a gluten-free diet. World J. Clin. Pediatr. 2017, 6, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Tsiountsioura, M.; Wong, J.E.; Upton, J.; McIntyre, K.; Dimakou, D.; Buchanan, E.; Cardigan, T.; Flynn, D.; Bishop, J.; Russell, R.K.; et al. Detailed assessment of nutritional status and eating patterns in children with gastrointestinal diseases attending an outpatients clinic and contemporary healthy controls. Eur. J. Clin. Nutr. 2014, 68, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Newnham, E.D.; Shepherd, S.J.; Strauss, B.J.; Hosking, P.; Gibson, P.R. Adherence to the gluten-free diet can achieve the therapeutic goals in almost all patients with coeliac disease: A 5-year longitudinal study from diagnosis. J. Gastroenterol. Hepatol. 2016, 31, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.C.; Pitzalis, G.; Ferri, M.; Nenna, R.; Thanasi, E.; Andreoli, A.; De Lorenzo, A.; Bonamico, M. Body composition in coeliac disease adolescents on a gluten-free diet: A longitudinal study. Acta Diabetol. 2003, 40, S171–S173. [Google Scholar] [CrossRef] [PubMed]
- Barera, G.; Mora, S.; Brambilla, P.; Ricotti, A.; Menni, L.; Beccio, S.; Bianchi, C. Body composition in children with celiac disease and the effects of a gluten-free diet: A prospective case-control study. Am. J. Clin. Nutr. 2000, 72, 71–75. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Di Campli, C.; Andreoli, A.; Sasso, G.F.; Bonamico, M.; Gasbarrini, A. Assessment of body composition by bioelectrical impedance in adolescent patients with celiac disease. Am. J. Gastroenterol. 1999, 94, 2951–2955. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y.; Morgan, S.L. Celiac disease and metabolic bone disease. J. Clin. Densitom. 2013, 16, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Więch, P.; Dąbrowski, M.; Bazaliński, D.; Sałacińska, I.; Korczowski, B.; Binkowska-Bury, M. Bioelectrical impedance phase angle as an indicator of malnutrition in hospitalized children with diagnosed inflammatory bowel diseases—A case control study. Nutrients 2018, 10, 499. [Google Scholar] [CrossRef] [PubMed]
- Bardella, M.T.; Molteni, N.; Prampolini, L.; Giunta, A.M.; Baldassarri, A.R.; Morganti, D.; Bianchi, P.A. Need for follow up in coeliac disease. Arch. Dis. Child. 1994, 70, 211–213. [Google Scholar] [CrossRef] [PubMed]
- Troncone, R.; Mayer, M.; Spagnuolo, F.; Maiuri, L.; Greco, L. Endomysial antibodies as unreliable markers for slight dietary transgressions in adolescents with celiac disease. J. Pediatr. Gastroenterol. Nutr. 1995, 21, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Yanovski, S.Z.; Hubbard, V.S.; Heymsfield, S.B.; Lukaski, H.C. Bioelectrical impedance analysis in body composition measurement: National institutes of health technology assessment conference statement. Am. J. Clin. Nutr. 1996, 64, 524S–532S. [Google Scholar]
- Kyle, U.G.; Bosaeus, I.; de Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gómez, J.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- Kushner, R.F. Bioelectrical impedance analysis: A review of principles and applications. J. Am. Coll. Nutr. 1992, 11, 199–209. [Google Scholar] [PubMed]
- Barone, M.; Della, V.N.; Rosania, R.; Facciorusso, A.; Trotta, A.; Cantatore, F.P.; Falco, S.; Pignatiello, S.; Viggiani, M.T.; Amoruso, A.; et al. A comparison of the nutritional status between adult celiac patients on a long-term, strictly gluten-free diet and healthy subjects. Eur. J. Clin. Nutr. 2016, 70, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Capristo, E.; Addolorato, G.; Mingrone, G.; De Gaetano, A.; Greco, A.V.; Tataranni, P.A.; Gasbarrini, G. Changes in body composition, substrate oxidation, and resting metabolic rate in adult celiac disease patients after a 1-y gluten-free diet treatment. Am. J. Clin. Nutr. 2000, 72, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Blazina, S.; Bratanic, N.; Campa, A.S.; Blagus, R.; Orel, R. Bone mineral density and importance of strict gluten-free diet in children and adolescents with celiac disease. Bone 2010, 47, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Delibasic, M.; Peta, V.; Turkulov, V.; De Lorenzo, A.; Medić-Stojanoska, M. Nutritional profile of adult patients with celiac disease. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4285–4292. [Google Scholar] [PubMed]
- Forchielli, M.L.; Fernicola, P.; Diani, L.; Scrivo, B.; Salfi, N.C.; Pessina, A.C.; Lima, M.; Conti, V.; Pession, A. Gluten-free diet and lipid profile in children with celiac disease: Comparison with general population standards. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Sue, A.; Dehlsen, K.; Ooi, C.Y. Paediatric patients with coeliac disease on a gluten-free diet: Nutritional adequacy and macro- and micronutrient imbalances. Curr. Gastroenterol. Rep. 2018, 22, 2. [Google Scholar] [CrossRef] [PubMed]
- Bessahraoui, M.; Bouziane, N.K.; Boudraa, G.; Touhami, M. Growth and puberty in the coeliac disease of the child. Pediatr. Res. 2011, 70, 365. [Google Scholar] [CrossRef]
- Rodrigues, M.; Yonamine, G.H.; Fernandes Satiro, C.A. Rate and determinants of non-adherence to a gluten-free diet and nutritional status assessment in children and adolescents with celiac disease in a tertiary Brazilian referral center: A cross-sectional and retrospective study. BMC Gastroenterol. 2018, 18, 15. [Google Scholar] [CrossRef]
- Dickey, W.; Kearney, N. Overweight in celiac disease: Prevalence, clinical characteristics, and effect of a gluten-free diet. Am. J. Gastroenterol. 2006, 101, 2356–2359. [Google Scholar] [CrossRef] [PubMed]
- Nenna, R.; Mosca, A.; Mennini, M.; Papa, R.E.; Petrarca, L.; Mercurio, R.; Montuori, M.; Piedimonte, A.; Bavastrelli, M.; De Lucia, I.C.; et al. Coeliac disease screening among a large cohort of overweight/obese children. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Reilly, N.R.; Aguilar, K.; Hassid, B.G.; Cheng, J.; Defelice, A.R.; Kazlow, P.; Bhagat, G.; Green, P.H. Celiac disease in normal-weight and overweight children: Clinical features and growth outcomes following a gluten-free diet. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 528–531. [Google Scholar] [CrossRef] [PubMed]
- Siddh, L.; Sengar, G.S.; Nagraj, N.; Shyam, R.; Garg, P. Body mass index in celiac disease and effect of a gluten-free diet on body mass index. Int. J. Adv. Med. 2016, 3, 813–815. [Google Scholar] [CrossRef]
- Radlović, N.; Mladenović, M.; Leković, Z.; Zivanović, D.; Brdar, R.; Radlović, V.; Ristić, D.; Pavlović, M.; Stojsić, Z.; Vuletić, B.; et al. Effect of gluten-free diet on the growth and nutritional status of children with coeliac disease. Srp. Arh. Celok. Lek. 2009, 137, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Glissen Brown, J.R.; Singh, P. Coeliac disease. Paediatr. Int. Child. Health. 2018, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, J.C.; Kumar, P.; Dutta, A.K.; Basu, S.; Kumar, A. Assessmentof dietary compliance to gluten free diet and psychosocialproblems in Indian children with celiac disease. Indian J. Pediatr. 2010, 77, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Roma, E.; Roubani, A.; Kolia, E.; Panayiotou, J.; Zellos, A.; Syriopoulou, V.P. Dietarycompliance and life style of children with coeliac disease. J. Hum. Nutr. Diet. 2010, 23, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.J.; Walker-Smith, J.; Milla, P.; Harris, G.; Colyer, J.; Halliday, R. Theteenage coeliac: Follow up study of 102 patients. Arch. Dis. Child. 1988, 63, 916–920. [Google Scholar] [CrossRef] [PubMed]
- White, L.E.; Bannerman, E.; Gillett, P.M. Coeliac disease and the gluten-free diet: A review of the burdens; factors associated with adherence and impact on health-related quality of life, with specific focus on adolescence. J. Hum. Nutr. Diet. 2016, 29, 593–606. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Celiac Disease (N = 41) | Control (N = 41) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age, years | 10.81 | 3.96 | 10.63 | 4.01 | 0.989 |
| Gender, n | 1.000 | ||||
| Male | 21 | n/a | 21 | n/a | |
| Female | 20 | n/a | 20 | n/a | |
| Weight, kg | 33.59 | 13.79 | 39.70 | 15.25 | 0.046 * |
| Height, cm | 137.62 | 21.68 | 144.20 | 19.63 | 0.167 |
| BMI, kg/m2 | 16.94 | 2.65 | 18.29 | 3.49 | 0.089 |
| Parameter | Celiac Disease (N = 41) | Control (N = 41) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| FM, kg | 6.66 | 4.19 | 9.47 | 5.15 | 0.007 * |
| FFM, kg | 26.15 | 10.72 | 30.24 | 11.57 | 0.098 |
| MM, kg | 17.17 | 7.45 | 19.55 | 8.10 | 0.168 |
| TBW, L | 22.71 | 10.96 | 23.73 | 8.72 | 0.312 |
| ECW, L | 9.33 | 3.47 | 10.28 | 3.73 | 0.246 |
| ICW, L | 12.35 | 4.86 | 13.55 | 5.16 | 0.170 |
| BCM, kg | 13.89 | 6.11 | 15.85 | 6.64 | 0.164 |
| FM% | 19.32 | 7.36 | 23.34 | 7.36 | 0.015 * |
| FFM% | 80.68 | 7.36 | 76.66 | 7.36 | 0.015 * |
| MM% | 50.72 | 5.98 | 48.94 | 5.62 | 0.168 |
| TBW% | 65.22 | 8.94 | 60.47 | 7.66 | 0.012 * |
| ECW% | 43.86 | 5.18 | 43.82 | 3.59 | 0.981 |
| ICW% | 56.14 | 5.18 | 56.18 | 3.59 | 0.981 |
| BCM% | 50.66 | 3.96 | 51.62 | 3.73 | 0.373 |
| BCMI | 6.91 | 1.28 | 7.22 | 1.50 | 0.322 |
| PA | 5.45 | 0.67 | 5.63 | 0.69 | 0.241 |
| Parameter | Compliant to GFD (N = 26) | Non-Compliant to GFD (N = 15) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age, years | 11.00 | 4.10 | 10.47 | 3.82 | 0.683 |
| Gender, n | 0.239 | ||||
| Male | 11 | n/a | 10 | n/a | |
| Female | 15 | n/a | 5 | n/a | |
| Disease duration, months | 74.23 | 58.10 | 26.07 | 40.93 | 0.002 * |
| Marsh scale | 0.584 | ||||
| IIIA | 4 | n/a | 3 | n/a | |
| IIIB | 9 | n/a | 7 | n/a | |
| IIIC | 13 | n/a | 5 | n/a | |
| Weight, kg | 35.67 | 14.07 | 29.99 | 12.96 | 0.208 |
| Height, cm | 141.02 | 21.73 | 131.73 | 21.00 | 0.190 |
| BMI | 17.22 | 2.55 | 16.45 | 2.84 | 0.272 |
| FM | 7.48 | 4.24 | 5.24 | 3.82 | 0.064 |
| FFM | 28.19 | 11.01 | 22.62 | 9.53 | 0.110 |
| MM | 17.95 | 7.63 | 15.83 | 7.17 | 0.388 |
| TBW | 22.49 | 8.00 | 23.08 | 15.12 | 0.675 |
| ECW | 9.65 | 3.56 | 8.76 | 3.35 | 0.434 |
| ICW | 12.91 | 4.67 | 11.37 | 5.18 | 0.457 |
| BCM | 14.52 | 6.26 | 12.79 | 5.89 | 0.390 |
| FM% | 20.81 | 6.60 | 16.73 | 8.10 | 0.087 |
| FFM% | 79.19 | 6.60 | 83.27 | 8.10 | 0.087 |
| MM% | 49.88 | 5.60 | 52.17 | 6.52 | 0.241 |
| TBW% | 63.89 | 8.69 | 67.52 | 9.19 | 0.214 |
| ECW% | 43.27 | 4.15 | 44.88 | 6.64 | 0.345 |
| ICW% | 56.73 | 4.15 | 55.12 | 6.64 | 0.345 |
| BCM% | 50.80 | 3.18 | 50.41 | 5.17 | 0.745 |
| BCMI | 6.91 | 1.16 | 6.90 | 1.50 | 0.978 |
| PA | 5.47 | 0.58 | 5.43 | 0.83 | 0.862 |
| Parameter | Baseline (N = 22) | Follow-Up (N = 22) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age, years | 10.05 | 4.08 | 11.41 | 4.08 | <0.001 * |
| Disease duration, months | 63.68 | 67.61 | 80.86 | 68.14 | <0.001 * |
| Weight, kg | 32.40 | 15.68 | 36.01 | 14.08 | <0.001 * |
| Height, cm | 134.50 | 24.62 | 142.14 | 23.14 | <0.001 * |
| BMI, kg/m2 | 16.81 | 2.76 | 17.07 | 2.09 | 0.046 * |
| FM, kg | 7.20 | 4.62 | 7.42 | 3.75 | 0.101 |
| FFM, kg | 25.20 | 12.17 | 28.59 | 11.91 | 0.001 * |
| MM, kg | 16.05 | 8.45 | 18.33 | 8.24 | <0.001 * |
| TBW, L | 20.16 | 9.25 | 22.81 | 9.02 | <0.001 * |
| ECW, L | 8.63 | 3.89 | 9.83 | 3.95 | 0.003 * |
| ICW, L | 11.63 | 5.61 | 12.98 | 5.28 | <0.001 * |
| BCM, kg | 12.99 | 6.93 | 14.85 | 6.74 | <0.001 * |
| FM% | 22.05 | 6.50 | 21.17 | 6.94 | 0.972 |
| FFM% | 77.95 | 6.50 | 78.83 | 6.94 | 0.972 |
| MM% | 48.78 | 5.76 | 49.96 | 5.76 | 0.167 |
| TBW% | 62.66 | 8.50 | 63.39 | 9.00 | 0.455 |
| ECW% | 43.79 | 5.03 | 43.56 | 4.40 | 0.788 |
| ICW% | 56.21 | 5.03 | 56.44 | 4.40 | 0.788 |
| BCM% | 50.40 | 3.58 | 51.13 | 3.19 | 0.102 |
| BCMI | 6.60 | 1.26 | 6.88 | 1.12 | 0.005 * |
| PA | 5.40 | 0.64 | 5.54 | 0.61 | 0.121 |
| Parameter | Compliant to GFD (N = 17) | Non-Compliant to GFD (N = 5) | p Value | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Weight increase, kg | 4.16 | 6.65 | 1.74 | 0.40 | 0.034 * |
| Height increase, cm | 8.12 | 5.47 | 6.00 | 3.37 | 0.426 |
| BMI increase, kg/m2 | 0.47 | 2.13 | -0.44 | 0.78 | 0.021 * |
| FM increase, kg | 0.47 | 3.66 | -0.64 | 2.06 | 0.078 |
| FFM increase, kg | 3.69 | 4.90 | 2.38 | 2.39 | 0.308 |
| MM increase, kg | 2.51 | 3.26 | 1.48 | 1.86 | 0.182 |
| TBW increase, L | 2.45 | 3.21 | 3.34 | 3.47 | 0.597 |
| ECW increase, L | 1.37 | 2.04 | 0.64 | 0.60 | 0.209 |
| ICW increase, L | 0.96 | 1.45 | 2.70 | 2.92 | 0.610 |
| BCM increase, kg | 2.05 | 2.64 | 1.22 | 1.57 | 0.240 |
| BCMI increase | 0.31 | 0.72 | 0.20 | 0.53 | 0.289 |
| PA increase | 0.14 | 0.41 | 0.12 | 0.40 | 0.919 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Więch, P.; Chmiel, Z.; Bazaliński, D.; Sałacińska, I.; Bartosiewicz, A.; Mazur, A.; Korczowski, B.; Binkowska-Bury, M.; Dąbrowski, M. The Relationship between Body Composition and a Gluten Free Diet in Children with Celiac Disease. Nutrients 2018, 10, 1817. https://doi.org/10.3390/nu10111817
Więch P, Chmiel Z, Bazaliński D, Sałacińska I, Bartosiewicz A, Mazur A, Korczowski B, Binkowska-Bury M, Dąbrowski M. The Relationship between Body Composition and a Gluten Free Diet in Children with Celiac Disease. Nutrients. 2018; 10(11):1817. https://doi.org/10.3390/nu10111817
Chicago/Turabian StyleWięch, Paweł, Zdzisława Chmiel, Dariusz Bazaliński, Izabela Sałacińska, Anna Bartosiewicz, Artur Mazur, Bartosz Korczowski, Monika Binkowska-Bury, and Mariusz Dąbrowski. 2018. "The Relationship between Body Composition and a Gluten Free Diet in Children with Celiac Disease" Nutrients 10, no. 11: 1817. https://doi.org/10.3390/nu10111817
APA StyleWięch, P., Chmiel, Z., Bazaliński, D., Sałacińska, I., Bartosiewicz, A., Mazur, A., Korczowski, B., Binkowska-Bury, M., & Dąbrowski, M. (2018). The Relationship between Body Composition and a Gluten Free Diet in Children with Celiac Disease. Nutrients, 10(11), 1817. https://doi.org/10.3390/nu10111817