Effects of Protein Supplementation Combined with Exercise Intervention on Frailty Indices, Body Composition, and Physical Function in Frail Older Adults

 , ,
, , 
Abstract
:1. Introduction
2. Method
2.1. Design
2.2. Search Strategy
2.3. Study Selection Criteria
2.4. Data Extraction
2.5. Outcome Measures
2.6. Assessment of Bias Risks and Methodological Quality of Included Studies
2.7. Data Synthesis and Analysis
3. Results
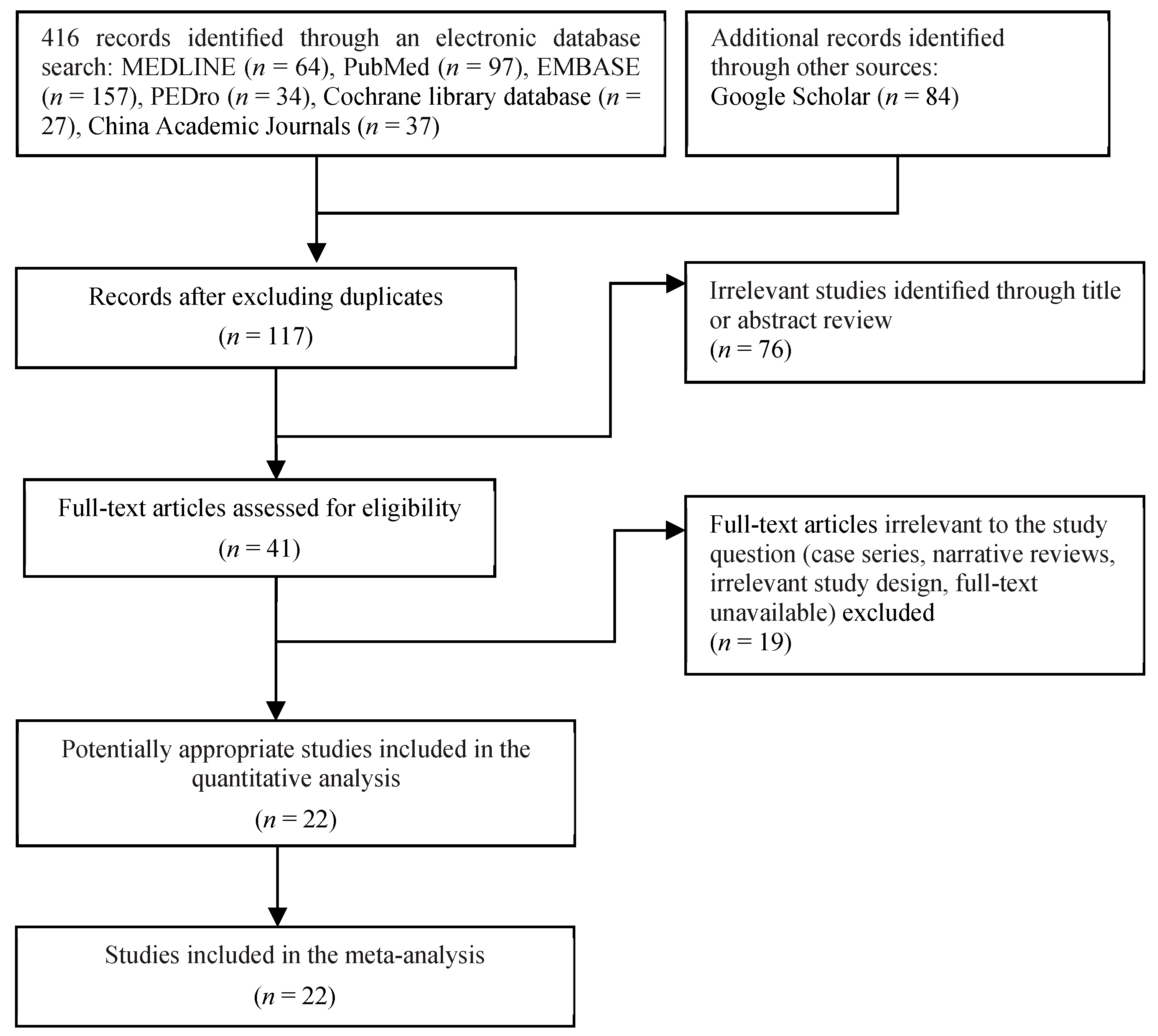
3.1. Trial Flow
3.2. Study Characteristics
3.3. Protein Supplementation Characteristics
3.4. Exercise Training Protocol
3.5. Risk of Bias in Included Studies
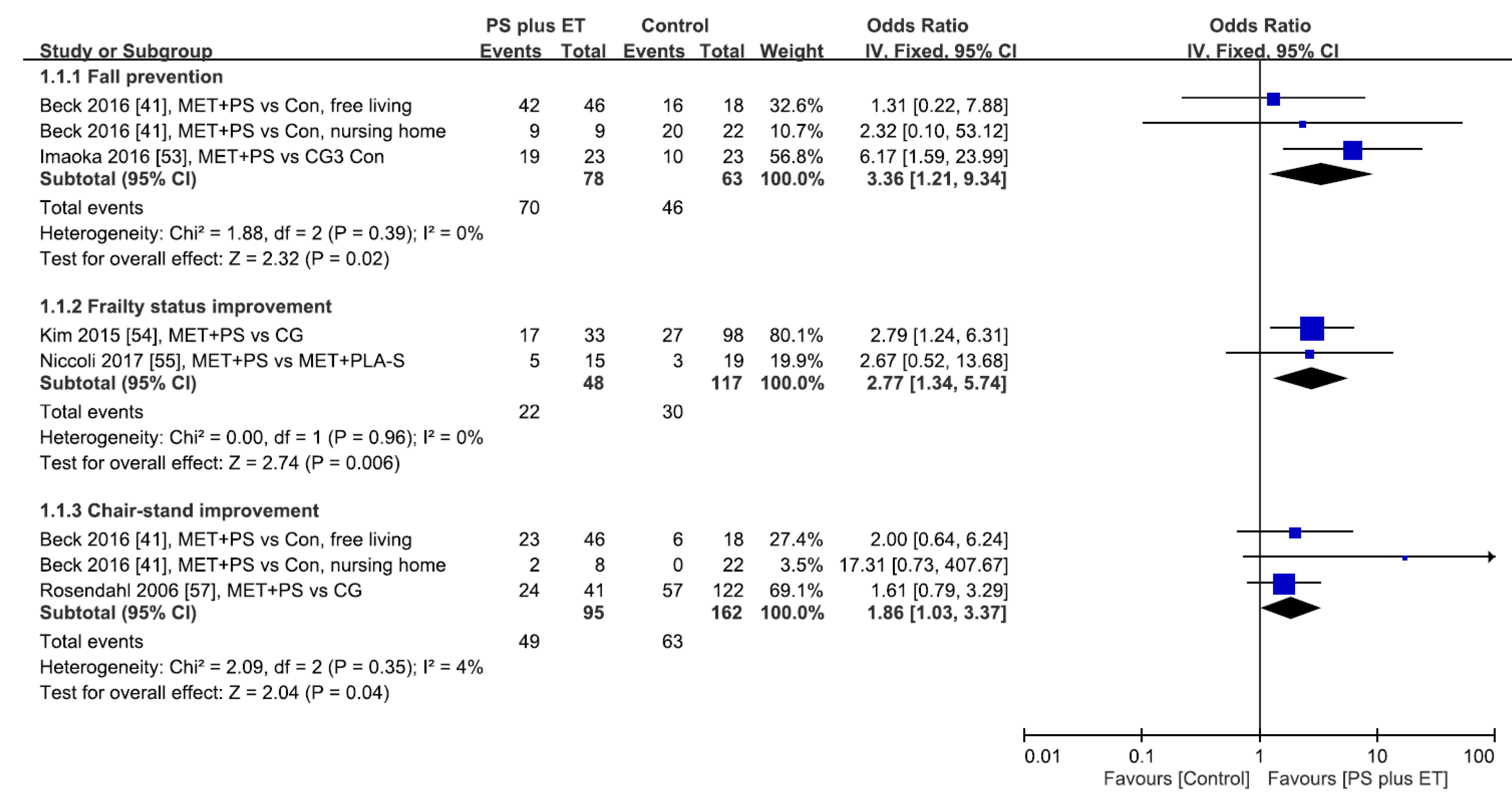
3.6. Success or Improvement Rates
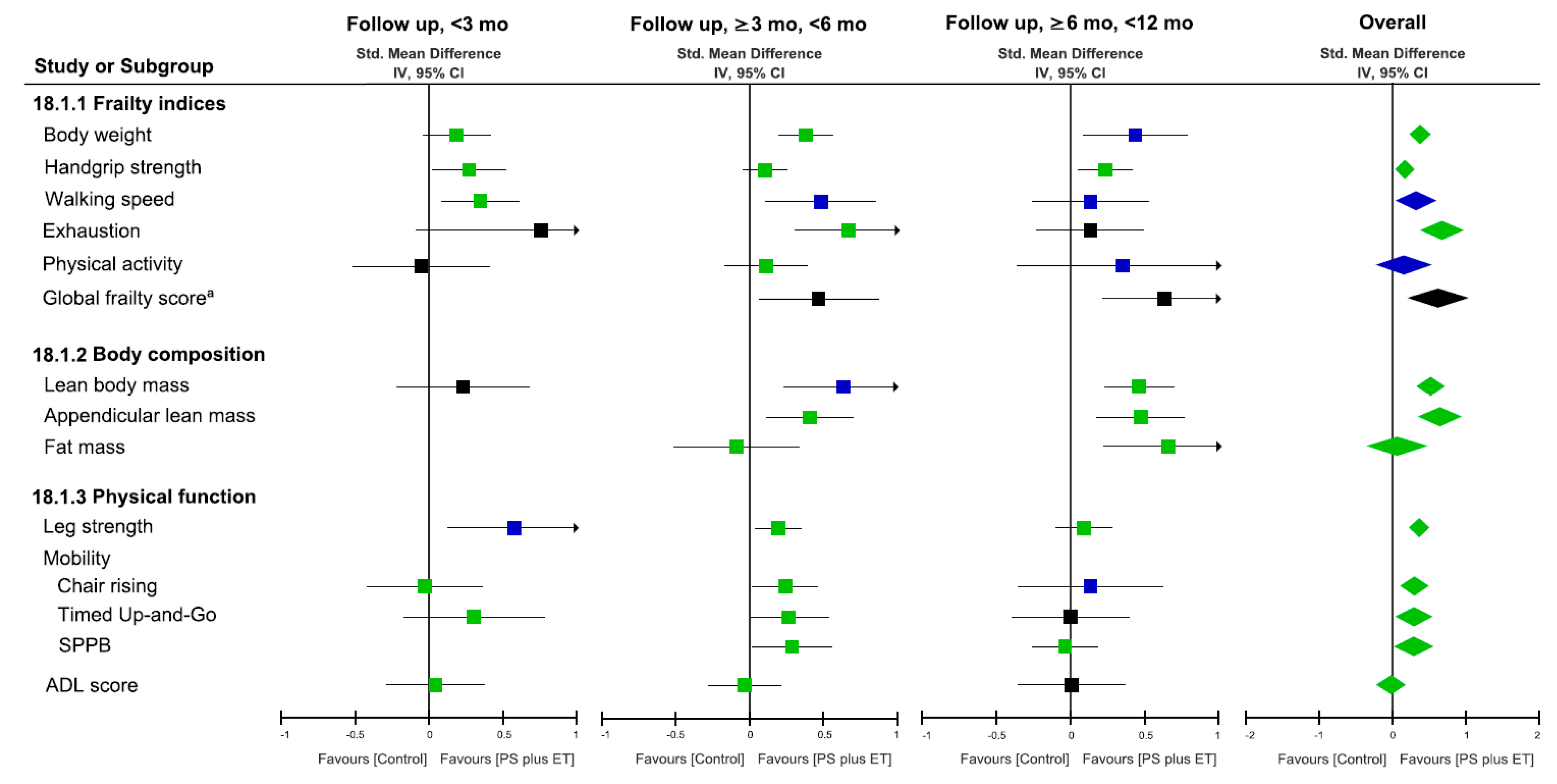
3.7. Effects on Frailty Indices
3.8. Effects on Body Composition
3.9. Effects on Leg Strength and Physical Mobility Outcome
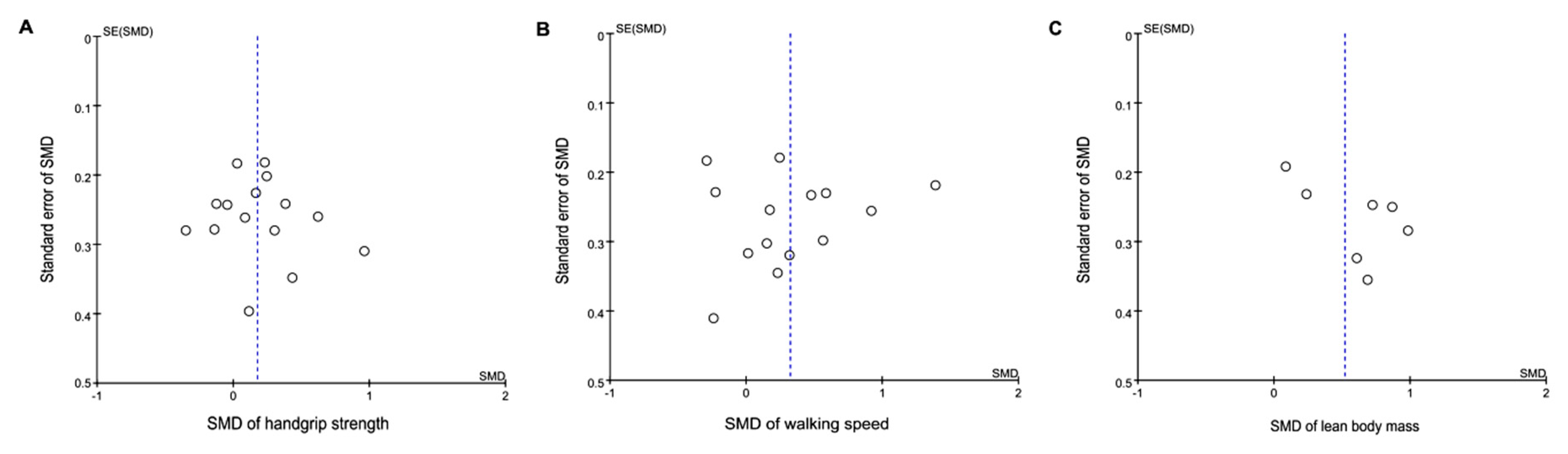
3.10. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bernabei, R.; Martone, A.M.; Vetrano, D.L.; Calvani, R.; Landi, F.; Marzetti, E. Frailty, Physical Frailty, Sarcopenia: A New Conceptual Model. Stud. Health Technol. Inform. 2014, 203, 78–84. [Google Scholar] [PubMed]
- Dodds, R.; Sayer, A.A. Sarcopenia and frailty: New challenges for clinical practice. Clin. Med. 2016, 16, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Harris, T. Muscle mass and strength: Relation to function in population studies. J. Nutr. 1997, 127, 1004S–1006S. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Deeg, D.J.; Lips, P.; Harris, T.B.; Bouter, L.M. Skeletal muscle mass and muscle strength in relation to lower-extremity performance in older men and women. J. Am. Geriatr. Soc. 2000, 48, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.N.; Ovesen, L.; Schroll, M.; Avlund, K.; Era, P. Body composition of 80-years old men and women and its relation to muscle strength, physical activity and functional ability. J. Nutr. Health Aging 2002, 6, 413–420. [Google Scholar] [PubMed]
- Yannakoulia, M.; Ntanasi, E.; Anastasiou, C.A.; Scarmeas, N. Frailty and nutrition: From epidemiological and clinical evidence to potential mechanisms. Metabol. Clin. Exp. 2017, 68, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Fabricio-Wehbe, S.C.; Rodrigues, R.A.; Haas, V.J.; Fhon, J.R.; Diniz, M.A. Association of frailty in hospitalized and institutionalized elderly in the community-dwelling. Revista Brasileira de Enfermagem 2016, 69, 691–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Vaca, J.; de la Rica-Escuin, M.; Silva-Iglesias, M.; Arjonilla-Garcia, M.D.; Varela-Perez, R.; Oliver-Carbonell, J.L.; Abizanda, P. Frailty in INstitutionalized older adults from ALbacete. The FINAL Study: Rationale, design, methodology, prevalence and attributes. Maturitas 2014, 77, 78–84. [Google Scholar] [CrossRef]
- Denison, H.J.; Cooper, C.; Sayer, A.A.; Robinson, S.M. Prevention and optimal management of sarcopenia: A review of combined exercise and nutrition interventions to improve muscle outcomes in older people. Clin. Interv. Aging 2015, 10, 859–869. [Google Scholar]
- Vincent, H.K.; Raiser, S.N.; Vincent, K.R. The aging musculoskeletal system and obesity-related considerations with exercise. Ageing Res. Rev. 2012, 11, 361–373. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.J.; Latham, N.K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009, CD002759. [Google Scholar] [CrossRef] [PubMed]
- Yarasheski, K.E. Exercise, aging, and muscle protein metabolism. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, M918–M922. [Google Scholar] [CrossRef]
- Seguin, R.; Nelson, M.E. The benefits of strength training for older adults. Am. J. Prev. Med. 2003, 25, 141–149. [Google Scholar] [CrossRef]
- Peterson, M.D.; Sen, A.; Gordon, P.M. Influence of resistance exercise on lean body mass in aging adults: A meta-analysis. Med. Sci. Sports Exerc. 2011, 43, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Bibas, L.; Levi, M.; Bendayan, M.; Mullie, L.; Forman, D.E.; Afilalo, J. Therapeutic interventions for frail elderly patients: Part I. Published randomized trials. Progr. Cardiovasc. Dis. 2014, 57, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Kong, J.; Underwood, C.; Petocz, P.; Hirani, V.; Dawson, B.; O’Leary, F. Systematic review and meta-analysis of the effect of protein and amino acid supplements in older adults with acute or chronic conditions. Br. J. Nutr. 2018, 119, 527–542. [Google Scholar] [CrossRef] [PubMed]
- Colonetti, T.; Grande, A.J.; Milton, K.; Foster, C.; Alexandre, M.C.; Uggioni, M.L.; Rosa, M.I. Effects of whey protein supplement in the elderly submitted to resistance training: Systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2017, 68, 257–264. [Google Scholar] [CrossRef]
- Finger, D.; Goltz, F.R.; Umpierre, D.; Meyer, E.; Rosa, L.H.; Schneider, C.D. Effects of protein supplementation in older adults undergoing resistance training: A systematic review and meta-analysis. Sports Med. 2015, 45, 245–255. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Wu, Y.T.; Cheng, C.P.; Chen, H.C.; Huang, Y.C.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Deeks, J.J.; Altman, D.G. Chapter 16: Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Neuberger, G.B. Measures of fatigue: The Fatigue Questionnaire, Fatigue Severity Scale, Multidimensional Assessment of Fatigue Scale, and Short Form-36 Vitality (Energy/Fatigue) Subscale of the Short Form Health Survey. Arthrit. Care Res. 2003, 49, S175–S183. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.M.; Damkjaer, K.; Beyer, N. Multifaceted nutritional intervention among nursing-home residents has a positive influence on nutrition and function. Nutrition 2008, 24, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Chen, K.T.; Hou, M.T.; Chang, Y.F.; Chang, C.S.; Liu, P.Y.; Wu, S.J.; Chiu, C.J.; Jou, I.M.; Chen, C.Y. Prevalence and associated factors of sarcopenia and severe sarcopenia in older Taiwanese living in rural community: The Tianliao Old People study 04. Geriatr. Gerontol. Int. 2014, 14 (Suppl. 1), 69–75. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar]
- McMurdo, M.E.; Johnstone, R. A randomized controlled trial of a home exercise programme for elderly people with poor mobility. Age Ageing 1995, 24, 425–428. [Google Scholar] [CrossRef]
- Briani, R.V.; Ferreira, A.S.; Pazzinatto, M.F.; Pappas, E.; De Oliveira Silva, D.; Azevedo, F.M. What interventions can improve quality of life or psychosocial factors of individuals with knee osteoarthritis? A systematic review with meta-analysis of primary outcomes from randomised controlled trials. Br. J. Sports Med. 2018, 52, 1031–1038. [Google Scholar] [CrossRef]
- Dorrestijn, O.; Stevens, M.; Winters, J.C.; van der Meer, K.; Diercks, R.L. Conservative or surgical treatment for subacromial impingement syndrome? A systematic review. J. Should. Elb. Surg. 2009, 18, 652–660. [Google Scholar] [CrossRef]
- Van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Functional fitness normative scores for community-residing older adults, ages 60–94. J. Aging Phys. Act. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.V.; Horak, F.B.; Tran, V.K.; Nutt, J.G. Multiple balance tests improve the assessment of postural stability in subjects with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Churchward-Venne, T.A.; Holwerda, A.M.; Phillips, S.M.; van Loon, L.J. What is the Optimal Amount of Protein to Support Post-Exercise Skeletal Muscle Reconditioning in the Older Adult? Sports Med. 2016, 46, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Beaudreuil, J.; Coudreuse, J.M.; Guyen, C.N.; Deat, P.; Chabaud, A.; Pereira, B.; Lorenzo, A.; Sailhan, F.; Rannou, F.; Coudeyre, E. An algorithm to improve knee orthosis prescription for osteoarthritis patients. Ann. Phys. Rehabil. Med. 2016, 59, e156. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.M.; Christensen, A.G.; Hansen, B.S.; Damsbo-Svendsen, S.; Moller, T.K. Multidisciplinary nutritional support for undernutrition in nursing home and home-care: A cluster randomized controlled trial. Nutrition 2016, 32, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.M.; Damkjaer, K.; Sorbye, L.W. Physical and social functional abilities seem to be maintained by a multifaceted randomized controlled nutritional intervention among old (>65 years) Danish nursing home residents. Arch. Gerontol. Geriatr. 2010, 50, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy, M.; Cornu, C.; Normand, S.; Boutitie, F.; Bugnard, F.; Rahmani, A.; Lacour, J.R.; Laville, M. The effects of exercise and protein-energy supplements on body composition and muscle function in frail elderly individuals: A long-term controlled randomised study. Br. J. Nutr. 2003, 89, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, M.; Littbrand, H.; Gustafson, Y.; Lundin-Olsson, L.; Lindelof, N.; Rosendahl, E.; Haglin, L. Effects of high-intensity exercise and protein supplement on muscle mass in ADL dependent older people with and without malnutrition: A randomized controlled trial. J. Nutr. Health Aging 2011, 15, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Chin A Paw, M.J.M.; de Jong, N.; Schouten, E.G.; Hiddink, G.J.; Kok, F.J. Physical exercise and/or enriched foods for functional improvement in frail, independently living elderly: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2001, 82, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, M.P.; Nelson, M.E.; Sacheck, J.M.; Reid, K.F.; Kirn, D.; Fielding, R.A.; Chui, K.K.H.; Folta, S.C. Efficacy of an Exercise and Nutritional Supplement Program on Physical Performance and Nutritional Status in Older Adults With Mobility Limitations Residing at Senior Living Facilities. J. Aging Phys. Act. 2017, 25, 453–463. [Google Scholar] [CrossRef] [PubMed]
- De Jong, N.; Chin A Paw, M.J.; de Groot, L.C.; de Graaf, C.; Kok, F.J.; van Staveren, W.A. Functional biochemical and nutrient indices in frail elderly people are partly affected by dietary supplements but not by exercise. J. Nutr. 1999, 129, 2028–2036. [Google Scholar] [CrossRef] [PubMed]
- Dirks, M.L.; Tieland, M.; Verdijk, L.B.; Losen, M.; Nilwik, R.; Mensink, M.; de Groot, L.C.P.G.M.; van Loon, L.J.C. Protein Supplementation Augments Muscle Fiber Hypertrophy but Does Not Modulate Satellite Cell Content During Prolonged Resistance-Type Exercise Training in Frail Elderly. J. Am. Med. Dir. Assoc. 2017, 18, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone, M.A.; O’Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise Training and Nutritional Supplementation for Physical Frailty in Very Elderly People. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef] [PubMed]
- Franzke, B.; Halper, B.; Hofmann, M.; Oesen, S.; Pierson, B.; Cremer, A.; Bacher, E.; Fuchs, B.; Baierl, A.; Tosevska, A.; et al. The effect of six months of elastic band resistance training, nutritional supplementation or cognitive training on chromosomal damage in institutionalized elderly. Exp. Gerontol. 2015, 65, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, M.; Schober-Halper, B.; Oesen, S.; Franzke, B.; Tschan, H.; Bachl, N.; Strasser, E.M.; Quittan, M.; Wagner, K.H.; Wessner, B. Effects of elastic band resistance training and nutritional supplementation on muscle quality and circulating muscle growth and degradation factors of institutionalized elderly women: The Vienna Active Ageing Study (VAAS). Eur. J. Appl. Physiol. 2016, 116, 885–897. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Aizawa, J.; Nagasawa, H.; Gomi, I.; Kugota, H.; Nanjo, K.; Jinno, T.; Masuda, T.; Morita, S. Effects and feasibility of exercise therapy combined with branched-chain amino acid supplementation on muscle strengthening in frail and pre-frail elderly people requiring long-term care: A crossover trial. Appl. Physiol. Nutr. Metabol. 2016, 41, 438–445. [Google Scholar] [CrossRef]
- Imaoka, M.; Higuchi, Y.; Todo, E.; Kitagwa, T.; Ueda, T. Low-frequency Exercise and Vitamin D Supplementation Reduce Falls Among Institutionalized Frail Elderly. Int. J. Gerontol. 2016, 10, 202–206. [Google Scholar] [CrossRef]
- Kim, H.; Suzuki, T.; Kim, M.; Kojima, N.; Ota, N.; Shimotoyodome, A.; Hase, T.; Hosoi, E.; Yoshida, H. Effects of exercise and milk fat globule membrane (MFGM) supplementation on body composition, physical function, and hematological parameters in community-dwelling frail Japanese women: A randomized double blind, placebo-controlled, follow-up trial. PLoS ONE 2015, 10, e0116256. [Google Scholar] [CrossRef] [PubMed]
- Niccoli, S.; Kolobov, A.; Bon, T.; Rafilovich, S.; Munro, H.; Tanner, K.; Pearson, T.; Lees, S.J. Whey Protein Supplementation Improves Rehabilitation Outcomes in Hospitalized Geriatric Patients: A Double Blinded, Randomized Controlled Trial. J. Nutr. Gerontol. Geriatr. 2017, 36, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Oesen, S.; Halper, B.; Hofmann, M.; Jandrasits, W.; Franzke, B.; Strasser, E.M.; Graf, A.; Tschan, H.; Bachl, N.; Quittan, M.; et al. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly—A randomized controlled trial. Exp. Gerontol. 2015, 72, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Rosendahl, E.; Lindelof, N.; Littbrand, H.; Yifter-Lindgren, E.; Lundin-Olsson, L.; Haglin, L.; Gustafson, Y.; Nyberg, L. High-intensity functional exercise program and protein-enriched energy supplement for older persons dependent in activities of daily living: A randomised controlled trial. Aust. J. Physiother. 2006, 52, 105–113. [Google Scholar] [CrossRef]
- Tieland, M.; Dirks, M.L.; van der Zwaluw, N.; Verdijk, L.B.; van de Rest, O.; de Groot, L.C.; van Loon, L.J. Protein supplementation increases muscle mass gain during prolonged resistance-type exercise training in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Trabal, J.; Forga, M.; Leyes, P.; Torres, F.; Rubio, J.; Prieto, E.; Farran-Codina, A. Effects of free leucine supplementation and resistance training on muscle strength and functional status in older adults: A randomized controlled trial. Clin. Interv. Aging 2015, 10, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Nishiguchi, S.; Fukutani, N.; Aoyama, T.; Arai, H. Mail-Based Intervention for Sarcopenia Prevention Increased Anabolic Hormone and Skeletal Muscle Mass in Community-Dwelling Japanese Older Adults: The INE (Intervention by Nutrition and Exercise) Study. J. Am. Med. Dir. Assoc. 2015, 16, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Zak, M.; Swine, C.; Grodzicki, T. Combined effects of functionally-oriented exercise regimens and nutritional supplementation on both the institutionalised and free-living frail elderly (double-blind, randomised clinical trial). BMC Public Health 2009, 9, 39. [Google Scholar] [CrossRef]
- Liao, C.-D.; Tsauo, J.-Y.; Chen, H.-C.; Liou, T.-H. Reply to RW Morton and SM Phillips. Am. J. Clin. Nutr. 2018, 107, 1056–1057. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; Rodrigues, B.; Uchida, M.; Marzetti, E. Low Protein Intake Is Associated with Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2018, 10, 1334. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, H.; Rezola-Pardo, C.; Gil, S.M.; Irazusta, J.; Rodriguez-Larrad, A. Physical training maintains or improves gait ability in long-term nursing home residents: A systematic review of randomized controlled trials. Maturitas 2018, 109, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznaric, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iuliano, S.; Poon, S.; Wang, X.; Bui, M.; Seeman, E. Dairy food supplementation may reduce malnutrition risk in institutionalised elderly. Br. J. Nutr. 2017, 117, 142–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tieland, M.; Beelen, J.; Laan, A.C.M.; Poon, S.; de Groot, L.; Seeman, E.; Wang, X.; Iuliano, S. An Even Distribution of Protein Intake Daily Promotes Protein Adequacy but Does Not Influence Nutritional Status in Institutionalized Elderly. J. Am. Med. Dir. Assoc. 2018, 19, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Douma, J.G.; Volkers, K.M.; Engels, G.; Sonneveld, M.H.; Goossens, R.H.M.; Scherder, E.J.A. Setting-related influences on physical inactivity of older adults in residential care settings: A review. BMC Geriatr. 2017, 17, 97. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Borgonjen-Van den Berg, K.J.; van Loon, L.J.; de Groot, L.C. Dietary protein intake in community-dwelling, frail, and institutionalized elderly people: Scope for improvement. Eur. J. Nutr. 2012, 51, 173–179. [Google Scholar] [CrossRef]
- Phillips, S.M. Nutritional supplements in support of resistance exercise to counter age-related sarcopenia. Adv. Nutr. 2015, 6, 452–460. [Google Scholar] [CrossRef]
- Hidayat, K.; Chen, G.-C.; Wang, Y.; Zhang, Z.; Dai, X.; Szeto, I.M.Y.; Qin, L.-Q. Effects of milk proteins supplementation in older adults undergoing resistance training: A meta-analysis of randomized control trials. J. Nutr. Health Aging 2018, 22, 237–245. [Google Scholar] [CrossRef]
- Guimarães-Ferreira, L.; Cholewa, J.M.; Naimo, M.A.; Zhi, X.I.; Magagnin, D.; de Sá, R.B.; Streck, E.L.; Teixeira Tda, S.; Zanchi, N.E. Synergistic effects of resistance training and protein intake: Practical aspects. Nutrition 2014, 30, 1097–1103. [Google Scholar] [CrossRef]
- Fry, A.C. The role of resistance exercise intensity on muscle fibre adaptations. Sports Med. 2004, 34, 663–679. [Google Scholar] [CrossRef] [PubMed]
- Helms, E.R.; Cronin, J.; Storey, A.; Zourdos, M.C. Application of the Repetitions in Reserve-Based Rating of Perceived Exertion Scale for Resistance Training. Strength Cond. J. 2016, 38, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Furtado, H.L.; Sousa, N.; Simao, R.; Pereira, F.D.; Vilaca-Alves, J. Physical exercise and functional fitness in independently living vs institutionalized elderly women: A comparison of 60- to 79-year-old city dwellers. Clin. Interv. Aging 2015, 10, 795–801. [Google Scholar] [PubMed]
- García-Molina, R.; Ruíz-Graob, M.C.; Noguerón-García, A.; Martinez-Reig, M.; Esbri-Victor, M.; Izquierdo, M.; Abizanda, P. Benefits of a multicomponent Falls Unit-based exercise program in older adults with falls in real life. Exp. Gerontol. 2018, 110, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Gwyther, H.; Bobrowicz-Campos, E.; Apostolo, J.L.A.; Marcucci, M.; Cano, A.; Holland, C. A realist review to understand the efficacy and outcomes of interventions designed to minimise, reverse or prevent the progression of frailty. Health Psychol. Rev. 2018, 12, 382–404. [Google Scholar] [CrossRef] [PubMed]
- Witard, O.C.; Jackman, S.R.; Breen, L.; Smith, K.; Selby, A.; Tipton, K.D. Myofibrillar muscle protein synthesis rates subsequent to a meal in response to increasing doses of whey protein at rest and after resistance exercise. Am. J. Clin. Nutr. 2014, 99, 86–95. [Google Scholar] [CrossRef]
- Moore, D.R.; Churchward-Venne, T.A.; Witard, O.; Breen, L.; Burd, N.A.; Tipton, K.D.; Phillips, S.M. Protein ingestion to stimulate myofibrillar protein synthesis requires greater relative protein intakes in healthy older versus younger men. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 57–62. [Google Scholar] [CrossRef]
- Francaux, M.; Demeulder, B.; Naslain, D.; Fortin, R.; Lutz, O.; Caty, G.; Deldicque, L. Aging reduces the activation of the mTORC1 pathway after resistance exercise and protein intake in human skeletal muscle: Potential role of REDD1 and impaired anabolic sensitivity. Nutrients 2016, 8, 47. [Google Scholar] [CrossRef]
- Yang, Y.; Breen, L.; Burd, N.A.; Hector, A.J.; Churchward-Venne, T.A.; Josse, A.R.; Tarnopolsky, M.A.; Phillips, S.M. Resistance exercise enhances myofibrillar protein synthesis with graded intakes of whey protein in older men. Br. J. Nutr. 2012, 108, 1780–1788. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, L.J.; Barbagallo, M. Perspective: Protein supplementation in frail older persons: Often necessary but not always sufficient. J. Am. Med. Dir. Assoc. 2013, 14, 72–73. [Google Scholar] [CrossRef]
- Morley, J.E. Do frail older persons need more protein? J. Am. Med. Dir. Assoc. 2012, 13, 667–668. [Google Scholar] [CrossRef] [PubMed]
- Tarazona-Santabalbina, F.J.; Gómez-Cabrera, M.C.; Pérez-Ros, P.; Martínez-Arnau, F.M.; Cabo, H.; Tsaparas, K.; Salvador-Pascual, A.; Rodriguez-Mañas, L.; Viña, J. A Multicomponent Exercise Intervention that Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2016, 17, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.; de Groot, L.C. Protein supplementation improves physical performance in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy, M.; Boutitie, F.; Mercier, C.; Gueyffier, F.; Carre, C.; Guetemme, G.; Ravis, B.; Laville, M.; Cornu, C. Efficacy of a home-based intervention programme on the physical activity level and functional ability of older people using domestic services: A randomised study. J. Nutr. Health Aging 2012, 16, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.E.; Alexander, D.D.; Perez, V. Effects of Whey Protein and Resistance Exercise on Body Composition: A Meta-Analysis of Randomized Controlled Trials. J. Am. Coll. Nutr. 2014, 33, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Gade, J.; Pedersen, R.J.; Beck, A.M. Effect of Protein or Essential Amino Acid Supplementation During Prolonged Resistance Exercise Training in Older Adults on Body Composition, Muscle Strength, and Physical Performance Parameters: A Systematic Review. Rehabil. Process Outcome 2018, 7, 1179572718765760. [Google Scholar] [CrossRef]
- Fu, R.; Gartlehner, G.; Grant, M.; Shamliyan, T.; Sedrakyan, A.; Wilt, T.J.; Griffith, L.; Oremus, M.; Raina, P.; Ismaila, A.; et al. Conducting quantitative synthesis when comparing medical interventions: AHRQ and the Effective Health Care Program. J. Clin. Epidemiol. 2011, 64, 1187–1197. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Notes on Subgroup Analyses and Meta-Regression. In Introduction to Meta-Analysis; Borenstein, M., Hedges, L.V., Higgins, J.P.T., Rothstein, H.R., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 205–212. [Google Scholar]
- Burd, N.A.; Tang, J.E.; Moore, D.R.; Phillips, S.M. Exercise training and protein metabolism: Influences of contraction, protein intake, and sex-based differences. J. Appl. Physiol. 2009, 106, 1692–1701. [Google Scholar] [CrossRef]
- Arnarson, A.; Gudny Geirsdottir, O.; Ramel, A.; Briem, K.; Jonsson, P.V.; Thorsdottir, I. Effects of whey proteins and carbohydrates on the efficacy of resistance training in elderly people: Double blind, randomised controlled trial. Eur. J. Clin. Nutr. 2013, 67, 821–826. [Google Scholar] [CrossRef]
- Leenders, M.; Verdijk, L.B.; Van der Hoeven, L.; Van Kranenburg, J.; Nilwik, R.; Wodzig, W.K.; Senden, J.M.; Keizer, H.A.; Van Loon, L.J. Protein supplementation during resistance-type exercise training in the elderly. Med. Sci. Sports Exerc. 2013, 45, 542–552. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year, Ref.) | Country (Area) | Groups 1 | Age (y) 2 | Sex (F/M) | N | Design | BMI (kg/m2) 2 | Patient Type | Body Composition Assessment Method | Exercise Intervention | Protein Supplement | Measured Time Point | Outcome Results | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type, Compliance (%, EG/CG) | Frequency × Duration | Type, Compliance (%, EG/CG) 10 | Intake Amount (g/day or g/session) | ||||||||||||
| Beck | Denmark | EG: PS + ET | 86.0 ± 8.4 | 41/14 | 55 | RCT | 20.7 ± 4.0 | Nursing- | NA | MET | 2 day/week × 11 weeks | Proteins | 18.0 g/session | Baseline | ↑ CRT7; HG8 |
| 2016 [41] | (Europe) | CG: Control3 | 87.3 ± 7.6 | 30/10 | 40 | 21.1 ± 3.3 | home residents | 71/NA | (22 sessions) | 100/NA | Posttest: 11 weeks | ||||
| Beck | Denmark | EG: PS + ET | 87 (84–90) | 42/20 | 62 | RCT | 23.4 (21.8–24.8) | Nursing- | DXA | MET | 2 day/week × 11 weeks | Milk protein | 7.0 g/day | Baseline | ↑ TUG7; ↑ HG7 |
| 2008 [26] | (Europe) | CG: Control3 | 86 (84–87) | 46/13 | 59 | SB | 23.4 (21.3–25.2) | home residents | 100/100 | (22 sessions) | 100/100 | 3.0 g/session | Posttest: 11 weeks | ↑ BBS7; ↑ CRT7 | |
| 2010 [42] | Follow-up: 27 weeks | ADL8; ↑ MDS-CPS7 | |||||||||||||
| Bonnefoy | France | EG: ET + PS | 83.5 ± 1.29 | 50/79 | 579 | RCT | 27.2 ± 0.99 | Frail older | DLW | MET | 3 day/week × 36 weeks | Proteins | 30.0 g/day | Baseline | FFM8; GS8; SC8 |
| 2003 [43] | (Europe) | CG 1: ET + PLA-S | SB | Individuals | method | 63-709 | (108 sessions) | 61/54 | Midtest: 12 weeks | ↑ Leg strength7 | |||||
| CG 2: PLA-S | Posttest: 36 weeks | ||||||||||||||
| Carlsson | Sweden | EG: PS + ET | 84.4 ± 6.3 | 33/9 | 42 | RCT | 25.1 ± 4.6 | Frail older | BIA | MET | 2–3 day/week × 13 weeks | Milk protein | 7.4 g /session | Baseline | ICW8; FM8; BBS8 |
| 2011 [44] | (Europe) | CG 1: ET + PLA-S | 85.3 ± 5.5 | 28/13 | 41 | DB | 25.2 ± 4.4 | individuals | 79/72 | (29 sessions) | 84/79 | Posttest: 12 weeks | |||
| CG 2: PS | 82.7 ± 6.4 | 34/13 | 47 | 24.9 ± 4.5 | Follow-up: 24 weeks | ||||||||||
| CG 3: PLA-S | 85.4 ± 7.2 | 36/11 | 47 | 24.6 ± 4.9 | |||||||||||
| Chin A | Netherlands | EG: PS + ET | 78.9 ± 6.0 | 31/11 | 42 | RCT | 25.0 ± 2.5 | Frail older | NA | MET | 2 day/week × 17 weeks | Proteins | 20.0 g/day | Baseline | ↑ GS7; ↑ TUG7 |
| Paw | (Europe) | CG 1: ET | 76.2 ± 4.5 | 28/11 | 39 | DB | 24.4 ± 2.9 | individuals | 90 (47–100) | (34 sessions) | 85/32 | Posttest: 17 weeks | |||
| 2001 [45] | CG 2: PS | 79.2 ± 4.8 | 28/11 | 39 | 24.5 ± 2.4 | ||||||||||
| CG 3: PLA-S | 78.6 ± 6.6 | 20/17 | 37 | 24.1 ± 3.1 | |||||||||||
| Corcoran | America | EG: PS + ET | 82.3 ± 7.6 | 56/11 | 67 | RCT | 28.2 ± 4.3 | Frail facility | NA | MET | 3 day/week × 24 weeks | Milk protein | 20.0 g /session | Baseline | ↑ PA6,8; ↑ HG6,8 |
| 2017 [46] | (Americas) | CG: Control3 | 81.2 ± 8.5 | 45/9 | 54 | SB | 28.5 ± 4.7 | residents | 81/68 | (72 sessions) | 87/NA | Midtest: 12 weeks | SPPB8; GS8 | ||
| Posttest: 24 weeks | |||||||||||||||
| de Jone | Netherlands | EG: PS + ET | 78.8 ± 6.1 | 28/11 | 39 | RCT, SB | 24.9 ± 2.5 | Frail older | NA | MET | 2 day/week × 17 weeks | Proteins | 20.0 g/day | Baseline | WBM8 |
| 1999 [47] | (Europe) | CG 1: ET | 76.5 ± 4.5 | 25/10 | 35 | 24.3 ± 3.1 | individuals | NR | (34 sessions) | NR | Posttest: 17 weeks | ||||
| CG 2: PS | 78.9 ± 4.8 | 26/11 | 37 | 24.3 ± 2.3 | |||||||||||
| CG 3: PLA-S | 78.7 ± 6.8 | 23/11 | 34 | 24.1 ± 3.2 | |||||||||||
| Dirks | Netherlands | EG: PS + ET | 76.0 ± 8.2 | 11/6 | 17 | RCT | 29.5 ± 4.9 | Frail older | DXA | RET | 2 day/week × 24 weeks | Milk protein | 30.0 g /session | Baseline | ↑ LBM6,7; ↑ ALM6,7; ↑ FM6,7 |
| 2017 [48] | (Europe) | CG: ET + PLA-S | 77.0 ± 8.2 | 11/6 | 17 | DB | 28.6 ± 3.7 | individuals | 84±29 | (48 sessions) | NR | Midtest: 12 weeks | ↓ CRT5,6; ↑ LP 1-RM5,6 | ||
| Posttest: 24 weeks | ↑ Muscle fiber CSA6 | ||||||||||||||
| Fiatarone | America | EG: PS + ET | 87.2 ± 6.0 | 16/9 | 25 | RCT | 24.5 ± 4.0 | Nursing- | WBP | RET | 3 day/week × 10 weeks | Soy protein | 40.8 g/day | Baseline | WBP8; ↑ GS6,7; ↑ SC6,7 |
| 1994 [49] | (Americas) | CG 1: ET + PLA-S | 86.2 ± 5.0 | 16/9 | 25 | DB | 24.9 ± 3.5 | home residents | method | 97/100 | (30 sessions) | 99/100 | Posttest: 10 weeks | ↑ leg strength6,7 | |
| CG 2: PS | 85.7 ± 5.8 | 17/7 | 24 | 25.4 ± 4.9 | Quadriceps CSA8 | ||||||||||
| CG 3: PLA-S | 89.2 ± 4.1 | 14/12 | 26 | 25.8 ± 5.1 | ↑ LP 1-RM6,7; ↑ PA6,7 | ||||||||||
| Franzke | Australia | EG: PS + ET | 82.5 ± 7.5 | 84/139 | 29 | RCT | NR | Institutionalized | NA | RET | 2 day/week × 24 weeks | Whey protein, | 20.7 g/day | Baseline | ↑ HG7; ↓ CRT5,6,7 |
| 2015 [50] | (Oceania) | CG 1: ET | 82.8 ± 5.7 | 35 | older | NR | (48 sessions) | Leucine, EAA, | 41.4 g /session | Midtest: 12 weeks | ↑ 6MWD5,6,7 | ||||
| CG 2: Control3 | 83.5 ± 5.4 | 33 | individuals | NR | Posttest: 24 weeks | ||||||||||
| Hofmann | Austria | EG: PS + ET | 84 (65–92) | 9/19 | 28 | RCT | 28.7 (22.9, 50.0) | Institutionalized | BIA | RET | 2 day/week × 24 weeks | Leucine, EAA | 20.7 g/day | Baseline | SMM8; HG8 |
| 2016 [51] | (Europe) | CG 1: ET | 83 (72–92) | 12/11 | 33 | 29.0 (22.7, 40.2) | older women | 71±26.59 | (48 sessions) | NR | 41.4 g /session | Midtest: 12 weeks | ↑ Leg MQ5,6,7 | ||
| CG 2: Control3 | 85 (69–92) | 10/20 | 30 | 29.7 (18.1, 36.9) | Posttest: 24 weeks | ||||||||||
| Ikeda | Japan | Tr 1 EG: PS + ET | 78.4 ± 7.8 | 9/18 | 27 | RCT, DB | 23.6 ± 3.4 | Frail older | NA | MET | 2 day/week × 12 weeks | EAA | 6.0 g/session | Baseline | ↑ LP 1-RM6; HG8; TUG8 |
| 2016 [52] | (Asian) | Tr 1 CG: ET + PLA-S | 80.4 ± 8.9 | 10/15 | 25 | Crossover | 21.9 ± 3.4 | individuals | 97.7/97.2 | (24 sessions) | 100/100 | Posttest: 12 weeks | Leg strength8; FRT6,7 | ||
| Tr 2 EG: PS + ET | 80.4 ± 8.9 | 10/15 | 25 | 21.6 ± 3.8 | 2 day/week × 12 weeks | Baseline | ↑ LP 1-RM6; HG8; TUG8 | ||||||||
| Tr 2 CG: ET + PLA-S | 78.4 ± 7.8 | 9/18 | 27 | 23.5 ± 3.5 | (24 sessions) | Posttest: 12 weeks | Quad strength8; FRT6 | ||||||||
| Imaoka | Japan | EG: PS + ET | 87.6 ± 6.5 | 18/5 | 23 | RCT | 20.4 ± 3.7 | Institutionalized | BIA | MET | 2 day/week × 12 weeks | Proteins | 4.1 g/day | Baseline | SMI8; FIM8 |
| 2016 [53] | (Asian) | CG 1: ET | 82.6 ± 9.1 | 16/6 | 22 | 20.5 ± 3.2 | frail older | NR | (24 sessions) | NR | Posttest: 12 weeks | ↓ Incidence of falls7 | |||
| CG 2: PS | 84.6 ± 7.7 | 20/3 | 23 | 20.4 ± 3.3 | individuals | Follow-up: 26 weeks | |||||||||
| CG 3: Control3 | 82.5 ± 10.9 | 15/8 | 23 | 20.6 ± 3.1 | |||||||||||
| Kim | Japan | EG: PS + ET | 81.0 ± 2.6 | 33/0 | 33 | RCT | 21.1 ± 3.64 | Frail older | DXA | MET | 2 day/week × 12 weeks | Milk protein | 22.0 g/day | Baseline | ALM8; LLM8; GH8 |
| 2015 [54] | (Asian) | CG 1: ET + PLA-S | 81.1 ± 2.8 | 33/0 | 33 | DB | 22.2 ± 4.34 | women | NR | (24 sessions) | NR | 22.0 g /session | Posttest: 12 weeks | ↑ GS7; ↑ TUG7 | |
| CG 2: PS | 81.0 ± 2.8 | 32/0 | 32 | 22.1 ± 4.24 | Follow-up: 28 weeks | Leg strength8 | |||||||||
| CG 3: PLA-S | 80.3 ± 3.3 | 33/0 | 33 | 22.9 ± 4.34 | ↓ Frailty score5,6,7 | ||||||||||
| Niccoli | Canada | EG: PS + ET | 81.8 ± 1.7 | 15/7 | 22 | RCT | 24.2 ± 5.2 | Hospitalized | NA | MET | 7 day/week × 4 wk10 | Whey protein | 24.0 g/day | Baseline | ↑ GS5,6,7; ↑ HG6,7 |
| 2017 [55] | (Americas) | CG: ET + PLA-S | 80.3 ± 1.6 | 17/8 | 25 | DB | 26.4 ± 6.6 | frail older individuals | NR | (28 sessions) | NR | Posttest: IPDC11 | ↓ TUG5,6; ↑ Leg strength6,7 | ||
| Oesen | Austria | EG: PS + ET | 81.8 ± 6.9 | 37/4 | 41 | RCT | 29.8 ± 6.1 | Institutionalized | NA | RET | 2 day/week | Leucine, EAA | 20.7 g/day | Baseline | ↑ Hand lifting5,6,7; ↓ CRT5,6,7 |
| 2015 [56] | (Europe) | CG 1: ET | 83.0 ± 5.5 | 31/5 | 36 | 28.9 ± 3.7 | older | 71±26.59 | × 24 weeks | NR | 41.4 g /session | Midtest: 12 weeks | ↑ Leg power5,6,7; ↑ GS5,6,7 | ||
| CG 2: Control3 | 83.4 ± 5.6 | 35/5 | 40 | 28.9 ± 5.0 | individuals | (48 sessions) | Posttest: 24 weeks | ↑ 6MWD5,6,7; ↑ PA5,6,7; FRT8 | |||||||
| Rosendahl | Sweden | EG: PS + ET | 85.0 ± 6.7 | 36/10 | 46 | RCT | 24.9 ± 4.6 | Institutionalized | NA | MET | 2−3 day/week | Milk protein | 7.4 g /session | Baseline | ↑ Leg power5,6,7 |
| 2006 [57] | (Europe) | CG 1: ET + PLA-S | 85.6 ± 5.5 | 31/14 | 45 | DB | 24.8 ± 4.4 | frail older | 72/70 | × 13 weeks | 82/78 | Posttest: 13 weeks | ↑ GS5,6,7; CRT6,7 | ||
| CG 2: PS | 82.9 ± 6.4 | 35/15 | 50 | 24.9 ± 4.4 | individuals | (29 sessions) | Follow-up: 24 weeks | ↑ BBS5,6,7 | |||||||
| CG 3: PLA-S | 85.6 ± 7.0 | 37/13 | 50 | 24.5 ± 4.9 | |||||||||||
| Tieland | Netherlands | EG: PS + ET | 78.0 ± 9.0 | 21/10 | 31 | RCT | 28.7 ± 4.5 | Frail older | DXA | RET | 2 day/week × 24 wk | Milk protein | 30.0 g/day | Baseline | ↑ LBM6,7; ↑ ALM6,7 |
| 2012 [58] | (Europe) | CG: ET + PLA-S | 79.0 ± 6.0 | 20/11 | 31 | DB | 28.2 ± 4.6 | individuals | ≥989 | (48 sessions) | ≥989 | Midtest: 12 weeks | ↑ FM6,7; ↑ LP 1-RM5,6 | ||
| Posttest: 24 weeks | ↓ CRT5,6 | ||||||||||||||
| Trabal | Spain | EG: PS + ET | 85.0 ± 8.0 | 16/89 | 12 | RCT | 26.6 ± 4.4 | Institutionalized | NR | MET | 4 day/week × 12 weeks | Leucine | 10.0 g/day | Baseline | ↑ Leg strength7; ↓ TUG7 |
| 2015 [59] | (Europe) | CG: ET + PLA-S | 84.0 ± 4.0 | 12 | DB | 26.0 ± 5.2 | older | 98±3/96±8 | (48 sessions) | 80±14/95±5 | Midtest: 4 weeks | ↑ Arm girth7; SLS8 | |||
| individuals | Posttest: 12 weeks | GS8; CRT8; SF-36 PF8 | |||||||||||||
| Yamada | Japan | EG: PS + ET | 78.1 ± 5.7 | 19/12 | 31 | RCT | 22.1 ± 3.6 | Frail older | BIA | Weighted | 7 day/week × 24 weeks | Protein | 10.0 g/day | Baseline | ↑ SMI7 |
| 2015 [60]12 | (Asian) | CG 1: ET | 75.7 ± 5.8 | 8/7 | 15 | 22.6 ± 3.1 | individuals | walking | (168 sessions) | (BCAA) | Posttest: 24 weeks | ||||
| CG 2: Control3 | 76.4 ± 6.2 | 15/10 | 25 | 23.2 ± 3.2 | NR | 80 (67−92) | |||||||||
| Zak | Poland | EG 1: PS + RET | 78.1 ± 7.6 | 16/3 | 19 | RCT | 24.7 ± 0.8 | Frail older | NA | RET | 5 day/week × 7 weeks | Proteins | 32.0 g/day | Baseline | ↑ 6MWD5,6 |
| 2009 [61] | (Europe) | CG 1: RET + PLA-S | 79.2 ± 9.2 | 17/4 | 21 | DB | 24.3 ± 0.6 | individuals | 100/100 | (35 sessions) | 100/100 | Posttest: 7 weeks | ↑ Tinetti-TS5 | ||
| EG 2: PS + SE | 78.3 ± 6.8 | 14/5 | 19 | 25.2 ± 0.7 | MET | ↑ Leg strength5,6 | |||||||||
| CG 2: SE + PLA-S | 81.1 ± 6.4 | 17/4 | 21 | 25.2 ± 0.6 | 100/100 | ||||||||||
| Study Author (Year) (Reference Number) | Overall b | Eligibility Criteria c | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beck 2016 [41] | 6/10 | X | X | X | X | X | X | X | ||||
| Beck 2008 [26] | 6/10 | X | X | X | X | X | X | X | ||||
| Beck 2010 [42] | 6/10 | X | X | X | X | X | X | X | ||||
| Bonnefoy 2003 [43] | 7/10 | X | X | X | X | X | X | X | X | |||
| Carlsson 2011 [44] | 9/10 | X | X | X | X | X | X | X | X | X | X | |
| Chin A Paw 2001 [45] | 9/10 | X | X | X | X | X | X | X | X | X | X | |
| Corcoran 2017 [46] | 6/10 | X | X | X | X | X | X | X | ||||
| de Jone 1999 [47] | 4/10 | X | X | X | X | |||||||
| Dirks 2017 [48] | 7/10 | X | X | X | X | X | X | X | X | |||
| Fiatarone 1994 [49] | 8/10 | X | X | X | X | X | X | X | X | X | ||
| Franzke 2015 [50] | 5/10 | X | X | X | X | X | X | |||||
| Hofmann 2016 [51] | 5/10 | X | X | X | X | X | ||||||
| Ikeda 2016 [52] | 7/10 | X | X | X | X | X | X | X | X | |||
| Imaoka 2016 [53] | 6/10 | X | X | X | X | X | X | X | ||||
| Kim 2015 [54] | 9/10 | X | X | X | X | X | X | X | X | X | X | |
| Niccoli 2017 [55] | 8/10 | X | X | X | X | X | X | X | X | X | ||
| Oesen 2015 [56] | 5/10 | X | X | X | X | X | X | |||||
| Rosendahl 2006 [57] | 8/10 | X | X | X | X | X | X | X | X | X | ||
| Tieland 2012 [58] | 7/10 | X | X | X | X | X | X | X | X | |||
| Trabal 2015 [59] | 5/10 | X | X | X | X | X | X | X | ||||
| Yamada 2015 [60] | 6/10 | X | X | X | X | X | X | X | ||||
| Zak 2009 [61] | 8/10 | X | X | X | X | X | X | X | X | X | ||
| Summary # | 20 | 22 | 5 | 22 | 11 | 6 | 10 | 14 | 14 | 22 | 22 |
| Subgroup | Global Frailty Score a | Whole Body Mass | Handgrip Strength | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparison, n (LoE) b | SMD | (95%CI) | p Value | I2 (%) | Comparison, n (LoE)b | SMD | (95%CI) | p Value | I2 (%) | Comparison, n (LoE)b | SMD | (95%CI) | p Value | I2 (%) | |
| Overall | 1 (M) | 0.62 | (0.21, 1.03) | 0.003 | NA | 11 (S) | 0.38 | (0.23, 0.52) † | <0.00001 | 37 | 15 (S) | 0.17 | (0.05, 0.30) † | 0.006 | 26 |
| MQ level (PEDro score) | |||||||||||||||
| ≥7/10 | 1 (M) | 0.62 | (0.21, 1.03) | 0.003 | NA | 6 (M) | 0.58 | (0.24, 0.92) ‡ | 0.0009 | 65 | 7 (S) | 0.31 | (0.11, 0.50) † | 0.002 | 50 |
| <7/10 | 0 | 5 (M) | 0.24 | (0.02, 0.46) † | 0.03 | 0 | 8 (C) | 0.08 | (0.08, 0.24) † | n.s. | 0 | ||||
| Subgroup difference | NA | NA | n.s. | 62.3 | n.s. | 54 | |||||||||
| Participant type | |||||||||||||||
| Community dweller | 1 (M) | 0.62 | (0.21, 1.03) | 0.003 | NA | 6 (M) | 0.58 | (0.25, 0.91) ‡ | 0.0006 | 65 | 7 (S) | 0.18 | (0.01, 0.36) † | 0.04 | 24 |
| Institutionalized resident | 0 | 5 (C) | 0.22 | (−0.02, 0.45) † | n.s. | 0 | 8 (C) | 0.17 | (−0.01, 0.34) † | n.s. | 37 | ||||
| Subgroup difference | NA | NA | n.s. | 66.5 | n.s. | 0 | |||||||||
| Population area | |||||||||||||||
| Americas | 0 | 1 (C) | 0.41 | (−0.06, 0.88) | n.s. | NA | 2 (C) | 0.46 | (−0.45, 1.37) ‡ | n.s. | 85 | ||||
| Asia | 1 (M) | 0.62 | (0.21, 1.03) | 0.003 | NA | 1 (M) | 0.66 | (0.26, 1.06) | 0.001 | NA | 4 (C) | 0.05 | (−0.19, 0.29) † | n.s. | 31 |
| Europe | 0 | 9 (S) | 0.33 | (0.16, 0.49) † | 0.0001 | 41 | 8 (S) | 0.24 | (0.06, 0.42) † | 0.007 | 0 | ||||
| Oceania | 0 | 0 | 1 (C) | −0.05 | (−0.52, 0.43) | n.s. | NA | ||||||||
| Subgroup difference | NA | NA | n.s. | 0 | n.s. | 0 | |||||||||
| Control group type | |||||||||||||||
| PLA-S or nonexercise | 1 (M) | 1.08 | (0.56, 1.60) | <0.0001 | NA | 7 (S) | 0.43 | (0.22, 0.64) † | <0.0001 | 38 | 9 (S) | 0.09 | (−0.09, 0.26) † | n.s. | 15 |
| Exercise | 1 (C) | 0.34 | (−0.14, 0.83) | n.s. | NA | 8 (S) | 0.32 | (0.14, 0.50) † | 0.0005 | 26 | 11 (S) | 0.28 | (0.12, 0.43) † | 0.0007 | 29 |
| PS | 1 (M) | 0.63 | (0.13, 1.13) | 0.01 | NA | 4 (S) | 0.37 | (0.11, 0.63) † | 0.006 | 56 | 2 (L) | 0.16 | (−0.22, 0.54) † | n.s. | 74 |
| Subgroup difference | n.s. | 52.1 | n.s. | 0 | n.s. | 4.7 | |||||||||
| Supplementation dose | |||||||||||||||
| ≥30 g/day (g/session) | 4 (S) | 0.65 | (0.36, 0.92 )† | <0.00001 | 35 | 5 (S) | 0.28 | (0.04, 0.51) † | 0.02 | 10 | |||||
| <30 g/day (g/session) | 1 (M) | 0.62 | (0.21, 1.03) | 0.003 | NA | 7 (S) | 0.26 | (0.07, 0.46) † | 0.001 | 9 | 10 (C) | 0.13 | (−0.01, 0.28) † | n.s. | 34 |
| Subgroup difference | NA | NA | 0.03 | 78.2 | n.s. | 0 | |||||||||
| Exercise type | |||||||||||||||
| RET | 0 | 4 (M) | 0.44 | (0.03, 0.84) ‡ | 0.04 | 63 | 6 (S) | 0.26 | (0.07, 0.46) † | 0.008 | 0 | ||||
| MET | 1 (M) | 0.62 | (0.21, 1.03) | 0.003 | NA | 7 (S) | 0.38 | (0.19, 0.56) † | <0.0001 | 21 | 9 (C) | 0.11 | (−0.05, 0.28) † | n.s. | 39 |
| Subgroup difference | NA | NA | n.s. | 0 | n.s. | 0 | |||||||||
| Intervention duration | |||||||||||||||
| <12 weeks | 0 | 5 (C) | 0.19 | (−0.04, 0.42) † | n.s. | 0 | 4 (C) | 0.29 | (−0.14, 0.72) ‡ | n.s. | 59 | ||||
| 12–24 weeks | 1 (M) | 0.62 | (0.21, 1.03) | 0.003 | NA | 7 (S) | 0.38 | (0.20, 0.57) † | <0.0001 | 19 | 11 (C) | 0.09 | (−0.05, 0.23) † | n.s. | 0 |
| ≥24 weeks | 0 | 4 (C) | 0.43 | (−0.02, 0.87) ‡ | 0.04 | 64 | 6 (S) | 0.23 | (0.04, 0.43) † | 0.02 | 0 | ||||
| Subgroup difference | NA | NA | n.s. | 0 | n.s. | 0 | |||||||||
| Overall | 14 (M) | 0.32 | (0.05, 0.59) ‡ | 0.02 | 75 | 2 (M) | 0.68 | (0.35, 1.02) † | <0.0001 | 0 | 6 (C) | 0.16 | (−0.22, 0.54) ‡ | n.s. | 76 |
| MQ level (PEDro score) | |||||||||||||||
| ≥7/10 | 10 (M) | 0.48 | (0.19, 0.77) ‡ | 0.001 | 67 | 2 (M) | 0.68 | (0.35, 1.02) † | <0.0001 | 0 | 4 (C) | 0.23 | (−0.35, 0.82) ‡ | n.s. | 83 |
| <7/10 | 4 (C) | 0.05 | (−0.54, 0.63) ‡ | n.s. | 82 | 0 | 2 (C) | 0.02 | (−0.30, 0.27) † | n.s. | 0 | ||||
| Subgroup difference | n.s. | 41.3 | NA | NA | n.s. | 0 | |||||||||
| Participant type | |||||||||||||||
| Community dweller | 8 (C) | 0.32 | (−0.08, 0.73) ‡ | n.s. | 80 | 0 | 4 (C) | 0.21 | (−0.38, 0.80) ‡ | n.s. | 85 | ||||
| Institutionalized resident | 6 (C) | 0.31 | (−0.03, 0.65) ‡ | n.s. | 65 | 2 (M) | 0.68 | (0.35, 1.02) † | <0.0001 | 52 | 2 (C) | 0.05 | (−0.28, 0.37) † | n.s. | 0 |
| Subgroup difference | n.s. | 0 | NA | NA | n.s. | 0 | |||||||||
| Population area | |||||||||||||||
| Americas | 3 (C) | 0.22 | (−0.36, 0.80) ‡ | n.s. | 79 | 0 | 2 (C) | −0.10 | 6(−0.38, 0.19) † | n.s. | 0 | ||||
| Asia | 1 (M) | 1.39 | (0.96, 1.82) | <0.0001 | NA | 0 | 9 (C) | 0.33 | (−0.43, 1.09) ‡ | n.s. | 86 | ||||
| Europe | 9 (S) | 0.17 | (0.01, 0.33) † | 0.04 | 0 | 2 (M) | 0.68 | (0.35, 1.02)† | <0.0001 | 52 | 1 (C) | 0.16 | (−0.31, 0.63) | n.s. | NA |
| Oceania | 1 (L) | 0.92 | (0.42, 1.42) | 0.0003 | NA | 0 | 0 | ||||||||
| Subgroup difference | <0.00001 | 90.5 | NA | NA | n.s. | 0 | |||||||||
| Control group type | |||||||||||||||
| PLA-S or nonexercise | 8 (M) | 0.38 | (0.21, 0.55) ‡ | <0.0001 | 77 | 0 | 4 (C) | 0.37 | (−0.15, 0.89)‡ | n.s. | 78 | ||||
| Exercise | 11 (C) | 0.16 | (−0.01, 0.33) † | n.s. | 0 | 2 (M) | 0.68 | (0.35, 1.02) † | <0.0001 | 52 | 5 (C) | 0.10 | (−0.51, 0.71) ‡ | n.s. | 84 |
| PS | 3 (S) | 0.44 | (0.16, 0.72) † | 0.002 | 60 | 0 | 2 (C) | 0.59 | (−0.27, 1.46) ‡ | n.s. | 80 | ||||
| Subgroup difference | n.s. | 40.5 | NA | NA | n.s. | 0 | |||||||||
| Supplementation dose | |||||||||||||||
| ≥30 g/day (g/session) | 8 (S) | 0.26 | (0.07, 0.45) † | 0.007 | 46 | 0 | 2 (C) | 0.05 | (−0.28, 0.37) † | n.s. | 0 | ||||
| <30 g/day (g/session) | 6 (C) | 0.39 | (−0.13, 0.91) ‡ | n.s. | 87 | 2 (M) | 0.68 | (0.35, 1.02) † | <0.0001 | 52 | 4 (M) | 0.21 | (−0.38, 0.80) ‡ | n.s. | 85 |
| Subgroup difference | n.s. | 0 | NA | NA | n.s. | 0 | |||||||||
| Exercise type | |||||||||||||||
| RET | 6 (C) | 0.31 | (−0.02, 0.64) ‡ | n.s. | 58 | 1 (L) | 0.67 | (0.30, 1.04) | 0.0003 | NA | 2 (C) | 0.05 | (−0.28, 0.37)† | n.s. | 0 |
| MET | 8 (C) | 0.32 | (−0.09, 0.73) ‡ | n.s. | 82 | 1 (C) | 0.75 | (−0.09, 1.58) | n.s. | NA | 4 (C) | 0.21 | (−0.38, 0.80)‡ | n.s. | 85 |
| Subgroup difference | n.s. | 0 | n.s. | 0 | n.s. | 0 | |||||||||
| Intervention duration | |||||||||||||||
| <12 weeks | 6 (S) | 0.32 | (0.11, 0.53) † | 0.003 | 0 | 1 (L) | 0.67 | (0.30, 1.04) | 0.0003 | NA | 1 (C) | −0.06 | (−0.51, 0.40)‡ | n.s. | NA |
| 12–24 weeks | 8 (M) | 0.53 | (0.09, 0.97) ‡ | 0.02 | 83 | 1 (C) | 0.75 | (−0.09, 1.58) | n.s. | NA | 3 (C) | 0.33 | (−0.43, 1.09)‡ | n.s. | 86 |
| ≥24 weeks | 6 (C) | −0.08 | (−0.28, 0.12) † | n.s. | 0 | 0 | 2 (C) | −0.02 | (−0.30, 0.27)† | n.s. | 0 | ||||
| Subgroup difference | 0.006 | 80.8 | n.s. | 0 | n.s. | 48.7 | |||||||||
| Subgroups | Lean Body Mass | Appendicular Skeletal Muscle Mass | Fat Mass | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparison, n (LoE) a | SMD | (95%CI) | p Value | I2 (%) | Comparison, n (LoE) a | SMD | (95%CI) | p Value | I2 (%) | Comparison, n (LoE) a | SMD | (95%CI) | p Value | I2 (%) | |
| Overall | 7 (S) | 0.52 | (0.33, 0.71) † | <0.00001 | 51 | 3 (S) | 0.64 | (0.34, 0.93) † | <0.0001 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| MQ level (PEDro score) | |||||||||||||||
| ≥7/10 | 5 (S) | 0.40 | (0.17, 0.62) † | 0.0005 | 53 | 3 (S) | 0.64 | (0.34, 0.93) † | <0.0001 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| <7/10 | 2 (M) | 0.80 | (0.45, 1.14) † | <0.00001 | 0 | 0 | 0 | ||||||||
| Subgroup difference | n.s. | 42.8 | NA | NA | NA | NA | |||||||||
| Participant type | |||||||||||||||
| Community dweller | 5 (S) | 0.51 | (0.28, 0.74) † | <0.0001 | 54 | 3 (S) | 0.64 | (0.34, 0.93) † | <0.0001 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| Institutionalized resident | 2 (M) | 0.53 | (0.20, 0.86) † | 0.002 | 71 | 0 | 0 | ||||||||
| Subgroup difference | n.s. | 0 | NA | NA | NA | NA | |||||||||
| Population area | |||||||||||||||
| Americas | 1 (C) | 0.24 | (−0.21, 0.69) | n.s. | NA | 0 | 0 | ||||||||
| Asia | 2 (M) | 0.80 | (0.45, 1.14) † | <0.00001 | 0 | 1 (M) | 0.54 | (0.14, 0.94) | 0.009 | NA | 0 | ||||
| Europe | 4 (S) | 0.45 | (0.19, 0.71) † | 0.0007 | 62 | 2 (S) | 0.75 | (0.32, 1.18) † | 0.0006 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| Oceania | 0 | 0 | 0 | ||||||||||||
| Subgroup difference | n.s. | 45.6 | n.s. | 0 | NA | NA | |||||||||
| Control group type | |||||||||||||||
| PLA-S or nonexercise | 5 (M) | 0.59 | (0.12, 1.07) ‡ | 0.01 | 72 | 1 (M) | 0.58 | (0.09, 1.07) | 0.02 | NA | 0 | ||||
| Exercise | 6 (S) | 0.51 | (0.27, 0.75) † | <0.0001 | 42 | 3 (S) | 0.59 | (0.26, 0.91) † | 0.0004 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| PS | 3 (S) | 0.35 | (0.04, 0.66) † | 0.02 | 44 | 1 (M) | 0.67 | (0.17, 1.17) | 0.009 | NA | 0 | ||||
| Subgroup difference | n.s. | 0 | n.s. | 0 | NA | NA | |||||||||
| Supplementation dose | |||||||||||||||
| ≥30 g/day (g/session) | 4 (S) | 0.71 | (0.40, 1.01)† | <0.00001 | 0 | 2 (S) | 0.75 | (0.32, 1.18) † | 0.0006 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| <30 g/day (g/session) | 3 (M) | 0.54 | (0.03, 104)† | n.s. | 45 | 1 (C) | 0.37 | (−0.11, 0.86) | n.s. | NA | 0 | ||||
| Subgroup difference | 0.04 | 76.7 | n.s. | 24.4 | NA | NA | |||||||||
| Exercise type | |||||||||||||||
| RET | 4 (S) | 0.61 | (0.35, 0.88)† | <0.00001 | 34 | 2 (S) | 0.75 | (0.32, 1.18) † | 0.0006 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| MET | 3 (C) | 0.49 | (−0.02, 1.01) ‡ | n.s. | 70 | 1 (C) | 0.37 | (−0.11, 0.86) | n.s. | NA | 0 | ||||
| Subgroup difference | 0.04 | 75.3 | n.s. | 24.4 | NA | NA | |||||||||
| Intervention duration | |||||||||||||||
| <12 weeks | 1 (C) | 0.24 | (−0.21, 0.69) | n.s. | NA | 0 | 0 | ||||||||
| 12–24 weeks | 5 (M) | 0.64 | (0.22, 1.06) ‡ | 0.003 | 67 | 3 (S) | 0.39 | (0.10, 0.68) † | 0.008 | 0 | 2 (C) | 0.08 | (−0.33, 0.50) † | n.s. | 0 |
| ≥24 weeks | 5 (S) | 0.51 | (0.18, 0.84) † | 0.002 | 48 | 2 (S) | 0.75 | (0.32, 1.18) † | 0.0006 | 0 | 2 (S) | 0.64 | (0.22, 1.07) † | 0.003 | 0 |
| Subgroup difference | n.s. | 0 | n.s. | 46.5 | n.s. | 70.9 | |||||||||
| Subgroups | Leg Muscle Strength | Chair Rise | Timed Up-and-Go | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparison, n (LoE) a | SMD | (95%CI) | p Value | I2 (%) | Comparison, n (LoE) a | SMD | (95%CI) | p Value | I2 (%) | Comparison, n (LoE) a | SMD | (95%CI) | p Value | I2 (%) | |
| Overall | 15 (S) | 0.37 | (0.23, 0.51) † | <0.00001 | 37 | 9 (S) | 0.30 | (0.11, 0.49) † | 0.002 | 25 | 5 (S) | 0.26 | (0.02, 0.51) † | 0.04 | 32 |
| MQ level (PEDro score) | |||||||||||||||
| ≥7/10 | 12 (S) | 0.38 | (0.16, 0.60) ‡ | 0.0006 | 50 | 4 (S) | 0.32 | (0.06, 0.59) † | 0.02 | 44 | 4 (C) | 0.25 | (−0.00, 0.50) † | n.s. | 46 |
| <7/10 | 3 (M) | 0.39 | (0.08, 0.70) † | 0.02 | 20 | 5 (M) | 0.27 | (0.01, 0.54) † | 0.04 | 23 | 1 (C) | 0.57 | (−0.69, 1.83) | n.s. | NA |
| Subgroup difference | n.s. | 0 | n.s. | 0 | n.s. | 0 | |||||||||
| Participant type | |||||||||||||||
| Community dweller | 9 (S) | 0.23 | (0.05, 0.41) † | 0.01 | 0 | 5 (C) | 0.22 | (−0.11, 0.55) ‡ | n.s. | 45 | 3 (C) | 0.25 | (−0.03, 0.53) † | n.s. | 64 |
| Institutionalized resident | 6 (S) | 0.57 | (0.36, 0.78) † | <0.00001 | 44 | 4 (M) | 0.39 | (0.08, 0.70) † | 0.01 | 0 | 2 (C) | 0.29 | (.23, 0.82) † | n.s. | 0 |
| Subgroup difference | 0.01 | 83.2 | n.s. | 0 | n.s. | 0 | |||||||||
| Population area | |||||||||||||||
| Americas | 2 (S) | 1.02 | (0.65, 1.40) † | <0.00001 | 0 | 0 | 1 (C) | 0.23 | (−0.34, 0.81) | n.s. | NA | ||||
| Asia | 3 (S) | 0.28 | (−0.09, 0.64) † | n.s. | 39 | 0 | 3 (C) | 0.25 | (0.03, 0.53) † | n.s. | 64 | ||||
| Europe | 10 (S) | 0.28 | (0.11, 0.45) † | 0.001 | 0 | 8 (S) | 0.31 | (0.10, 0.51) † | 0.003 | 34 | 1 (C) | 0.57 | (−0.69, 1.83) | n.s. | NA |
| Oceania | 0 | 1 (C) | 0.25 | (−0.26, 0.75) | n.s. | NA | 0 | ||||||||
| Subgroup difference | 0.002 | 84.5 | n.s. | 0 | n.s. | 0 | |||||||||
| Control group type | |||||||||||||||
| PLA-S or nonexercise | 7 (S) | 0.45 | (0.24, 0.67) † | <0.0001 | 37 | 6 (S) | 0.42 | (0.19, 0.65) † | 0.0003 | 31 | 1 (C) | 0.84 | (0.33, 1.34) | 0.001 | NA |
| Exercise | 13 (S) | 0.20 | (0.04, 0.36) † | 0.01 | 39 | 5 (S) | 0.09 | (−0.19, 0.36) † | n.s. | 12 | 5 (C) | −0.01 | (−0.27, 0.25) † | n.s. | 0 |
| PS | 4 (S) | 0.30 | (0.02, 0.59) † | 0.03 | 50 | 0 | 1 (M) | 1.30 | (0.77, 1.84) | <0.00001 | NA | ||||
| Subgroup difference | n.s. | 20.4 | n.s. | 61.4 | <0.0001 | 91.3 | |||||||||
| Supplementation dose | |||||||||||||||
| ≥30 g/day (g/session) | 8 (M) | 0.40 | (0.21, 0.59) ‡ | 0.008 | 52 | 5 (S) | 0.35 | (0.10, 0.59) † | 0.005 | 42 | 0 | ||||
| <30 g/day (g/session) | 7 (S) | 0.34 | (0.15, 0.53) † | 0.0004 | 22 | 4 (C) | 0.34 | (0.15, 0.53) † | n.s. | 12 | 5 (S) | 0.26 | (0.02, 0.51) † | 0.04 | 32 |
| Subgroup difference | n.s. | 0 | n.s. | 0 | NA | NA | |||||||||
| Exercise type | |||||||||||||||
| RET | 6 (M) | 0.37 | (0.04, 0.70) ‡ | 0.03 | 57 | 4 (S) | 0.29 | (0.03, 0.56) † | 0.03 | 50 | 0 | ||||
| MET | 9 (S) | 0.37 | (0.17, 0.58) † | 0.0004 | 24 | 5 (S) | 0.31 | (0.03, 0.58) † | 0.03 | 16 | 5 (S) | 0.26 | (0.02, 0.51) † | 0.04 | 32 |
| Subgroup difference | n.s. | 0 | n.s. | 0 | NA | NA | |||||||||
| Intervention duration | |||||||||||||||
| <12 weeks | 5 (M) | 0.58 | (0.14, 1.01) ‡ | 0.009 | 60 | 3 (C) | −0.03 | (−0.42, 0.36) † | n.s. | 0 | 4 (C) | 0.06 | (−0.25, 0.37) † | n.s. | 0 |
| 12–24 weeks | 11 (S) | 0.22 | (0.06, 0.37) † | 0.006 | 10 | 6 (M) | 0.23 | (0.01, 0.45) † | 0.04 | 8 | 4 (M) | 0.27 | (0.01, 0.55) ‡ | 0.04 | 49 |
| ≥24 weeks | 5 (C) | 0.21 | (−0.03, 0.45) † | n.s. | 0 | 5 (S) | 0.14 | (−0.35, 0.63) ‡ | n.s. | 75 | 0 | ||||
| Subgroup difference | n.s. | 16.7 | n.s. | 0 | n.s. | 0 | |||||||||
| Measures | PS Plus Exercise Training | PS plus MET | PS Plus RET | Influence Factors | |||
|---|---|---|---|---|---|---|---|
| Effect Size (SMD) a | LoE b | Effect Size (SMD) a | LoE b | Effect Size (SMD) a | LoE b | ||
| Frailty index c | |||||||
| Whole body mass | Large (0.44) | S | Medium (0.38) | M | Large (0.44) | S | Supplementation dose |
| Handgrip strength | Medium (0.26) | S | n.s. | C | Medium (0.26) | S | none |
| Walking speed | Medium (0.32) | M | n.s. | C | n.s. | C | Intervention duration Population area |
| Exhaustion | Large (0.68) | M | n.s. | C | Large (0.67) | L | none |
| Physical activity | n.s. | C | n.s. | C | n.s. | C | none |
| Global frailty score | Medium (0.26) | M | Large (0.62) | M | No evidence | none | |
| Body composition | |||||||
| LBM | Large (0.52) | S | n.s. | C | Large (0.61) | S | Supplementation dose Exercise type |
| ASM | Large (0.64) | S | n.s. | C | Large (0.75) | S | none |
| Leg strength | Medium (0.37) | S | Medium (0.37) | S | Medium (0.37) | M | Participant type; population area |
| Mobility | |||||||
| Chair rise | Medium (0.30) | S | Medium (0.31) | S | Medium (0.29) | S | none |
| TUG | Medium (0.26) | S | Medium (0.26) | S | No evidence | none | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-D.; Lee, P.-H.; Hsiao, D.-J.; Huang, S.-W.; Tsauo, J.-Y.; Chen, H.-C.; Liou, T.-H. Effects of Protein Supplementation Combined with Exercise Intervention on Frailty Indices, Body Composition, and Physical Function in Frail Older Adults. Nutrients 2018, 10, 1916. https://doi.org/10.3390/nu10121916
Liao C-D, Lee P-H, Hsiao D-J, Huang S-W, Tsauo J-Y, Chen H-C, Liou T-H. Effects of Protein Supplementation Combined with Exercise Intervention on Frailty Indices, Body Composition, and Physical Function in Frail Older Adults. Nutrients. 2018; 10(12):1916. https://doi.org/10.3390/nu10121916
Chicago/Turabian StyleLiao, Chun-De, Pi-Hsia Lee, Dun-Jen Hsiao, Shih-Wei Huang, Jau-Yih Tsauo, Hung-Chou Chen, and Tsan-Hon Liou. 2018. "Effects of Protein Supplementation Combined with Exercise Intervention on Frailty Indices, Body Composition, and Physical Function in Frail Older Adults" Nutrients 10, no. 12: 1916. https://doi.org/10.3390/nu10121916
APA StyleLiao, C. -D., Lee, P. -H., Hsiao, D. -J., Huang, S. -W., Tsauo, J. -Y., Chen, H. -C., & Liou, T. -H. (2018). Effects of Protein Supplementation Combined with Exercise Intervention on Frailty Indices, Body Composition, and Physical Function in Frail Older Adults. Nutrients, 10(12), 1916. https://doi.org/10.3390/nu10121916