Influence of Feeding Practices on Malnutrition in Haitian Infants and Young Children


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Prevalence of Malnutrition
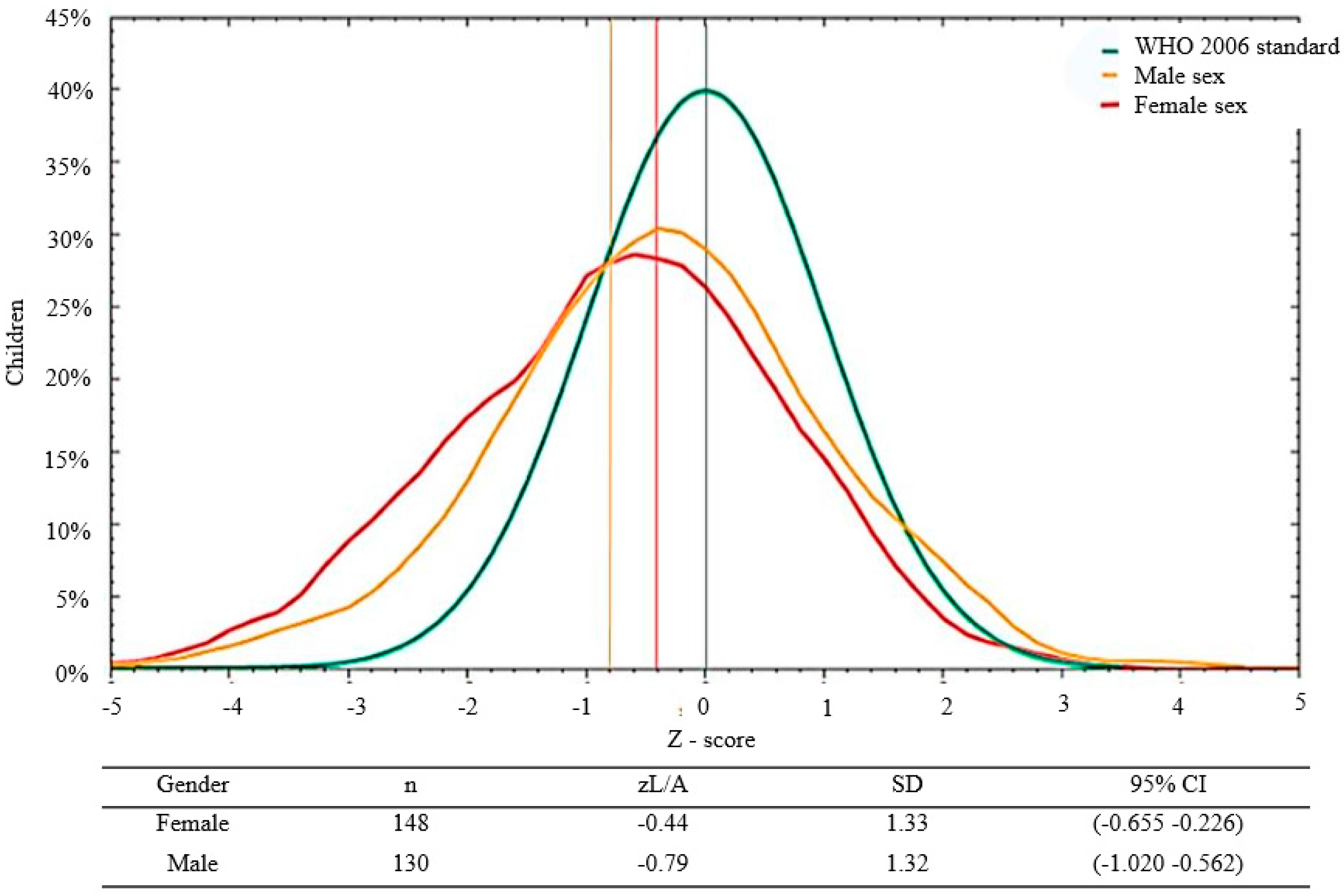
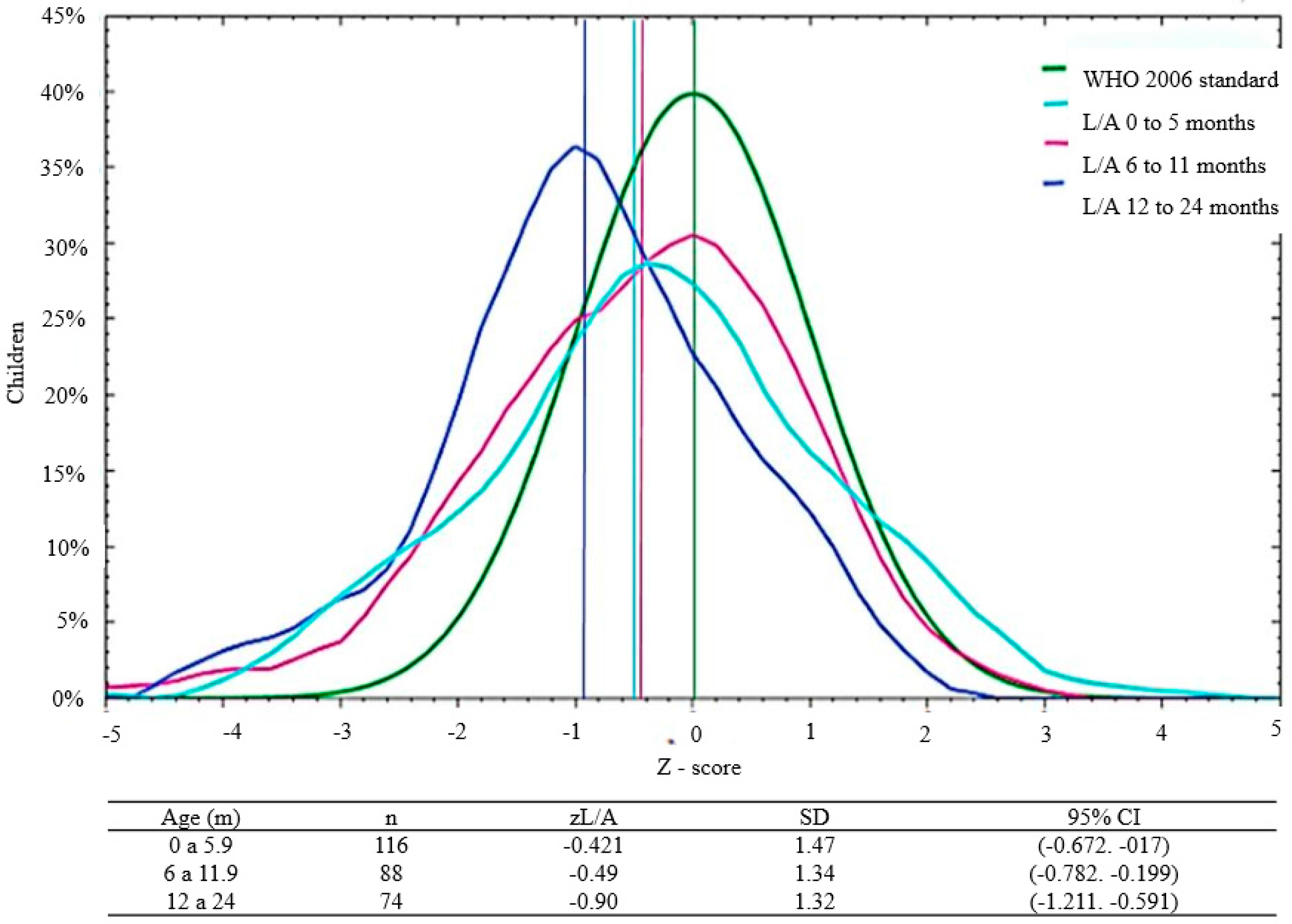
3.2. Malnutrition by Sex and Age
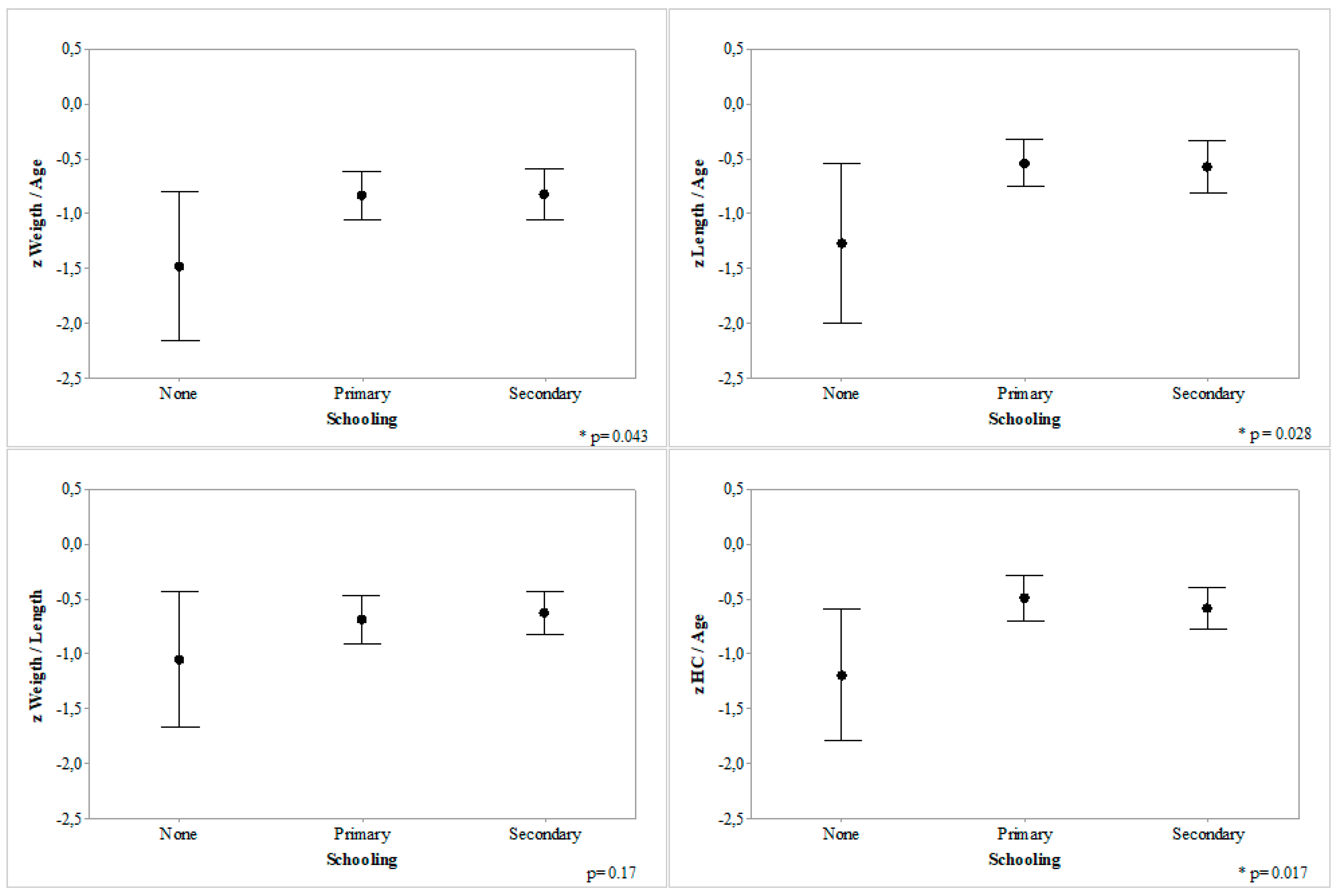
3.3. Malnutrition According to Family Characteristics
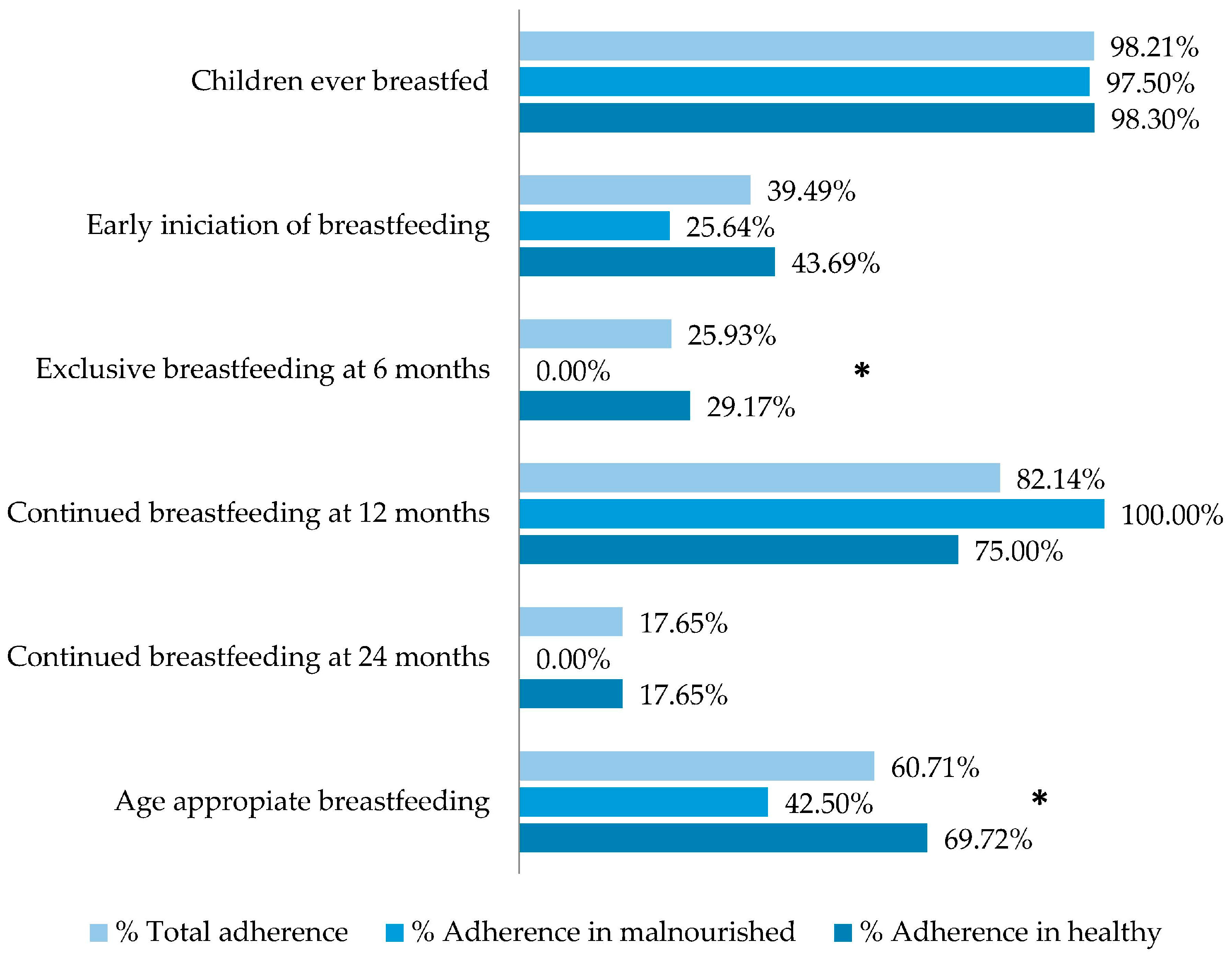
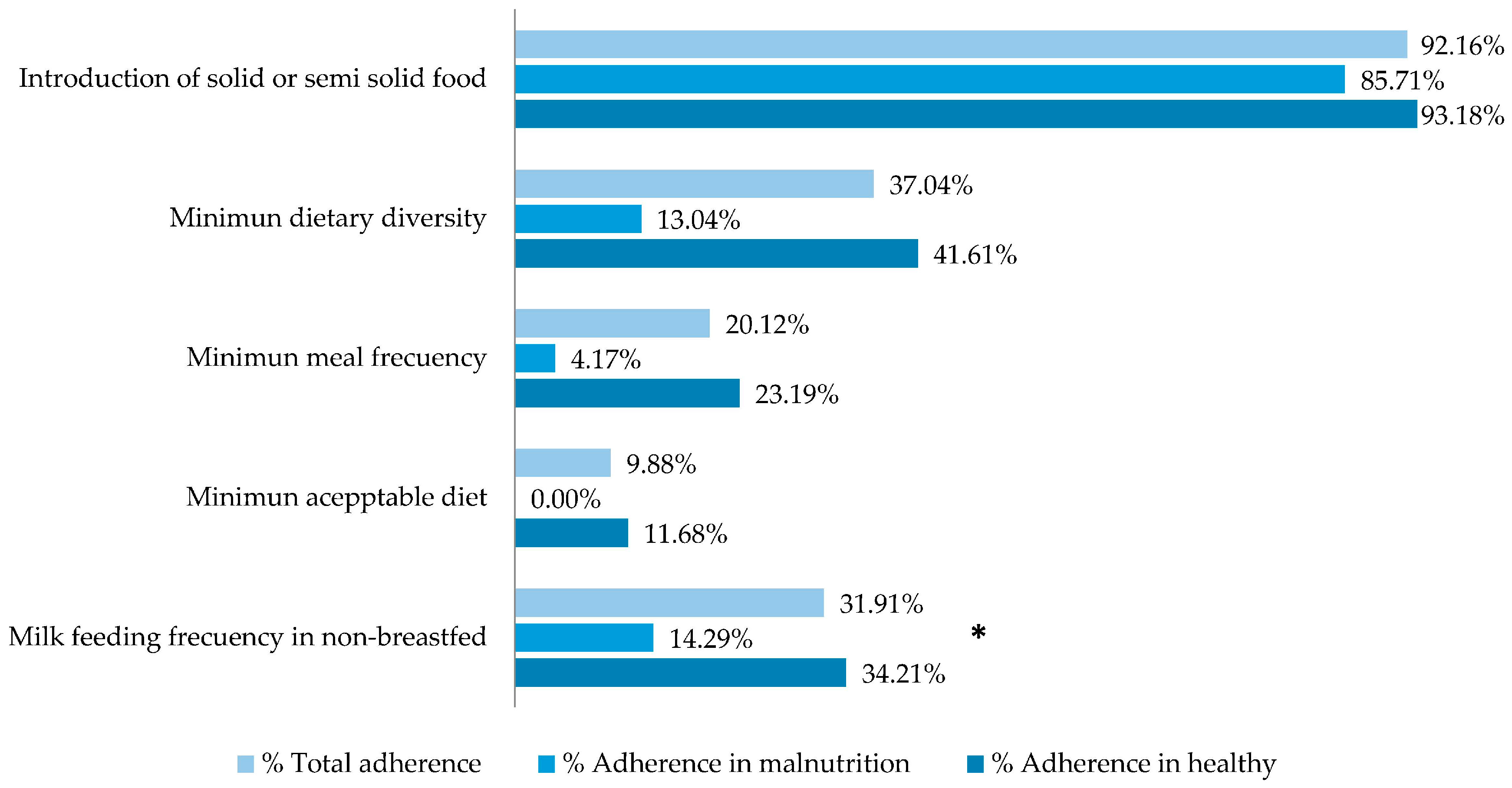
3.4. Feeding Practices
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
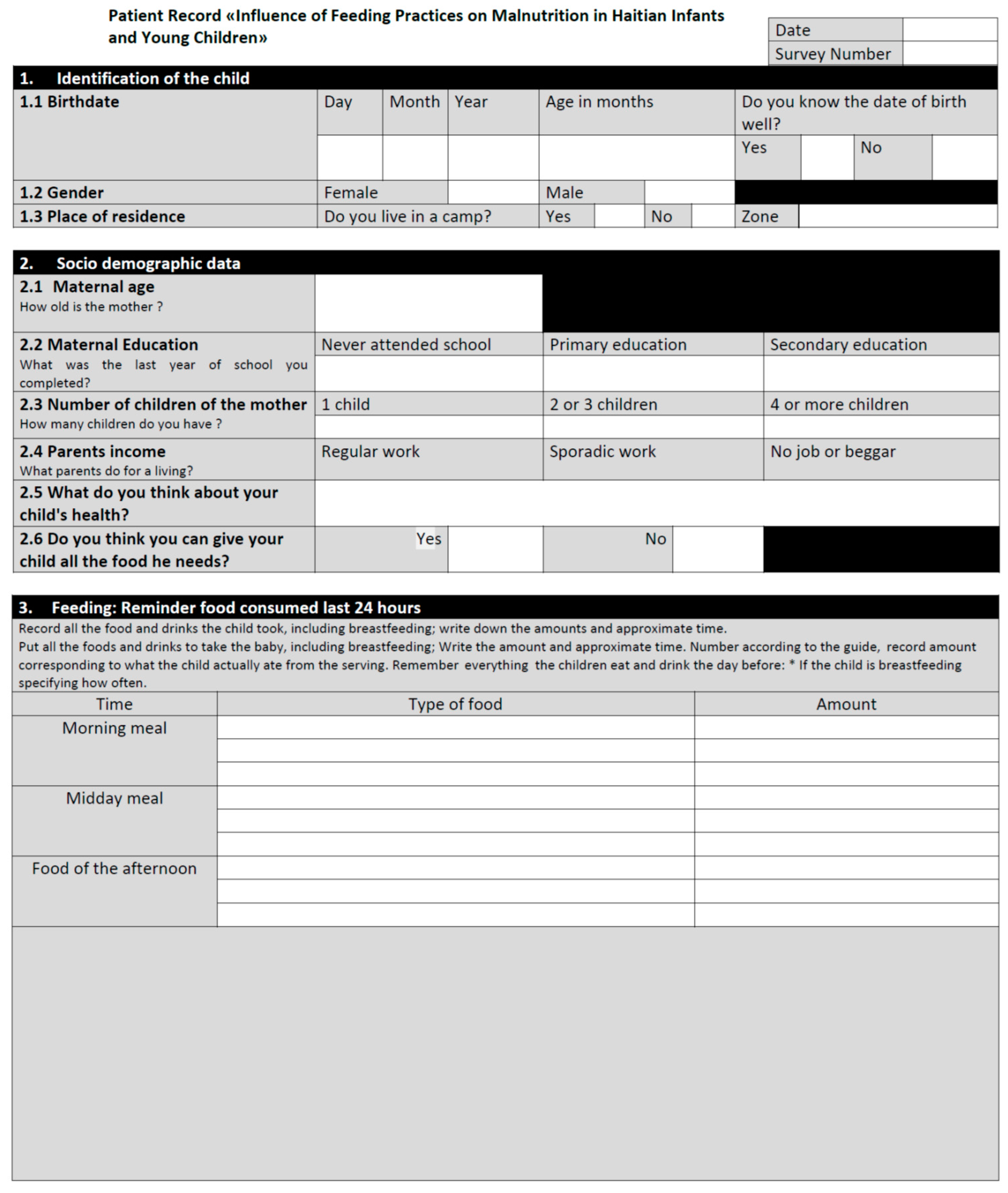
Appendix A
- Identification and general characteristics of the patient
- Brief social evaluation
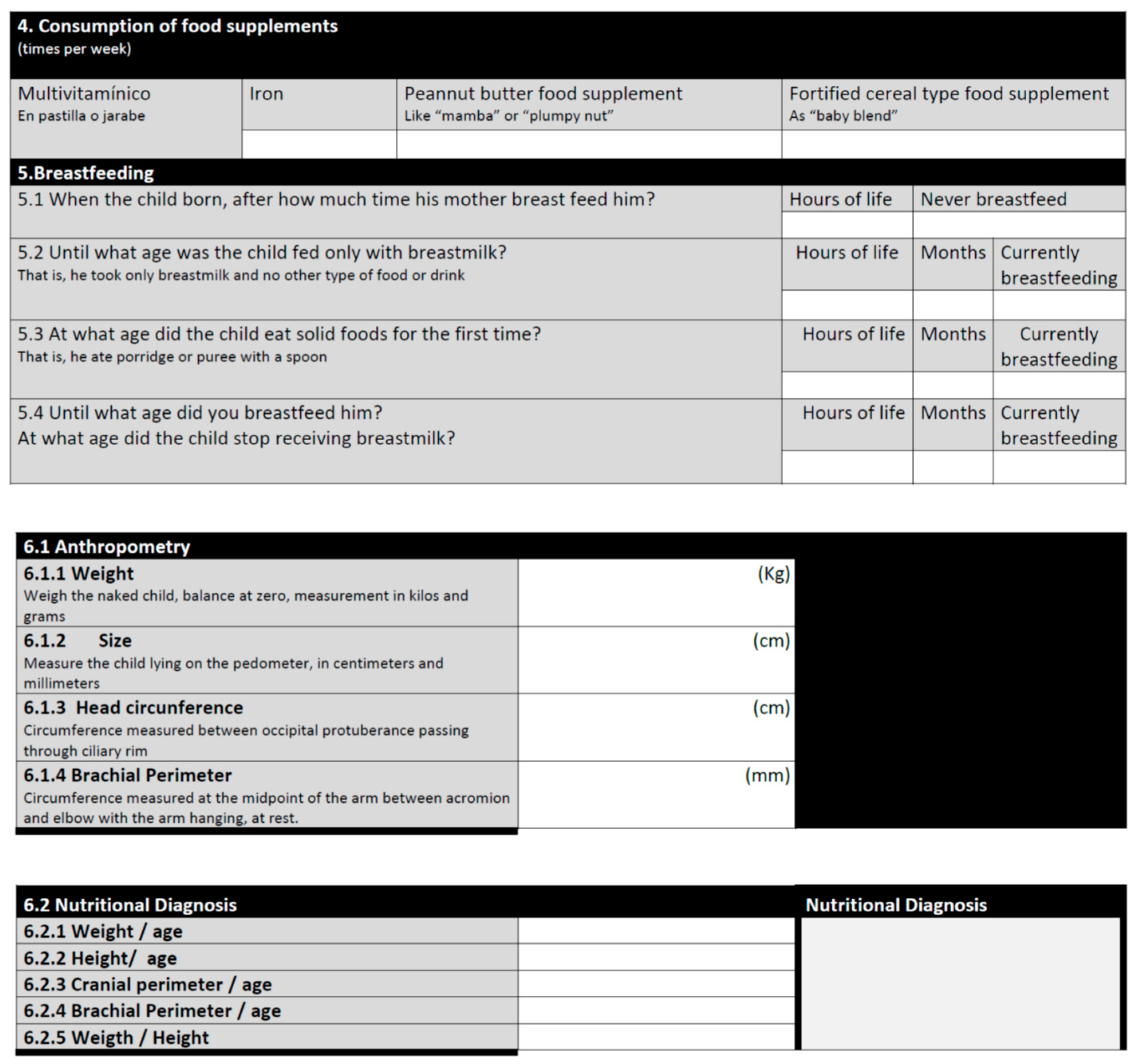
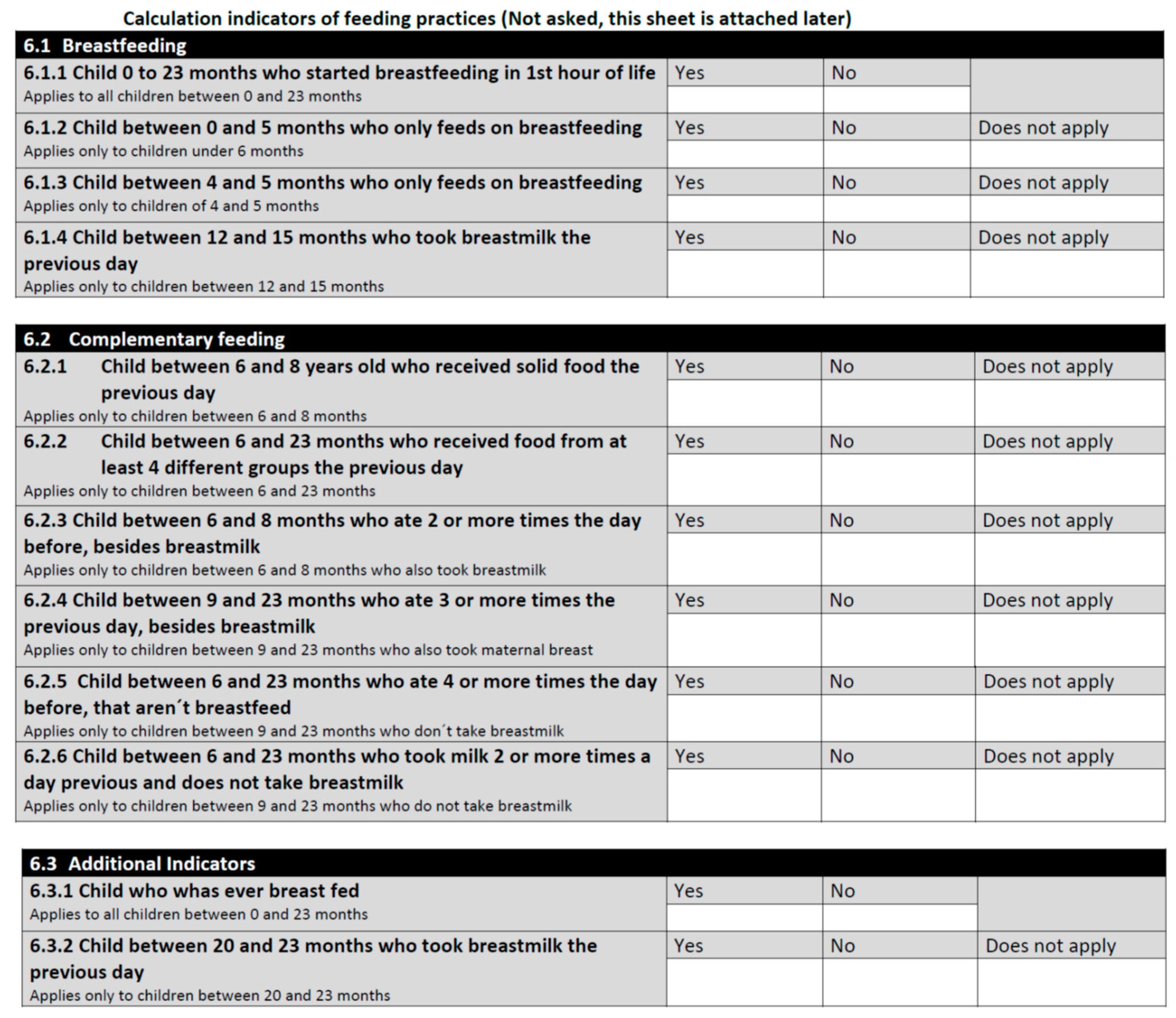
- Nutritional information
- 3.1.
- 24-h dietary recall
- 3.2.
- Use of nutritional supplements
- 3.3.
- Additional breastfeeding questions
- Anthropometry



Appendix B


References
- Ministry of health and population Haiti. Rapport de l’enquete Nutritionnelle Nationale Avec la Methodologie SMART. 2012. Available online: http://mspp.gouv.ht/site/downloads/SMART.pdf (accessed on 10 April 2016).
- Ministère de la Santé Publique et de la Population. Enquete Mortalite, Morbidite et Utilisation des Services EMMUS–IV Haiti 2005–2006; Institut Haïtien de l’Enfance Pétion-Ville, Haïti y Macro International Inc.: Calverton, MD, USA, 2007. Available online: https://dhsprogram.com/pubs/pdf/FR192/FR192.pdf (accessed on 10 April 2016).
- Ministère de la Santé Publique et de la Population. Enquete Mortalite, Morbidite et Utilisation des Services EMMUS–V Haiti 2012; Institut Haïtien de l’Enfance Pétion-Ville: Borno, Haiti, 2012. Available online: http://unfpahaiti.org/pdf/JMP2013_Rapport_de_synthEse_Haiti.pdf (accessed on 10 April 2016).
- World Health Organization (WHO) Country profiles. Haiti Country Profile. 2012. Available online: http://www.who.int/countries/hti/en/ (accessed on 18 January 2016).
- Ministry of Public Health and Population. [le Ministère de la Santé Publique and de la Population] (MSPP), Haitian Childhood Institute [l’Institut Haïtien de l’Enfance] (IHE) and ICF International. 2012 Haïti Mortality, Morbidity, and Service Utilization Survey: Key Findings; Ministry of Public Health and Population: Port-au-Prince, Haiti; MSPP, IHE, and ICF International: Calverton, MD, USA, 2013; p. 8. Available online: http://procurement-notices.undp.org/view_file.cfm?doc_id=17735 (accessed on 10 April 2016).
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices, Country profiles, Part I Definitions. Maternal, Newborn, Child and Adolescent Health; World Health Organization: Geneva, Switzerland, 2010; ISBN 9789241596664. Available online: http://www.who.int/maternal_child_adolescent/documents/9789241596664/en/ (accessed on 10 April 2016).
- Dependent on the Church of the Holy Spirit Catholic Church in Memphis, Tenesse. Available online: http://www.hspirit.com/ (accessed on 10 April 2016).
- Sunguya, B.F.; Poudel, K.C.; Mlunde, L.B.; Shakya, P.; Urassa, D.P.; Jimba, M.; Yasuoka, J. Effectiveness of nutrition training of health workers toward improving caregivers’ feeding practices for children aged six months to two years: A systematic review. Nutr. J. 2013, 12, 66–80. [Google Scholar] [CrossRef] [PubMed]
- Panamerican Health Organization. Guiding Principles for Complementary Feeding of the Breastfed Child; Nutrition Unit, Family Health and community Panamerican Health Organization: Washington, DC, USA, 2003; ISBN 9275324603. Available online: http://iris.paho.org/xmlui/handle/123456789/752 (accessed on 10 April 2016).
- World Health Organization. Guiding Principles for Feeding Non-Breastfed Children 6–24 Months of Age; World Health Organization: Geneva, Switzerland, 2005; ISBN 9789275327951. Available online: http://www.who.int/maternal_child_adolescent/documents/9241593431/en/ (accessed on 10 April 2016).
- World Health Organization. WHO Growth Standards for 0–5 Years; World Health Organization: Geneva, Switzerland, 2006; Available online: http://www.who.int/childgrowth/standards/en/ (accessed on 18 January 2016).
- Department of Nutrition, World Health Organization. WHO Anthro: Software for Assessing Growth and Development of the World’s Children; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- De Onis, M.; Yip, R.; Mei, Z. The development of MUAC-for age reference data recommended by a WHO Expert Committee. Bull. World Health Organ. 1997, 75, 11–18. [Google Scholar] [PubMed]
- De Onis, M.; Blössner, M. WHO Global Database on Child Growth and Malnutrition; World Health Organization: Geneva, Switzerland, 1997; pp. 45–47. [Google Scholar]
- Report of Monthly Patient Care Statistics; Klinik Saint Esprit: Port Au Prince, Haiti, 2014.
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization, Child Growth Standards: Geneva, Switzerland, 2016. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2004, 371, 243–260. [Google Scholar] [CrossRef]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Victora, C.G.; de Onis, M.; Hallal, P.C.; Blössner, M.; Shrimpton, R. Worldwide timing of growth faltering: Revisiting implications for interventions. Pediatrics 2010, 125, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Kac, G.; Alvear, J.L.G. Malnutrition in Latin America Network Program of Science and Technology for Development. Epidemiology of malnutrition in Latin America: Current situation. Nutr. Hosp. 2010, 25 (Suppl. 3), 50–56. [Google Scholar]
- Haroon, S.; Das, J.K.; Salam, R.A.; Imdad, A.; Bhutta, Z.A. Breastfeeding promotion interventions and breastfeeding practices: A systematic review. BMC Public Health 2013, 13 (Suppl. 3), S20. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Adu-Afarwuah, S. Systematic review of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern. Child Nutr. 2008, 4 (Suppl. 1), 24–85. [Google Scholar] [CrossRef] [PubMed]
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Imdad, A.; Yakoob, M.Y.; Bhutta, Z.A. Impact of maternal education about complementary feeding and provision of complementary foods on child growth in developing countries. BMC Public Health 2011, 13, S25. [Google Scholar] [CrossRef] [PubMed]
- Renfrew, M.J.; McCormick, F.M.; Wade, A.; Quinn, B.; Dowswell, T. Support for healthy breastfeeding mothers with healthy term babies. Cochrane Database Syst. Rev. 2012, CD001141. [Google Scholar] [CrossRef]
- Heckert, J.; Boatemaa, S.; Altman, C.E. Migrant youth’s emerging dietary patterns in Haiti: The role of peer social engagement. Public Health Nutr. 2014, 18, 1262–1271. [Google Scholar] [CrossRef] [PubMed]
- Diop El, H.I.; Dossou, N.I.; Ndour, N.M.; Briend, A.; Wade, S. Comparison of the efficacy of a solid ready-to-use food and a liquid, milk-based diet for the rehabilitation of severely malnourished children: A randomized trial. Am. J. Clin. Nutr. 2003, 78, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Ciliberto, M.A.; Sandige, H.; Ndekha, M.J.; Ashorn, P.; Briend, A.; Ciliberto, H.M.; Manary, M.J. Comparison of home-based therapy with ready-to-use therapeutic food with standard therapy in the treatment of malnourished Malawian children: A controlled, clinical effectiveness trial. Am. J. Clin. Nutr. 2005, 81, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Bisits Bullen, B.A. The positive deviance/hearth approach to reducing child malnutrition: Systematic review. Trop. Med. Int. Health 2011, 16, 1354–1366. [Google Scholar] [CrossRef] [PubMed]
- Picot, J.; Hartwell, D.; Harris, P.; Mendes, D.; Clegg, A.J.; Takeda, A. The effectiveness of interventions to treat severe acute malnutrition in young children: A systematic review. Health Technol. Assess. 2012, 16, 1–316. [Google Scholar] [CrossRef] [PubMed]
- Uauy, R. Undernutrition is undernourished. Public Health Nutr. 2008, 11, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Pridmore, P.; Carr-Hill, R. Tackling the drivers of child undernutrition in developing countries: What works and how should interventions be designed? Public Health Nutr. 2011, 14, 688–693. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization and UNICEF. Global Strategy for Infant and Young Child Feeding; WHO: Geneva, Switzerland, 2003; ISBN 924356221. Available online: http://www.who.int/nutrition/publications/infantfeeding/9241562218/en/ (accessed on 10 April 2016).
- World Health Organization. Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition; WHO: Geneva, Switzerland, 2013; ISBN 9789241505550. Available online: http://www.who.int/nutrition/publications/infantfeeding/essential_nutrition_actions/en/ (accessed on 10 April 2016).
- Ward, K.N.; Byrne, J.P. A critical review of the impact of continuing breastfeeding education provided to nurses and midwives. J. Hum. Lact. 2011, 27, 381–393. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics | Percentage | |
|---|---|---|
| Housing | Located in Croix de Bouquetes | 70.77% |
| Lightweight material houses or camp | 17.9% | |
| Parental work | Any kind of work: formal/informal | 34.5% |
| Parental education | Completed primary education | 43.5% |
| Illiterate | 15.35% | |
| Never attended to school | 6.5% | |
| Number of children | One child | 35.7% |
| Two or three children | 41.8% | |
| Four or more children | 22.5% | |
| Anthropometric Index | Nutritional Diagnosis | Degree | z-Score (WHO 2006) | Prevalence (%) |
|---|---|---|---|---|
| Weight/Age | Underweight | Severe | z W/A ≤ −3 | 6.12 |
| Moderate | z W/A −2 to −3 | 12.23 | ||
| Normal | z W/A −2 to +2 | 80.22 | ||
| Overweight | z W/A ≥ +2 | 1.44 | ||
| Weight/Length | Wasting | Severe | z W/L < −3 | 3.60 |
| Moderate | z W/L −2 to −3 | 10.07 | ||
| Normal | z W/L −2 to +2 | 84.9 | ||
| Overweight and obesity | z W/L > +2 | 1.80 | ||
| Length/Age | Stunting | z L/A < −2 | 13.31 | |
| Normal | z L/A −2 to +2 | 85.25 | ||
| Tall | z L/A > +2 | 1.44 | ||
| Head circumference/Age | Microcephaly | z HC/A < −2 | 10.80 | |
| Normal | z HC/A −2 to +2 | 86.68 | ||
| Macrocephaly | z HC/A > +2 | 2.52 | ||
| Brachial Circumference/Age | Low | z BC/A < −2 | 4.67 | |
| Normal | z BC/A > −2 | 95.33 | ||
| Indicator | Nutritional Status # (p) | ||
|---|---|---|---|
| Wasting | Underweight | Stunting | |
| 1. Children ever breastfed | 0.92 | 0.59 | 0.13 |
| 2. Early initiation of breastfeeding | 0.21 | 0.002 * | 0.04 * |
| 3. Exclusive breastfeeding under 6 months | 0.09 | 0.32 | 0.59 |
| 4. Predominant breastfeeding under 6 months | 0.97 | 0.000 * | 0.02 * |
| 5. Exclusive breastfeeding at 6 months | 0.03 * | 0.003 * | 0.54 |
| 6. Continued breastfeeding at 12 months | 0.73 | 0.82 | 1.00 |
| 7. Continued breastfeeding at 24 months | 0.16 | 0.54 | nv |
| 8. Age-appropriate breastfeeding | 0.03 * | 0.20 | 0.20 |
| 9. Introduction of complementary foods | 0.83 | 0.97 | 0.34 |
| 10. Minimum dietary diversity | 0.10 | 0.11 | 0.90 |
| 11. Minimum meal frequency | 0.75 | 0.70 | 0.90 |
| 12. Minimum acceptable diet | 0.21 | 0.049 * | 0.35 |
| 13. Milk feeding frequency for non-breastfed children | 0.02 * | 0.06 | 0.23 |
| 14. Consumption of iron rich foods | nv | nv | nv |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irarrázaval, B.; Barja, S.; Bustos, E.; Doirsaint, R.; Senethmm, G.; Guzmán, M.P.; Uauy, R. Influence of Feeding Practices on Malnutrition in Haitian Infants and Young Children. Nutrients 2018, 10, 382. https://doi.org/10.3390/nu10030382
Irarrázaval B, Barja S, Bustos E, Doirsaint R, Senethmm G, Guzmán MP, Uauy R. Influence of Feeding Practices on Malnutrition in Haitian Infants and Young Children. Nutrients. 2018; 10(3):382. https://doi.org/10.3390/nu10030382
Chicago/Turabian StyleIrarrázaval, Belén, Salesa Barja, Edson Bustos, Romel Doirsaint, Gloria Senethmm, María Paz Guzmán, and Ricardo Uauy. 2018. "Influence of Feeding Practices on Malnutrition in Haitian Infants and Young Children" Nutrients 10, no. 3: 382. https://doi.org/10.3390/nu10030382
APA StyleIrarrázaval, B., Barja, S., Bustos, E., Doirsaint, R., Senethmm, G., Guzmán, M. P., & Uauy, R. (2018). Influence of Feeding Practices on Malnutrition in Haitian Infants and Young Children. Nutrients, 10(3), 382. https://doi.org/10.3390/nu10030382