The Impact of Abdominal Fat Levels on All-Cause Mortality Risk in Patients Undergoing Hemodialysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Data Collection
2.3. Follow-Up Study
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
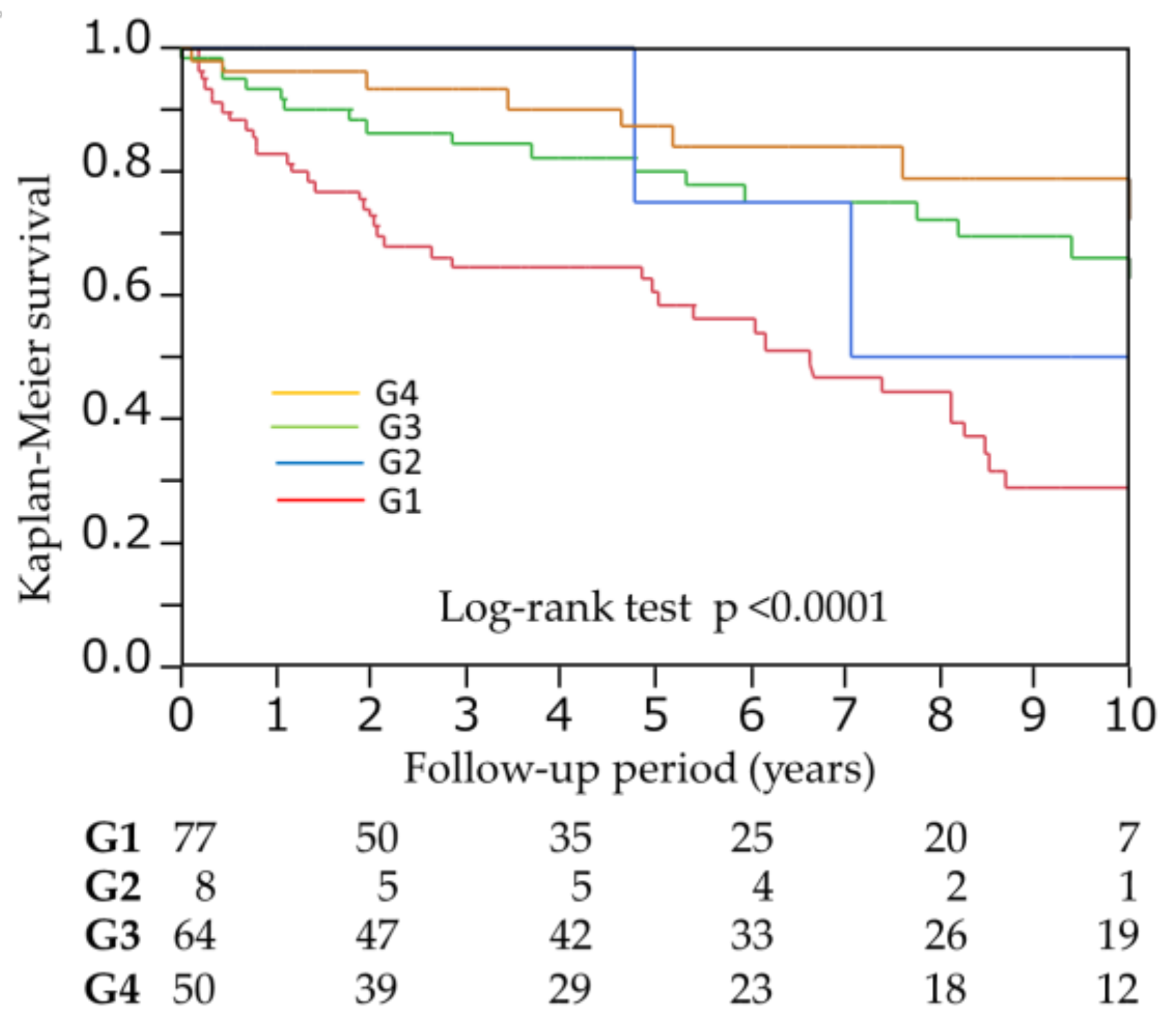
3.2. Abdominal Fat Level and Mortality
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Prospective Studies Collaboration; Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J.; Qizilbash, N.; Collins, R.; Peto, R. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar]
- Berrington de Gonzalez, A.; Hartge, P.; Cerhan, J.R.; Flint, A.J.; Hannan, L.; MacInnis, R.J.; Moore, S.C.; Tobias, G.S.; Anton-Culver, H.; Freeman, L.B.; et al. Body-mass index and mortality among 1.46 million white adults. N. Engl. J. Med. 2010, 363, 2211–2219. [Google Scholar] [CrossRef] [PubMed]
- Abbott, K.C.; Glanton, C.W.; Trespalacios, F.C.; Oliver, D.K.; Ortiz, M.I.; Agodoa, L.Y.; Cruess, D.F.; Kimmel, P.L. Body mass index, dialysis modality, and survival: Analysis of the United States Renal Data System Dialysis Morbidity and Mortality Wave II Study. Kidney Int. 2004, 65, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Ahmadi, S.F.; Streja, E.; Molnar, M.Z.; Flegal, K.M.; Gillen, D.; Kovesdy, C.P.; Kalantar-Zadeh, K. Obesity paradox in end-stage kidney disease patients. Prog. Cardiovasc. Dis. 2014, 56, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Jensen, M.D.; Thomas, R.J.; Squires, R.W.; Allison, T.G.; Korinek, J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to detect obesity in patients with coronary artery disease. Eur. Heart J. 2007, 28, 2087–2093. [Google Scholar] [CrossRef] [PubMed]
- Rankinen, T.; Kim, S.Y.; Pérusse, L.; Després, J.P.; Bouchard, C. The prediction of abdominal visceral fat level from body composition and anthropometry: ROC analysis. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Banerji, M.A.; Buckley, M.C.; Chaiken, R.L.; Gordon, D.; Lebovitz, H.E.; Kral, J.G. Liver fat, serum triglycerides and visceral adipose tissue in insulin-sensitive and insulin-resistant black men with NIDDM. Int. J. Obes. Relat. Metab. Disord. 1995, 19, 846–850. [Google Scholar] [PubMed]
- Després, J.P.; Lemieux, S.; Lamarche, B.; Prud’homme, D.; Moorjani, S.; Brun, L.D.; Gagné, C.; Lupien, P.J. The insulin resistance-dyslipidemic syndrome: Contribution of visceral obesity and therapeutic implications. Int. J. Obes. Relat. Metab. Disord. 1995, 19, S76–S86. [Google Scholar] [PubMed]
- Fox, C.S.; Massaro, J.M.; Hoffmann, U.; Pou, K.M.; Maurovich-Horvat, P.; Liu, C.Y.; Vasan, R.S.; Murabito, J.M.; Meigs, J.B.; Cupples, L.A.; et al. Abdominal visceral and subcutaneous adipose tissue compartments: Association with metabolic risk factors in the Framingham Heart Study. Circulation 2007, 116, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Kuk, J.L.; Katzmarzyk, P.T.; Nichaman, M.Z.; Church, T.S.; Blair, S.N.; Ross, R. Visceral fat is an independent predictor of all-cause mortality in men. Obesity 2006, 14, 336–341. [Google Scholar] [CrossRef] [PubMed]
- McNeely, M.J.; Shofer, J.B.; Leonetti, D.L.; Fujimoto, W.Y.; Boyko, E.J. Associations among visceral fat, all-cause mortality, and obesity-related mortality in Japanese Americans. Diabetes Care 2012, 35, 296–298. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Mire, E.; Bouchard, C. Abdominal obesity and mortality: The Pennington Center Longitudinal Study. Nutr. Diabetes 2012, 2, e42. [Google Scholar] [CrossRef] [PubMed]
- Britton, K.A.; Massaro, J.M.; Murabito, J.M.; Kreger, B.E.; Hoffmann, U.; Fox, C.S. Body fat distribution, incident cardiovascular disease, cancer, and all-cause mortality. J. Am. Coll. Cardiol. 2013, 62, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Shil Hong, E.; Khang, A.R.; Roh, E.; Jeong Ku, E.; An Kim, Y.; Min Kim, K.; Hoon Moon, J.; Hee Choi, S.; Soo Park, K.; Woong Kim, K.; et al. Counterintuitive relationship between visceral fat and all-cause mortality in an elderly Asian population. Obesity 2015, 23, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Koster, A.; Murphy, R.A.; Eiriksdottir, G.; Aspelund, T.; Sigurdsson, S.; Lang, T.F.; Gudnason, V.; Launer, L.J.; Harris, T.B. Fat distribution and mortality: The AGES-Reykjavik Study. Obesity 2015, 23, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Son, J.Y.; Kim, J.M.; Hwang, S.S.; Han, J.S.; Heo, N.J. Body fat distribution is more predictive of all-cause mortality than overall adiposity. Diabetes Obes. Metab. 2018, 20, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Morimoto, S.; Ikenoue, T.; Furumatsu, Y.; Ichihara, A. Visceral fat level is an independent risk factor for cardiovascular mortality in hemodialysis patients. Am. J. Nephrol. 2014, 20, 141–147. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Block, G.; Humphreys, M.H.; Kopple, J.D. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int. 2003, 63, 793–808. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Abbott, K.C.; Salahudeen, A.K.; Kilpatrick, R.D.; Horwich, T.B. Survival advantages of obesity in dialysis patients. Am. J. Clin. Nutr. 2005, 81, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Block, G.; McAllister, C.J.; Humphreys, M.H.; Kopple, J.D. Appetite and inflammation, nutrition, anemia, and clinical outcome in hemodialysis patients. Am. J. Clin. Nutr. 2004, 80, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Lowrie, E.G. Acute-phase inflammatory process contributes to malnutrition, anemia, and possibly other abnormalities in dialysis patients. Am. J. Kidney Dis. 1998, 32, S105–S112. [Google Scholar] [CrossRef]
- Boyko, E.J.; Fujimoto, W.Y.; Leonetti, D.L.; Newell-Morris, L. Visceral adiposity and risk of type 2 diabetes: A prospective study among Japanese Americans. Diabetes Care 2000, 23, 465–471. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, T.; Lamendola, C.; Liu, A.; Abbasi, F. Preferential fat deposition in subcutaneous versus visceral depots is associated with insulin sensitivity. J. Clin. Endocrinol. Metab. 2011, 96, E1756–E1760. [Google Scholar] [CrossRef] [PubMed]
- Nazare, J.A.; Smith, J.D.; Borel, A.L.; Haffner, S.M.; Balkau, B.; Ross, R.; Massien, C.; Alméras, N.; Després, J.P. Ethnic influences on the relations between abdominal subcutaneous and visceral adiposity, liver fat, and cardiometabolic risk profile: The International Study of Prediction of Intra-Abdominal Adiposity and Its Relationship With Cardiometabolic Risk/Intra-Abdominal Adiposity. Am. J. Clin. Nutr. 2012, 96, 714–726. [Google Scholar] [PubMed]
- Samaras, K.; Botelho, N.K.; Chisholm, D.J.; Lord, R.V. Subcutaneous and visceral adipose tissue gene expression of serum adipokines that predict type 2 diabetes. Obesity 2010, 18, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Wagenknecht, L.E.; Langefeld, C.D.; Scherzinger, A.L.; Norris, J.M.; Haffner, S.M.; Saad, M.F.; Bergman, R.N. Insulin sensitivity, insulin secretion, and abdominal fat: The Insulin Resistance Atherosclerosis Study (IRAS) Family Study. Diabetes 2003, 52, 2490–2496. [Google Scholar] [CrossRef] [PubMed]
- Pou, K.M.; Massaro, J.M.; Hoffmann, U.; Vasan, R.S.; Maurovich-Horvat, P.; Larson, M.G.; Keaney, J.F., Jr.; Meigs, J.B.; Lipinska, I.; Kathiresan, S.; et al. Visceral and subcutaneous adipose tissue volumes are cross-sectionally related to markers of inflammation and oxidative stress: The Framingham Heart Study. Circulation 2007, 116, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, A.C.; Qureshi, A.R.; Stenvinkel, P.; Heimbürger, O.; Axelsson, J.; Bárány, P.; Lindholm, B.; Carrero, J.J. Abdominal fat deposition is associated with increased inflammation, protein-energy wasting and worse outcome in patients undergoing haemodialysis. Nephrol. Dial. Transplant. 2010, 25, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Martin, L.; Ghosh, S.; Field, C.J.; Lehner, R.; Baracos, V.E.; Mazurak, V.C. Subcutaneous adiposity is an independent predictor of mortality in cancer patients. Br. J. Cancer 2017, 117, 148. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All Patients (N = 201) | G1 (N = 79) | G2 (N = 8) | G3 (N = 64) | G4 (N = 50) | p Value | |
|---|---|---|---|---|---|---|
| Age (years) | 63.3 ± 13.1 | 64.9 ± 12.1 | 68.9 ± 9.9 | 60.6 ± 15.4 | 63.3 ± 11.2 | 0.14 |
| Male (%) | 72.1 | 77.2 | 87.5 | 60.9 | 76.0 | 0.10 |
| Duration of HD (months) | 1.9 (0.4–27.2) | 2.3 (0.4–23.4) | 1.9 (0.3–5.3) | 1.9 (0.5–28.4) | 1.2 (0.4–29.4) | 0.57 |
| Diabetes (%) | 45.2 | 29.1 | 50.0 | 56.3 | 56.0 | 0.0027 |
| Hypertension (%) | 98.0 | 98.7 | 100 | 96.9 | 98.0 | 0.82 |
| Smoking (%) | 23.9 | 20.3 | 0 | 23.4 | 34.0 | 0.056 |
| Previous CVD (%) | 76.6 | 72.2 | 87.5 | 79.7 | 78.0 | 0.60 |
| BMI (kg/m2) | 21.3 ± 3.4 | 18.7 ± 1.9 | 21.2 ± 1.8 | 21.9 ± 2.5 | 24.7 ± 3.2 | <0.0001 |
| BUN (mg/dL) | 56.0 ± 14.7 | 54.3 ± 16.1 | 52.5 ± 19.7 | 56.4 ± 12.6 | 58.6 ± 14.2 | 0.39 |
| Creatinine (mg/dL) | 8.6 ± 3.0 | 8.26 ± 2.99 | 9.4 ± 4.0 | 8.6 ± 3.0 | 9.0 ± 3.0 | 0.51 |
| Albumin (g/dL) | 3.7 ± 0.4 | 3.7 ± 0.5 | 3.6 ± 0.5 | 3.8 ± 0.4 | 3.7 ± 0.3 | 0.55 |
| Hemoglobin (g/dL) | 10.6 ± 1.5 | 10.5 ± 1.5 | 10.3 ± 1.8 | 10.7 ± 1.6 | 10.6 ± 1.4 | 0.76 |
| T-Cho (mg/dL) | 153 ± 34 | 151 ± 33 | 149 ± 38 | 150 ± 30 | 161 ± 40 | 0.32 |
| Uric acid (mg/dL) | 7.0 ± 1.5 | 6.6 ± 1.4 | 6.4 ± 2.4 | 7.1 ± 1.5 | 7.4 ± 1.5 | 0.020 |
| Ca (mg/dL) | 8.9 ± 0.9 | 8.9 ± 1.0 | 9.3 ± 1.0 | 8.9 ± 0.8 | 8.9 ± 1.0 | 0.76 |
| P (mg/dL) | 5.2 ± 1.4 | 4.8 ± 1.2 | 4.7 ± 1.3 | 5.4 ± 1.3 | 5.7 ± 1.6 | 0.0014 |
| Glucose (mg/dL) | 146 ± 64 | 131 ± 48 | 192 ± 103 | 146 ± 64 | 160 ± 73 | 0.013 |
| CRP (mg/dL) | 0.14 (0.06–0.50) | 0.12 (0.05–0.53) | 0.13 (0.07–0.42) | 0.11 (0.04–0.36) | 0.29 (0.13–0.72) | 0.71 |
| VFA (cm2) | 66.4 ± 49.5 | 32.0 ± 19.0 | 107.2 ± 21.4 | 50.3 ± 17.0 | 135 ± 41.6 | <0.0001 |
| SFA (cm2) | 112.1 ± 64.3 | 59.0 ± 22.7 | 80.3 ± 6.3 | 138.9 ± 52.3 | 166.8 ± 61.7 | <0.0001 |
| VFA | SFA | |||
|---|---|---|---|---|
| Variables | β | p Value | β | p Value |
| Age | - | - | −0.080 | 0.075 |
| Male gender | - | - | −0.292 | <0.0001 |
| Diabetes | 0.115 | 0.031 | 0.117 | 0.0065 |
| Smoking | 0.018 | 0.74 | - | - |
| BMI | 0.631 | <0.0001 | 0.725 | <0.0001 |
| Phosphorus | 0.083 | 0.12 | 0.048 | 0.28 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| cross-classified with VFA and SFA | <0.0001 | 0.012 | ||
| G2 (vs. G1) | 0.46 (0.08–1.51) | 0.23 | 0.30 (0.05–1.09) | 0.070 |
| G3 (vs. G1) | 0.37 (0.21–0.66) | 0.0005 | 0.37 (0.18–0.76) | 0.0065 |
| G4 (vs. G1) | 0.24 (0.10–0.49) | <0.0001 | 0.22 (0.07–0.62) | 0.0035 |
| Variable | C-Index | p Value | NRI | p Value | IDI | p Value |
|---|---|---|---|---|---|---|
| Established risk factors | 0.784 (0.716–0.853) | Reference | Reference | Reference | ||
| +cross-classified with VFA and SFA | 0.817 (0.753–0.881) | 0.075 | 0.612 | 0.00002 | 0.066 | 0.00005 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yajima, T.; Yajima, K.; Takahashi, H.; Yasuda, K. The Impact of Abdominal Fat Levels on All-Cause Mortality Risk in Patients Undergoing Hemodialysis. Nutrients 2018, 10, 480. https://doi.org/10.3390/nu10040480
Yajima T, Yajima K, Takahashi H, Yasuda K. The Impact of Abdominal Fat Levels on All-Cause Mortality Risk in Patients Undergoing Hemodialysis. Nutrients. 2018; 10(4):480. https://doi.org/10.3390/nu10040480
Chicago/Turabian StyleYajima, Takahiro, Kumiko Yajima, Hiroshi Takahashi, and Keigo Yasuda. 2018. "The Impact of Abdominal Fat Levels on All-Cause Mortality Risk in Patients Undergoing Hemodialysis" Nutrients 10, no. 4: 480. https://doi.org/10.3390/nu10040480
APA StyleYajima, T., Yajima, K., Takahashi, H., & Yasuda, K. (2018). The Impact of Abdominal Fat Levels on All-Cause Mortality Risk in Patients Undergoing Hemodialysis. Nutrients, 10(4), 480. https://doi.org/10.3390/nu10040480