Milk-Related Symptoms and Immunoglobulin E Reactivity in Swedish Children from Early Life to Adolescence


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions
2.2.1. Milk-Related Symptoms
2.2.2. Phenotypes Related to Age at Onset and Persistence of Milk-Related Symptoms
Persistent Milk-Related Symptoms
Transient Milk-Related Symptoms
Adolescent Milk-Related Symptoms
2.2.3. Types of Parent-Reported Symptoms at Age 16 Years
Symptoms Reported Specifically in Association with Milk Consumption
- Gastrointestinal: Vomiting, stomach ache/pain, diarrhoea, constipation.
- Skin: Eczema, generalised urticaria, facial oedema.
- Respiratory: Itchy, runny or stuffy nose, breathing difficulties, wheeze, dyspnoea, cough, hoarseness, indistinct speech, swollen feeling in mouth/throat.
- Cardiovascular/Neurological: Unconsciousness, pronounced fatigue.
- Anaphylaxis: Any reaction involving at least two organ systems (gastrointestinal, dermatological, lower respiratory, cardiovascular) per current criteria [16], immediately following milk consumption.
Symptom Reported by Children at Age 16 Years, not Specifically in Association with Milk Consumption
2.2.4. Other Allergy-Related Outcomes in Early Life
Early Life Asthma
Early Life Eczema
Early Life Rhinitis
2.2.5. Clinical Follow-Ups: Assessment of IgE Reactivity
Milk IgE Reactivity
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
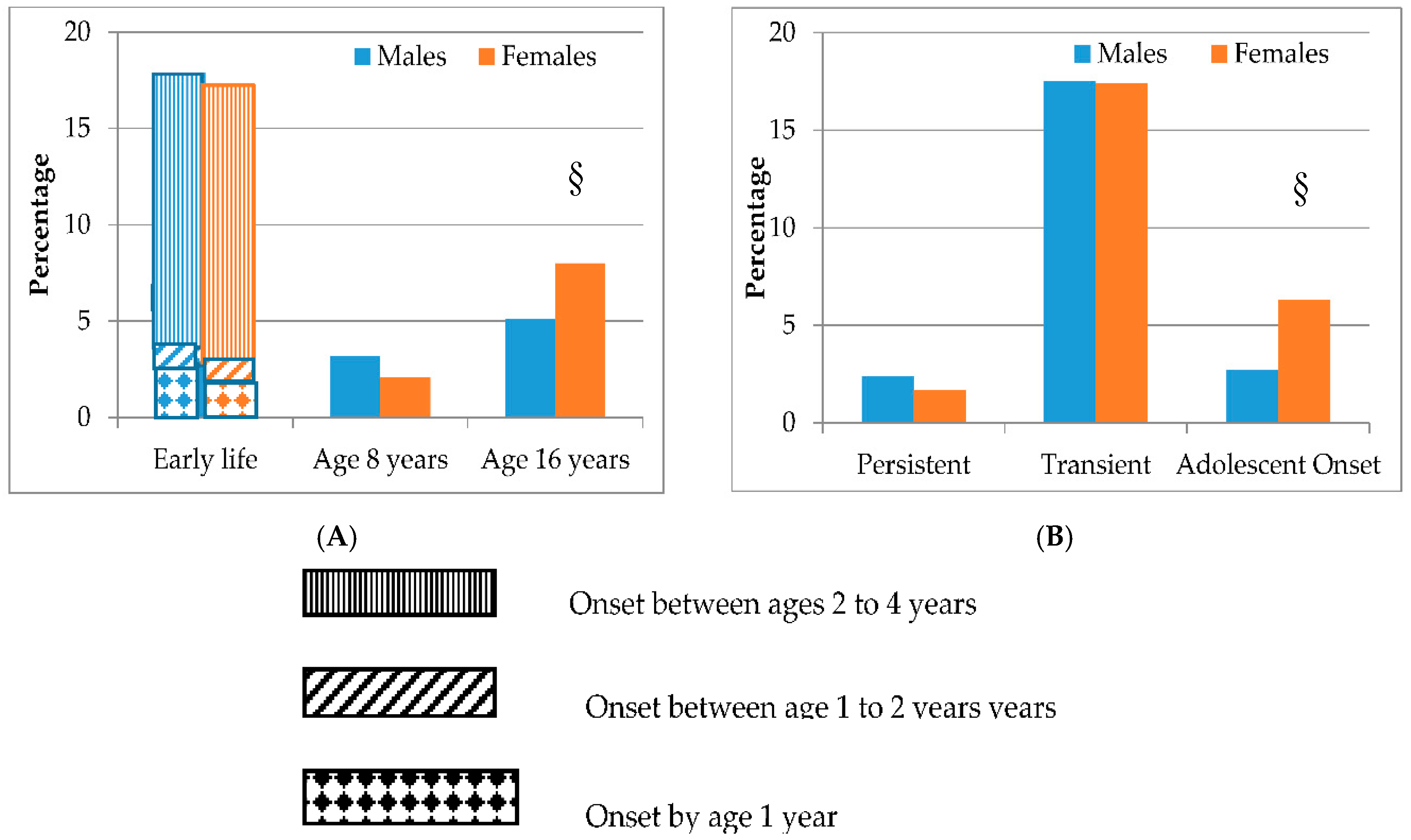
3.2. Prevalence of Milk-Related Symptoms from Birth to Adolescence by Age of Symptom Onset and Sex
3.3. Types of Milk-Related Symptoms and Recurrent Abdominal Pain at Age 16 Years
3.4. IgE Reactivity at Different Ages by Age of Symptom Onset
4. Discussion
4.1. Strengths and Limitations
4.2. Findings in Relation to Previous Studies
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Osterballe, M.; Hansen, T.K.; Mortz, C.G.; Host, A.; Bindslev-Jensen, C. The prevalence of food hypersensitivity in an unselected population of children and adults. Pediatr. Allergy Immunol. 2005, 16, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Host, A. Cow’s milk protein allergy and intolerance in infancy. Some clinical, epidemiological and immunological aspects. Pediatr. Allergy Immunol. 1994, 5, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.A.; Sicherer, S.H.; Vickery, B.P.; Jones, S.M.; Liu, A.H.; Fleischer, D.M.; Henning, A.K.; Mayer, L.; Burks, A.W.; Grishin, A. The natural history of milk allergy in an observational cohort. J. Allergy Clin. Immunol. 2013, 13, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Skripak, J.M.; Matsui, E.C.; Mudd, K.; Wood, R.A. The natural history of IgE-mediated cow’s milk allergy. J. Allergy Clin. Immunol. 2007, 120, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Kavaliūnas, A.; Surkienė, G.; Dubakienė, R.; Stukas, R.; Zagminas, K.; Saulytė, J.; Burney, P.G.; Kummeling, I.; Mills, C. EuroPrevall survey on prevalence and pattern of self-reported adverse reactions to food and food allergies among primary schoolchildren in Vilnius, Lithuania. Medicina 2012, 48, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Grabenhenrich, L.B.; Dölle, S.; Moneret-Vautrin, A.; Köhli, A.; Lange, L.; Spindler, T.; Ruëff, F.; Nemat, K.; Maris, I.; Roumpedaki, E.; et al. Anaphylaxis in children and adolescents: The European Anaphylaxis Registry. J. Allergy Clin. Immunol. 2016, 137, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, A.; Mehlig, K.; Borres, M.P.; Oxelmark, L.; Björkelund, C.; Lissner, L. Monitoring the impact of cow’s milk allergy on children and their families with the FLIP questionnaire—A six-month follow-up study. Pediatr. Allergy Immunol. 2015, 26, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Protudjer, J.L.P.; Jansson, S.A.; Östblom, E.; Heibert Arnlind, M.; Bengtsson, U.; Dahlen, S.-E.; Kallström-Bengtsson, I.; Marklund, B.; Middelveld, R.J.M.; Rentzos, G.; Sundqvist, A.C. Health-related quality of life in children with objectively-diagnosed staple food allergy assessed with a disease-specific questionnaire. Acta Paediatr. 2015, 104, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Protudjer, J.L.P.; Jansson, S.A.; Arnlind Heibert, M.; Bengtsson, U.; Kallström-Bengtsson, I.; Marklund, B.; Middelveld, R.; Rentzos, G.; Sundqvist, A.C.; Åkerström, J.; et al. Household costs associated with objectively-diagnosed allergy to staple foods in children and adolescents. J. Allergy Clin. Immunol. Pract. 2015, 3, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Winberg, A.; West, C.E.; Strinnholm, Å.; Nordström, G.; Hedman, L.; Rönmark, E. Milk allergy is a minor cause of milk avoidance due to perceived hypersensitivity among schoolchildren in Northern Sweden. Acta Paediatr. 2016, 105, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Venkataraman, D.; Erlewyn-Lajeunesse, M.; Kurukulaaratchy, R.J.; Potter, S.; Roberts, G.; Matthews, S.; Arshad, S.H. Prevalence and longitudinal trends of food allergy during childhood and adolescence: Results of the Isle of Wight Birth Cohort study. Clin. Exp. Allergy 2018, 48, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Kull, I.; Almqvist, C.; Lilja, G.; Pershagen, G.; Wickman, M. Breast-feeding reduces the risk of asthma during the first 4 years of life. J. Allergy Clin. Immunol. 2004, 114, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Westman, M.; Lupinek, C.; Bousquet, J.; Andersson, N.; Pahr, S.; Baar, A.; Holmström, M.; Stjärne, P.; Carlsen, K.C.L.; Carlsen, K.H. Early childhood IgE reactivity to pathogenesis-related class 10 proteins predicts allergic rhinitis in adolescence. J. Allergy Clin. Immunol. 2014, 135, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Östblom, E.; Egmar, A.C.; Gardulf, A.; Lilja, G.; Wickman, M. The impact of food hypersensitivity reported in 9-year-old children by their parents on health-related quality of life. Allergy 2008, 63, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Venter, C.; Brown, T.; Shah, N.; Walsh, J.; Fox, A.T. Diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy—A UK primary care practical guide. Clin. Transl. Allergy 2013, 3, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampson, H.A.; Muñoz-Furlong, A.; Campbell, R.L.; Adkinson, N.F., Jr.; Bock, S.A.; Branum, A.; Brown, S.G.; Camargo, C.A.; Cydulka, R.; Galli, S.J.; et al. Second symposium on the definition and management of anaphylaxis: Summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. Ann. Emerg. Med. 2006, 47, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Olen, O.; Neuman, Å.; Koopman, B.; Ludvigsson, J.F.; Ballardini, N.; Westman, M.; Melén, E.; Kull, I.; Simrén, M.; Bergström, A. Allergy-related diseases and recurrent abdominal pain during childhood—A birth cohort study. Aliment. Pharmacol. Ther. 2014, 40, 1349–1358. [Google Scholar] [CrossRef] [PubMed]
- Winberg, A.; Strinnholm, Å.; Hedman, L.; West, C.E.; Perzanowski, M.S.; Rönmark, E. High incidence and remission of reported food hypersensitivity in Swedish children followed from 8 to 12 years of age—A population based cohort study. Clin. Transl. Allergy 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.; Johns, C.B. Food allergy: Epidemiology and natural history. Immunol. Allergy Clin N. Am. 2015, 35, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Östblom, E.; Lilja, G.; Pershagen, G.; van Hage, M.; Wickman, M. Phenotypes of food hypersensitivity and development of allergic diseases during the first 8 years of life. Clin. Exp. Allery 2008, 38, 1325–1332. [Google Scholar] [CrossRef] [PubMed]
- Jeong, K.; Kim, J.; Ahn, K.; Lee, S.Y.; Min, T.K.; Pyun, B.Y.; Kim, Y.H.; Kim, K.W.; Sohn, M.H.; Kim, K.E.; et al. Age-based causes and clinical characteristics of immediate-type food allergy in Korean children. Allergy Asthma Immunol. Res. 2017, 9, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, S.T.; Buyuktiryaki, B.; Sahiner, U.M.; Birben, E.; Tuncer, A.; Yakarisik, S.; Karabulut, E.; Kalayci, O.; Sackesen, C. Factors that predict the clinical reactivity and tolerance in children with cow’s milk allergy. Ann. Allergy Asthma Immunol. 2013, 110, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Dror, D.K.; Allen, L.H. Dairy product intake in children and adolescents in developed countries: Trends, nutritional contribution, and a review of association with health outcomes. Nutr. Rev. 2014, 72, 68–81. [Google Scholar] [CrossRef] [PubMed]
- von Post-Skagegård, M.; Samuelson, G.; Karlström, B.; Mohsen, R.; Berglund, L.; Bratteby, L.E. Changes in food habits in healthy Swedish adolescents during the transition from adolescence to adulthood. Eur. J. Clin. Nutr. 2002, 56, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Hansen, K.L.; Brustad, M.; Johnsen, K. Prevalence of self-reported stomach symptoms after consuming milk among indigenous Sami and non-Sami in Northern- and Mid-Norway—The SAMINOR study. Int. J. Circumpolar Health 2015, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gijsbers, C.F.; Kneepkens, C.M.; Buller, H.A. Lactose and fructose malabsorption in children with recurrent abdominal pain: Results of double-blinded testing. Acta Paediatr. 2012, 101, e441-5. [Google Scholar] [CrossRef] [PubMed]
- Tolone, C.; Pellino, V.; Piccirillo, M.; Letizia, M.; Belfiore, I.; Tolone, S. Recurrent abdominal pain in children: Underlying pathologies in the absence of “alarm” symptoms. Minerva Pediatr. 2017, 69, 239–244. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Original Cohort (N = 4089) | Study Population (N = 2985) | Subpopulation (N = 1634) | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline Characteristics | n | Percent | n | Percent | (95% CI) | n | Percent | (95% CI) |
| Female | 2024/4089 | 49.5 | 1503/2985 | 50.4 | 48.5; 52.2 | 814/1634 | 49.8 | 47.4; 52.3 |
| High socio-economic status | 3323/4018 | 82.7 | 2498/2949 | 84.7 | 83.3; 86.0 | 1389/1616 | 86.0 | 84.2; 87.6 |
| Exclusive breastfeeding * | 3116/3919 | 79.5 | 2366/2929 | 80.8 | 79.3; 82.2 | 1311/1615 | 81.2 | 79.2; 83.1 |
| Immigrant parents | 718/3409 | 21.1 | 609/2979 | 20.4 | 19.0; 21.9 | 325/1631 | 19.9 | 18.0; 21.9 |
| Parental allergy † | 1200/4041 | 29.7 | 910/2961 | 30.7 | 29.1; 32.4 | 527/1621 | 32.5 | 30.2; 34.9 |
| Doctor-diagnosed food allergy ‡ | 325/3299 | 9.0 | 229/2863 | 8.0 | 7.3; 9.1 | 130/1602 | 8.1 | 6.8; 9.6 |
| Other allergy-related outcomes in early life | ||||||||
| Asthma | 474/3629 | 13.1 | 358/2872 | 12.5 | 11.3; 13.7 | 204/1600 | 12.8 | 11.2; 14.5 |
| Eczema | 1272/3700 | 34.4 | 956/2895 | 33.0 | 31.3; 34.8 | 536/1611 | 33.3 | 31.0; 35.6 |
| Rhinitis | 545/3575 | 15.2 | 420/2817 | 14.9 | 13.6; 16.3 | 235/1576 | 14.9 | 13.2; 16.8 |
| No Early Life Milk-Related Symptoms | Early Life Milk-Related Symptoms | p-Value | |||
|---|---|---|---|---|---|
| (N = 2448) | (N = 537) | ||||
| n | Percent | n | Percent | ||
| Baseline characteristics | |||||
| Females | 1237 | 50.5 | 266 | 49.5 | 0.68 |
| High socio-economic status | 2049 | 84.7 | 449 | 84.7 | 0.99 |
| Exclusive breastfeeding for ≥4 months | 1945 | 81.0 | 421 | 79.7 | 0.50 |
| Immigrant parents | 488 | 20.0 | 121 | 22.6 | 0.18 |
| Parental allergy * | 709 | 29.2 | 201 | 37.8 | <0.001 |
| Doctor-diagnosed food allergy by age 4 years | 70 | 3.0 | 159 | 30.3 | <0.001 |
| Other allergy-related outcomes in early life | |||||
| Asthma | 268 | 11.4 | 90 | 17.2 | <0.001 |
| Eczema | 668 | 28.2 | 288 | 54.6 | <0.001 |
| Rhinitis | 266 | 11.6 | 154 | 29.7 | <0.001 |
| Persistent | Transient | Adolescent-Onset | ||||
|---|---|---|---|---|---|---|
| N = 62 | N = 520 | N = 134 | ||||
| n | Percent | n | Percent | n | Percent | |
| Baseline characteristics | ||||||
| Females | 26 | 41.9 | 261 | 50.2 | 94 | 70.2 |
| High socio-economic status | 47 | 75.8 | 438 | 85.4 | 103 | 78.6 |
| Exclusive breastfeeding for ≥4 months | 51 | 83.6 | 401 | 78.5 | 107 | 83.0 |
| Immigrant parents | 16 | 25.8 | 118 | 22.7 | 39 | 29.1 |
| Parental allergy * | 30 | 49.2 | 191 | 37.0 | 41 | 30.8 |
| Doctor-diagnosed food allergy by age 4 years | 24 | 40.0 | 141 | 27.8 | 9 | 7.3 |
| Other allergy-related outcomes in early life | ||||||
| Asthma | 13 | 21.7 | 80 | 15.8 | 18 | 14.3 |
| Eczema | 32 | 53.3 | 276 | 54.1 | 43 | 33.6 |
| Rhinitis | 25 | 41.7 | 140 | 27.9 | 19 | 15.2 |
| Persistent | Adolescent-Onset | p-Value | |||
|---|---|---|---|---|---|
| (N = 62) | (N = 134) | ||||
| n | % | n | % | ||
| Gastrointestinal † | 46 | 74.2 | 110 | 82.1 | 0.10 |
| Skin * | 15 | 24.2 | 4 | 3.0 | <0.001 |
| Respiratory ‡ | 1 | 1.6 | 2 | 1.5 | 0.68 |
| Cardiovascular/Neurological § | 1 | 1.6 | 1 | 0.7 | 0.53 |
| Anaphylaxis | 3 | 4.8 | 0 | 0.0 | 0.03 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Protudjer, J.L.P.; Olén, O.; Vetander, M.; Kull, I.; Melén, E.; Van Hage, M.; Wickman, M.; Bergström, A. Milk-Related Symptoms and Immunoglobulin E Reactivity in Swedish Children from Early Life to Adolescence. Nutrients 2018, 10, 651. https://doi.org/10.3390/nu10050651
Protudjer JLP, Olén O, Vetander M, Kull I, Melén E, Van Hage M, Wickman M, Bergström A. Milk-Related Symptoms and Immunoglobulin E Reactivity in Swedish Children from Early Life to Adolescence. Nutrients. 2018; 10(5):651. https://doi.org/10.3390/nu10050651
Chicago/Turabian StyleProtudjer, Jennifer L. P., Ola Olén, Mirja Vetander, Inger Kull, Erik Melén, Marianne Van Hage, Magnus Wickman, and Anna Bergström. 2018. "Milk-Related Symptoms and Immunoglobulin E Reactivity in Swedish Children from Early Life to Adolescence" Nutrients 10, no. 5: 651. https://doi.org/10.3390/nu10050651
APA StyleProtudjer, J. L. P., Olén, O., Vetander, M., Kull, I., Melén, E., Van Hage, M., Wickman, M., & Bergström, A. (2018). Milk-Related Symptoms and Immunoglobulin E Reactivity in Swedish Children from Early Life to Adolescence. Nutrients, 10(5), 651. https://doi.org/10.3390/nu10050651