What Is the Role of Nutritional Supplements in Support of Total Hip Replacement and Total Knee Replacement Surgeries? A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria, Information Sources
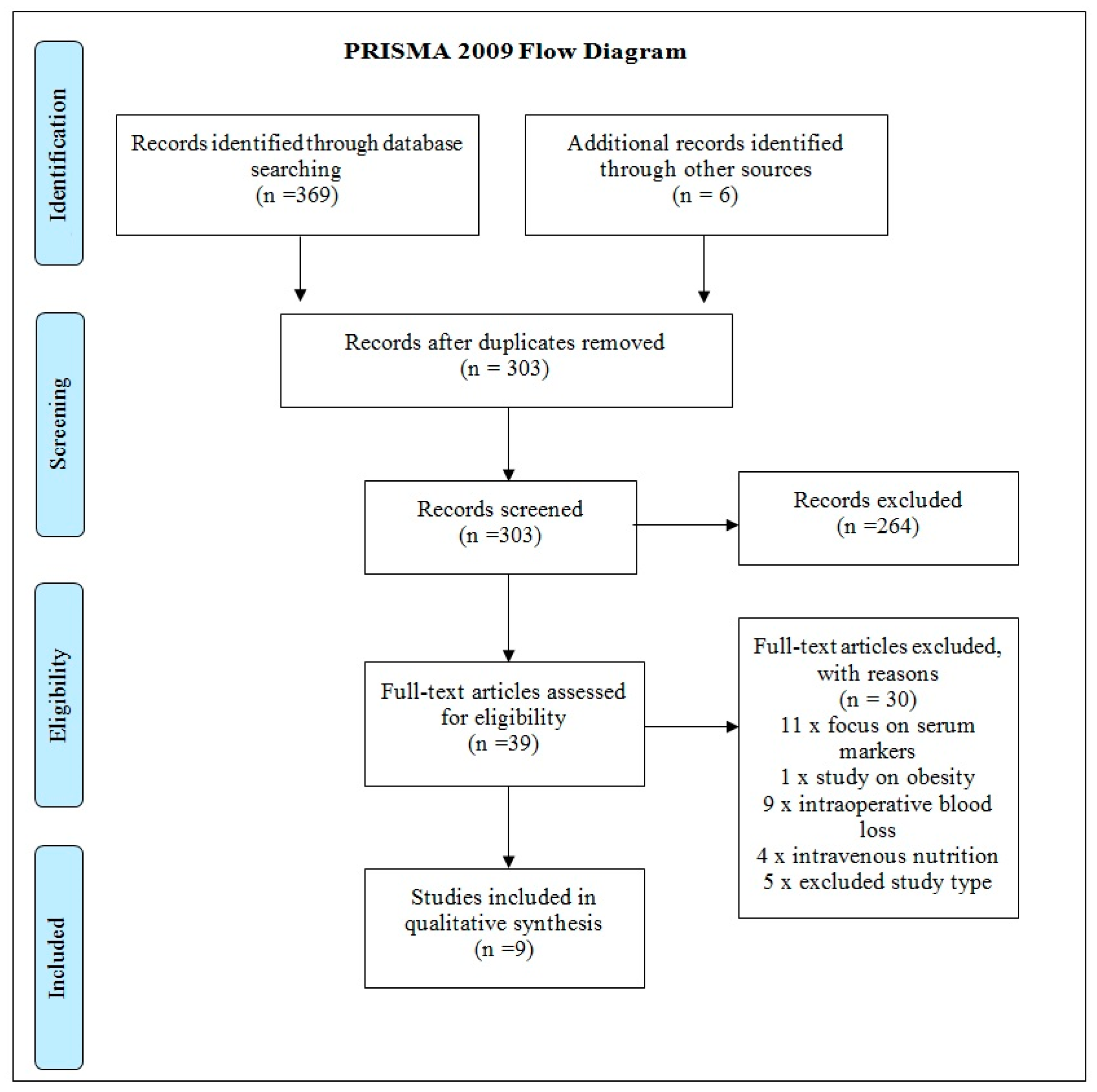
2.2. Search Strategy and Study Selection
2.3. Quality Assessment
3. Results
4. Discussion
4.1. Carbohydrate Drinks
4.2. Amino Acid Supplementation
4.3. Beta-Hydroxy Beta-Methylbutyrate, l-Arginine, and l-Glutamine
5. Future Work and Directions
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rosenberg, I.H.; Miller, J.W. Nutritional factors in physical and cognitive functions of elderly people. Am. J. Clin. Nutr. 1992, 55, 1237S–1243S. [Google Scholar] [CrossRef] [PubMed]
- Molfino, A.; Gioia, G.; Fanelli, F.P.; Muscaritoli, M. The role of dietary omega-3 fatty acids supplementation in older adults. Nutrients 2014, 6, 4058–4072. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Ferreira, V. Prehabilitation: A new era of integration between geriatricians, anaesthesiologists, and exercise therapists. Aging Clin. Exp. Res. 2018, 30, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Braga, M. The 2015 ESPEN Arvid Wretlind lecture. Evolving concepts on perioperative metabolism and support. Clin. Nutr. 2016, 35, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Dardai, E.; Allison, S.P. Basics in Clinical Nutrition: Perioperative Nutrition. Clin. Nutr. e-SPEN 2010, 5, e93–e96. [Google Scholar] [CrossRef]
- Paddon-Jones, D.; Coss-Bu, J.A.; Morris, C.R.; Phillips, S.M.; Wernerman, J. Variation in protein origin and utilisation: Research and clinical application. Nutr. Clin. Pract. 2017, 32, 48S–57S. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.M. Current concepts and unresolved questions in dietary protein requirements and supplements in adults. Front. Nutr. 2017, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.M. Nutritional supplements in support of resistance exercise to counter age-related sarcopenia. Adv. Nutr. 2015, 6, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, H.C.; Volpi, E. Role of protein and amino acids in the pathophysiology and treatment of sarcopenia. J. Am. Coll. Nutr. 2011, 24, 140S–145S. [Google Scholar] [CrossRef]
- Brady, M.C.; Kinn, S.; Stuart, P. Preoperative fasting for adults to prevent perioperative complications. Cochrane Database Syst. Rev. 2003. [Google Scholar] [CrossRef] [PubMed]
- Bilku, D.K.; Dennison, A.R.; Hall, T.C.; Metcalfe, M.S.; Garcea, G. Role of preoperative carbohydrate loading: A systematic review. Ann. R. Coll. Surg. Engl. 2014, 96, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Soreide, E. Preoperative fasting. Br. J. Surg. 2003, 90, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Lassen, K.; Soop, M.; Nygren, J.; Cox, P.B.; Hendry, P.O.; Spies, C.; von Meyenfeldt, M.F.; Fearon, K.C.; Revhaug, A.; Norderval, S.; et al. Consensus review of optimal perioperative care in colorectal surgery. Enhanced Recovery After Surgery (ERAS) Group Recommendations. JAMA Surg. 2009, 144, 961–969. [Google Scholar]
- Svanfeldt, M.; Thorell, A.; Hausel, J.; Soop, M.; Rooyackers, O.; Nygren, J.; Ljungqvist, O. Randomized clinical trial of the effect of preoperative oral carbohydrate treatment on postoperative whole-body protein and glucose kinetics. Br. J. Surg. 2007, 94, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Nygren, J.; Thorell, A. Modulation of post-operative insulin resistance by pre-operative carbohydrate loading. Proc. Nutr. Soc. 2002, 61, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Soop, M.; Hedstrom, M. Why metabolism matters in elective orthopaedic surgery. A review. Acta Orthop. 2007, 78, 610–615. [Google Scholar] [CrossRef] [PubMed]
- National Joint Registry. National Joint Registry 14th Annual Report. 2017. Available online: http://www.njrcentre.org.uk/ (accessed on 2 March 2018).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Moher, D.; Schulz, K.F.; Sterne, J.A.C. Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyer, H.C.; Strycker, L.A.; Senesac, H.A.; Hocker, A.D.; Smolkowski, K.; Shah, S.N.; Jewett, B.A. Essential amino acid supplementation in patients following total knee arthroplasty. J. Clin. Investig. 2013, 123, 4654–4666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishizaki, K.; Ikegami, H.; Tanaka, Y.; Imai, R.; Matsumura, H. Effects of supplementation with a combination of β-hydroxy-β-methyl butyrate, L-arginine, and L-glutamine on postoperative recovery of quadriceps muscle strength after total knee arthroplasty. Asia Pac. J. Clin. Nutr. 2015, 24, 412–420. [Google Scholar] [PubMed]
- Alito, M.A.; de Aguilar-Nascimento, J.E. Multimodal perioperative care plus immunonutrition versus traditional care in total hip arthroplasty: A randomized pilot study. Nutr. J. 2016, 15, 34. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, A.; Al-Ani, N.A.; Brismar, K.; Hedstrőm, K. A carbohydrate-rich drink shortly before surgery affected IGF-1 bioavailability after a total hip replacement. A double-blind placebo controlled study on 29 patients. Aging Clin. Exp. Res. 2008, 21, 97–101. [Google Scholar] [CrossRef]
- Hartsen, A.; Hjartarson, H.; Toksvig-Larsen, S. Total hip arthroplasty and perioperative oral carbohydrate treatment: A randomised, double blind, controlled trial. Eur. J. Anaesthesiol. 2012, 29, 259–260. [Google Scholar]
- Ljunggren, S.; Hahn, R.G. Oral nutrition or water loading before hip replacement surgery; a randomized clinical trial. Trials 2012, 13, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nygren, J.; Soop, M.; Thorell, A.; Nair, K.S.; Ljungqvist, O. Preoperative oral carbohydrates and postoperative insulin resistance. Clin. Nutr. 1999, 18, 117–120. [Google Scholar] [CrossRef]
- Soop, M.; Nygren, J.; Myrenfors, P.; Thorell, A.; Ljungqvist, O. Preoperative oral carbohydrate treatment attenuates immediate postoperative insulin resistance. Am. J. Physiol. Endocrinol. Metab. 2001, 280, E576–E583. [Google Scholar] [CrossRef] [PubMed]
- Soop, M.; Nygren, J.; Thorell, A.; Weidenhielm, L.; Lungberg, M.; Hammargvist, F.; Ljungqvist, O. Preoperative oral carbohydrate treatment attenuates endogenous glucose release 3 days after surgery. Clin. Nutr. 2004, 23, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, D.J.; Hossian, T.; Hill, D.S.; Phillips, B.E.; Crossland, H.; Williams, J.; Loughna, P.; Churchward-Venne, T.A.; Breen, L.; Phillips, S.M.; et al. Effects of leucine and its metabolite β-hydroxy-β-methylbutyrate on human skeletal muscle protein metabolism. J. Physiol. 2013, 591, 2911–2923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Husted, H.; Lunn, T.H.; Troelsen, A.; Gaarn-Larsen, L.; Kristensen, B.B.; Kehlet, H. Why still in hospital after fast-track hip and knee arthroplasty? Acta Orthop. 2011, 82, 679–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehlet, H. Fast-track hip and knee arthroplasty. Lancet 2013, 381, 1600–1602. [Google Scholar] [CrossRef]
- Gaudilliere, B.; Fragiadakis, G.K.; Bruggner, R.V.; Nicolau, M.; Finck, R.; Tingle, M.; Silva, J.; Ganio, E.A.; Yeh, C.G.; et al. Clinical recovery from surgery correlates with single-cell immune signatures. Sci. Transl. Med. 2014, 6, 255ra131. [Google Scholar] [CrossRef] [PubMed]
- Bamman, M.M.; Ferrando, A.A.; Evans, R.P.; Stec, M.J.; Kelly, N.A.; Gruenwald, J.M.; Corrick, K.L.; Trump, J.R.; Singh, J.A. Muscle inflammation susceptibility: A prognostic index of recovery potential after hip arthroplasty? Am. J. Physiol. Endocrimol. Metab. 2015, 308, E670–E679. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Omega-3 Fatty Acids and Inflammatory Processes. Nutrients 2010, 2, 355–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burd, N.A.; Gorissen, S.H.; van Loon, L.J.C. Anabolic resistance of muscle protein synthesis with aging. Exerc. Sport Sci. Rev. 2013, 41, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Irving, B.A.; Robinson, M.M.; Nair, K.S. Age effect on myocellular remodelling: Response to exercise and nutrition in humans. Ageing Res. Rev. 2012, 11, 374–389. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.E.; Von Allmen, M.T.; Devries, M.C.; Phillips, S.M. Muscle disuse as a pivotal problem in sarcopenia-related muscle loss and dysfunction. J. Frailty Aging 2016, 5, 33–41. [Google Scholar] [PubMed]
- Wall, B.T.; Morton, J.P.; Van Loon, L.J.C. Strategies to maintain skeletal muscle mass in the injured athlete: Nutritional considerations and exercise mimetics. Eur. J. Sport Sci. 2015, 15, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Greig, C.A.; Gray, C.; Rankin, D.; Young, A.; Mann, V.; Noble, B.; Atherton, P.J. Blunting of adaptive responses to resistance exercise training in women over 75y. Exp. Gerontol. 2011, 46, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Scheede-Bergdahl, C. Prehabilitation to enhance perioperative care. Anaesthesiol. Clin. 2015, 33, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Tipton, K.D.; Wolfe, R.R. Exercise, protein metabolism, and muscle growth. Int. J. Sport Nutr. Exerc. Metab. 2001, 11, 109–132. [Google Scholar] [CrossRef] [PubMed]
- Finger, D.; Goltz, F.R.; Umpierre, D.; Meyer, E.; Rosa, L.H.; Schneider, C.D. Effects of protein supplementation in older adults undergoing resistance training: A systematic review and meta-analysis. Sports Med. 2015, 45, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.E.; Snijders, T.; Zulyniak, M.; Kumbhare, D.; Parise, G.; Chabowski, A.; Phillips, S.M. A whey protein-based multi-ingredient nutritional supplement stimulates gains in lean body mass and strength in healthy older men: A randomized controlled trial. PLoS ONE 2017, 12, e0181387. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.E.; Snijders, T.; Zulyniak, M.A. A multi-ingredient nutritional supplement enhances exercise training-related reductions in markers of systemic inflammation in healthy older men. Appl. Physiol. Nutr. Metab. 2017, 43, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Pennings, B.; Koopman, R.; Beelen, M.; Senden, J.M.; Saris, W.H. Exercising before protein intake allows for greater use of dietary protein-derived amino acids for de novo protein synthesis in both young and elderly men. Am. J. Clin. Nutr. 2011, 93, 322–331. [Google Scholar] [CrossRef] [PubMed]
- Burd, N.A.; West, D.W.D.; Moore, D.R.; Atherton, P.J.; Staples, A.W.; Prior, T.; Tang, J.E.; Rennie, M.J.; Baker, S.K.; et al. Enhanced amino acid sensitivity of myofibrillar protein synthesis persists for up to 24 h after resistance exercise in young men. J. Nutr. 2011, 141, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Pereira, S.L.; Hays, N.P.; Oliver, J.S.; Edens, N.K.; Evans, C.M.; Wolfe, R.R. Effect of β-hydroxy-β-methylbutyrate (HMB) on lean body mass during 10 days of bed rest in older adults. Clin. Nutr. 2013, 32, 704–712. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Population | |
| Total hip replacement patients | Studies on animals |
| Total knee replacement patients | |
| Intervention | |
| Pre-operative or post-operative oral nutrition | Intravenous nutritional supplementation Assessments of intraoperative blood loss |
| Iron supplementation | |
| Outcome Measure | |
| Length of stay | |
| Post-operative complications | |
| Insulin resistance | |
| Pain | |
| Functionality | |
| C-reactive protein | |
| Vitamin D | |
| Methodology | |
| Randomized clinical trials | Review articles |
| Pilot randomized clinical trials | Case studies |
| Cross-sectional studies | |
| Historical studies | |
| Non-randomized clinical trials | |
| Publication | |
| Published in English | Unpublished studies |
| Access to full text | Study protocols |
| Search Strategy | ||
|---|---|---|
| Operation | Timing | Topic |
| (“Arthroplasty, Replacement, Hip”) OR (“Hip Prosthesis”) (Hip*) (arthroplast* OR prosthes* OR replace*) OR THA OR THR OR (“Arthroplasty, Replacement, Knee”) OR (“Knee Prosthesis”) OR (Knee*) (arthroplast* OR prosthes* OR replace*) TKA OR TKR | Preoperative OR pre-operative OR pre operative OR (“Preoperative Period”) Postoperative OR post-operative OR post operative OR (“Postoperative Period”) | Nutriti* OR (MH “Dietary Carbohydrates”) OR Carbohydrat* OR (MH “Diet+”) OR Protein OR amino acids OR “branched chain amino acid” OR Glutamine OR Omega-3 fatty acids OR Docosahexaenoic acid OR DHA OR Eicosapentenoic acid OR EPA OR Iron OR Vitamin C OR Ascorbic acid OR Vitamin D OR B vitamin* OR Selenium OR Zinc OR Calcium |
| Study | Design and Sample Size | Patient, Population. or Problem | Intervention, Prognostic Factor or Exposure | Comparison or Intervention | Outcomes | Main Findings |
|---|---|---|---|---|---|---|
| Dreyer et al., 2013 [20] | RCT n = 28 | TKR patients | 20 g of essential amino acids (EAA) twice daily between meals for 1 week before and 2 weeks after TKR. | Placebo supplementation (20 g (100% alanine) | Muscle atrophy, muscle strength, and functional mobility. | The placebo group exhibited greater quadriceps muscle atrophy (−14.3 ± 3.6% change) from baseline to 2 weeks post-surgery. EAAs also attenuated atrophy in the non-operated quadriceps and in the hamstring and adductor muscles of both extremities. The EAA group demonstrated better functional mobility at 2 and 6 weeks post-operatively (all p < 0.05). |
| Nishizaki et al., 2015 [21] | RCT n = 23 | TKR patients | Beta-hydroxy beta-methylbutyrate (HMB; 2400 mg), l-arginine (Arg; 14,000 mg) and l-glutamine (Gln; 14,000 mg) (HMB/Arg/Gln) (158 kcal of energy) for 5 days before the surgery and for 28 days after the surgery. Patients fasted on the day of surgery. | Control food (orange juice, 226 kcal of energy and 280 mg of protein) | Body weight, bilateral knee extension strength, rectus femoris cross-sectional area. | Maximal quadriceps strength was 1.1 ± 0.62 Nm/kg pre-surgery and 0.7 ± 0.9 Nm/kg 14 days post-surgery in the control group (p = 0.02). In the HMB/Arg/Gln group, maximum quadriceps strength was 1.1 ± 0.3 Nm/kg before surgery and 0.9 ± 0.4 Nm/kg 14 days after surgery. The muscle loss was significant in the control group, but not in the intervention group. |
| Alito and de Aguilar-Nascimento 2016 [22] | Pilot RCT n = 32 | THR patients | 6 h pre-operative fasting for solids, an oral drink (200 mL of 12.5% maltodextrin) up to 2 h before induction of anesthesia, restricted intravenous fluids (only 1000 mL of cystalloid fluid after surgery), and pre-operative immune nutrition (600 mL/day of Impact—Nestle, Brazil) for 5 days prior to surgery. | Control group (traditional care, 6–8 h of pre-operative fasting, intravenous hydration until the 1st post-operative day and no pre-operative immune supplementation) | Length of stay, C-reactive protein. | Median length of stay (LOS) was 3 (2–5) days in the intervention group and 6 (3–8) days in controls (p < 0.01). Post-operative C-reactive protein was higher in the control group (p < 0.001). |
| Aronsson et al., 2008 [23] | Pilot RCT n = 29 | THR patients | Carbohydrate-rich drink (an iso-osmolar carbohydrate-rich solution: 12.5 g carbohydrate/100 mL, pH 5.0) pre-operatively. | Placebo drink (flavored water) | IGF-1 and IGFBP-1 were determined in serum by RIA. Body composition was determined by dual energy X-ray absorptiometry (performed the day before surgery and at 6–8 weeks after surgery) | Compared to placebo, the authors found a relative increase in IGF-1 bioavailability post-operatively after a carbohydrate-rich drink given shortly before surgery. There were no significant differences in the changes in fat or lean body mass between groups (p = 0.08). |
| Hartsen et al., 2012 [24] | RCT n = 60 | ASA physical status I–III patients scheduled for THR | 400 mL of an oral 12.5% carbohydrate solution | Placebo drink (flavored water) | Visual analog scales were used to score six discomfort parameters. | Immediately after surgery, carbohydrate-treated patients were less hungry (median scores 9.5 vs. 22 mm) and experienced less nausea (0 vs. 1.5 mm) (p < 0.05). |
| Ljunggren and Hahn 2012 [25] | RCT n = 57 | THR patients | Tap Water: 800 mL by mouth, 2 h before entering the operating room OR Nutrition: an iso-osmolar carbohydrate drink (50 kcal/100 mL) 800 mL in the evening before the surgery (day 0), and 400 mL 2 h before entering the operating room (day 1). | Fasting (no food or water from midnight before the surgery) | Intravenous glucose tolerance, physical stress, muscle catabolism, body fluid volumes, complications, wellbeing, and insulin sensitivity. | Pre-operative ingestion of tap water or a nutritional drink had no statistically significant effect on glucose clearance, insulin sensitivity, post-operative complications, or wellbeing in patients undergoing THR. |
| Nygren et al., 1999 [26] | RCT n = 16 | THR patients | Pre-operative oral iso-osmolar carbohydrate administration (800 mL 12.5% carbohydrates), the evening before the operation. Another 400 mL of the same beverage was allowed 2 h after midnight, taken no later than 2 h before the initiation of anesthesia. | Placebo drink | Insulin sensitivity | Patients given a carbohydrate drink shortly before elective surgery displayed less reduced insulin sensitivity (−16% (not significant)) after surgery compared to patients undergoing surgery after an overnight fast (37% p < 0.05 vs. pre-operatively). Insulin sensitivity and whole-body glucose disposal were reduced in both groups. |
| Soop et al., 2001 [27] | RCT n = 15 | THR patients | Carbohydrate-rich drink (12.5 g/100 mL carbohydrate, 12% monosaccharides, 12% disaccharides, 76% polysaacharides, 285 mosmol/kg), 800 mL between 7 p.m. and 12:00 a.m. on the evening before surgery and 400 mL on the morning of surgery. | Placebo drink (acesulfame-K, 0.64 g/100 mL citrate, 107 mosmol/kg) | Glucose, lactate and insulin concentrations, glycerol, NEFA, glucoregulatory hormone concentrations, glucose kinetics, and substrate utilization. | Whole-body insulin sensitivity decreased by 18% in the intervention group vs. 43% in the placebo group. This was attributable to a less reduced glucose disposal in peripheral tissues and increased glucose oxidation rates. |
| Soop et al., 2004 [28] | RCT n = 14 | THR patients | Carbohydrate rich drink (12.5 g /100 mL carbohydrate, 12% monosaccharides, 12% disaccharides, 76% polysaacharides, 285 mosm/kg, 800 mL between 7 p.m. and 12:00 a.m. on the evening before surgery and 400 mL on the morning of surgery. | Placebo drink | Glucose kinetics, substrate utilization, nitrogen balance, ambulation time, food consumption, and LOS. | Whole-body glucose disposal and nitrogen balance were similar between groups. Pre-operative carbohydrate treatment significantly attenuated post-operative endogenous glucose release (0.69 (0.07) vs. 1.21 (0.13) mg kg−1, (p < 0.01), compared to the placebo group. Whole-body glucose disposal and nitrogen balance were similar between groups. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burgess, L.C.; Phillips, S.M.; Wainwright, T.W. What Is the Role of Nutritional Supplements in Support of Total Hip Replacement and Total Knee Replacement Surgeries? A Systematic Review. Nutrients 2018, 10, 820. https://doi.org/10.3390/nu10070820
Burgess LC, Phillips SM, Wainwright TW. What Is the Role of Nutritional Supplements in Support of Total Hip Replacement and Total Knee Replacement Surgeries? A Systematic Review. Nutrients. 2018; 10(7):820. https://doi.org/10.3390/nu10070820
Chicago/Turabian StyleBurgess, Louise C., Stuart M. Phillips, and Thomas W. Wainwright. 2018. "What Is the Role of Nutritional Supplements in Support of Total Hip Replacement and Total Knee Replacement Surgeries? A Systematic Review" Nutrients 10, no. 7: 820. https://doi.org/10.3390/nu10070820
APA StyleBurgess, L. C., Phillips, S. M., & Wainwright, T. W. (2018). What Is the Role of Nutritional Supplements in Support of Total Hip Replacement and Total Knee Replacement Surgeries? A Systematic Review. Nutrients, 10(7), 820. https://doi.org/10.3390/nu10070820