Effect of Heat-Killed Lactobacillus paracasei KW3110 Ingestion on Ocular Disorders Caused by Visual Display Terminal (VDT) Loads: A Randomized, Double-Blind, Placebo-Controlled Parallel-Group Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. In Vitro Experiments
2.1.1. Preparation of Human PBMC-Derived M2 Macrophages and Culture Media
2.1.2. Enzyme-Linked Immunosorbent Assay (ELISA)
2.1.3. Cell Culture
2.1.4. Cell Death Analyses after Blue Light Exposure
2.1.5. Cellular Metabolic Activity Assay
2.2. Clinical Study
2.2.1. Ethics
2.2.2. Subjects
2.2.3. L. paracasei KW3110-Containing Capsules and Placebo Capsules
2.2.4. Study Design
2.2.5. Primary Outcome Measures
2.2.6. Secondary Outcome Measures
2.2.7. Subgroup Analysis
2.2.8. Statistical Analysis
3. Results
3.1. In Vitro Experiments
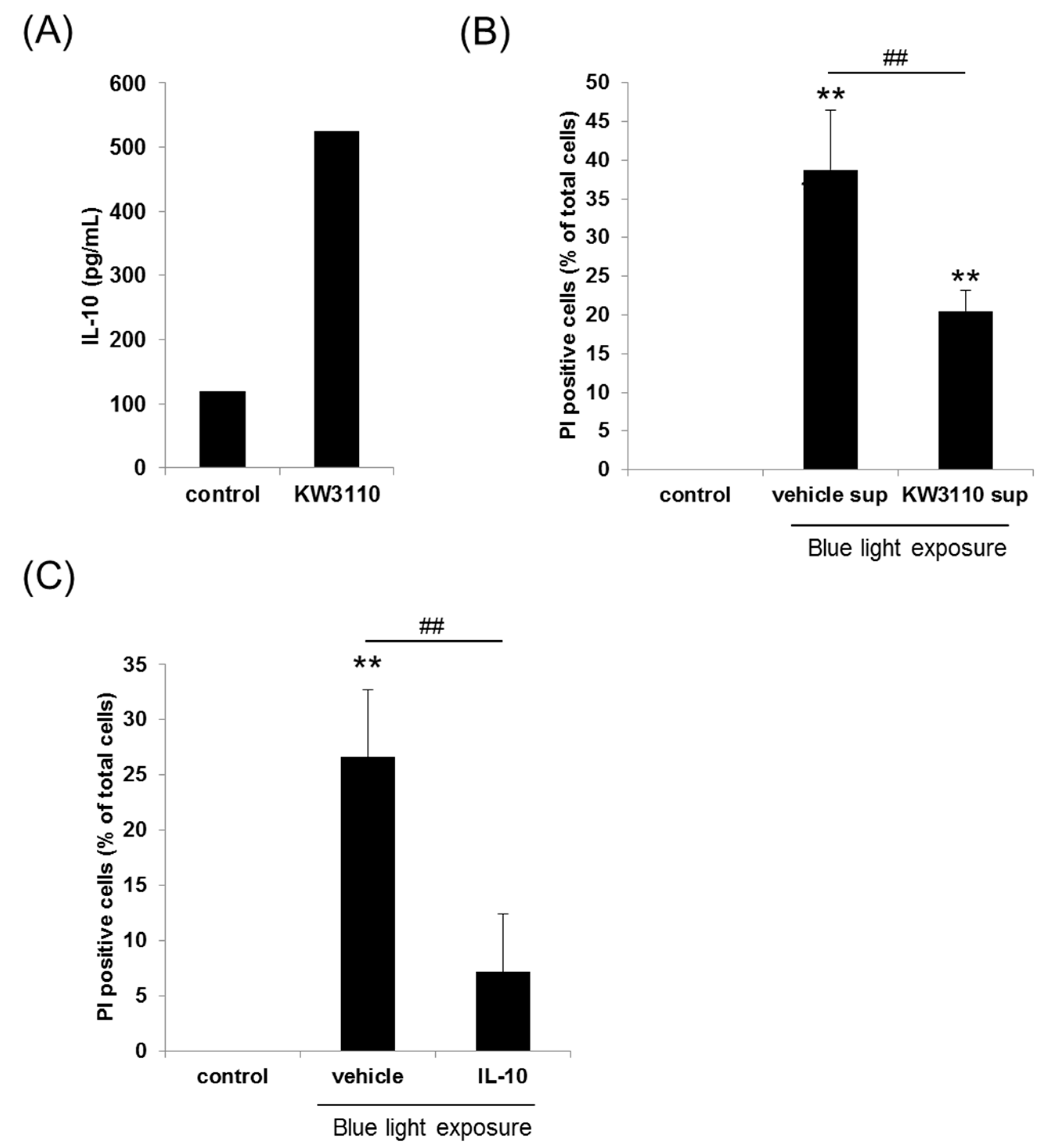
3.1.1. Effects of L. paracasei KW3110 on Human PBMC-Derived M2 Macrophage Activation
3.1.2. Effects of L. paracasei KW3110 on Blue Light-Induced Human Retinal Cell Death
3.2. Clinical Study
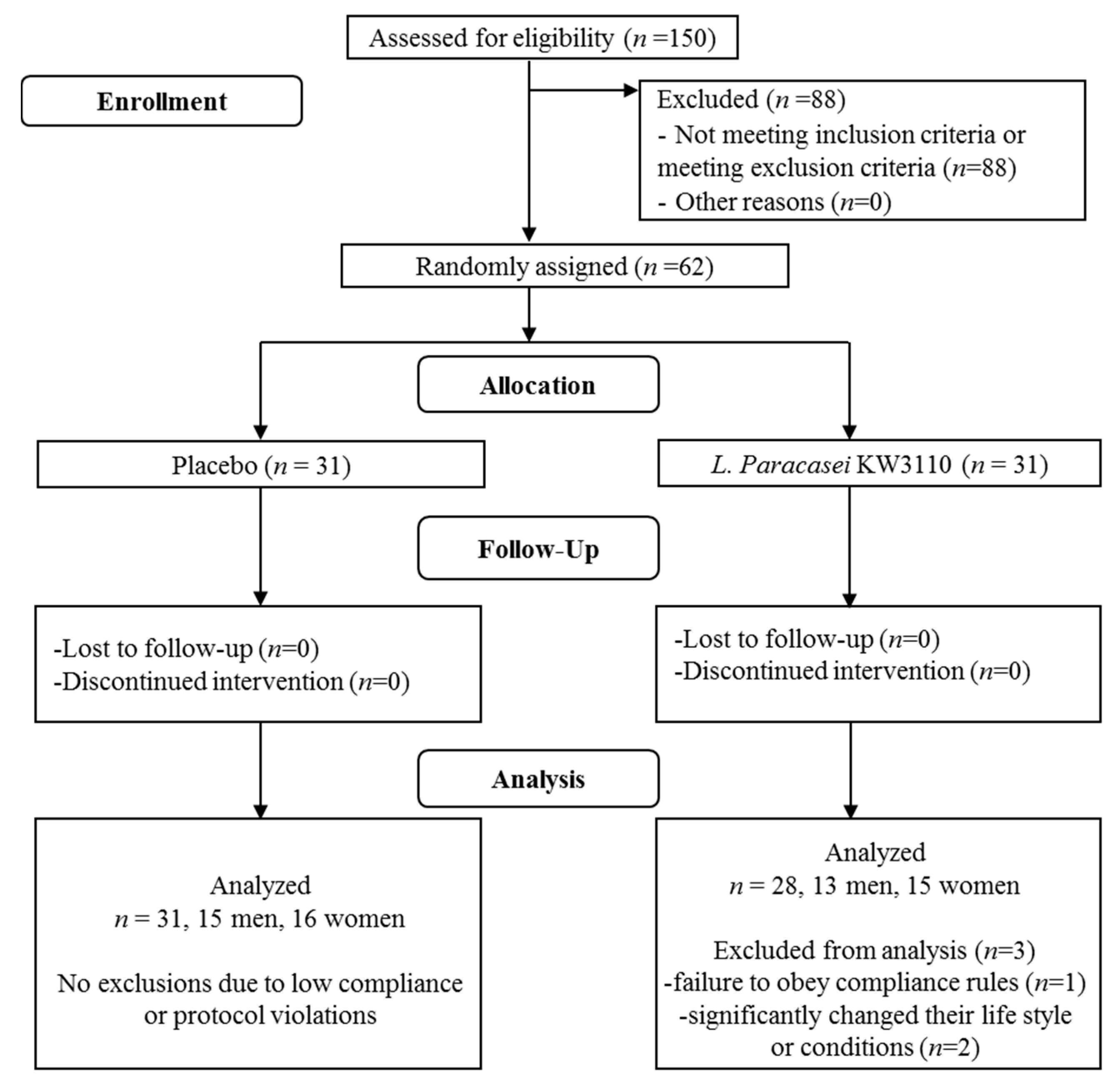
3.2.1. Background Information and Baseline Characteristics of the Subjects
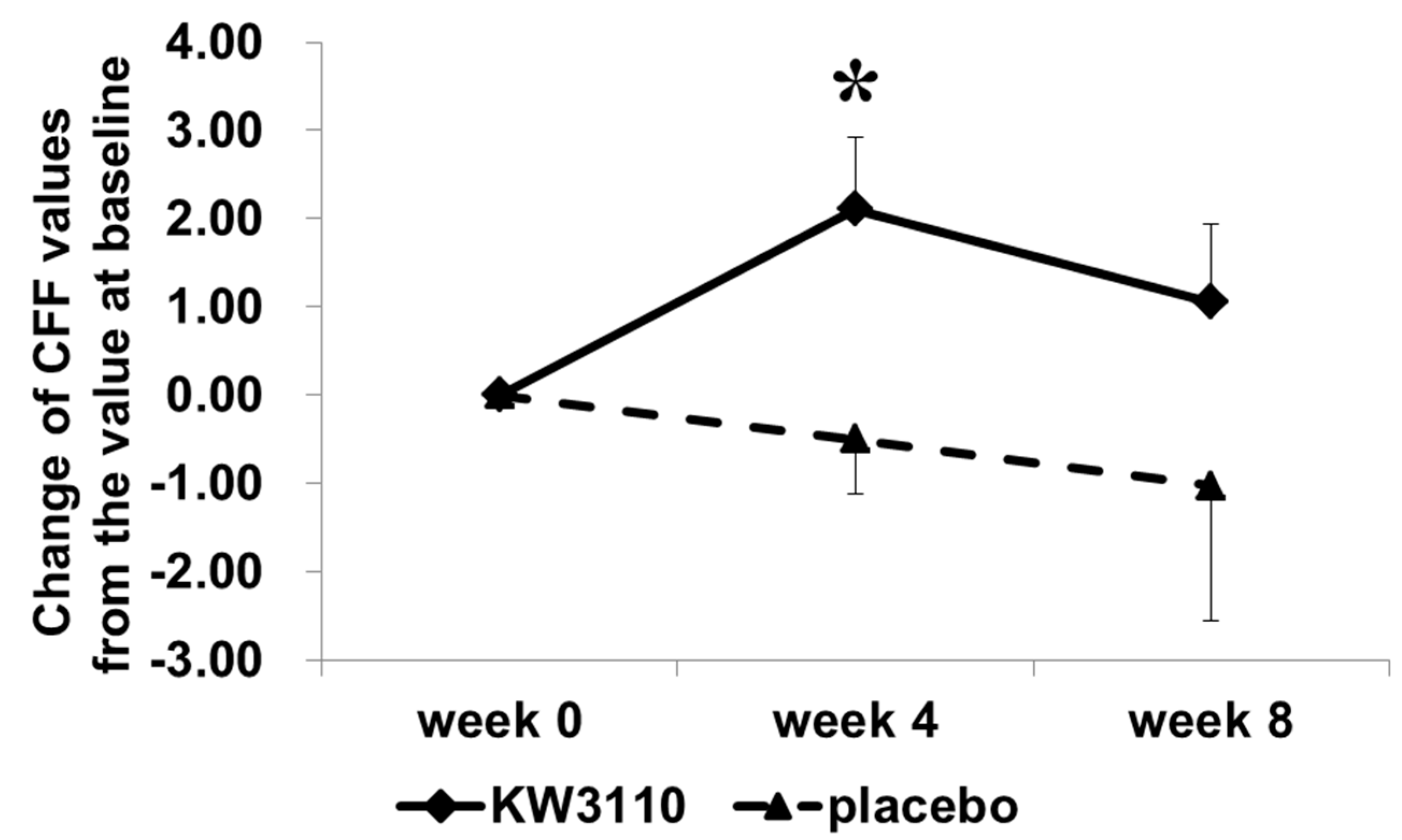
3.2.2. Ophthalmic Survey to Determine the Effects of L. paracasei KW3110 on VDT Load-Induced Eye Disorders
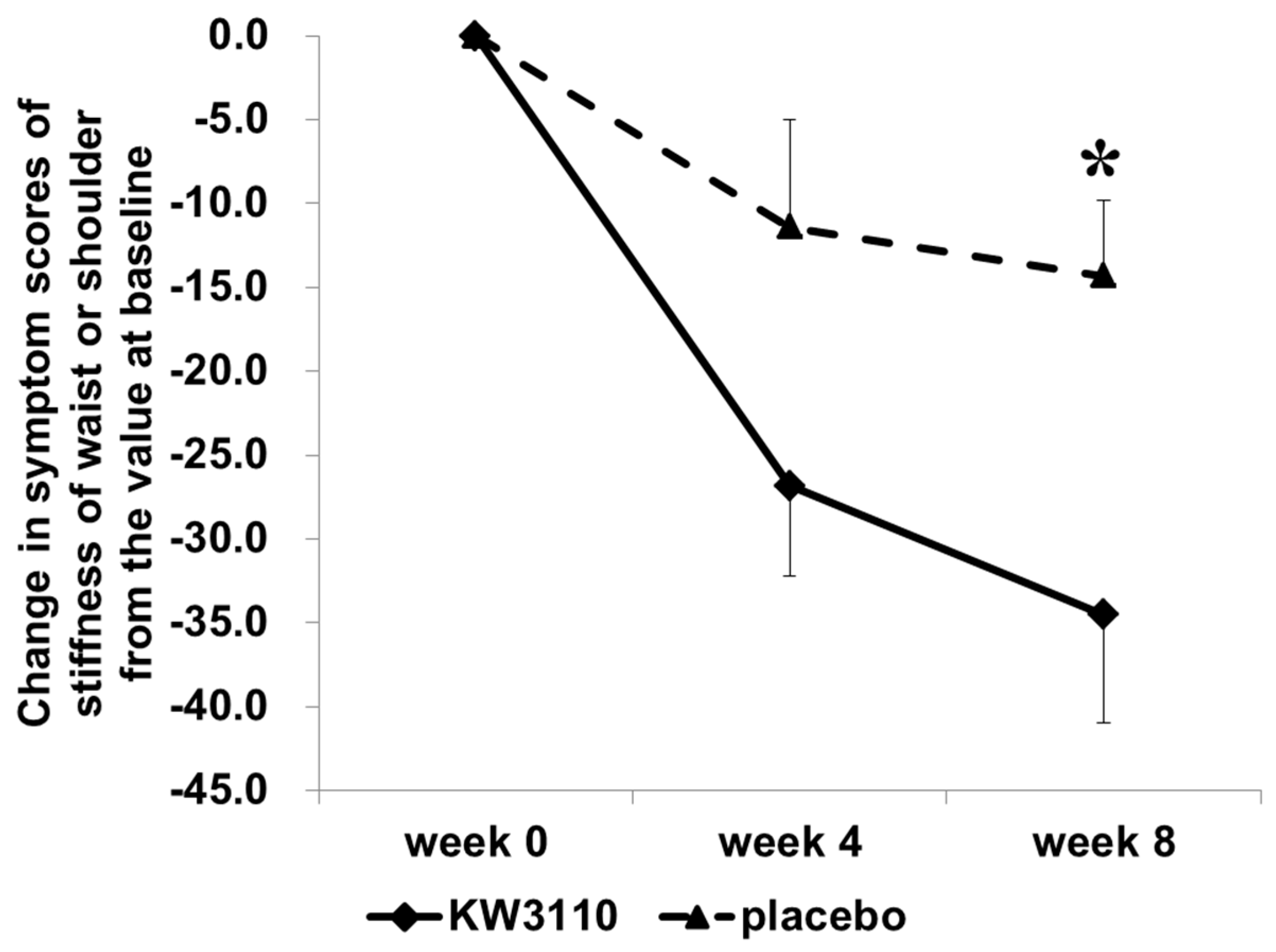
3.2.3. Questionnaire Survey to Determine the Effects of L. paracasei KW3110 on VDT Load-Induced Subjective Eye Conditions
3.2.4. Effects of L. paracasei KW3110 on VDT-Induced Eye Conditions in the Subjects Having a High-Level of Ocular Fatigue Sensation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bergqvist, U. Possible health effects of working with vdus. Br. J. Ind. Med. 1989, 46, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Knave, B.G.; Wibom, R.I.; Voss, M.; Hedstrom, L.D.; Bergqvist, U.O. Work with video display terminals among office employees. I. Subjective symptoms and discomfort. Scand. J. Work Environ. Health 1985, 11, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Eltayeb, S.; Staal, J.B.; Hassan, A.; de Bie, R.A. Work related risk factors for neck, shoulder and arms complaints: A cohort study among dutch computer office workers. J. Occup. Rehabil. 2009, 19, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Parihar, J.K.; Jain, V.K.; Chaturvedi, P.; Kaushik, J.; Jain, G.; Parihar, A.K. Computer and visual display terminals (vdt) vision syndrome (cvdts). Med. J. Armed Forces India 2016, 72, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, G.; Stromberg, A. Work content and eye discomfort in vdt work. Int. J. Occup. Saf. Ergon. 1995, 1, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Kawakami, N.; Saito, Y.; Hino, E. Central nervous system effects and visual fatigue in vdt workers. Int. Arch. Occup. Environ. Health 1991, 63, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Araki, S.; Yokoyama, K.; Yamashita, K.; Okumatsu, T.; Sakou, S. Accumulation of vdt work-related visual fatigue assessed by visual evoked potential, near point distance and critical flicker fusion. Ind. Health 1996, 34, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Goto, E.; Yagi, Y.; Matsumoto, Y.; Tsubota, K. Impaired functional visual acuity of dry eye patients. Am. J. Ophthalmol. 2002, 133, 181–186. [Google Scholar] [CrossRef]
- Uchino, M.; Schaumberg, D.A.; Dogru, M.; Uchino, Y.; Fukagawa, K.; Shimmura, S.; Satoh, T.; Takebayashi, T.; Tsubota, K. Prevalence of dry eye disease among japanese visual display terminal users. Ophthalmology 2008, 115, 1982–1988. [Google Scholar] [CrossRef] [PubMed]
- Thomson, W.D. Eye problems and visual display terminals—The facts and the fallacies. Ophthalmic Physiol. Opt. 1998, 18, 111–119. [Google Scholar] [CrossRef]
- Ye, Z.; Abe, Y.; Kusano, Y.; Takamura, N.; Eida, K.; Takemoto, T.; Aoyagi, K. The influence of visual display terminal use on the physical and mental conditions of administrative staff in japan. J. Physiol. Anthropol. 2007, 26, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.J. Impact of dry eye disease and treatment on quality of life. Curr. Opin. Ophthalmol. 2010, 21, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Vilela, M.A.; Pellanda, L.C.; Fassa, A.G.; Castagno, V.D. Prevalence of asthenopia in children: A systematic review with meta-analysis. J. Pediatr. 2015, 91, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Collier, J.D.; Rosenfield, M. Accommodation and convergence during sustained computer work. Optometry 2011, 82, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Kurimoto, S.; Iwasaki, T.; Nomura, T.; Noro, K.; Yamamoto, S. Influence of vdt (visual display terminals) work on eye accommodation. J. UOEH 1983, 5, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Kajita, M.; Ono, M.; Suzuki, S.; Kato, K. Accommodative microfluctuation in asthenopia caused by accommodative spasm. Fukushima J. Med. Sci. 2001, 47, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Portello, J.K.; Rosenfield, M.; Chu, C.A. Blink rate, incomplete blinks and computer vision syndrome. Optom. Vis. Sci. 2013, 90, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Uchino, Y.; Uchino, M.; Dogru, M.; Fukagawa, K.; Tsubota, K. Improvement of accommodation with anti-oxidant supplementation in visual display terminal users. J. Nutr. Health Aging 2012, 16, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Kim, J.C.; Kim, W.S.; Oh, H.J.; Yang, J.M.; Lee, J.B.; Yoon, K.C. Clinical effect of antioxidant glasses containing extracts of medicinal plants in patients with dry eye disease: A multi-center, prospective, randomized, double-blind, placebo-controlled trial. PLoS ONE 2015, 10, e0139761. [Google Scholar] [CrossRef] [PubMed]
- Snodderly, D.M. Evidence for protection against age-related macular degeneration by carotenoids and antioxidant vitamins. Am. J. Clin. Nutr. 1995, 62, 1448S–1461S. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, H.K.; Kim, C.Y.; Hong, Y.J.; Choe, C.M.; You, T.W.; Seong, G.J. Purified high-dose anthocyanoside oligomer administration improves nocturnal vision and clinical symptoms in myopia subjects. Br. J. Nutr. 2005, 93, 895–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.J.; Su, S.; Wu, J.; Du, H.; Li, S.S.; Huo, J.W.; Zhang, Y.; Wang, L.S. Variation of anthocyanins and flavonols in vaccinium uliginosum berry in lesser khingan mountains and its antioxidant activity. Food Chem. 2014, 160, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Galbis-Estrada, C.; Pinazo-Duran, M.D.; Martinez-Castillo, S.; Morales, J.M.; Monleon, D.; Zanon-Moreno, V. A metabolomic approach to dry eye disorders. The role of oral supplements with antioxidants and omega 3 fatty acids. Mol. Vis. 2015, 21, 555–567. [Google Scholar] [PubMed]
- Neuringer, M. Infant vision and retinal function in studies of dietary long-chain polyunsaturated fatty acids: Methods, results, and implications. Am. J. Clin. Nutr. 2000, 71, 256S–267S. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, R.; Kumar, P.; Phogat, H.; Kaur, A.; Kumar, M. Oral omega-3 fatty acids treatment in computer vision syndrome related dry eye. Contact Lens Anterior Eye 2015, 38, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Rutar, M.; Natoli, R.; Provis, J.M. Small interfering rna-mediated suppression of ccl2 in muller cells attenuates microglial recruitment and photoreceptor death following retinal degeneration. J. Neuroinflamm. 2012, 9, 221. [Google Scholar] [CrossRef] [PubMed]
- Jiao, H.; Natoli, R.; Valter, K.; Provis, J.M.; Rutar, M. Spatiotemporal cadence of macrophage polarisation in a model of light-induced retinal degeneration. PLoS ONE 2015, 10, e0143952. [Google Scholar] [CrossRef] [PubMed]
- Miyake, S.; Takahashi, N.; Sasaki, M.; Kobayashi, S.; Tsubota, K.; Ozawa, Y. Vision preservation during retinal inflammation by anthocyanin-rich bilberry extract: Cellular and molecular mechanism. Lab. Investig. 2012, 92, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Bermudez-Brito, M.; Plaza-Diaz, J.; Munoz-Quezada, S.; Gil, A. Sources, isolation, characterisation and evaluation of probiotics. Br. J. Nutr. 2013, 109 (Suppl. S2), S35–S50. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, S.; Fujii, R.; Fujiwara, D.; Komiyama, Y.; Kaisho, T.; Sakaguchi, M.; Konishi, Y. Myd88 but not tlr2, 4 or 9 is essential for il-12 induction by lactic acid bacteria. Biosci. Biotechnol. Biochem. 2007, 71, 3026–3032. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Nariai, C.; Takemura, F.; Nakao, W.; Fujiwara, D. Dietary supplementation with lactic acid bacteria attenuates the development of atopic-dermatitis-like skin lesions in nc/nga mice in a strain-dependent manner. Int. Arch. Allergy Immunol. 2008, 145, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, D.; Inoue, S.; Wakabayashi, H.; Fujii, T. The anti-allergic effects of lactic acid bacteria are strain dependent and mediated by effects on both th1/th2 cytokine expression and balance. Int. Arch. Allergy Immunol. 2004, 135, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, S.; Miyake, M.; Fujii, R.; Konishi, Y. Orally administered lactobacillus paracasei kw3110 induces in vivo il-12 production. Biosci. Biotechnol. Biochem. 2009, 73, 1561–1565. [Google Scholar] [CrossRef] [PubMed]
- Moriguchi, S. “Nikkagiren Suchihyo” [Numerical Scheme]; JUSE Press: Tokyo, Japan, 1968; Volume 80, pp. 37–43. (In Japanese) [Google Scholar]
- Richer, S.; Stiles, W.; Statkute, L.; Pulido, J.; Frankowski, J.; Rudy, D.; Pei, K.; Tsipursky, M.; Nyland, J. Double-masked, placebo-controlled, randomized trial of lutein and antioxidant supplementation in the intervention of atrophic age-related macular degeneration: The veterans last study (lutein antioxidant supplementation trial). Optometry 2004, 75, 216–230. [Google Scholar] [CrossRef]
- Sakane, Y.; Yamaguchi, M.; Yokoi, N.; Uchino, M.; Dogru, M.; Oishi, T.; Ohashi, Y.; Ohashi, Y. Development and validation of the dry eye-related quality-of-life score questionnaire. JAMA Ophthalmol. 2013, 131, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Kaji, R.; Kiyoshima-Shibata, J.; Nagaoka, M.; Nanno, M.; Shida, K. Bacterial teichoic acids reverse predominant il-12 production induced by certain lactobacillus strains into predominant il-10 production via tlr2-dependent erk activation in macrophages. J. Immunol. 2010, 184, 3505–3513. [Google Scholar] [CrossRef] [PubMed]
- Herz, J.; Filiano, A.J.; Smith, A.; Yogev, N.; Kipnis, J. Myeloid cells in the central nervous system. Immunity 2017, 46, 943–956. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.O.; Helming, L.; Gordon, S. Alternative activation of macrophages: An immunologic functional perspective. Annu. Rev. Immunol. 2009, 27, 451–483. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.K.; Mantovani, A. Macrophage plasticity and interaction with lymphocyte subsets: Cancer as a paradigm. Nat. Immunol. 2010, 11, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Sica, A.; Mantovani, A. Macrophage plasticity and polarization: In vivo veritas. J. Clin. Investig. 2012, 122, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Satoh, T.; Kidoya, H.; Naito, H.; Yamamoto, M.; Takemura, N.; Nakagawa, K.; Yoshioka, Y.; Morii, E.; Takakura, N.; Takeuchi, O.; et al. Critical role of trib1 in differentiation of tissue-resident m2-like macrophages. Nature 2013, 495, 524–528. [Google Scholar] [CrossRef] [PubMed]
- London, A.; Itskovich, E.; Benhar, I.; Kalchenko, V.; Mack, M.; Jung, S.; Schwartz, M. Neuroprotection and progenitor cell renewal in the injured adult murine retina requires healing monocyte-derived macrophages. J. Exp. Med. 2011, 208, 23–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, L.I.; Chiou, S.H.; Liu, C.J.; Yen, M.Y.; Wei, Y.H. The effect of photo-oxidative stress and inflammatory cytokine on complement factor H expression in retinal pigment epithelial cells. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6832–6841. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.B.; Gerratt, B.W.; Bassi, C.J.; Apte, R.S. Short-wavelength light-blocking eyeglasses attenuate symptoms of eye fatigue. Investig. Ophthalmol. Vis. Sci. 2017, 58, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Ayaki, M.; Hattori, A.; Maruyama, Y.; Nakano, M.; Yoshimura, M.; Kitazawa, M.; Negishi, K.; Tsubota, K. Protective effect of blue-light shield eyewear for adults against light pollution from self-luminous devices used at night. Chronobiol. Int. 2016, 33, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Maeda, E.; Yoshikawa, T.; Hayashi, N.; Akai, H.; Hanaoka, S.; Sasaki, H.; Matsuda, I.; Yoshioka, N.; Ohtomo, K. Radiology reading-caused fatigue and measurement of eye strain with critical flicker fusion frequency. Jpn. J. Radiol. 2011, 29, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Luczak, A.; Sobolewski, A. Longitudinal changes in critical flicker fusion frequency: An indicator of human workload. Ergonomics 2005, 48, 1770–1792. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Zhu, H.; Xu, J.; Wu, S.; Li, X.; He, S. Human cortical neural correlates of visual fatigue during binocular depth perception: An fnirs study. PLoS ONE 2017, 12, e0172426. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, N.; Imai, S.; Inokuchi, Y.; Shimazawa, M.; Yokota, S.; Araki, Y.; Hara, H. Bilberry and its main constituents have neuroprotective effects against retinal neuronal damage in vitro and in vivo. Mol. Nutr. Food Res. 2009, 53, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, Y.; Kawashima, M.; Inoue, S.; Inagaki, E.; Suzuki, A.; Ooe, E.; Kobayashi, S.; Tsubota, K. Bilberry extract supplementation for preventing eye fatigue in video display terminal workers. J. Nutr. Health Aging 2015, 19, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Kamm, K.E.; Stull, J.T.; Azuma, H. Delphinidin-3-rutinoside relaxes the bovine ciliary smooth muscle through activation of etb receptor and no/cgmp pathway. Exp. Eye Res. 2005, 80, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Uchino, M.; Yokoi, N.; Uchino, Y.; Dogru, M.; Kawashima, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Schaumberg, D.A.; et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: The osaka study. Am. J. Ophthalmol. 2013, 156, 759–766. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (1) | Subjects who had amblyopia or strabismus |
| (2) | Subjects who were diagnosed as presbyopia [the control width was less than 2.5 diopters (D) for the dominant eye] |
| (3) | Subjects who had an uncorrected serious refractive error for the dominant eye |
| (4) | Subjects who had undergone ophthalmic surgery for the dominant eye |
| (5) | Subjects who had best-corrected visual acuity <1.0 for the dominant eye |
| (6) | Subjects who had a serious eye disease |
| (7) | Subjects who were under treatment for any chronic disease and/or used medicines continuously or medical supplies that were being commonly used |
| (8) | Subjects who had the experience of a serious disease (e.g., diabetes, liver disease, kidney disease, and/or heart disease, thyroid gland disease, adrenal gland disease, digestive system disease, and/or metabolic disorder) |
| (9) | Subjects who could not stop eating foods similar to the test foods and/or were taking drugs or health foods including lactic acid bacteria or Bifidobacterium |
| (10) | Subjects with excessive alcohol-drinking behavior |
| (11) | Subjects who regularly took drugs or health foods, which might have had effects on the eyes or were expected to be used during the study |
| (12) | Subjects who could not stop taking drugs or health foods, which might have effects on immune functions |
| (13) | Subjects with the possibility of drug and/or food allergy |
| (14) | Subjects who could not stop drinking alcoholic beverages for 2 days until the pre-check day and check days |
| (15) | Subjects who had a history of pollinosis |
| (16) | Subjects who have a tendency to get diarrhea by eating dairy products |
| (17) | Subjects diagnosed with drug or alcohol dependence |
| (18) | Subjects who and/or whose family worked in a company selling or manufacturing health foods or foods with functional claims |
| (19) | Subjects who could not execute a display work load test |
| (20) | Subjects who were participating in other clinical studies or revoked an agreement acquisition day and/or participated in other clinical studies within 3 months or who were planning to participate in other clinical studies during this study |
| (21) | Subjects who were pregnant, breastfeeding, planning to get pregnant, or breastfeeding during the study |
| (22) | Subjects who were judged as unsuitable by the physician for laboratory data, anthropometric measurements, or physical examination values |
| (23) | Subjects who were judged as unsuitable for the study as assessed by the background questionnaire |
| (24) | Subjects who were judged as unsuitable by the supervising physician for other reasons |
| Characteristic | KW3110 | Placebo | p Values |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Number of subjects (male/female) | 28 (13/15) | 31 (15/16) | 0.880 |
| Age (years) | 40.3 ± 2.7 | 40.6 ± 2.8 | 0.651 |
| Body weight (kg) | 58.27 ± 10.29 | 59.34 ± 10.60 | 0.695 |
| BMI (kg/m2) | 21.48 ± 2.53 | 21.86 ± 2.40 | 0.564 |
| CFF (Hz) | KW3110 Group (n = 28) | Placebo Group (n = 31) | ||||
|---|---|---|---|---|---|---|
| Week 0 | Week 4 | Week 8 | Week 0 | Week 4 | Week 8 | |
| Before VDT load | 39.13 ± 2.47 | 39.57 ± 2.95 | 39.98 ± 2.94 | 39.03 ± 2.62 | 39.45 ± 2.36 | 39.77 ± 2.83 |
| After VDT load | 37.68 ± 2.40 | 39.87 ± 2.52 ** | 39.56 ± 2.92 ** | 38.10 ± 2.97 | 39.24 ± 2.15 * | 39.95 ± 2.13 * |
| Variation a | −1.45 ± 2.38 | 0.30 ± 2.70 * | −0.42 ± 2.31 | −0.94 ± 2.04 | −0.22 ± 2.03 | 0.17 ± 2.97 |
| Symptoms | KW3110 Group (n = 28) | Placebo Group (n = 31) | |||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 4 | Week 8 | Week 0 | Week 4 | Week 8 | ||
| Ocular pain | Before VDT load | 15.0 ± 17.9 | 9.3 ± 13.5 | 7.4 ± 14.3 | 12.5 ± 20.2 | 7.8 ± 14.3 | 8.9 ± 18.2 |
| After VDT load | 28.5 ± 28.7 | 23.4 ± 26.4 | 17.6 ± 22.7 | 25.5 ± 26.6 | 20.5 ± 25.5 | 16.7 ± 22.3 | |
| Variation a | 13.5 ± 20.8 | 14.1 ± 19.8 | 10.3 ± 16.6 | 13.0 ± 20.3 | 12.7 ± 21.4 | 7.8 ± 16.0 | |
| Blurred vision | Before VDT load | 15.6 ± 22.0 | 9.8 ± 16.9 | 8.1 ± 14.6 | 13.8 ± 15.8 | 10.2 ± 17.1 | 9.5 ± 15.5 |
| After VDT load | 25.0 ± 26.3 | 19.6 ± 25.4 | 16.7 ± 24.5 | 26.3 ± 26.1 | 20.6 ± 24.3 | 19.8 ± 22.9 | |
| Variation a | 9.4 ± 16.4 | 9.8 ± 15.4 | 8.6 ± 17.5 | 12.5 ± 21.1 | 10.4 ± 17.8 | 10.4 ± 14.9 | |
| Excess tearing | Before VDT load | 8.8 ± 14.5 | 8.9 ± 15.7 | 3.5 ± 5.7 | 8.2 ± 13.7 | 7.9 ± 17.0 | 7.3 ± 17.3 |
| After VDT load | 16.8 ± 22.0 | 13.6 ± 23.8 | 12.9 ± 19.2 | 17.8 ± 23.5 | 13.7 ± 21.4 | 11.4 ± 19.8 | |
| Variation a | 8.1 ± 18.8 | 4.7 ± 20.9 | 9.4 ± 15.5 | 9.6 ± 20.3 | 5.8 ± 12.8 | 4.1 ± 13.4 | |
| Stiffness of waist or shoulder | Before VDT load | 40.9 ± 24.5 | 29.9 ± 22.9 * | 21.1 ± 20.7 ** | 31.7 ± 23.7 | 23.9 ± 24.9 * | 20.2 ± 22.0 ** |
| After VDT load | 60.3 ± 21.8 | 44.3 ± 29.5 ** | 42.1 ± 25.5 ** | 48.0 ± 31.3 | 42.3 ± 31.4 | 35.5 ± 26.5 ** | |
| Variation a | 19.4 ± 16.3 | 14.4 ± 21.2 | 21.0 ± 19.1 | 16.3 ± 25.7 | 18.4 ± 24.8 | 15.3 ± 21.5 | |
| Ocular fatigue sensation | Before VDT load | 33.8 ± 25.6 | 23.0 ± 25.0 | 16.1 ± 20.6 ** | 27.5 ± 23.9 | 16.5 ± 20.5 ** | 15.0 ± 23.1 ** |
| After VDT load | 56.7 ± 26.4 | 43.6 ± 29.7 ** | 37.9 ± 27.8 ** | 53.9 ± 26.1 | 42.5 ± 30.4 ** | 38.2 ± 26.7 ** | |
| Variation a | 22.9 ± 18.3 | 20.6 ± 21.2 | 21.8 ± 23.4 | 26.4 ± 22.1 | 26.0 ± 24.2 | 23.2 ± 19.2 | |
| Dazzled vision | Before VDT load | 7.4 ± 14.9 | 7.9 ± 15.9 | 5.8 ± 14.1 | 5.9 ± 9.9 | 5.2 ± 11.6 | 2.6 ± 6.0 |
| After VDT load | 17.6 ± 20.1 | 12.9 ± 20.7 | 13.9 ± 23.1 | 14.9 ± 22.4 | 11.2 ± 21.5 | 9.3 ± 19.8 | |
| Variation a | 10.2 ± 16.5 | 5.0 ± 13.8 | 8.2 ± 17.4 | 9.0 ± 19.6 | 6.0 ± 23.5 | 6.6 ± 16.9 | |
| Double vision | Before VDT load | 7.1 ± 14.1 | 7.5 ± 15.5 | 5.1 ± 13.2 | 4.2 ± 9.1 | 5.4 ± 11.5 | 3.1 ± 6.0 |
| After VDT load | 12.8 ± 20.1 | 11.8 ± 19.9 | 11.4 ± 22.7 | 11.0 ± 22.0 | 9.4 ± 19.9 | 4.0 ± 7.4 | |
| Variation a | 5.7 ± 14.6 | 4.3 ± 12.0 | 6.3 ± 16.0 | 6.8 ± 19.5 | 4.0 ± 20.9 | 0.9 ± 4.1 | |
| Frustration | Before VDT load | 11.3 ± 15.6 | 8.2 ± 12.0 | 7.4 ± 11.0 | 9.2 ± 16.6 | 9.1 ± 16.8 | 5.9 ± 10.2 |
| After VDT load | 25.1 ± 27.7 | 21.4 ± 26.9 | 20.3 ± 27.1 | 18.7 ± 26.0 | 14.7 ± 17.7 | 14.5 ± 17.9 | |
| Variation a | 13.9 ± 19.2 | 13.3 ± 23.2 | 12.9 ± 21.0 | 9.5 ± 29.0 | 5.6 ± 18.9 | 8.5 ± 16.2 | |
| Stuffy head | Before VDT load | 18.0 ± 22.0 | 11.0 ± 14.3 | 7.8 ± 13.8 * | 11.9 ± 20.7 | 7.9 ± 12.9 | 7.8 ± 15.8 |
| After VDT load | 31.8 ± 27.8 | 23.5 ± 28.7 | 20.3 ± 25.6 * | 19.3 ± 26.8 | 18.6 ± 28.7 | 17.5 ± 25.0 | |
| Variation a | 13.8 ± 22.3 | 12.6 ± 22.8 | 12.5 ± 19.6 | 7.4 ± 15.2 | 10.7 ± 22.6 | 9.6 ± 16.3 | |
| Eye redness | Before VDT load | 12.2 ± 16.2 | 8.6 ± 11.6 | 6.9 ± 12.1 | 13.2 ± 22.1 | 13.6 ± 23.7 | 11.4 ± 25.6 |
| After VDT load | 14.9 ± 21.6 | 15.4 ± 26.0 | 10.8 ± 20.4 | 17.0 ± 23.5 | 13.6 ± 22.3 | 10.3 ± 20.5 | |
| Variation a | 2.7 ± 17.2 | 6.9 ± 20.2 | 3.9 ± 16.3 | 3.8 ± 9.7 | −0.1 ± 11.2 | −1.1 ± 17.0 | |
| Headache | Before VDT load | 10.0 ± 17.4 | 7.8 ± 11.8 | 4.5 ± 9.7 | 7.5 ± 16.9 | 6.9 ± 15.2 | 6.5 ± 15.9 |
| After VDT load | 26.9 ± 28.4 | 18.9 ± 24.0 | 14.6 ± 21.9 | 18.4 ± 25.7 | 15.4 ± 24.6 | 15.5 ± 23.4 | |
| Variation a | 16.9 ± 27.1 | 11.1 ± 20.1 | 10.0 ± 17.1 | 10.8 ± 19.5 | 8.4 ± 18.5 | 8.9 ± 15.1 | |
| KW3110 Group (n = 13) | Placebo Group (n = 12) | |||||
|---|---|---|---|---|---|---|
| Week 0 | Week 4 | Week 8 | Week 0 | Week 4 | Week 8 | |
| Before VDT load | 39.36 ± 2.32 | 39.03 ± 2.05 | 40.51 ± 3.10 | 38.75 ± 2.75 | 39.56 ± 2.37 | 40.42 ± 3.46 |
| After VDT load | 37.87 ± 2.29 | 39.64 ± 1.91 * | 40.08 ± 2.66 * | 38.33 ± 3.32 | 38.64 ± 2.07 | 38.97 ± 1.79 |
| Variation a | −1.49 ± 2.35 | 0.62 ± 2.18 * | −0.44 ± 2.47 | −0.42 ± 2.48 | −0.92 ± 1.75 | −1.44 ± 3.48 |
| Symptoms | KW3110 Group (n = 13) | Placebo Group (n = 12) | |||||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 4 | Week 8 | Week 0 | Week 4 | Week 8 | ||
| Ocular pain | Before VDT load | 28.0 ± 18.0 | 7.7 ± 5.5 * | 11.5 ± 19.9 | 25.6 ± 26.5 | 17.4 ± 19.0 | 20.6 ± 25.2 |
| After VDT load | 49.2 ± 26.7 | 31.2 ± 24.8 | 24.5 ± 22.8 | 38.4 ± 30.6 | 35.3 ± 29.6 | 32.2 ± 28.1 | |
| Variation a | 21.2 ± 25.9 | 23.5 ± 24.1 | 12.9 ± 16.4 | 12.8 ± 27.7 | 17.9 ± 28.6 | 11.6 ± 23.9 | |
| Stiffness of waist or shoulder | Before VDT load | 60.8 ± 13.8 | 33.9 ± 21.3 ** | 26.2 ± 25.0 ** | 50.4 ± 15.8 | 39.0 ± 21.8 | 36.1 ± 25.0 ** |
| After VDT load | 74.5 ± 13.1 | 51.8 ± 27.8 * | 50.4 ± 26.2 ** | 65.6 ± 24.1 | 60.5 ± 22.5 | 51.8 ± 22.6 * | |
| Variation a | 13.7 ± 12.5 | 17.9 ± 26.8 | 24.2 ± 23.4 | 15.2 ± 18.5 | 21.5 ± 18.5 | 15.8 ± 14.3 | |
| Ocular fatigue sensation | Before VDT load | 59.1 ± 10.1 | 28.3 ± 23.8 ** | 23.8 ± 26.0 ** | 53.3 ± 15.2 | 34.5 ± 22.5 * | 35.8 ± 25.8 * |
| After VDT load | 74.8 ± 15.4 | 55.7 ± 24.7 * | 50.2 ± 25.0 ** | 71.4 ± 17.4 | 62.6 ± 22.8 | 61.8 ± 18.7 | |
| Variation a | 15.7 ± 16.0 | 27.4 ± 22.6 | 26.5 ± 27.4 | 18.2 ± 16.6 | 28.1 ± 20.5 | 26.0 ± 19.4 | |
| Stuffy head | Before VDT load | 32.2 ± 24.6 | 12.3 ± 12.3 * | 10.8 ± 18.2 * | 21.5 ± 28.0 | 16.1 ± 16.6 | 15.8 ± 21.9 |
| After VDT load | 43.5 ± 28.4 | 29.5 ± 28.2 | 25.1 ± 29.0 | 32.9 ± 30.4 | 31.0 ± 30.3 | 29.0 ± 28.2 | |
| Variation a | 11.4 ± 19.2 | 17.2 ± 28.5 | 14.3 ± 20.4 | 11.4 ± 19.1 | 14.9 ± 19.8 | 13.2 ± 18.0 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morita, Y.; Jounai, K.; Miyake, M.; Inaba, M.; Kanauchi, O. Effect of Heat-Killed Lactobacillus paracasei KW3110 Ingestion on Ocular Disorders Caused by Visual Display Terminal (VDT) Loads: A Randomized, Double-Blind, Placebo-Controlled Parallel-Group Study. Nutrients 2018, 10, 1058. https://doi.org/10.3390/nu10081058
Morita Y, Jounai K, Miyake M, Inaba M, Kanauchi O. Effect of Heat-Killed Lactobacillus paracasei KW3110 Ingestion on Ocular Disorders Caused by Visual Display Terminal (VDT) Loads: A Randomized, Double-Blind, Placebo-Controlled Parallel-Group Study. Nutrients. 2018; 10(8):1058. https://doi.org/10.3390/nu10081058
Chicago/Turabian StyleMorita, Yuji, Kenta Jounai, Mika Miyake, Masaharu Inaba, and Osamu Kanauchi. 2018. "Effect of Heat-Killed Lactobacillus paracasei KW3110 Ingestion on Ocular Disorders Caused by Visual Display Terminal (VDT) Loads: A Randomized, Double-Blind, Placebo-Controlled Parallel-Group Study" Nutrients 10, no. 8: 1058. https://doi.org/10.3390/nu10081058
APA StyleMorita, Y., Jounai, K., Miyake, M., Inaba, M., & Kanauchi, O. (2018). Effect of Heat-Killed Lactobacillus paracasei KW3110 Ingestion on Ocular Disorders Caused by Visual Display Terminal (VDT) Loads: A Randomized, Double-Blind, Placebo-Controlled Parallel-Group Study. Nutrients, 10(8), 1058. https://doi.org/10.3390/nu10081058