Lutein Intake and Blood Lutein Concentration Are Positively Associated with Physical Activity in Adults: A Systematic Review




Abstract
:1. Introduction
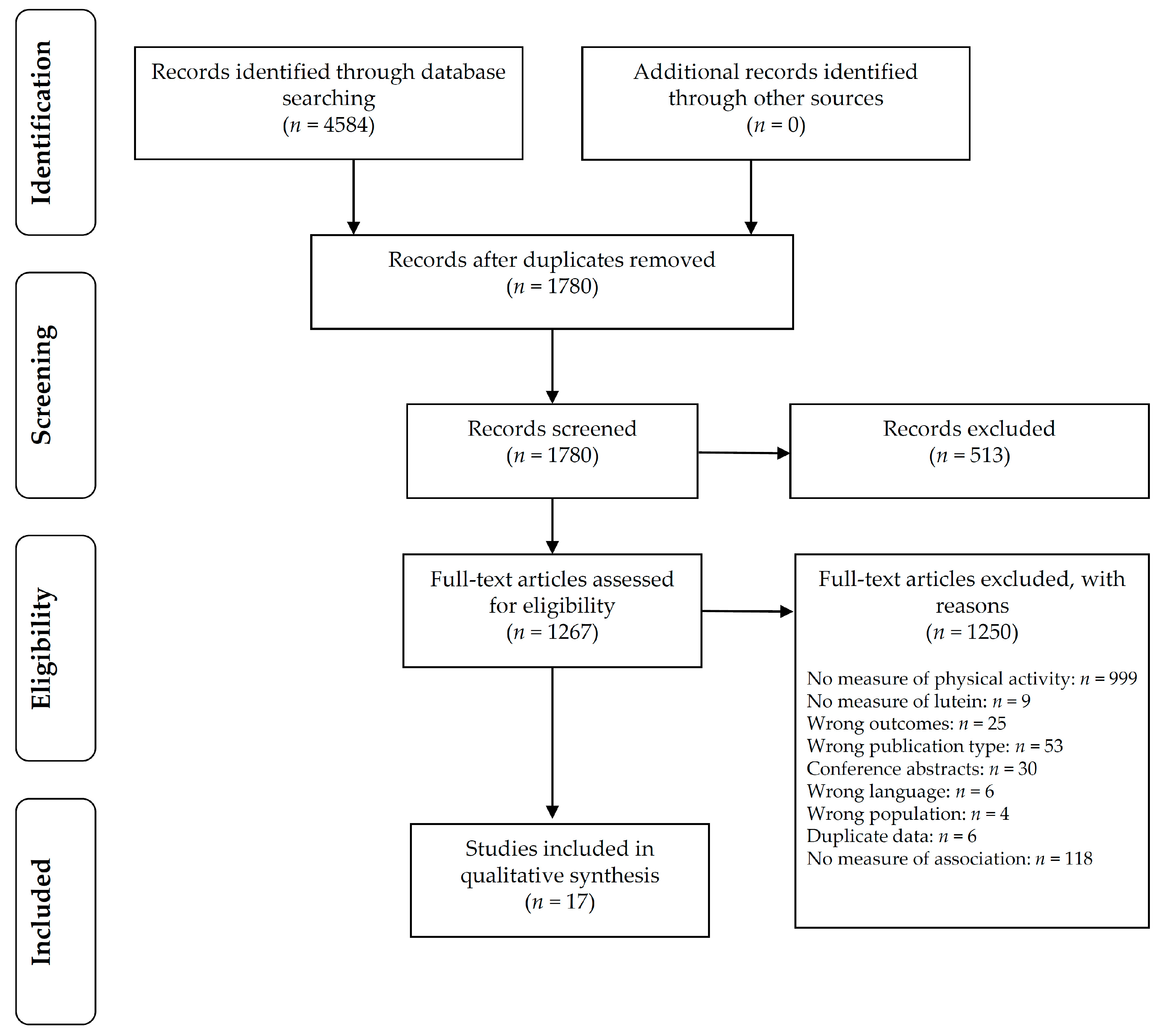
2. Materials and Methods
3. Results
3.1. Synthesis of Results
3.2. Risk of Bias within Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Australian Bureau of Statistics. National Health Survey: First Results 2014-15; Australian Bureau of Statistics: Canberra, Australia, 2015.
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the united states measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Impact of Physical Inactivity as a Risk Factor for Chronic Conditions: Australian Burden of Disease Study; Australian Institute of Health and Welfare: Canberra, Australia, 2017. [Google Scholar]
- Australian Department of Health. Australia’s Physical Activity and Sedentary Behaviour Guidelines. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines/$File/FS-Adults-18-64-Years.PDF (accessed on 24 November 2015).
- Slentz, C.; Houmard, J.; Kraus, W. Modest exercise prevents the progressive disease associated with physical inactivity. Exerc. Sport Sci. Rev. 2007, 35, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Sommerburg, O.; Keunen, J.; Bird, A.; van Kuijk, F. Fruits and vegetables that are sources for lutein and zeaxanthin: The macular pigment in human eyes. Br. J. Opthalmol. 1998, 82, 907–910. [Google Scholar] [CrossRef]
- Mares-Perlman, J.; Millen, A.; Ficek, T.; Hankinson, S. The body of evidence to support a protective role for lutein and zeaxanthin in delaying chronic disease. J. Nutr. 2002, 132, 518S–524S. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Hagio, M.; Inoue, R.; Mitani, T.; Yajima, M.; Hara, H.; Yajima, T. Long-term oral feeding of lutein-fortified milk increases voluntary running distance in rats. PLoS ONE 2014, 9, e93529. [Google Scholar] [CrossRef] [PubMed]
- Thomson, R.L.; Coates, A.M.; Howe, P.R.; Bryan, J.; Matsumoto, M.; Buckley, J.D. Increases in plasma lutein through supplementation are correlated with increases in physical activity and reductions in sedentary time in older adults. Nutrients 2014, 6, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.; Elias, M.; Alkerwi, A.; Buckley, J. Intake of lutein-rich vegetables is associated with higher levels of physical activity. Nutrients 2015, 7, 8058–8071. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooke, M.; Buckley, J.; Coates, A.M.; Buckley, E. Does Dietary Intake of Lutein Affect Physical Activity Behavior in Adults? A Systematic Review and Meta-Analysis. Available online: https://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42016046749 (accessed on 29 August 2016).
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (axis). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Gross, M.D.; Jacobs, D.R., Jr. Association of serum carotenoids and tocopherols with γ- glutamyltransferase: The cardiovascular risk development in young adults (cardia) study. Clin. Chem. 2004, 50, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Hozawa, A.; Iribarren, C.; Daviglus, M.L.; Matthews, K.A.; Gross, M.D.; Jacobs, D.R., Jr. Longitudinal association of serum carotenoids and tocopherols with hostility: The cardia study. Am. J. Epidemiol. 2008, 167, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, Y.; Tanaka, K.; Kiyohara, C.; Hirohata, T.; Tomita, Y.; Ishibashi, M.; Kido, K. Relationship of alcohol use, physical activity and dietary habits with serum carotenoids, retinol and alpha-tocopherol among male Japanese smokers. Int. J. Epidemiol. 1997, 26, 307–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamulka, J.; Wawrzyniak, A.; Gadomska, M.; Gronowska-Senger, A.B.; Bawa, S. The influence of selected demographic and lifestyle factors on lutein intakes by groups of polish women. Int. J. Food Sci. Nutr. 2009, 60, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Gaziano, J.M.; Norkus, E.P.; Buring, J.E.; Sesso, H.D. Associations of plasma carotenoids with risk factors and biomarkers related to cardiovascular disease in middle-aged and older women. Am. J. Clin. Nutr. 2008, 88, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.E.; Ainsworth, B.E. Associations of food consumption, serum vitamins and metabolic syndrome risk with physical activity level in middle-aged adults: The national health and nutrition examination survey (nhanes) 2005–2006. Public Health Nutr. 2016, 19, 1674–1683. [Google Scholar] [CrossRef] [PubMed]
- Ciulla, T.A.; Curran-Celantano, J.; Cooper, D.A.; Hammond, B.R., Jr.; Danis, R.P.; Pratt, L.M.; Riccardi, K.A.; Filloon, T.G. Macular pigment optical density in a midwestern sample. Ophthalmology 2001, 108, 730–737. [Google Scholar] [CrossRef]
- Coyne, T.; Ibiebele, T.I.; McNaughton, S.; Rutishauser, I.H.E.; O’Dea, K.; Hodge, A.M.; McClintock, C.; Findlay, M.G.; Lee, A. Evaluation of brief dietary questions to estimate vegetable and fruit consumption—Using serum carotenoids and red-cell folate. Public Health Nutr. 2005, 8, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Thornquist, M.D.; Neuhouser, M.L.; Kristal, A.R.; Neumark-Sztainer, D.; Cooper, D.A.; Patterson, R.E.; Cheskin, L.J. Diet and lifestyle correlates of lutein in the blood and diet. J. Nutr. 2002, 132, 525S–530S. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.; Potter, J.D. Physical activity and colon cancer: Confounding or interaction? Med. Sci. Sports Exerc. 2002, 34, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Stimpson, J.P.; Nash, A.C.; Ju, H.; Eschbach, K. Neighborhood deprivation is associated with lower levels of serum carotenoids among adults participating in the third national health and nutrition examination survey. J. Am. Diet. Assoc. 2007, 107, 1895–1902. [Google Scholar] [CrossRef] [PubMed]
- Tormo, M.J.; Navarro, C.; Chirlaque, M.D.; Barber, X.; Argilaga, S.; Agudo, A.; Amiano, P.; Barricarte, A.; Beguiristain, J.M.; Dorronsoro, M.; et al. Physical sports activity during leisure time and dietary intake of foods and nutrients in a large spanish cohort. Int. J. Sport Nutr. Exerc. 2003, 13, 47–64. [Google Scholar] [CrossRef]
- Wang, Y.; Chung, S.J.; McCullough, M.L.; Song, W.O.; Fernandez, M.L.; Koo, S.I.; Chun, O.K. Dietary carotenoids are associated with cardiovascular disease risk biomarkers mediated by serum carotenoid concentrations. J. Nutr. 2014, 144, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Gruber, M.; Chappell, R.; Millen, A.; LaRowe, T.; Moeller, S.M.; Iannaccone, A.; Kritchevsky, S.B.; Mares, J. Correlates of serum lutein + zeaxanthin: Findings from the third national health and nutrition examination survey. J. Nutr. 2004, 134, 2387–2394. [Google Scholar] [CrossRef] [PubMed]
- Sahli, M.W.; Mares, J.A.; Meyers, K.J.; Klein, R.; Brady, W.E.; Klein, B.E.K.; Ochs-Balcom, H.M.; Donahue, R.P.; Millen, A.E. Dietary intake of lutein and diabetic retinopathy in the atherosclerosis risk in communities study (aric). Ophthalmic Epidemiol. 2016, 23, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Moeller, S.M.; Parekh, N.; Tinker, L.; Ritenbaugh, C.; Blodi, B.; Wallace, R.B.; Mares, J.A.; CAREDS Research Study Group. Associations between intermediate age-related macular degeneration and lutein and zeaxanthin in the carotenoids in age-related eye disease study (careds): Ancillary study of the women’s health initiative. Arch. Ophthalmol. 2006, 124, 1151–1162. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council of Australia. Nhmrc Levels of Evidence and Grades for Recommendations for Developers of Clinical Practice Guidelines. Available online: https://www.nhmrc.gov.au/_files_nhmrc/file/guidelines/developers/nhmrc_levels_grades_evidence_120423.pdf (accessed on 5 December 2016).
- Hamulka, J.; Koczara, J.; Gronek, M. Lutein content of selected polish foods and estimation of its intake. Pol. J. Food Nutr. Sci. 2005, 14/15, 201–206. [Google Scholar]
- The atherosclerosis risk in communities (aric) study: Design and objectives. The aric investigators. Am. J. Epidemiol. 1989, 129, 687–702. [Google Scholar]
- Natarajan, L.; Flatt, S.W.; Sun, X.; Gamst, A.C.; Major, J.M.; Rock, C.L.; Al-Delaimy, W.; Thomson, C.A.; Newman, V.A.; Pierce, J.P.; et al. Validity and systematic error in measuring carotenoid consumption with dietary self-report instruments. Am. J. Epidemiol. 2006, 163, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, C.; Betts, N.; Hoos, T.; Glenn, M. Young adult exercisers and nonexercisers differ in food attitudes, perceived dietary changes, and food choices. Int. J. Sport Nutr. 1996, 6, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Charreire, H.; Kesse-Guyot, E.; Bertrais, S.; Simon, C.; Chaix, B.; Weber, C.; Touvier, M.; Galan, P.; Hercberg, S.; Oppert, J.M. Associations between dietary patterns, physical activity (leisure-time and occupational) and television viewing in middle-aged french adults. Br. J. Nutr. 2011, 105, 902–910. [Google Scholar] [CrossRef] [PubMed]
- Olinto, M.T.; Willett, W.C.; Gigante, D.P.; Victora, C.G. Sociodemographic and lifestyle characteristics in relation to dietary patterns among young Brazilian adults. Public Health Nutr. 2011, 14, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Schmid, D.; Ricci, C.; Baumeister, S.E.; Leitzmann, M.F. Replacing sedentary time with physical activity in relation to mortality. Med. Sci. Sports Exerc. 2016, 48, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Fishman, E.I.; Steeves, J.A.; Zipunnikov, V.; Koster, A.; Berrigan, D.; Harris, T.A.; Murphy, R. Association between objectively measured physical activity and mortality in nhanes. Med. Sci. Sports Exerc. 2016, 48, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 4364.0.55.004—Australian Health Survey: Physical Activity, 2011–12. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/4364.0.55.004Chapter1002011-12 (accessed on 5 June 2017).
- Vishwanathan, R.; Neuringer, M.; Snodderly, D.M.; Schalch, W.; Johnson, E.J. Macular lutein and zeaxanthin are related to brain lutein and zeaxanthin in primates. Nutr. Neurosci. 2013, 16, 21–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdman, J.W., Jr.; Smith, J.W.; Kuchan, M.J.; Mohn, E.S.; Johnson, E.J.; Rubakhin, S.S.; Wang, L.; Sweedler, J.V.; Neuringer, M. Lutein and brain function. Foods 2015, 4, 547–564. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Study Design | NHMRC Level of Evidence | CA Score | Sample Characteristics | Physical Activity Outcome Measure | Physical Activity Measure | Lutein Outcome Measure | Measure of Lutein Status | Measure of Association (Type, Strength, Direction, and Significance) |
|---|---|---|---|---|---|---|---|---|---|
| Randomised control trials | |||||||||
| Thomson et al. (2014) [10] | RCT | II | 7 | Australia n = 44 Sedentary, but otherwise healthy males and females 68.8 ± 6.4 years BMI 25.3 ± 2.6 kg/m2 | Subjective and objective Amount of sedentary PA, light PA and mod–vig PA by exercise diary Cut-point PA levels using accelerometer (7164 ActiGraph) over 7-day period | Lutein (Mean values) Sed: 235 min/day (SD 61), light PA: 301 min/day (SD 88), mod-vig PA: 22 min/day (SD 14) Accelerometer 235,292 counts per day (SD 82, 693) Placebo Sed: 219 mins/day (SD 46), light PA: 341 min/day (SD 76), mod-vig PA: 24 min/day (SD 18) Accelerometer 273,760 counts per day (SD 85, 018) | Objective HPLC (plasma lutein and zeaxanthin separately) | Lutein: mean 10.3 ug/dL (SD 2.5) Placebo: mean 10.1 ug/dL (SD 3.6) | (1) Correlation SEDENTARY: Plasma lutein and time spent sedentary: r = −0.36 (p = 0.03) PA: Plasma lutein and activity counts: r = 0.29, p = 0.08 (2) % change correlation SEDENTARY: Time sedentary and relative % change in plasma lutein: r = −0.39 (p = 0.02) PA: % difference lutein with % difference activity, r = 0.36, p = 0.03 |
| Cross sectional studies ^ | |||||||||
| Choi et al. (2016) [20] | Cross sectional | IV | 17 | USA n = 1661 NHANES 40–70 years | Objective Accelerometer daily steps (sedentary [s], intermediate [i], and active [a]) | Male: s <6802 steps/day i = 6082–10, 698 steps/day a >10, 698 steps/day Female: s < 5785 steps/day i = 5785–9225 steps/day a ≥ 9226 steps/day | Objective Serum lutein and zeaxanthin | Male: s = 14.0 ug/dL mean (SE 0.7) i = 16.3 ug/dL mean (SE 0.6) a = 18.9 ug/dL mean (SE 0.6) Female: s = 14.8 ug/dL mean (SE 0.6) i = 17.1 ug/dL mean (SE 0.5) a = 18.6 ug/dL mean (SE 0.5) | ANCOVA tertiles of step counts. Covariates: age, BMI, total energy intake M: positive increase serum lutein/zeaxanthin with increasing tertile step counts (p < 0.01) F: positive increase serum lutein/zeaxanthin with increasing tertile step counts (p < 0.01) >26% higher serum lutein + zexanthin in active vs sedentary participants Associated with >57% difference in accelerometer step counts between sedentary and active participants |
| Coyne et al. (2005) [22] | Cross sectional | IV | 17 | Australia n = 1598 Random sample of adults ≥25 years | Subjective Self-report questionnaire previous week. PA time: sum of time walking or moderate intensity activity plus double time vigorous activity | Sufficiently active >150 min/week In-sufficiently active <150 min/week Sedentary 0 min/week | Objective HPLC serum lutein/zeaxanthin | Active: 0.39 umol/L mean (95% CI 0.37–0.41) In-sufficiently active: 0.39 umol/L mean. (95% CI 0.37–0.41) Sedentary: 0.37 umol/L mean (95% CI 0.34–0.39) | ANOVA No significant difference serum lutein/zeaxanthin across PA tertiles, p > 0.01 |
| Gruber et al. (2004) [28] | Cross sectional | IV | 15 | USA n = 7059 NHANES ≥40 years | Subjective Interview | PA ‘yes’ by quintiles of serum lutein/zeaxanthin Q1: 51%, Q3: 62%, Q5: 69%. | Objective HPLC serum lutein/zeaxanthin | Q1: 0.02–0.25 umol/L Q3: 0.33–0.44 umol/L Q5: 0.58–4.45 umol/L | Participants who were physically active had 13% higher serum lutein/zeaxanthin than those who were not active, p < 0.01 |
| Kitamura et al. (1997) [17] | Cross sectional | IV | 15 | Japan n = 194 Healthy male smokers (>15 cigarettes/day) 24–60 years | Subjective Self-reported questionnaire (closed questions) | Average duration walking/day (<30 min, 30 min to 1 h, 1–2 h, >2 h) Frequency participating in sports (none, occasional, frequent) | Objective HPLC (serum lutein) | HPLC: Mean 39.2 ug/dL (95% CI 37.5–41.0) | Spearman rank correlation coefficient (adjusted for age) Between walking time and serum lutein, r = 0.01 (p > 0.05) Between frequency of sport participation and serum lutein, r = 0.12 (p < 0.05) |
| Lee et al. (2004) [15] | Cross sectional | IV | 15 | USA n = 3128 Black and white males and females 17–35 years | Subjective CARDIA PA history, Minnesota Leisure time PA questionnaire (Simplified version) | Data not reported | Objective HPLC serum lutein/zeaxanthin | Data not reported | Linear regression analysis r = 0.08 (p < 0.01) |
| Slattery & Potter (2002) [24] | Cross sectional (case control) | IV | 15 | USA Colon cancer cases n = 1993 Control n = 2410 30–79 years | Subjective CARDIA PA questionnaire (Scoring 1 = no vigorous leisure time PA) 2 = 1–250 cal/week. 3 = 251–1000 cal/week. 4 ≥ 1000 cal/week) | Men: Case: 1: n = 233, 2: n = 312, 3: n = 329, 4: n = 225. Control: 1: n = 216, 2: n = 314, 3: n = 379, 4: n = 380 Women: Case: 1: n = 326, 2: n = 233, 3: n = 189, 4: n = 146. Control: 1: n = 318, 2: n = 314, 3: n = 264, 4: n = 224 | Subjective Nutrient values calculated using Minnesota NCC database | Data not reported | (1) Correlation coefficient: Male: r = 0.08 (p < 0.05) Female: r = 0.05 (p > 0.05) |
| Hamulka et al. (2009) [18] | Cross sectional | IV | 14 | Poland n = 100 Female 48.6 ± 16.2 years BMI 24.6 kg/m2 | Subjective Self-reported questionnaire | Sedentary, moderate, high (values not reported) | Subjective Dietary lutein intake from food records | Sed: mean 2.02 mg/day (SD 0.67) Mod: mean 2.29 mg/day (SD 1.21) High: mean 1.85 mg/day (SD 0.74) | Non-parametric Kruskal–Wallis ANOVA, p = 0.33 Spearman rank correlation: Crude: r = 0.105 (p = 0.30) Adjusted for age, BMI, place of dwelling and level of education: r = −0.062 (p = 0.55) |
| Sahli et al. (2016) [29] | Cross sectional | IV | 14 | USA n = 1430 Black and white male and female 45–65 years Diabetes mellitus | Subjective Modified Baecke PA questionnaire | By quintiles of lutein intake Q1: PA at work 2.2 (SD 0.6) Sports in leisure time 2.3 (SD 0.8) Other leisure time PA 2.3 (SD 0.6) Q4: PA at work 2.1 (SD 1.0) Sports in leisure time 2.4 (SD 0.7) Other leisure time physical activity 2.3 (SD 0.6) | Subjective (outcome measure not reported) | Q1: mean 435.2 ug/1000 kcal (SD 165.1) Q4: mean 4853.1 ug/1000 kcal (SD 2695.3) | ANOVA PA at work index p = 0.29 Sports in leisure time index p = 0.89 Other leisure time PA index p = 0.25 |
| Stimpson et al. (2007) [25] | Cross sectional | IV | 13 | USA n = 17, 002 NHANES ≥17 years | Subjective Self-reported questionnaire | PA score of 0: n = 11,757 PA score >1: n = 5236 Missing: n = 9 | Objective HPLC serum lutein/zeaxanthin | PA score 0: mean 22.62 ug/dL (SD 12.59) PA score ≥1: mean 23.17 ug/dL (SD 13.33) | Multivariate linear regression ≥1, using high PA as a reference B value = −1.10 (SE 0.34) p < 0.01. Indicating that as serum lutein + zeaxanthin increased physical inactivity decreased |
| Tormo et al. (2003) [26] | Cross sectional | IV | 13 | Spain n = 37, 287 Healthy male and female 50.9 ± 7.2 years BMI 28.4 ± 3.4 kg/m2 31% smokers 17% heavy drinkers | Subjective PA questionnaire | 0–0.5 h/week, >0.5–2 h/week, >2–3 h/week, >3 h/week | Subjective Lutein intake, food recalls against Food Composition table | 0–0.5 h/week (ref): mean 784.7 ug/day (SD 826.0) >0.5–2 h/week mean 898.8 ug/day (SD 828.6) >2–3 h/week mean 935.6 (SD 910.7) >3 h/week mean 854.7 ug/day (SD 840.0) | p < 0.05 for ANOVA comparing mean value of each PA category with reference level p < 0.05 for ANCOVA comparing mean PA category with reference level adjusted by age, BMI, current smoking, excessive alcohol drinking, secondary/higher education, sedentary PA at work and interaction of education with PA at work ≥600% difference in hours of PA |
| Ciulla et al. (2001) [21] | Cross sectional | IV | 12 | USA n = 280 Male and female 18–50 years 26% smokers | Subjective Self-reported questionnaire | Number of times exercise per week | Objective Serum lutein/zeaxanthin (umol/L) Subjective FFQ lutein/zeaxanthin (ug/day) | Serum: 0.372 umol/L mean (SD 0.169) Intake: 1102 ug/day mean (SD 839) | Spearman correlation coefficient Serum: r = 0.02, p > 0.05 Intake: r = 0.25, p < 0.05 |
| Moeller et al. (2006) [30] | Cross sectional | IV | 12 | USA n = 1787 Female 50–79 years | Subjective Self-reported questionnaire | Physical activity levels Low: 12 MET/week High PA: 18 MET/week | Objective HPLC serum lutein/zeaxanthin Subjective Dietary intake questionnaire | Dietary lutein intake Low: mean 792 ug/day (SD 169) High: mean 2868 ug/day (SD 919) | No measure of association between serum lutein and physical activity reported 50% difference in physical activity between low and high dietary intake groups (t-test, p ≤ 0.001). |
| Ohira et al. (2008) [16] | Cross sectional | IV | 12 | USA n = 3579 18–30 years | Subjective Self-reported total PA score, habitual PA, and participation in 13 different PA categories (vigorous to moderate) over 12 months | Total CARDIA PA history score (arbitrary units) | Objective HPLC 12-h fasting serum lutein/zeaxanthin | Data not reported | Correlation coefficient, adjusted for age, gender, race, and serum lipid r = 0.06, p < 0.01 |
| Wang et al. (2008) [19] | Cross sectional | IV | 11 | USA n = 2895 Female ≥45 years Self-reported free from cardiovascular disease and cancer (except non-melanoma skin cancer) | Subjective Questionnaire: self-reported vigorous PA | Rarely/never (ref), <1 time/week, 1–3 times/week, >4 times/week | Objective HPLC serum lutein/zeaxanthin | Reported as mean (95% CI) Rarely/never (ref): 0.279 umol/L (0.271–0.286) <1 time/week: 0.284 umol/L (0.274–0.296) 1–3 times/week 0.300 umol/L (0.290–0.309) >4-times/week: 0.310 umol/L (0.293–0.328) | Serum lutein + zeaxanthin significantly higher in 1–3 times/week and >4 times/week compared with rarely or never (t-test) p < 0.001 >400% difference between reference and >4 times per week of physical activity |
| Rock et al. (2002) [23] | Cross sectional | IV | 9 | USA n = 2786 Male and female 44 ± 16 years BMI 27.5 ± 6.1 kg/m2 | Subjective Questionnaire, PA minutes/day | <30 min/day (ref), 30–60 min/day or >60 min/day | Subjective Dietary lutein/zeaxanthin intake | Mean intake 1347 (891) ug/day | % difference in dietary intake of lutein + zeaxanthin from reference physical activity group (<30 min/day) 30–60 min/day: 10.3% higher dietary intake (5.6–15.3%) p = 0.05 >60 min/day: 19.3% higher dietary intake (9.6–29.8%) p = 0.05 |
| Wang et al. (2014) [27] | Cross sectional | IV | 9 | USA n = 2856 NHANES Male and female ≥ 20 years | Subjective Questionnaire | <2.5 MET h/week (ref) 2.5–<4 MET h/week 4–<11.5 MET h/week >11.5 MET h/week | Subjective Dietary lutein/zeaxanthin intake | <2.5 MET h/week: dietary intake of 0.65 mg/day (0.59–0.71) 2.5–<4 MET h/week: dietary intake of 0.84 mg/day (0.75–0.94) 4–<11.5 MET h/week: dietary intake of 0.82 mg/day (0.73-0.92) >11.5 MET h/week: dietary intake of 0.75 mg/day (0.68–0.83) | Multivariate model geometric means (95% CIs) Dietary lutein/zeaxanthin intake for 2.5–<4 MET h/week and 4–<11.5 MET h/week significantly different from <2.5 MET-h/week (ref) (p < 0.017) >400% difference in physical activity between dietary lutein intake of 0.65 mg/day (<2.5 MET h/week group) and dietary intake of 0.82–0.84 mg/day (2.5 to <11.5 MET h/week groups) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cooke, M.C.; Coates, A.M.; Buckley, E.S.; Buckley, J.D. Lutein Intake and Blood Lutein Concentration Are Positively Associated with Physical Activity in Adults: A Systematic Review. Nutrients 2018, 10, 1186. https://doi.org/10.3390/nu10091186
Cooke MC, Coates AM, Buckley ES, Buckley JD. Lutein Intake and Blood Lutein Concentration Are Positively Associated with Physical Activity in Adults: A Systematic Review. Nutrients. 2018; 10(9):1186. https://doi.org/10.3390/nu10091186
Chicago/Turabian StyleCooke, Madeline C., Alison M. Coates, Elizabeth S. Buckley, and Jonathan D. Buckley. 2018. "Lutein Intake and Blood Lutein Concentration Are Positively Associated with Physical Activity in Adults: A Systematic Review" Nutrients 10, no. 9: 1186. https://doi.org/10.3390/nu10091186
APA StyleCooke, M. C., Coates, A. M., Buckley, E. S., & Buckley, J. D. (2018). Lutein Intake and Blood Lutein Concentration Are Positively Associated with Physical Activity in Adults: A Systematic Review. Nutrients, 10(9), 1186. https://doi.org/10.3390/nu10091186