1. Introduction
Accurate and detailed characterization of dietary intake is essential in nutrition research. However, assessment of intake is challenging because researchers must typically rely on self-reported methods, including 24-h dietary recalls, food-frequency questionnaires, and food records [
1]. Dietary intake data collected in this way are subject to bias stemming from systematic measurement error, which may result in inaccurate and imprecise estimates of dietary intake [
2,
3,
4]. Compared to other self-reporting instruments, 24-h dietary recalls capture intake with less bias, and have, therefore, emerged as a preferred means of dietary assessment [
3,
4]. Until recently, dietary recalls were typically conducted in person or via telephone using the computer-assisted Automated Multiple Pass Method. In this method, trained interviewers use a five-step multiple-pass approach to obtain details of all foods consumed from midnight to midnight the previous day, with manual data entry and auto-coding for most foods [
1]. The time and expense of collecting and analyzing data gathered in this way made 24-h recalls impractical for use in most large, community-based studies.
In 2009, the National Cancer Institute released the Automated Self-Administered 24-h Dietary Assessment Tool (ASA24): an automated, self-administered web-based tool that guides participants through completion of a 24-h dietary recall and automatically codes the data [
5]. The ASA24-Canada was released in 2014 and updated in 2016 [
6]. The self-administered and automated nature of the ASA24 has made collection of 24-h dietary recall data feasible in large studies. Nevertheless, despite its apparent advantages, eliminating contact with an interviewer may introduce additional challenges and different sources of error, with potential implications for the quantity and quality of the data that are collected.
A limited number of studies have discussed the usability of the ASA24 in relation to the quality of dietary intake data collected [
2,
7]. Although intakes were on average underreported on the ASA24 compared to more objective measures [
2,
7], the ASA24 nevertheless appeared to provide reasonable estimates of dietary intake comparable to, or better than, those derived from other self-report methods [
2,
7,
8,
9]. Usability related to the acceptability and feasibility of use of the ASA24 has been examined through retrospective questionnaires and by examining completion rates and intake data. Findings suggest that lack of internet access and/or lower levels of computer literacy may limit participation by some populations such as older adults, racial minorities, and those with lower levels of education [
8]. Participant workload may also pose a barrier with some participants finding it simpler and faster to interact with an interviewer rather than to search for and select foods themselves [
8]. Other limitations include difficulties finding exact matches for foods entered in search bars and a resulting tendency to select items that appear near the top of the list [
7,
10]. Overall, varying levels of receptivity to using the tool have been reported [
8,
9,
10].
Comparing intake data generated by the ASA24 to data generated by other measures can allow quantification of measurement error. However, such assessments cannot identify critical points in the reporting process where errors often originate. Similarly, although retrospective reports can identify socio-demographic characteristics of participants who find the ASA24 challenging to complete, the comprehensiveness, accuracy, and ultimate usefulness of these data is diminished by a reliance on participants’ ability to recall specific details of difficulties they encountered during a lengthy reporting process (~40 min [
9,
10]) and by the questionable assumption that participants can accurately pinpoint the errors they made as well as their cause. Moreover, the common use of closed-ended questions to query participants limits the ability to describe specific qualitative aspects of usability in detail.
In this respect, the science of Human Factors may offer new avenues for understanding how human–system interactions contribute to dietary measurement error, particularly those associated with novel technology-enabled assessments such as the ASA24. Human Factors as a science is concerned with the interaction between people and designed systems, and how human limitations and capabilities (e.g., limitations in human working memory), and the design of those systems (e.g., the number of digits an individual has to keep in working memory to complete a task), interact. The study of usability is a sub-discipline within the Human Factors field that seeks to understand the extent to which individuals can interact with a system to achieve a desired outcome with effectiveness (i.e., the accuracy and completeness with which specified users can achieve specified goals in particular environments), efficiency (i.e., the resources expended in relation to the accuracy and completeness of goals achieved), and satisfaction (i.e., the comfort and acceptability of a system to its users and other people affected by its use) [
11]. The construct of usability can also be extended to include concepts such as learnability, legibility, readability, and comprehension. A simpler way to frame the usability paradigm is to examine the relationship between usability, utility, and usefulness: a system may be technically able to deliver utility (i.e., it is technically functional) when used under perfect circumstances, but usability defines the required effort, and experience of, an individual to access that utility and ultimately interact with the system to produce a useful outcome [
12].
There are a variety of methods available to evaluate software usability. The present study follows the guidelines established by the International Organization for Standardization (ISO), where usability testing of a system engages representative users to complete representative tasks within the system in order to calculate measures of efficiency, effectiveness, and satisfaction [
13]. Usability testing also includes a methodology to identify usability issues and inform system design through the collection and analysis of qualitative data regarding users’ perspectives [
14]. Techniques such as the “think-aloud” method encourage users to verbalize cognitive processes while interacting with the system of interest [
15].
To our knowledge, no previous studies have involved structured usability testing of the ASA24 to obtain quantitative measures of efficiency and effectiveness, or to describe qualitative aspects of usability in detail. Therefore, the purpose of this study was to conduct a structured usability test of the ASA24 to generate quantitative measures of user performance (i.e., task success, task time, food item count, and usability issue frequency) and to examine qualitative aspects of usability (i.e., describe usability issues and user preferences) within a specific user population. The results of the usability test can provide insights that can be applied to configure and administer the ASA24 in a manner that makes the tool more usable for individuals completing a dietary recall, thereby increasing the quantity and quality of the dietary intake data that are collected.
4. Discussion
This study presents the results of a structured usability test of the ASA24 within a group of low-income, non-University and food insecure adults (85% female, average age 48.2 years) living in British Columbia, Canada. Detailed quantitative data describing how effectively (i.e., task success) and efficiently (i.e., completion time and usability issue count) participants were able to use the ASA24 were collected in real-time and analyzed. In addition, qualitative data were collected and analyzed to explain why individuals performed the way they did. This approach represents a considerable advance over previous studies that evaluated the usability of the ASA24 by relying on users to identify and report retrospectively problematic issues themselves. When considering why researchers, developers, and users of the ASA24 should be concerned about usability, it is helpful to consider the relationship between usability, utility, and usefulness [
12]. In the context of the ASA24, utility is the system’s technical capability to enable participants to independently search for, and accurately enter, dietary intake data in a manner that provides the information that researchers require. Usability refers to quantitative and qualitative aspects reflecting how individuals feel and behave while interacting with the ASA24 to access that utility. Usefulness can be considered from two perspectives: (1) how useful is the ASA24 to users who need to enter dietary intake data and (2) how useful is the ASA24 for nutrition researchers who rely on the data it captures. A system with “high usability” makes it easy for users to access its utility and will, therefore, provide data that are more useful for researchers. The purpose of performing a usability test of the ASA24 was to quantify user performance such that usability issues could be identified, quantified and qualitatively described in order to identify opportunities to improve the tool.
4.1. Findings and Recommendations to Enhance Effectiveness of the ASA24
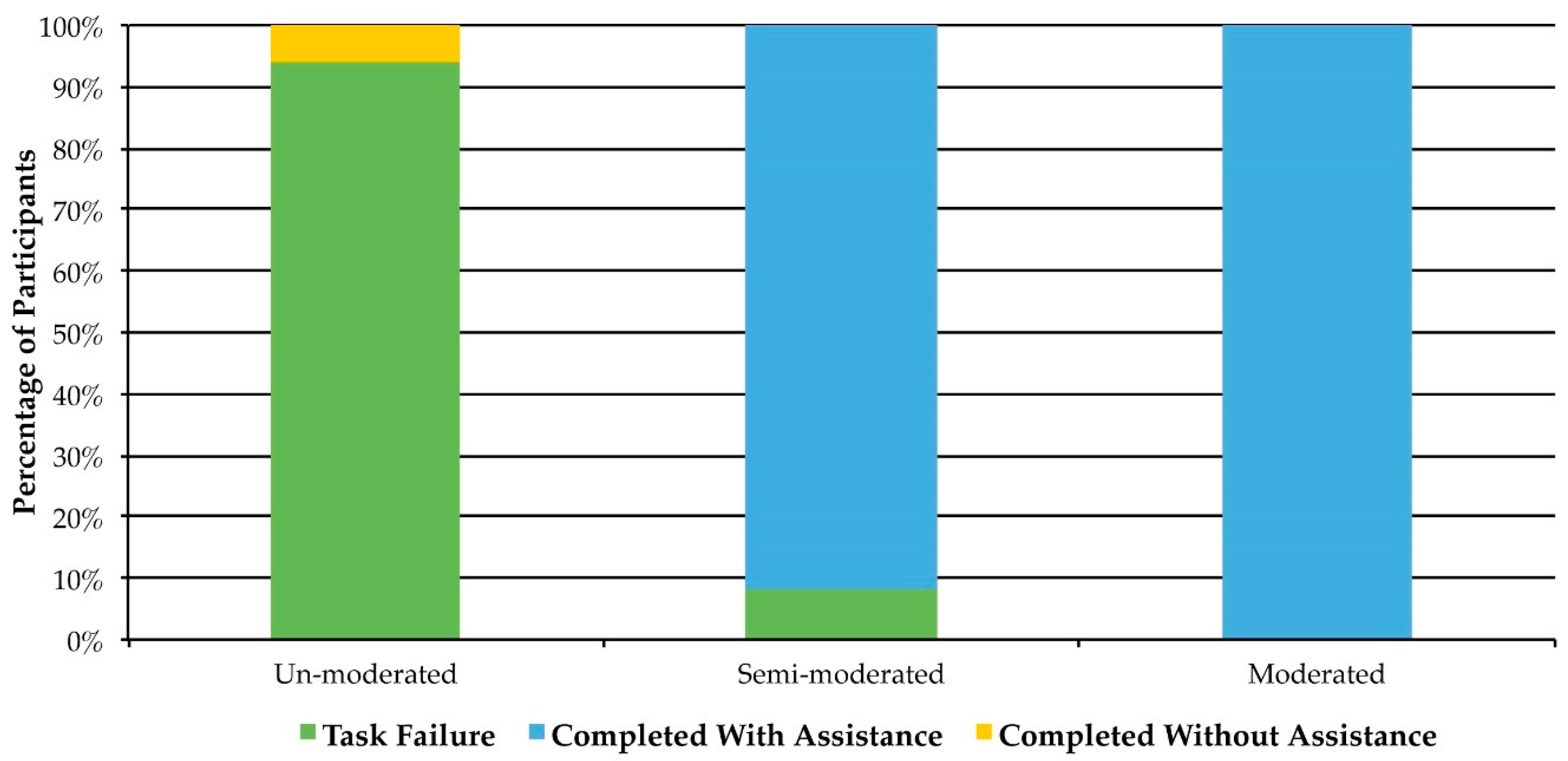
Only one of 17 participants in the unmoderated group successfully completed a dietary recall using the ASA24. Thirteen of the 17 failed to initiate the ASA24 altogether while the other three began the ASA24 but did not complete it. This task failure rate is concerning considering that the unmoderated group was the most representative of how individuals use the ASA24 outside the context of a usability test (i.e. without the support of a moderator). Time pressures may have prevented some participants from initiating the survey within the 36-h time window provided. Others completed the initial socio-demographic/health-related survey, but failed to initiate the ASA24, suggesting that problems logging into the ASA24 and/or participant fatigue led to task failure. Because these participants were not recorded or observed by the moderator it is not possible to identify specific factors that contributed to task failure. Notably, 58% of unmoderated participants were seniors, whereas less than half of those in the other groups were seniors. Among those who initiated, but did not fully complete the ASA24, general usability issues described in
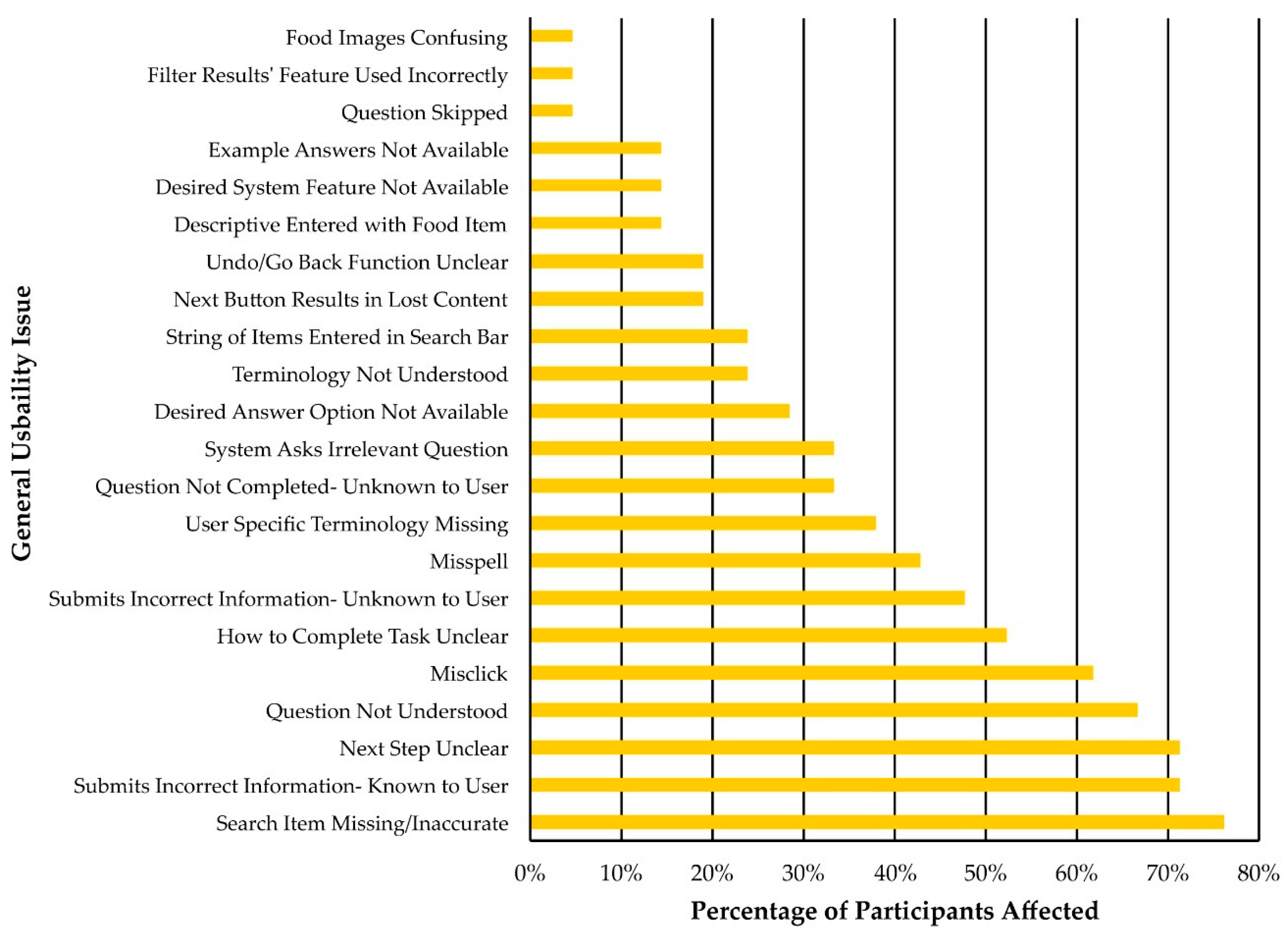
Section 3.7.1 can provide a sense of why they may have struggled successfully to complete the ASA24 independently. Of particular note was the common issue of participants being uncertain of the sequence of steps needed to complete a task (Next Step Unclear = 71.4% of participants (15 of 21), How to Complete Task Unclear = 52.4% of participants (11 of 21)). When participants were unclear on how to proceed with a task, it is likely that without the support of a moderator they may have exited the system or potentially entered data incorrectly.
Further study is needed to understand task failure in individuals using the ASA24 without the assistance of a moderator. Website analytics can provide a useful means of determining problematic sections of the ASA24. For example, a website’s Exit Rate is the percentage of individuals who leave a website from an individual page [
14]. The pages of the ASA24 with the highest Exit Rates will likely be associated with task failures. These data could be analyzed by ASA24 developers.
In the moderated and semi-moderated groups, 21 of 22 participants completed the dietary recall process successfully; however, all of these participants relied on assistance from a moderator at some point to assist them in navigating through usability issues. Whether or not this assistance was necessary for participants to complete a dietary recall is unclear; however, it is clear that the majority of participants benefitted from the support of a moderator. These quantitative data indicate that although the self-administered nature of the ASA24 facilitates data collection, it may ultimately result in low participation rates for groups who encounter frequent usability issues. As the complexity of interaction with a software system increases, it is reasonable to expect that a degree of technical support might be required to support individuals in using that system. None of the participants indicated that they had used the ASA24 before and, therefore, they can be considered novices, demonstrating performance typical of a population of untrained users. Based on these findings, researchers relying on the ASA24 to assess dietary intake in similar populations might expect novice users to require technical support to effectively use the tool for the first time. Thus, availability of on-demand technical assistance may be important to maximize the quantity and quality of data that are collected via the ASA24 and support participant retention.
4.2. Findings and Recommendations to Enhance Efficiency of Use of the ASA24
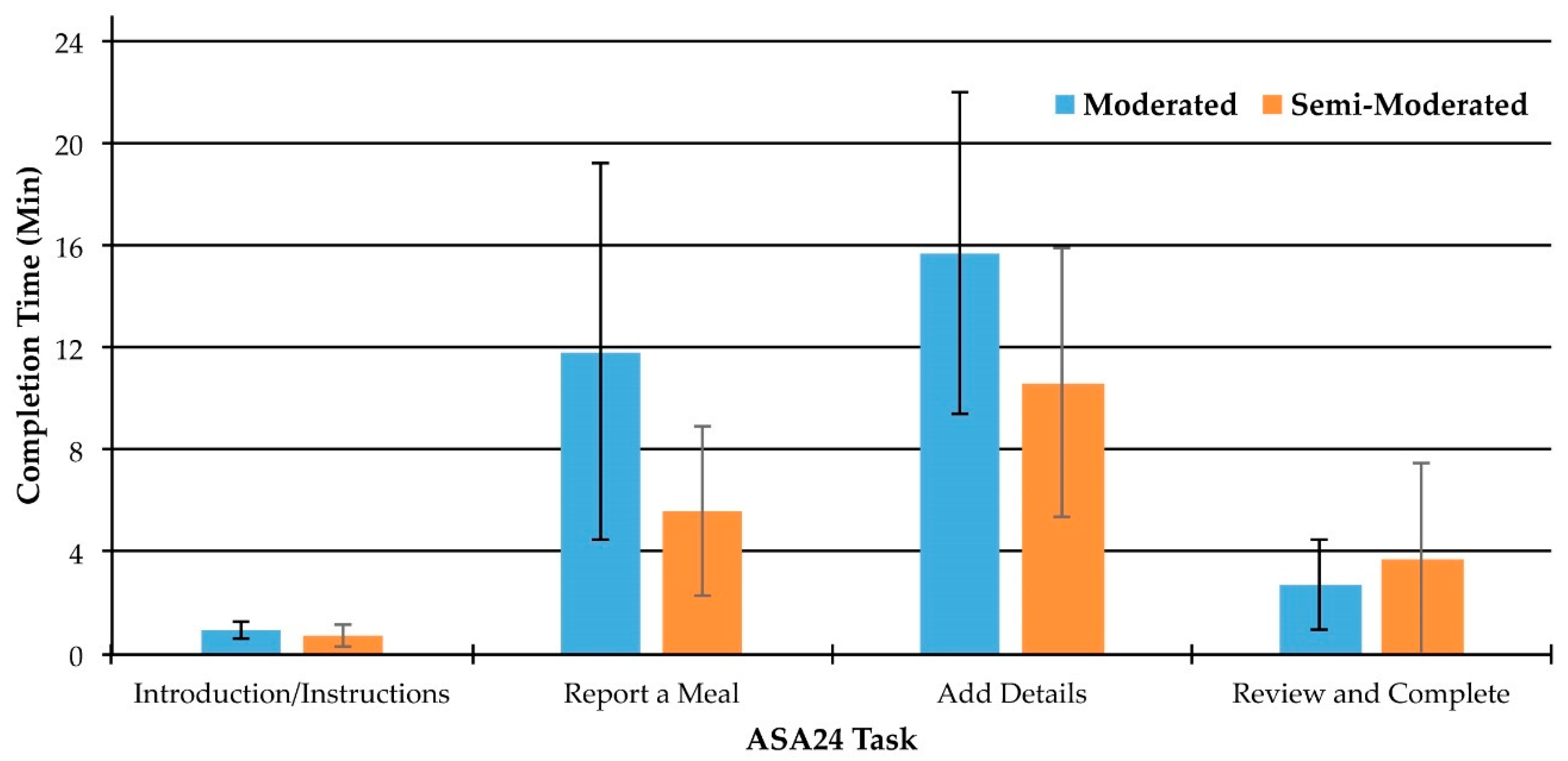
Participants in the present study completed the ASA24 more quickly (~27 min) than has been reported in other studies (~35 min [
9,
10]) despite the think-aloud procedure and interaction with a moderator. However, these times are comparable to the range reported on the ASA24 website (17–34 min). A strong correlation was observed between task time and food item count in the moderated and semi-moderated groups, with participants consuming an average of 11.5 items daily. Although other studies have not reported item count, an average of 11.5 items daily appears low. Given that the majority of participants had experienced moderate or severe food insecurity during the previous month, this low item count may be related to diminished food access and dietary diversity in our sample, potentially leading to lower ASA24 completion times relative to previous studies. Other characteristics, such as living alone or aging, may also be implicated due to reduced interest in, or capacity to cook. Individuals who are less inclined to cook may consume relatively simple meals with few ingredients. In addition to participant characteristics, the context of completion may also have been influential. Moderators assisted all participants in the moderated and semi-moderated groups at least once. Therefore, it is possible that the task completion times we observed are simply what can be expected when participants have support to use the tool.
Task time itself is a particularly meaningful usability metric when evaluating repetitive tasks [
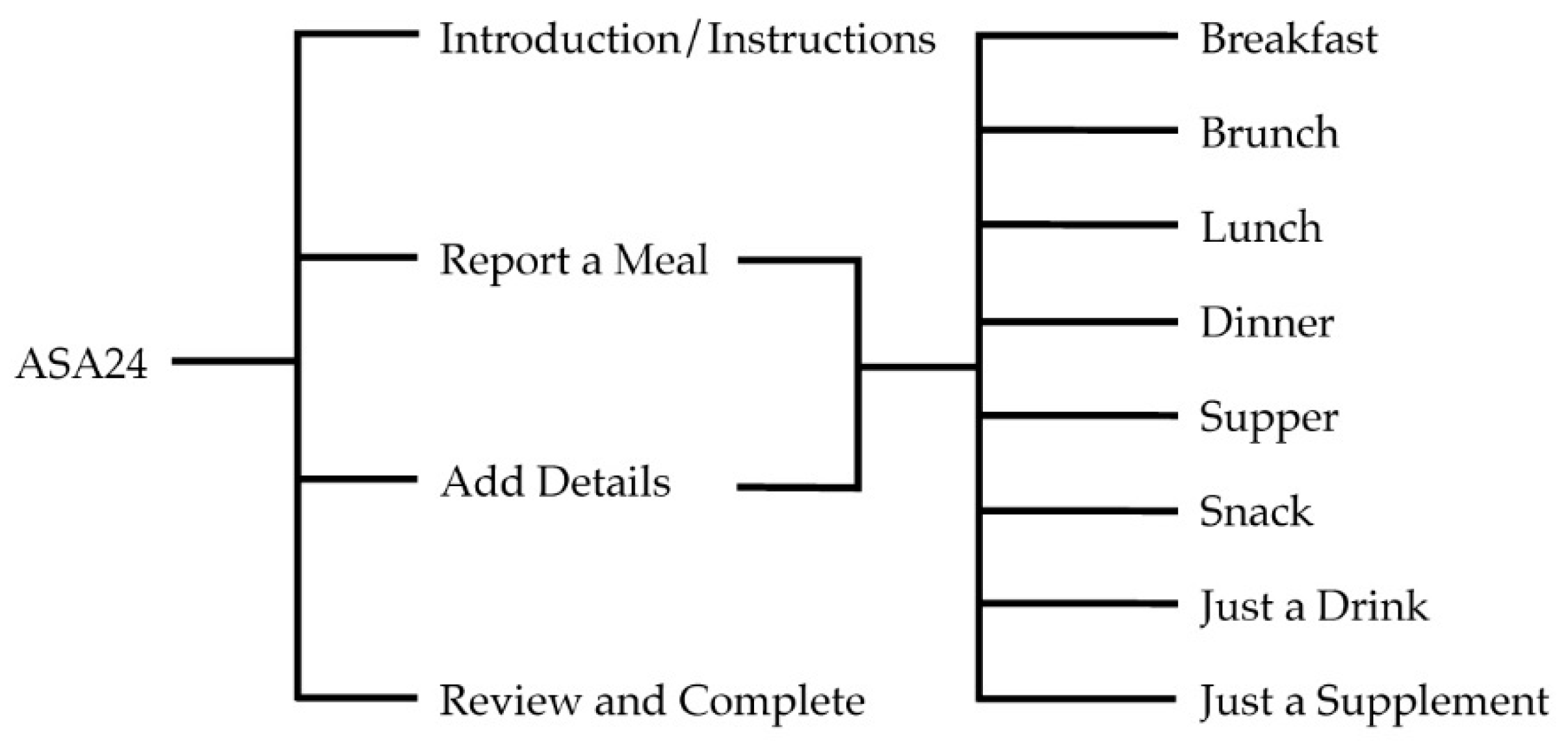
14]. If task time can be reduced for tasks that most participants must perform repeatedly, gains in efficiency will be achieved. The add details task was the most lengthy to complete for both the moderated and semi-moderated groups. Therefore, supporting users during the add details task will have the greatest impact with respect to enhancing efficiency of use of the ASA24.
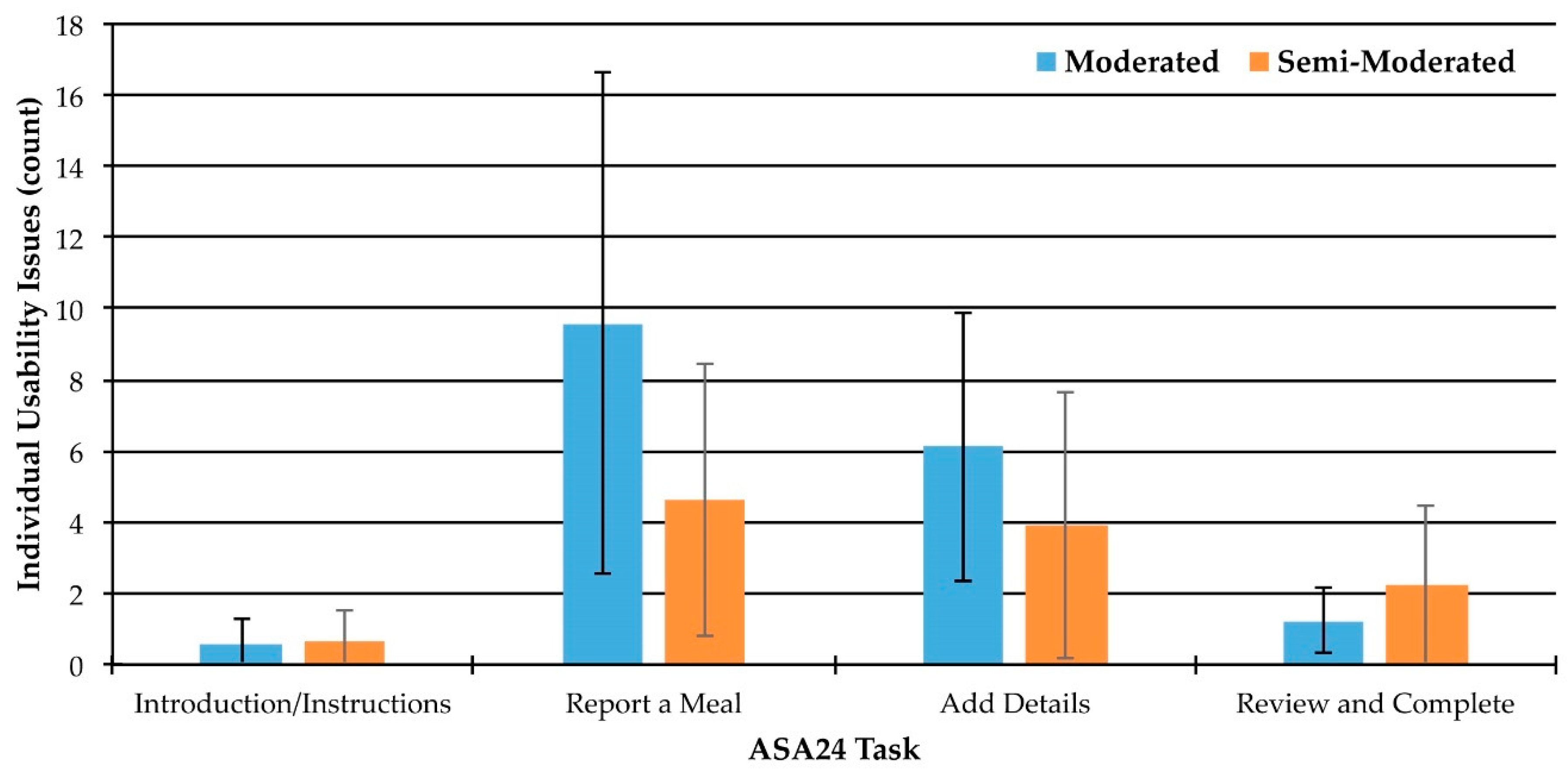
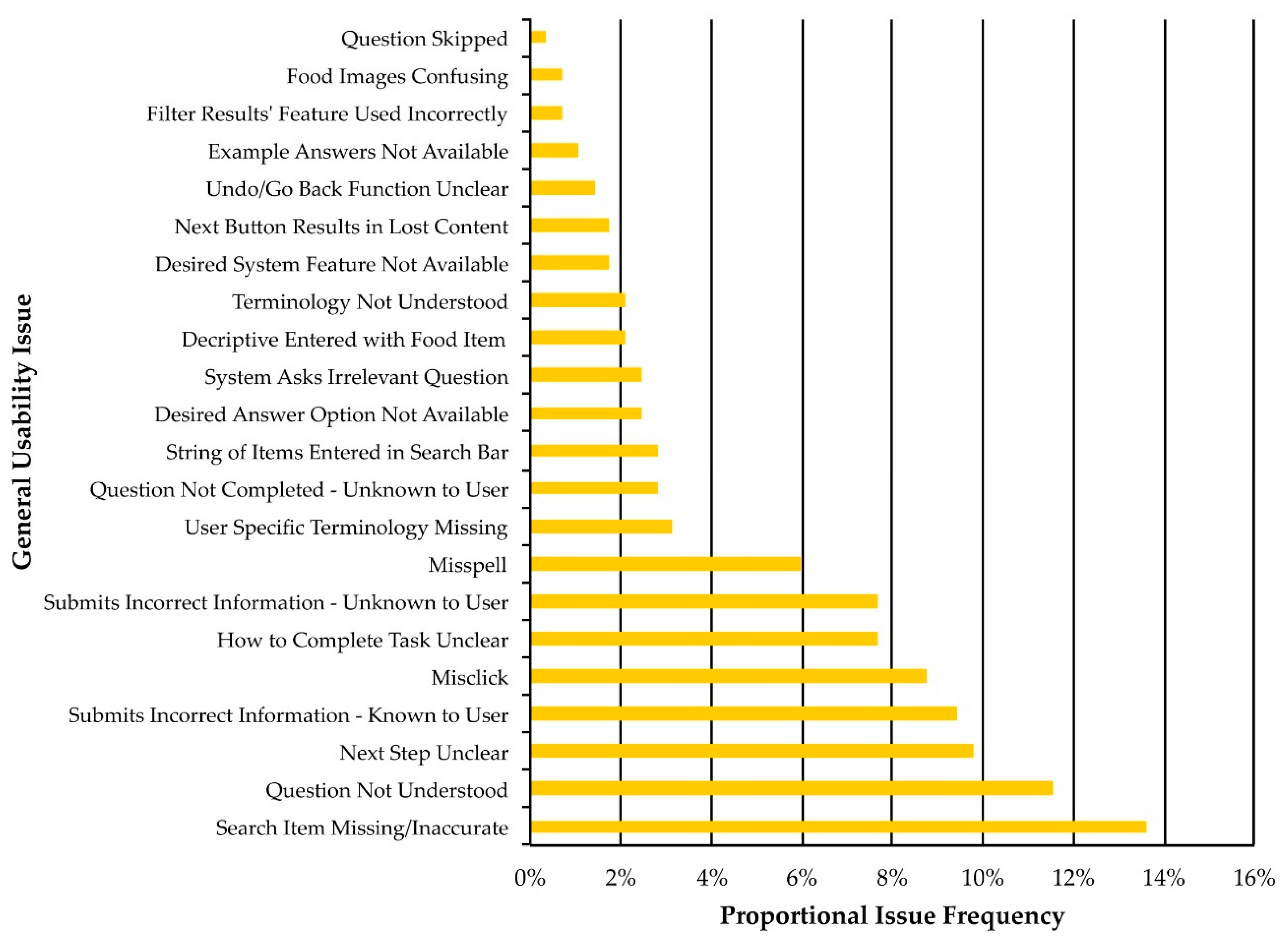
Another aspect of how efficiently the ASA24 can be used relates to the overall number and types of usability issues that participants encountered. Participants encountered an average of 13.7 individual usability issues per session. This is concerning considering that usability issues can diminish data quality and present opportunities for task failure or study dropout. The most common general usability issue, experienced by 76.2% of participants (16 of 21), was the inability to find a specific food item. Considering that one of the primary functions of the ASA24 is to enable users to record food intake independently, the prevalence of this usability issue is noteworthy. The inability to locate items was a key source of dietary measurement error. For instance, in the moderated and semi-moderated groups, 71.4% of participants (15 of 21) indicated that they knowingly entered incorrect information at least once, primarily because they were unable to find a specific food item using the search function.
Table 5 demonstrates that when this occurred users often selected other items (e.g., substituting steak for a chipotle steak sandwich), used the “I can’t find what I’m looking for” function (the impact of which was having to answer supplemental questions, some of which were irrelevant), or omitted the item entirely. The quantitative impact of this error is unclear, as the current study was not intended to quantify measurement error, but rather to examine its source in order to understand how to mitigate it. However, others have shown that energy intake in adults aged 50–74 years is underestimated by 15–17% on the ASA24 compared to recovery biomarkers, with no difference in mean protein and sodium densities [
2]. The current findings can provide complementary data to understand factors that contribute to misreporting of energy intake using the ASA24.
Additional search-related usability issues concern findings that participants often entered a string of items (e.g., “eggs and toast and water and coffee”) or entered additional descriptive information (e.g., “cold cereal”) into the search bar. Users will increasingly expect any web-based platform they interact with to provide them with “Google-Like” performance, likely with little appreciation for the investment that providing this functionality requires of the developer. Therefore, in addition to adding new food items to the ASA24 database, the intelligence of the ASA24 search algorithm could be improved to recognize plural forms of food items (e.g., the system returned a result for “taco” but not “tacos”) and to suggest potential matches when multiple words or descriptors are entered into the search bar.
Usability issues related to misclicking and misspelling were also prevalent. This could be a reflection of users not knowing what to do in the system, contributing to data errors or task failures (e.g., exiting the system). Additionally, entering an incorrectly spelled food item into the system can lead the user through additional irrelevant questions. This contributes to increased task times, and potentially decreased user satisfaction. This inefficiency could be quantified in subsequent usability tests using the metric of “lostness” [
33] by comparing the number of steps an individual performs to the minimum number of steps possible. This calculation would enable the impact of misclicks to be more thoroughly understood from an efficiency perspective. Some degree of user error (whether typos or accidental clicks) is outside the control of designers or researchers, however others can be addressed through relatively simple design changes (e.g., the visual differentiation or clarification of a button or text field’s function).
4.3. Findings and Recommendations to Enhance Satisfaction with the ASA24
Satisfaction in use is perhaps one of the most easily conceptualized aspects of usability; presumably, if someone is happy using a system then it is likely usable. Previous studies have asked participants to self-report their satisfaction with the ASA24, finding that the majority of participants had a favourable view of the system [
8,
34,
35,
36]. The current study examined specific system features that contributed to user satisfaction or dissatisfaction. Given these different outcomes, ability to compare our findings with those of others was limited. However, similar themes emerged in our study compared to others’, including frustrations about the time involved in completing a recall and how to proceed to the next step, not understanding how to use the search function, and not being able to find food items [
10]. Users who feel that a system is not designed to allow them to use it intuitively are unlikely to want to continue to use that system. One design approach to address satisfaction is to provide users with shortcuts that allow them to duplicate repetitive actions [
37]. Future usability tests could compare how easy individuals expect a task to be before attempting it (expectation score) to how easy they found it after completing it (experience score). When users expect a task to be easy to complete but then find it difficult (i.e., expectation score is much higher than the experience score), it is very likely to lead to dissatisfaction [
38]. This approach would help prioritize potential design changes specifically to improve satisfaction.
4.4. Findings and Recommendations to Enhance Comprehension of the ASA24
The second most frequent general usability issue identified was Question Not Understood, which accounted for 11.5% of all issues and was experienced by 66.7% of participants (14 of 21). Often, when participants were confused, it was observed that they had only partially processed the elements of the question being asked (e.g., mistaking which particular food item they were being asked about) or that they had not understood the specific words or phrasing of the question itself (e.g., general comments such as “I don’t know what this means.”). An individual who does not understand what the ASA24 is asking them to do, or who becomes confused by terminology or imagery, is likely to have difficulty using the tool to provide accurate information. A general approach to enhancing comprehension is to match the user’s mental model (e.g., ensuring language doesn’t exceed the user’s reading level, presenting visuals in a way that match the way the user consumes the food, requesting measurements of quantity that align with the user’s method of measurement, etc.). This can be challenging given the wide variability in individuals’ mental models, particularly for a tool such as the ASA24 that is intended to be used broadly across multiple populations. Two alternate design strategies that might be considered would be to: (1) allow users to customize the ASA24 to match their mental model (e.g., switching units from metric to imperial, alternative visual depictions of foods, customizable reading levels for text presentation), or (2) standardize the tool but ensure that it has been optimized to meet the needs of the majority of users through comparative comprehension testing.
4.6. User Characteristics and Usability Testing
Participants were recruited from a population participating in a nutrition coupon program and as such were primarily low-income, low- to mid-educated, and food insecure adults, many of whom were seniors. Older adults and those of a lower socioeconomic status may have lower computer literacy compared to the general population [
39] and it is, therefore, possible that some of the usability issues identified here may be particular to this sample. As we did not assess computer literacy, it is unclear whether this was an issue in our sample. Darajeh and Singh [
40] have summarized design recommendations to enhance usability for those with lower computer literacy, including creating simple layouts with limited clutter, providing user guides, reducing the use of complex terminology, creating simple navigation paths, using similar functions for different tasks, and including descriptive text for tool use. Dietary inequities and strategies to support optimal dietary patterns among older adults are significant concerns worldwide, and thus our findings can inform nutrition studies among these priority populations.
4.7. Strengths and Limitations
One of the strengths of the mixed methods approach was the ability to both quantify and qualitatively describe usability issues, providing a much more comprehensive and in-depth perspective of the usability of the ASA24. Moreover, the think-aloud procedures and inductive nature of the analyses enlarged the scope of investigation beyond researchers’ pre-determined questions and response options to uncover novel usability issues. The qualitative analysis had a sufficient sample size to reach a point of thematic saturation and we are, therefore, confident that the analysis uncovered the most salient usability issues in this particular sample.
The validity of a usability test is partially dependent on creating test conditions that reflect the actual conditions under which a user interacts with a system. The presence of a moderator may create a Hawthorne or Observer Effect in which participant behavior changes due to being observed, participants are overly reliant on assistance from a moderator to complete a task, or experience heightened sensitivity to usability issues. Having participants think-aloud may also create additional cognitive demand and thereby alter task performance. These factors could all contribute to a test scenario in which reported usability issues and performance metrics are not perfect representations of those that would have been encountered during actual use.
In addition, the definition of task failure as used in this study is specific to our methodological design. Participants were not given multiple attempts to complete the ASA24; if they failed to complete it upon their first attempt this was recorded as a task failure. However, the tool does allow participants to complete a dietary recall in multiple attempts. This study also looked at the ASA24 when used in combination with a socio-demographic/health-related survey. This survey was administered before the ASA24, which may have influenced participant behavior. For example, completing surveys prior to the ASA24 may create additional fatigue, affecting motivation to complete the ASA24. Finally, participants in the unmoderated group may have failed to complete the ASA24 for reasons unrelated to its usability (e.g., interruptions, variability in motivation). Researchers interested in using the ASA24 in a similar population should be aware of these potentially high participant drop-out rates.
4.8. Help Documentation and Training in Relation to Usability.
The ASA24 does provide a help guide for users and Best Practices information for researchers, in addition to the help feature embedded in the ASA24 [
41]. However, just one of the 22 participants observed in the moderated and semi-moderated groups accessed the ASA24’s help feature. Help functions do not, however, improve usability because they place the onus of efficient and effective system use on the user, increasing their workload rather than making system changes to enhance usability. Moreover, users often do not read support materials [
42]. One of the main benefits of conducting usability testing, or designing usable systems, is that the process will reduce costs associated with training and customer support [
43].









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}