Free Sugars Intake, Sources and Determinants of High Consumption among Australian 2-Year-Olds in the SMILE Cohort

 ,
,  , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
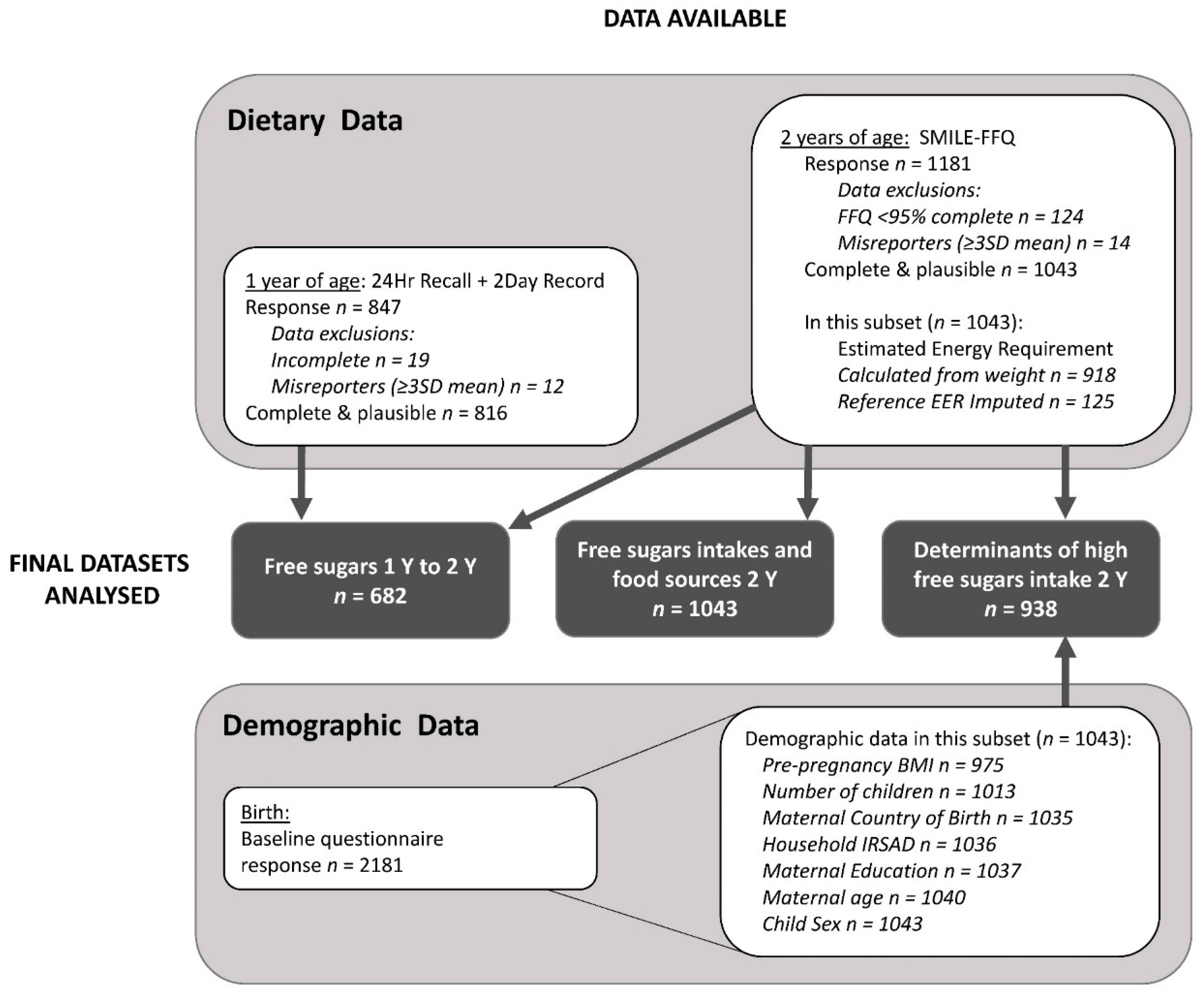
2.1. Recruitment and Data Source
2.2. Dietary Intake Data
2.3. Sociodemographic Data
2.4. Statistical Methods
3. Results
3.1. Participants
3.2. Free Sugars Intakes at 2 Years of Age
3.3. Food Group Contribution to Free Sugars Intakes
3.4. Changes in Free Sugars Consumption from 1 to 2 Years of Age
3.5. Determinants of High Free Sugars Intakes at 2 Years of Age
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Birch, L.L.; Doub, A.E. Learning to eat: Birth to age 2 y. Am. J. Clin. Nutr. 2014, 99, 723s–728s. [Google Scholar] [CrossRef] [PubMed]
- Nicklaus, S. Development of food variety in children. Appetite 2009, 52, 253–255. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Eat For Health: Australian Dietary Guidelines; No: N55; NHMRC: Canberra, Australia, 2013. Available online: http://www.eatforhealth.gov.au/guidelines (accessed on 6 December 2018).
- National Health and Medical Research Council. Infant Feeding Guidelines: Information for Health Workers; No: N56; NHMRC: Canberra, Australia, 2012. Available online: http://www.eatforhealth.gov.au/guidelines (accessed on 6 December 2018).
- World Health Organization. Guideline: Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Drewnowski, A.; Mennella, J.A.; Johnson, S.L.; Bellisle, F. Sweetness and Food Preference. J. Nutr. 2012, 142, 1142S–1148S. [Google Scholar] [CrossRef] [Green Version]
- Mennella, J.A. Ontogeny of taste preferences: Basic biology and implications for health. Am. J. Clin. Nutr. 2014, 99, 704s–711s. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Australian Health Survey: Consumption of Added Sugars, 2011–2012; No: 4364.0.55.011; ABS: Canberra, Australia, 2017. Available online: http://www.abs.gov.au (accessed on 16 January 2018).
- Food Standards Australia and New Zealand. Determining the Amount of Added Sugars and Free Sugars in Foods Listed in the AUSNUT 2011–13 Dataset. Available online: http://www.foodstandards.gov.au (accessed on 19 February 2018).
- Koh, G.; Scott, J.; Oddy, W.; Graham, K.; Binns, C. Exposure to non-core foods and beverages in the first year of life: Results from a cohort study. Nutr. Diet. 2010. [Google Scholar] [CrossRef]
- Byrne, R.; Magarey, A.; Daniels, L. Food and beverage intake in Australian children aged 12–16 months participating in the NOURISH and SAIDI studies. Aust. N. Z. J. Public Health 2014, 38, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.; Zhou, Y.; Perry, R.; Mauch, C.; Magarey, A. Beverage intake of Australian children and relationship with intake of fruit, vegetables, milk and body weight at 2, 3.7 and 5 years of age. Nutr. Diet. 2018. [Google Scholar] [CrossRef]
- Amezdroz, E.; Carpenter, L.; O’Callaghan, E.; Johnson, S.; Waters, E. Transition from milks to the introduction of solid foods across the first 2 years of life: Findings from an Australian birth cohort study. J. Hum. Nutr. Diet. 2015, 28, 375–383. [Google Scholar] [CrossRef]
- Bell, L.; Ullah, S.; Olds, T.; Magarey, A.; Leslie, E.; Jones, M.; Miller, M.; Cobiac, L. Prevalence and socio-economic distribution of eating, physical activity and sedentary behaviour among South Australian children in urban and rural communities: Baseline findings from the OPAL evaluation. Public Health 2016, 140, 196–205. [Google Scholar] [CrossRef]
- Conn, J.A.; Davies, M.J.; Walker, R.B.; Moore, V.M. Food and nutrient intakes of 9-month-old infants in Adelaide, Australia. Public Health Nutr. 2009, 12, 2448–2456. [Google Scholar] [CrossRef]
- Scott, J.; Davey, K.; Ahwong, E.; Devenish, G.; Ha, D.; Do, L. A Comparison by Milk Feeding Method of the Nutrient Intake of a Cohort of Australian Toddlers. Nutrients 2016, 8, 501. [Google Scholar] [CrossRef] [PubMed]
- Webb, K.; Rutihauser, I.; Knezevic, N. Foods, nutrients and portions consumed by a sample of Australian children aged 16-24 months. Nutr. Diet. 2008, 65, 56–65. [Google Scholar] [CrossRef]
- Atkins, L.A.; McNaughton, S.A.; Campbell, K.J.; Szymlek-Gay, E.A. Iron intakes of Australian infants and toddlers: Findings from the Melbourne Infant Feeding, Activity and Nutrition Trial (InFANT) Program. Br. J. Nutr. 2016, 115, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Spence, A.C.; Campbell, K.J.; Lioret, S.; McNaughton, S.A. Early Childhood Vegetable, Fruit, and Discretionary Food Intakes Do Not Meet Dietary Guidelines, but Do Show Socioeconomic Differences and Tracking over Time. J. Acad. Nutr. Diet. 2018, 118, 1634–1643.e1. [Google Scholar] [CrossRef]
- Cameron, A.J.; Ball, K.; Pearson, N.; Lioret, S.; Crawford, D.A.; Campbell, K.; Hesketh, K.; McNaughton, S.A. Socioeconomic variation in diet and activity-related behaviours of Australian children and adolescents aged 2–16 years. Pediatr. Obes. 2012, 7, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Peeters, A.; Gearon, E.; Backholer, K. Contribution of discretionary food and drink consumption to socio-economic inequalities in children’s weight: Prospective study of Australian children. Int. J. Epidemiol. 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Devenish, G.; Ytterstad, E.; Begley, A.; Do, L.; Scott, J. Intake, sources, and determinants of free sugars intake in Australian children aged 12-14 months. Matern. Child Nutr. 2018, e12692. [Google Scholar] [CrossRef]
- Do, L.G.; Scott, J.A.; Thomson, W.M.; Stamm, J.W.; Rugg-Gunn, A.J.; Levy, S.M.; Wong, C.; Devenish, G.; Ha, D.H.; Spencer, A.J. Common risk factor approach to address socioeconomic inequality in the oral health of preschool children—A prospective cohort study. BMC Public Health 2014, 14, 429. [Google Scholar] [CrossRef]
- Scheil, W.; Jolly, K.; Scott, J.; Catcheside, B.; Sage, L.; Kennare, R. Pregnancy Outcome in South Australia 2013; Pregnancy Outcome Unit, SA Health, Government of South Australia: Adelaide, Australia, 2015. [Google Scholar]
- World Health Organization. Physical Status: Use and Interpretation of Anthropometry; WHO Expert Committee on Physical Status: Geneva, Switzerland, 1995. [Google Scholar]
- Devenish, G.; Mukhtar, A.; Begley, A.; Do, L.; Scott, J. Development and Relative Validity of a Food Frequency Questionnaire to Assess Intakes of Total and Free Sugars in Australian Toddlers. Int. J. Environ. Res. Public Health 2017, 14, 1361. [Google Scholar] [CrossRef]
- Louie, J.C.Y.; Moshtaghian, H.; Boylan, S.; Flood, V.M.; Rangan, A.M.; Barclay, A.W.; Brand-Miller, J.C.; Gill, T.P. A systematic methodology to estimate added sugar content of foods. Eur. J. Clin. Nutr. 2015, 69, 154–161. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand; NHMRC: Canberra, Australia, 2006.
- Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Australian Bureau of Statistics. Australian Health Survey Users’ Guide, 2011–2013: 24-Hour Dietary Recall; No: 4363.0.55.001; ABS: Canberra, Australia, 2014. Available online: http://www.abs.gov.au (accessed on 21 September 2018).
- Thompson, F.E.; Subar, A.F. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease, 3rd ed.; Coulston, A.M., Boushey, C., Ferruzzi, M., Eds.; Academic Press: London, UK, 2013. [Google Scholar]
- Food Standards Australia and New Zealand. AUSNUT 2011-13—Australian Food Composition Database; FSANZ: Canberra, Australia, 2014.
- Harttig, U.; Haubrock, J.; Knuppel, S.; Boeing, H. The MSM program: Web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65 (Suppl. 1), S87–S91. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas (SEIFA); No: 2033.0.55.001; ABS: Canberra, Australia, 2013. Available online: http://www.abs.gov.au (accessed on 6 March 2018).
- Masson, L.F.; McNeill, G.; Tomany, J.O.; Simpson, J.A.; Peace, H.S.; Wei, L.; Grubb, D.A.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire: Use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Nielsen Scantrack. The George Institute. Low Sugar Hitting a Sweet Spot in Australia; The Nielsen Company: New York, NY, USA, 2018. [Google Scholar]
- Singerman, D. The Shady History of Big Sugar. The New York Times. 16 September 2016. Available online: https://www.nytimes.com/2016/09/17/opinion/the-shady-history-of-big-sugar.html (accessed on 6 December 2018).
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results—Foods and Nutrients, 2011–2012; No: 4364.0.55.007; ABS: Canberra, Australia, 2015. Available online: http://www.abs.gov.au (accessed on 6 December 2018).
- North, K.; Emmett, P. Multivariate analysis of diet among three-year-old children and associations with socio-demographic characteristics. The Avon Longitudinal Study of Pregnancy and Childhood (ALSPAC) Study Team. Eur. J. Clin. Nutr. 2000, 54, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Durao, C.; Severo, M.; Oliveira, A.; Moreira, P.; Guerra, A.; Barros, H.; Lopes, C. Association of maternal characteristics and behaviours with 4-year-old children’s dietary patterns. Matern. Child Nutr. 2017, 13. [Google Scholar] [CrossRef]
- Bell, L.K.; Golley, R.K.; Daniels, L.; Magarey, A.M. Dietary patterns of Australian children aged 14 and 24 months, and associations with socio-demographic factors and adiposity. Eur. J. Clin. Nutr. 2013, 67, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Cameron, A.J.; McNaughton, S.A.; Crawford, D.; Spence, A.C.; Hesketh, K.; Campbell, K.J. Association between maternal education and diet of children at 9 months is partially explained by mothers’ diet. Matern. Child Nutr. 2015, 11, 936–947. [Google Scholar] [CrossRef]
- Backholer, K.; Spencer, E.; Gearon, E.; Magliano, D.J.; McNaughton, S.A.; Shaw, J.E.; Peeters, A. The association between socio-economic position and diet quality in Australian adults. Public Health Nutr. 2016, 19, 477–485. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.R.; de Lauzon-Guillain, B.; Holub, S.C.; Leporc, E.; Charles, M.A. Child and parent characteristics related to parental feeding practices. A cross-cultural examination in the US and France. Appetite 2009, 52, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Kiwanuka, S.N.; Åstrøm, A.N.; Trovik, T.A. Sugar snack consumption in Ugandan schoolchildren: Validity and reliability of a food frequency questionnaire. Community Dent. Oral Epidemiol. 2006, 34, 372–380. [Google Scholar] [CrossRef]
- Gulati, S.; Misra, A.; Colles, S.L.; Kondal, D.; Gupta, N.; Goel, K.; Bansal, S.; Mishra, M.; Madkaikar, V.; Bhardwaj, S. Dietary intakes and familial correlates of overweight/obesity: A four-cities study in India. Ann. Nutr. Metab. 2013, 62, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Yothasamut, J.; Camfield, L.; Pfeil, M. Practices and values regarding milk consumption among pre-schoolers in Bangkok. Int. J. Qualitative Stud. Health Well-Being 2018, 13, 1461515. [Google Scholar] [CrossRef] [PubMed]
- Holmboe-Ottesen, G.; Wandel, M. Changes in dietary habits after migration and consequences for health: A focus on South Asians in Europe. Food Nutr. Res. 2012, 56. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.C.; Naidoo, N.; Ferzacca, S.; Reddy, G.; Van Dam, R.M. The role of women in food provision and food choice decision-making in Singapore: A case study. Ecol. Food Nutr. 2014, 53, 658–677. [Google Scholar] [CrossRef]
- Satia, J.A. Dietary acculturation and the nutrition transition: An overview. Appl. Physiol. Nutr. Metab. 2010, 35, 219–223. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the Commission on Ending Childhood Obesity; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- IBISWorld Australia. IBISWorld Industry Report OD5058 Baby Food Manufacturing in Australia; IBISWorld Australia: Melbourne, Australia, 2017. [Google Scholar]
- Rayner, M.; Wood, A.; Lawrence, M.; Mhurchu, C.N.; Albert, J.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; Kumanyika, S.; et al. Monitoring the health-related labelling of foods and non-alcoholic beverages in retail settings. Obes. Rev. 2013, 14, 70–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulker, C.E.; Trapp, G.S.A.; Scott, J.A.; Pollard, C.M. Alignment of Supermarket Own Brand Foods’ Front-of-Pack Nutrition Labelling with Measures of Nutritional Quality: An Australian Perspective. Nutrients 2018, 10, 1465. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. Australia New Zealand Food Standards Code—Standard 2.9.2—Food for Infants; No: F2017C00334; FSANZ: Canberra, Australia, 2017. Available online: https://www.legislation.gov.au/Details/F2017C00334 (accessed on 13 March 2018).
- Ha, D.H.; Do, L.G.; Spencer, A.J.; Thomson, W.M.; Golley, R.K.; Rugg-Gunn, A.J.; Levy, S.M.; Scott, J.A. Factors Influencing Early Feeding of Foods and Drinks Containing Free Sugars—A Birth Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1270. [Google Scholar] [CrossRef]
- National Institutes of Health; National Cancer Institute. Dietary Assessment Primer. Available online: http://dietassessmentprimer.cancer.gov (accessed on 13 March 2018).
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Ortiz-Andrellucchi, A.; Henríquez-Sánchez, P.; Sánchez-Villegas, A.; Peña-Quintana, L.; Mendez, M.; Serra-Majem, L. Dietary assessment methods for micronutrient intake in infants, children and adolescents: A systematic review. Br. J. Nutr. 2010, 102, S87–S117. [Google Scholar] [CrossRef]
- Livingstone, M.B.; Robson, P.J.; Wallace, J.M. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92 (Suppl. 2), S213–S222. [Google Scholar] [CrossRef] [Green Version]
- Radnitz, C.; Todd, L.E. Social desirability may explain why some caregivers of overweight children report less frequent high calorie food intake. Eat. Behav. 2016, 23, 48–51. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All Participants (n = 2181) | Responders 2 Years (n = 1043) | Non-Responders 2 Years (n = 1138) | p a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | mean | SD | n | mean | SD | n | mean | SD | ||
| Mother’s age at birth (years) | 2101 | 29.9 | 5.4 | 1040 | 30.6 | 5.0 | 1061 | 29.2 | 5.7 | <0.001 |
| Total number of children | 1867 | 1.8 | 1.0 | 1013 | 1.8 | 0.9 | 854 | 1.9 | 1.0 | 0.012 |
| Child’s birthweight (g) | 2083 | 3356 | 572 | 1032 | 3393 | 547 | 1051 | 3319 | 593 | 0.003 |
| n | % | n | % | n | % | |||||
| Mother’s age at birth (years) | <0.001 | |||||||||
| <25 | 336 | 16.0 | 105 | 10.1 | 231 | 21.8 | ||||
| 25–34.99 | 1353 | 64.4 | 717 | 68.9 | 636 | 59.9 | ||||
| ≥35 | 412 | 19.6 | 218 | 21.0 | 194 | 18.3 | ||||
| Mother’s pre-pregnancy BMI (kg/m2) | 0.274 | |||||||||
| <25 | 1086 | 56.2 | 565 | 57.9 | 521 | 54.4 | ||||
| 25–29.99 (overweight) | 455 | 23.5 | 218 | 22.4 | 237 | 24.7 | ||||
| ≥30 (obese) | 392 | 20.3 | 192 | 19.7 | 200 | 20.9 | ||||
| Mother’s Country of Birth | <0.001 | |||||||||
| Australia or New Zealand | 1453 | 69.3 | 755 | 72.9 | 698 | 65.7 | ||||
| Other | 644 | 30.7 | 280 | 27.1 | 364 | 34.3 | ||||
| Mother’s Education | <0.001 | |||||||||
| high school/vocational | 1136 | 54.0 | 451 | 43.5 | 685 | 64.2 | ||||
| some university and above | 968 | 46.0 | 586 | 56.5 | 382 | 35.8 | ||||
| IRSAD | <0.001 | |||||||||
| Deciles 1–2 (most disadvantaged) | 462 | 22.2 | 172 | 16.6 | 290 | 27.8 | ||||
| Deciles 3–4 | 446 | 21.4 | 214 | 20.7 | 232 | 22.2 | ||||
| Deciles 5–6 | 390 | 18.7 | 210 | 20.3 | 180 | 17.2 | ||||
| Deciles 7–8 | 385 | 18.5 | 199 | 19.2 | 186 | 17.8 | ||||
| Deciles 9–10 (most advantaged) | 398 | 19.1 | 241 | 23.3 | 157 | 15.0 | ||||
| Total number of children | 0.111 | |||||||||
| 1 | 863 | 46.2 | 480 | 47.4 | 383 | 44.8 | ||||
| 2 | 670 | 35.9 | 369 | 36.4 | 301 | 35.2 | ||||
| ≥3 | 334 | 17.9 | 164 | 16.2 | 170 | 19.9 | ||||
| Child’s sex | 0.579 | |||||||||
| Male | 1146 | 52.7 | 556 | 53.3 | 590 | 52.1 | ||||
| Female | 1029 | 47.3 | 487 | 46.7 | 542 | 47.9 | ||||
| Median | Percentile | Range | ||
|---|---|---|---|---|
| 25th | 75th | |||
| Free Sugars (g/day) | 22.5 | 12.8 | 37.7 | 0.3–140.7 |
| Tertile 1 (low) | 10.6 | 7.4 | 13.0 | 0.3–15.8 |
| Tertile 2 (mid) | 22.7 | 19.0 | 26.4 | 15.81–31.6 |
| Tertile 3 (high) | 47.2 | 38.0 | 66.7 | 31.61–140.7 |
| Total Sugars (g/day) | 77.5 | 56.0 | 105.3 | 9.4–294.8 |
| Estimated Energy Requirement (kJ/day) | 4730 | 4357 | 5214 | 2644–8193 |
| Percentage of Estimated Energy Requirement from Free Sugars (%) | 8.0 | 4.6 | 13.2 | 0.1–61.3 |
| All Participants (n = 1043) | Consumers | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Food group a | mean ± SD free sugars (g) | % contribution to free sugars | n (%) | mean ± SD free sugars (g) | |||||
| Non-alcoholic beverages | 4.7 | ± | 9.7 | 15.9 | 1037 | (99.4) | 4.7 | ± | 9.7 |
| Fruit and vegetable juices, and drinks | 3.1 | ± | 7.3 | 10.7 | 590 | (56.6) | 5.5 | ± | 9.0 |
| Cordials | 0.8 | ± | 3.8 | 2.6 | 179 | (17.2) | 4.5 | ± | 8.4 |
| Soft drinks, flavored mineral waters | 0.2 | ± | 1.3 | 0.8 | 147 | (14.1) | 1.7 | ± | 3.1 |
| Other beverage flavorings | 0.3 | ± | 1.7 | 0.9 | 246 | (23.6) | 1.2 | ± | 3.5 |
| Cereals and cereal products | 1.1 | ± | 2.1 | 3.7 | 953 | (91.4) | 1.2 | ± | 2.1 |
| Breakfast cereals, ready to eat | 1.1 | ± | 2.1 | 3.7 | 884 | (84.8) | 1.3 | ± | 2.2 |
| Cereal based products and dishes | 5.5 | ± | 6.9 | 18.8 | 1028 | (98.6) | 5.6 | ± | 6.9 |
| Sweet biscuits | 2.2 | ± | 3.5 | 7.4 | 908 | (87.1) | 2.5 | ± | 3.6 |
| Savory biscuits | 0.3 | ± | 0.5 | 0.9 | 947 | (90.8) | 0.3 | ± | 0.5 |
| Cakes, muffins, doughnuts, cake-type desserts b | 2.2 | ± | 4.2 | 7.5 | 674 | (64.6) | 3.4 | ± | 4.8 |
| Batter-based products, scones, sweet breads b | 0.8 | ± | 1.6 | 2.6 | 468 | (44.9) | 1.7 | ± | 2.0 |
| Fruit products and dishes c | 0.3 | ± | 1.2 | 1.2 | 1029 | (98.7) | 0.3 | ± | 1.2 |
| Milk products and dishes | 4.8 | ± | 7.1 | 16.4 | 1015 | (97.3) | 4.9 | ± | 7.2 |
| Yogurt | 2.6 | ± | 5.2 | 8.8 | 787 | (75.5) | 3.4 | ± | 5.8 |
| Frozen milk products | 0.9 | ± | 1.9 | 3.1 | 605 | (58.0) | 1.5 | ± | 2.2 |
| Custards | 0.9 | ± | 3.3 | 2.9 | 325 | (31.2) | 2.8 | ± | 5.5 |
| Flavored milks and milkshakes | 0.4 | ± | 1.5 | 1.2 | 211 | (20.2) | 1.8 | ± | 3.0 |
| Dairy and meat substitutes | 1.7 | ± | 4.9 | 5.8 | 438 | (42.0) | 4.0 | ± | 6.9 |
| Dairy milk substitutes, unflavored | 1.2 | ± | 3.8 | 4.2 | 245 | (23.5) | 5.2 | ± | 6.5 |
| Savory sauces and condiments | 0.5 | ± | 1.0 | 1.8 | 792 | (75.9) | 0.7 | ± | 1.2 |
| Gravies and savory sauces | 0.5 | ± | 0.9 | 1.6 | 758 | (72.7) | 0.6 | ± | 1.0 |
| Sugar products and dishes | 3.4 | ± | 5.7 | 11.7 | 846 | (81.1) | 4.2 | ± | 6.0 |
| Sugar, honey and syrups | 1.5 | ± | 3.5 | 5.1 | 609 | (58.4) | 2.6 | ± | 4.3 |
| Jam and lemon spreads, chocolate spreads, sauces | 1.0 | ± | 2.7 | 3.3 | 541 | (51.9) | 1.8 | ± | 3.5 |
| Dishes and products other than confectionery where sugar is the major component | 1.0 | ± | 2.8 | 3.3 | 450 | (43.1) | 2.2 | ± | 3.9 |
| Confectionery and cereal, nut, fruit, seed bars | 2.8 | ± | 3.9 | 9.4 | 871 | (83.5) | 3.3 | ± | 4.0 |
| Chocolate and chocolate-based confectionery | 1.3 | ± | 2.5 | 4.6 | 719 | (68.9) | 1.9 | ± | 2.8 |
| Muesli or cereal style bars | 0.7 | ± | 1.6 | 2.4 | 404 | (38.7) | 1.8 | ± | 2.2 |
| Other confectionery | 0.7 | ± | 1.7 | 2.5 | 439 | (42.1) | 1.7 | ± | 2.4 |
| Infant formula and foods | 4.3 | ± | 5.9 | 14.9 | 770 | (73.8) | 5.9 | ± | 6.2 |
| Infant and Toddler formula | 1.1 | ± | 3.3 | 3.8 | 150 | (14.4) | 7.7 | ± | 5.1 |
| Infant foods | 2.8 | ± | 4.4 | 9.7 | 658 | (63.1) | 4.5 | ± | 4.8 |
| Infant custards or yogurts | 2.8 | ± | 4.4 | 9.7 | 658 | (63.1) | 4.5 | ± | 4.8 |
| Infant drinks d | 0.4 | ± | 1.7 | 1.3 | 155 | (14.9) | 2.7 | ± | 3.8 |
| Infant fruit juices | 0.4 | ± | 1.7 | 1.3 | 155 | (14.9) | 2.7 | ± | 3.8 |
| Free Sugars at 2 Years | ||||
|---|---|---|---|---|
| Low | Mid | High | ||
| Free Sugars at 1 Year | Low | 118 (17.3%) | 72 (10.6%) | 37 (5.4%) |
| Mid | 82 (12.0%) | 76 (11.1%) | 70 (10.3%) | |
| High | 49 (7.2%) | 67 (9.8%) | 111 (16.3%) | |
| Free Sugars Highest Tertile | Free Sugars Intake ≥ 10%EER | |||
|---|---|---|---|---|
| PR | 95% CI | PR | 95% CI | |
| Mother’s age at birth (years) | ||||
| <25 | 1.50 | 1.07–2.12 | 1.42 | 1.05–1.91 |
| 25–34.99 | 1.06 | 0.84–1.34 | 1.05 | 0.85–1.29 |
| ≥35 | 1.00 | 1.00 | ||
| Mother’s pre-pregnancy BMI | ||||
| <25 Healthy weight or below | 1.00 | 1.00 | ||
| 25–29.99 Overweight | 1.06 | 0.85–1.32 | 1.03 | 0.85–1.24 |
| ≥30 Obese | 0.95 | 0.74–1.23 | 0.92 | 0.73–1.17 |
| Mother’s Country of Birth | ||||
| Other | 1.58 | 1.28–1.94 | 1.59 | 1.33–1.90 |
| Australia, New Zealand | 1.00 | 1.00 | ||
| Mother’s Education | ||||
| University | 0.83 | 0.68–1.01 | 0.82 | 0.69–0.98 |
| High school/vocational | 1.00 | 1.00 | ||
| IRSAD | ||||
| Deciles 1–2 (most disadvantaged) | 1.58 | 1.19–2.10 | 1.44 | 1.13–1.84 |
| Deciles 3–4 | 1.40 | 1.06–1.85 | 1.34 | 1.06–1.70 |
| Deciles 5–6 | 1.03 | 0.76–1.40 | 0.98 | 0.75–1.29 |
| Deciles 7–8 | 1.00 | 0.73–1.38 | 0.95 | 0.72–1.25 |
| Deciles 9–10 (most advantaged) | 1.00 | 1.00 | ||
| Total number of children | ||||
| 1 | 1.00 | 1.00 | ||
| 2 | 1.28 | 1.04–1.57 | 1.22 | 1.02–1.47 |
| ≥3 | 1.52 | 1.17–1.97 | 1.39 | 1.11–1.76 |
| Child’s sex | ||||
| Female | 0.93 | 0.77–1.11 | 0.98 | 0.83–1.15 |
| Male | 1.00 | 1.00 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devenish, G.; Golley, R.; Mukhtar, A.; Begley, A.; Ha, D.; Do, L.; Scott, J.A. Free Sugars Intake, Sources and Determinants of High Consumption among Australian 2-Year-Olds in the SMILE Cohort. Nutrients 2019, 11, 161. https://doi.org/10.3390/nu11010161
Devenish G, Golley R, Mukhtar A, Begley A, Ha D, Do L, Scott JA. Free Sugars Intake, Sources and Determinants of High Consumption among Australian 2-Year-Olds in the SMILE Cohort. Nutrients. 2019; 11(1):161. https://doi.org/10.3390/nu11010161
Chicago/Turabian StyleDevenish, Gemma, Rebecca Golley, Aqif Mukhtar, Andrea Begley, Diep Ha, Loc Do, and Jane A. Scott. 2019. "Free Sugars Intake, Sources and Determinants of High Consumption among Australian 2-Year-Olds in the SMILE Cohort" Nutrients 11, no. 1: 161. https://doi.org/10.3390/nu11010161
APA StyleDevenish, G., Golley, R., Mukhtar, A., Begley, A., Ha, D., Do, L., & Scott, J. A. (2019). Free Sugars Intake, Sources and Determinants of High Consumption among Australian 2-Year-Olds in the SMILE Cohort. Nutrients, 11(1), 161. https://doi.org/10.3390/nu11010161