A High Adherence to Six Food Targets of the Mediterranean Diet in the Late First Trimester is Associated with a Reduction in the Risk of Materno-Foetal Outcomes: The St. Carlos Gestational Diabetes Mellitus Prevention Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
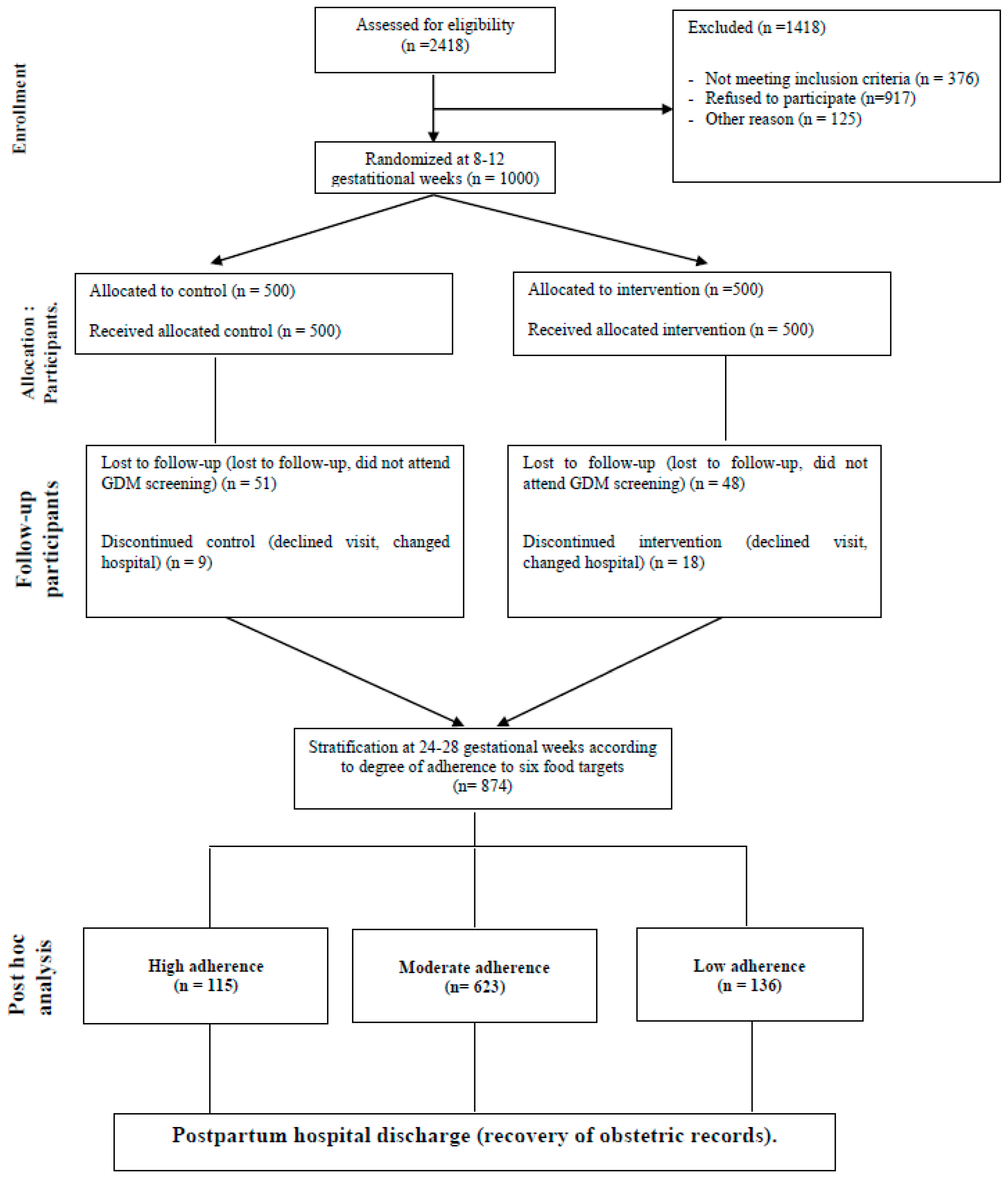
2.1. Study Design
2.2. Dietary Patterns Classification
2.3. Dietary Assessments
2.4. Study Population
2.5. Outcomes Measures
2.6. Other Assessments
2.6.1. Participant’s History
2.6.2. Anthropometric Data
2.6.3. Maternal, Delivery, and Neonatal Outcomes
2.6.4. Biochemical Analysis
2.6.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Dietary Habits at Baseline and 24–28 GWs
3.3. Socio-Demographic, Clinical, and Biochemical Characteristics of Women According to Late First-Trimester Degree of Adherence to Six Food Targets
3.4. Dietary Habits According to the Late First-Trimester Degrees of Adherence to Six Food Targets at Baseline and at 24–28 GWs
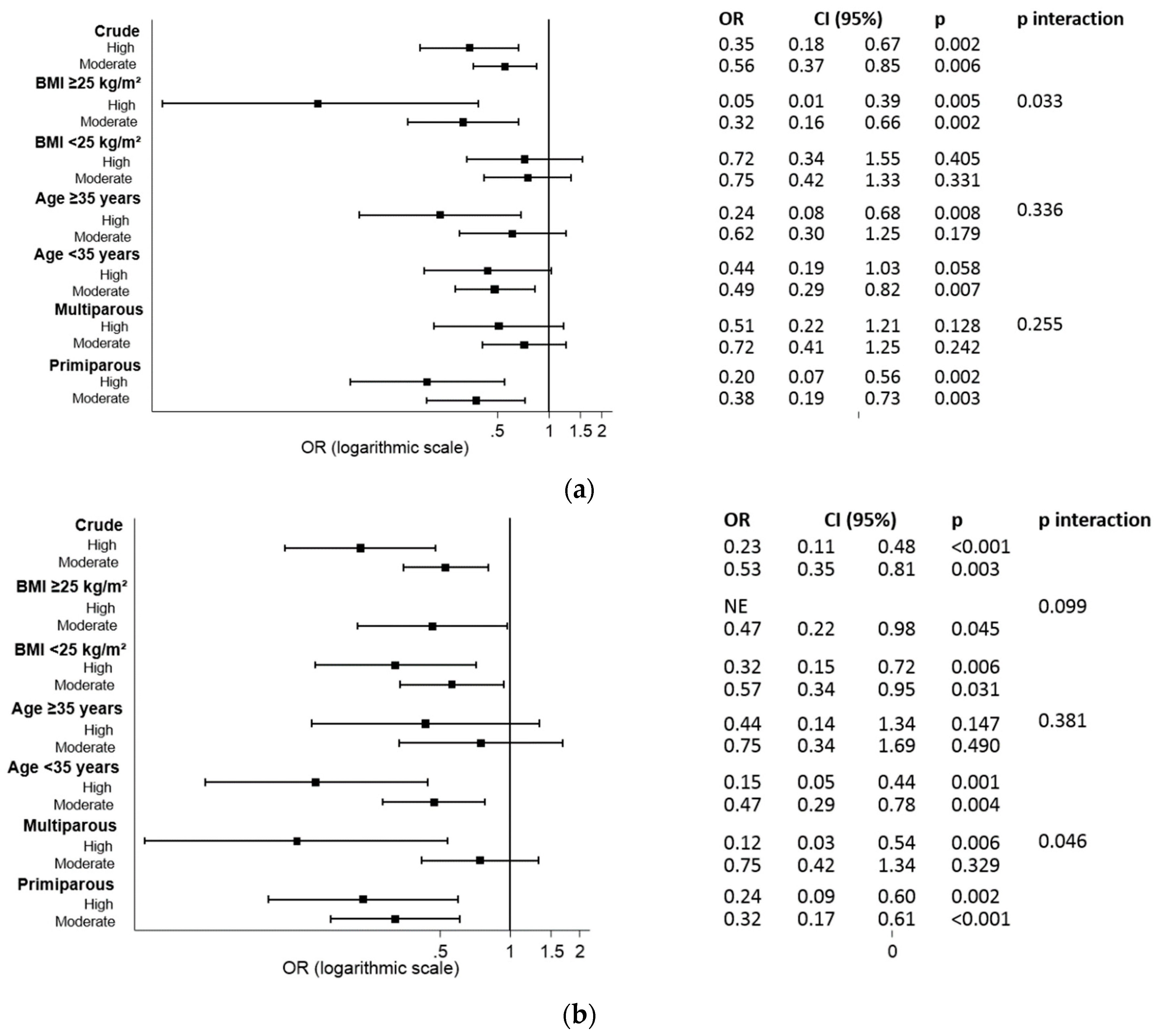
3.5. Associations between Late First-Trimester Degrees of Adherence and Materno-Foetal Complications
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Statement
References
- Chen, X.; Zhao, D.; Mao, X.; Xia, Y.; Baker, P.N.; Zhang, H. Maternal Dietary Patterns and Pregnancy Outcome. Nutrients 2016, 8, 351. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary Patterns during Pregnancy Are Associated with Risk of Gestational Diabetes Mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef] [Green Version]
- Meltzer, H.M.; Brantsæter, A.L.; Nilsen, R.M.; Magnus, P.; Alexander, J.; Haugen, M. Effect of dietary factors in pregnancy on risk of pregnancy complications: Results from the Norwegian Mother and Child Cohort Study. Am. J. Clin. Nutr. 2011, 94, 1970S–1974S. [Google Scholar] [CrossRef]
- Haugen, M.; Margrete Meltzer, H.; Lise Brantsaeter, A.; Mikkelsen, T.; Louise Østerdal, M.; Alexander, J.; Olsen, S.F.; Bakketeig, L. Mediterranean-type diet and risk of preterm birth among women in the Norwegian Mother and Child Cohort Study (MoBa): A prospective cohort study. Acta Obstet. Gynecol. Scand. 2008, 87, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Jarman, M.; Mathe, N.; Ramazani, F.; Pakseresht, M.; Robson, P.J.; Johnson, S.T.; Bell, R.C. APrON and ENRICH study teams, the Ap. and E. study. Dietary Patterns Prior to Pregnancy and Associations with Pregnancy Complications. Nutrients 2018, 10, 914. [Google Scholar] [CrossRef] [PubMed]
- Loy, S.-L.; Marhazlina, M.; Azwany, Y.N.; Hamid Jan, J.M. Higher intake of fruits and vegetables in pregnancy is associated with birth size. Southeast Asian J. Trop. Med. Public Health 2011, 42, 1214–1223. [Google Scholar] [PubMed]
- Tryggvadottir, E.A.; Medek, H.; Birgisdottir, B.E.; Geirsson, R.T.; Gunnarsdottir, I. Association between healthy maternal dietary pattern and risk for gestational diabetes mellitus. Eur. J. Clin. Nutr. 2016, 70, 237–242. [Google Scholar] [CrossRef]
- Brantsæter, A.L.; Haugen, M.; Samuelsen, S.O.; Torjusen, H.; Trogstad, L.; Alexander, J.; Magnus, P.; Meltzer, H.M. A Dietary Pattern Characterized by High Intake of Vegetables, Fruits, and Vegetable Oils Is Associated with Reduced Risk of Preeclampsia in Nulliparous Pregnant Norwegian Women. J. Nutr. 2009, 139, 1162–1168. [Google Scholar] [CrossRef] [Green Version]
- Hajianfar, H.; Esmaillzadeh, A.; Feizi, A.; Shahshahan, Z.; Azadbakht, L. Major Maternal Dietary Patterns during Early Pregnancy and Their Association with Neonatal Anthropometric Measurement. BioMed Res. Int. 2018, 2018, 4692193. [Google Scholar] [CrossRef]
- Schoenaker, D.A.; Soedamah-Muthu, S.S.; Callaway, L.K.; Mishra, G.D. Prepregnancy dietary patterns and risk of developing hypertensive disorders of pregnancy: Results from the Australian Longitudinal Study on Women’s Health. Am. J. Clin. Nutr. 2015, 102, 94–101. [Google Scholar] [CrossRef]
- Ruiz-Gracia, T.; Duran, A.; Fuentes, M.; Rubio, M.A.; Runkle, I.; Carrera, E.F.; Torrejón, M.J.; Bordiú, E.; del Valle, L.; García de la Torre, N.; et al. Lifestyle patterns in early pregnancy linked to gestational diabetes mellitus diagnoses when using IADPSG criteria. The St Carlos gestational study. Clin. Nutr. 2016, 35, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Assaf-Balut, C.; García de la Torre, N.; Durán, A.; Fuentes, M.; Bordiú, E.; del Valle, L.; Familiar, C.; Ortolá, A.; Jiménez, I.; Herraiz, M.A.; et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): A randomized controlled trial: The St. Carlos GDM prevention study. PLoS ONE 2017, 12, e0185873. [Google Scholar] [CrossRef] [PubMed]
- Kibret, K.T.; Chojenta, C.; Gresham, E.; Tegegne, T.K.; Loxton, D. Maternal dietary patterns and risk of adverse pregnancy (hypertensive disorders of pregnancy and gestational diabetes mellitus) and birth (preterm birth and low birth weight) outcomes: A systematic review and meta-analysis. Public Health Nutr. 2018, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Schroder, H.; Fito, M.; Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Lamuela-Raventos, R.; Ros, E.; Salaverria, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos-Leví, A.M.; Pérez-Ferre, N.; Fernández, M.D.; del Valle, L.; Bordiu, E.; Bedia, A.R.; Herraiz, M.A.; Torrejón, M.J.; Calle-Pascual, A.L. Risk Factors for Gestational Diabetes Mellitus in a Large Population of Women Living in Spain: Implications for Preventative Strategies. Int. J. Endocrinol. 2012, 2012, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. PREDIMED Study Investigators Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.F.; Calle-Pascual, A.L. Diabetes and Nutrition Study Group, Spanish Diabetes Association Diabetes Nutrition and Complications Trial: Trends in nutritional pattern between 1993 and 2000 and targets of diabetes treatment in a sample of Spanish people with diabetes. Diabetes Care 2004, 27, 984–987. [Google Scholar] [PubMed]
- Edvardsson, K.; Ivarsson, A.; Eurenius, E.; Garvare, R.; Nyström, M.E.; Small, R.; Mogren, I. Giving offspring a healthy start: Parents’ experiences of health promotion and lifestyle change during pregnancy and early parenthood. BMC Public Health 2011, 11, 936. [Google Scholar] [CrossRef]
- Lee, K. Capitalizing on Pregnancy as a Teachable Moment for Healthy Eating and Diabetes Prevention among CENTRAL American Immigrants in Washington, D.C. Ph.D. Thesis, Johns Hopkins University, Baltimore, MD, USA, 2016. [Google Scholar]
- Forbes, L.E.; Graham, J.E.; Berglund, C.; Bell, R.C. Dietary Change during Pregnancy and Women’s Reasons for Change. Nutrients 2018, 10, 1032. [Google Scholar] [CrossRef]
- Hillier, S.E.; Olander, E.K. Women’s dietary changes before and during pregnancy: A systematic review. Midwifery 2017, 49, 19–31. [Google Scholar] [CrossRef]
- Englund-Ögge, L.; Brantsæter, A.L.; Sengpiel, V.; Haugen, M.; Birgisdottir, B.E.; Myhre, R.; Meltzer, H.M.; Jacobsson, B. Maternal dietary patterns and preterm delivery: Results from large prospective cohort study. BMJ 2014, 348, G1446. [Google Scholar] [CrossRef] [PubMed]
- Cetin, I.; Laoreti, A. The importance of maternal nutrition for health. J. Pediatr. Neonatal Individ. Med. 2016, 4, e040220. [Google Scholar] [CrossRef]
- Thompson, J.M.D.; Wall, C.; Becroft, D.M.O.; Robinson, E.; Wild, C.J.; Mitchell, E.A. Maternal dietary patterns in pregnancy and the association with small-for-gestational-age infants. Br. J. Nutr. 2010, 103, 1665–1673. [Google Scholar] [CrossRef] [PubMed]
- Karamanos, B.; Thanopoulou, A.; Anastasiou, E.; Assaad-Khalil, S.; Albache, N.; Bachaoui, M.; Slama, C.B.; El Ghomari, H.; Jotic, A.; Lalic, N.; et al. MGSD-GDM Study Group Relation of the Mediterranean diet with the incidence of gestational diabetes. Eur. J. Clin. Nutr. 2014, 68, 8–13. [Google Scholar] [CrossRef]
- Timmermans, S.; Steegers-Theunissen, R.P.; Vujkovic, M.; den Breeijen, H.; Russcher, H.; Lindemans, J.; Mackenbach, J.; Hofman, A.; Lesaffre, E.E.; Jaddoe, V.V.; et al. The Mediterranean diet and fetal size parameters: The Generation R Study. Br. J. Nutr. 2012, 108, 1399–1409. [Google Scholar] [CrossRef]
- Martínez-Galiano, J.; Olmedo-Requena, R.; Barrios-Rodríguez, R.; Amezcua-Prieto, C.; Bueno-Cavanillas, A.; Salcedo-Bellido, I.; Jimenez-Moleon, J.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M.; Olmedo-Requena, R.; et al. Effect of Adherence to a Mediterranean Diet and Olive Oil Intake during Pregnancy on Risk of Small for Gestational Age Infants. Nutrients 2018, 10, 1234. [Google Scholar] [CrossRef]
- Ramiro-Cortijo, D.; Herrera, T.; Rodríguez-Rodríguez, P.; López De Pablo, Á.L.; De La Calle, M.; López-Giménez, M.R.; Mora-Urda, A.I.; Gutiérrez-Arzapalo, P.Y.; Gómez-Rioja, R.; Aguilera, Y.; et al. Maternal plasma antioxidant status in the first trimester of pregnancy and development of obstetric complications. Placenta 2016, 47, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Maged, A.M.; Torky, H.; Fouad, M.A.; GadAllah, S.H.; Waked, N.M.; Gayed, A.S.; Salem, A.K. Role of antioxidants in gestational diabetes mellitus and relation to fetal outcome: A randomized controlled trial. J. Matern. Neonatal Med. 2016, 29, 4049–4054. [Google Scholar] [CrossRef]
- Carmichael, S.; Yang, W.; Shaw, G. National Birth Defects Prevention Study Maternal Dietary Nutrient Intake and Risk of Preterm Delivery. Am. J. Perinatol. 2012, 30, 579–588. [Google Scholar] [CrossRef]
- Endeshaw, M.; Ambaw, F.; Aragaw, A.; Ayalew, A. Effect of Maternal Nutrition and Dietary Habits on Preeclampsia: A Case-Control Study. Int. J. Clin. Med. 2014, 5, 1405–1416. [Google Scholar] [CrossRef]
- Cuffe, J.S.; Xu, Z.C.; Perkins, A. V Biomarkers of oxidative stress in pregnancy complications. Biomark. Med. 2017, 11, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.M.; Beddaoui, M.; Kramer, M.S.; Platt, R.W.; Basso, O.; Kahn, S.R. Maternal Antioxidant Levels in Pregnancy and Risk of Preeclampsia and Small for Gestational Age Birth: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0135192. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total Sample (n = 874) |
|---|---|
| Age (years) | 32.9 ± 5.1 |
| Race/Ethnicity | |
| Caucasian | 587 (67.2) |
| Hispanic | 260 (29.7) |
| Others | 27 (3.1) |
| Family history of | |
| Type 2 diabetes | 180 (20.6) |
| Family history of MetS (>2 components) | 183 (20.9) |
| Previous history of | |
| Gestational diabetes | 25 (2.9) |
| Miscarriages | 278 (31.8) |
| Educational status | |
| Elementary education | 88 (8.9) |
| Secondary school | 212 (24.3) |
| University degree | 577 (66.0) |
| UNK | 7 (0.8) |
| Employment | 674 (77.1) |
| Number of pregnancies | |
| Primiparous | 378 (43.3) |
| Second pregnancy | 281 (32.2) |
| >2 pregnancies | 215 (24.5) |
| Never smoker | 477 (54.6) |
| Current smoker | 72 (8.2) |
| Gestational age at baseline (weeks) | 12.1 ± 0.6 |
| Prepregnancy body weight (kg) | 60.8 ± 10.8 |
| Body weight at entry (kg) | 62.9 ± 11.1 |
| Weight gain (kg) | 2.1 ± 3.0 |
| Prepregnancy BMI (kg/m2) | 23.1 ± 3.8 |
| BMI at baseline (kg/m2) | 23.9 ± 3.9 |
| Systolic blood pressure (mm Hg) | 107 ± 11 |
| Diastolic blood pressure (mm Hg) | 66 ± 10 |
| Fasting blood glucose (mg/dL) | 81 ± 6 |
| HbA1c % | 5.1 ± 0.3 |
| Cholesterol mg/dL | 174 ± 30 |
| Triglycerides mg/dL | 82 ± 40 |
| TSH mcUI/mL | 2.0 ± 1.3 |
| T4L ng/dL | 8.6 ± 1.5 |
| MEDAS score | 4.9 ± 1.7 |
| Nutrition score | 0.4 ± 3.2 |
| Total Sample | |||||
|---|---|---|---|---|---|
| Servings/Week | At Targets | Servings/Week | At Targets | ||
| Variables | Baseline | n (%) | 24–28 GWs | n (%) | p Value |
| Vegetables | 6.3 (6.0–6.3) | 146 (16.7) | 7.1 (6.8–7.4) | 179 (20.1) | 0.001 |
| Pieces of fruit | 10.7 (10.1–11.2) | 420 (40.1) | 15.0 (14.5–15.5) | 643 (72.8) | 0.001 |
| Nuts | 1.4 (1.3–1.5) | 122 (14.0) | 2.6 (2.5–2.9) | 305 (32.9) | 0.001 |
| EVOO (days/week) | 6.1 (6.0–6.3) | 738 (84.4) | 6.4 (6.3–6.5) | 750 (85.8) | 0.001 |
| Oily fish or ibérico ham | 1.0 (1.0–1.2) | 9 (1.0) | 1.0 (0.9–1.2) | 66 (7.6) | 0.264 |
| Canned fish | 1.5 (1.4–1.6) | 20 (2.3) | 1.2 (1.1–1.3) | 64 (7.2) | 0.001 |
| White fish | 1.2 (1.1–1.3) | N.A. | 1.2 (1.1–1.3) | N.A. | 0.499 |
| Shellfish | 0.2 (0.2–0.3) | N.A. | 0.2 (0.1–0.2) | N.A. | 0.026 |
| Whole grain bread and cereals | 1.9 (1.7–2.1) | 157 (18.0) | 2.5 (2.3–2.7) | 215 (24.6) | 0.001 |
| White rice, bread and/or pasta | 5.2 (5.0–5.3) | 77 (8.7) | 4.8 (4.7–5.0) | 83 (9.5) | 0.001 |
| Legumes | 1.7 (1.6–1.8) | 167 (19.1) | 1.8 (1.7–1.9) | 198 (22.6) | 0.005 |
| Skimmed dairy products | 2.6 (2.4–2.9) | 10 (1.1) | 3.3 (3.1–3.5) | 357 (40.8) | 0.001 |
| Semi-skimmed dairy products | 2.7 (2.5–3.0) | N.A. | 2.8 (2.5–3.0) | N.A. | 0.982 |
| Full-fat dairy products | 4.4 (4.2–4.6) | N.A. | 4.4 (4.2–4.6) | N.A. | 0.780 |
| Supplemented dairy products | 1.3 (1.2–1.5) | N.A. | 2.0 (1.8–2.2) | N.A. | 0.001 |
| Butter | 1.6 (1.4–1.7) | N.A. | 1.4 (1.2–1–5) | N.A. | 0.003 |
| Red meat | 2.3 (2.2–2.4) | 282 (32.3) | 1.9 (1.9–2.0) | 392 (46.2) | 0.001 |
| Low-fat processed cold meat | 2.7 (2.6–2.9) | 204 (23.3) | 2.3 (2.2–2.5) | 297 (35.0) | 0.001 |
| Processed red meat | 0.8 (0.7–0.9) | 455 (52.1) | 0.5 (0.4–0.5) | 563 (64.4) | 0.001 |
| Poultry, turkey or rabbit | 3.0 (2.9–3.1) | N.A. | 2.8 (2.7–2.9) | N.A. | 0.001 |
| Commercial sauces | 0.8 (0.7–0.9) | 553 (63.3) | 0.4 (0.3–0.4) | 650 (74.4) | 0.001 |
| Juices and/or sweetened drinks | 3.7 (3.5–3.9) | 283 (32.4) | 2.9 (2.7–3.1) | 364 (42.9) | 0.001 |
| Pastries and biscuits | 4.7 (4.5–4.9) | 136 (14.4) | 4.1 (3.9–4.3) | 179 (21.1) | 0.001 |
| Coffees | 6.9 (6.5–7.4) | N.A. | 4.2 (3.9–4.5) | N.A. | 0.001 |
| Homemade sauces | 2.3 (2.1–2.4) | 48 (5.5) | 2.4 (2.3–2.6) | 50 (5.9) | 0.021 |
| EVOO mL/day | 28 (26–29) | 55 (17.8) | 29 (28–31) | 211 (24.1) | 0.176 |
| Nutrition score | 0.4 (0.1–0.6) | N.A. | 2.6 (2.4–2.9) | N.A. | 0.001 |
| MEDAS score | 4.9 (4.8–5.0) | N.A. | 6.7 (6.5–6.8) | N.A. | 0.001 |
| Physical activity Score ≥ 0 | 99 (11.3) | N.A. | 58 (6.9) | N.A. | 0.406 |
| Variables | Groups | p Value | ||
|---|---|---|---|---|
| Low Adherence (n = 136/15.6%) | Moderate Adherence (n = 623/71.3%) | High Adherence (n = 115/13.1%) | ||
| Age (years) | 31.2 ± 6.0 | 33.1 ± 4.9 | 33.9 ± 4.9 | 0.001 |
| Race/Ethnicity | ||||
| Caucasian | 79 (58.1) | 420 (67.4) | 88 (76.5) | 0.005 |
| Hispanic | 51 (37.5) | 188 (30.2) | 21 (18.3) | |
| Others | 6 (4.4) | 15 (2.4) | 6 (5.2) | |
| Family history of: | ||||
| Type 2 diabetes | 28 (20.6) | 131 (21.0) | 21 (18.3) | 0.019 |
| MetS (>2 components) | 18 (13.2) | 135 (21.7) | 30 (26.1) | |
| Previous history of: | ||||
| Gestational diabetes | 7 (5.1) | 15 (2.4) | 3 (2.6) | 0.342 |
| Miscarriages | 45 (33.1) | 196 (31.5) | 37 (32.2) | |
| Educational status | ||||
| Elementary education | 19 (14.0) | 54 (8.7) | 5 (4.3) | 0.001 |
| Secondary school | 49 (36.0) | 145 (23.3) | 18 (15.7) | |
| University degree | 65 (47.8) | 420 (67.4) | 92 (80.0) | |
| UNK | 3 (2.2) | 4 (0.6) | 0 (0) | |
| Employment | 100 (73.5) | 482 (77.4) | 92 (80.0) | 0.815 |
| Number of pregnancies | ||||
| Primiparous | 50 (36.8) | 274 (44.0) | 54 (47.8) | 0.017 |
| Second pregnancy | 43 (31.6) | 196 (31.5) | 42 (36.8) | |
| >2 pregnancies | 43 (31.6) | 153 (24.5) | 19 (15.4) | |
| Smoker | ||||
| Never | 75 (55.1) | 334 (53.6) | 68 (59.1) | 0.260 |
| Current | 16 (11.8) | 52 (8.3) | 4 (3.5) | |
| Gestational age (weeks) at baseline | 12.1 ± 0.7 | 12.1 ± 0.5 | 12.0 ± 0.5 | 0.137 |
| Body Weight (kg) | ||||
| Prepregnancy | 61.1 ± 11.8 | 61.0 ± 10.8 | 59.5 ± 9.3 | 0.383 |
| At entry | 63.3 ± 11.3 | 63.1 ± 11.1 | 61.5 ± 8.4 | 0.356 |
| Weight gain | 2.2 ± 3.2 | 2.0 ± 3.0 | 2.0 ± 2.7 | 0.707 |
| BMI (kg/m2) | ||||
| Prepregnancy | 23.4 ± 4.1 | 23.2 ± 3.8 | 22.5 ± 3.4 | 0.137 |
| At baseline | 24.3 ± 4.3 | 23.9 ± 3.9 | 23.3 ± 3.5 | 0.111 |
| Blood pressure (mm Hg): | ||||
| Systolic | 107 ± 10 | 107 ± 11 | 107 ± 10 | 0.972 |
| Diastolic | 66 ± 15 | 66 ± 9 | 66 ± 8 | 0.809 |
| Fasting blood glucose mg/dL | 82 ± 5 | 81 ± 6 | 81 ± 7 | 0.377 |
| HbA1c % | 5.2 ± 0.2 | 5.2 ± 0.3 | 5.1 ± 0.3 | 0.436 |
| Cholesterol mg/dL | 171 ± 28 | 175 ± 31 | 176 ± 25 | 0.507 |
| Triglycerides mg/dL | 82 ± 38 | 83 ± 42 | 76 ± 30 | 0.288 |
| TSH mcUI/mL | 1.9 ± 1.2 | 2.0 ± 1.3 | 2.1 ± 1.4 | 0.610 |
| T4L ng/dL | 8.6 ± 1.3 | 8.6 ± 1.6 | 8.9 ± 1.2 | 0.144 |
| Variables | Groups | |||||||
|---|---|---|---|---|---|---|---|---|
| Low Adherence (n = 136/15.6%) | Moderate Adherence (n = 623/71.3%) | High Adherence (n = 115/13.1%) | ||||||
| Baseline | 24–28 GW | Baseline | 24–28 GW | Baseline | 24–28 GW | pa | pb | |
| Vegetables | 4.7 (4.1–5.2) | 4.2 (3.8–4.7) | 6.3 (6.0–6.7) | 6.8 (6.5–7.2) | 8.2 (7.4–9.1) | 12.2 (11.6–12.9) | 0.001 | 0.001 |
| Pieces of fruit | 8.0 (6.6–9.4) | 8.5 (7.2–9.7) | 10.6 (10.0–11.3) | 15.7 (15.1–16.3) | 13.9 (12.4–15.4) | 18.8 (17.7–19.9) | 0.001 | 0.001 |
| Nuts | 0.9 (0.7–1.0) | 0.7 (0.5–0.9) | 1.4 (1.2–1.5) | 2.6 (2.4–2.8) | 2.2 (1.7–2.6) | 5.5 (5.0–5.9) | 0.001 | 0.001 |
| EVOO (days/week) | 4.8 (4.3–5.3) | 4.2 (3.7–4.8) | 6.4 (6.2–6.5) | 6.8 (6.7–6.9) | 6.5 (6.2–6.8) | 7.0 (6.9–7.0) | 0.001 | 0.001 |
| Oily fish or Iberico ham | 0.8 (0.7–1.2) | 0.8 (0.7–1.0) | 1.0 (1.0–1.1) | 1.0 (0.7–1.1) | 1.1 (1.0–1.3) | 1.2 (1.0–1.4) | 0.035 | 0.025 |
| Canned fish | 1.6 (1.3–1.9) | 1.0 (0.8–1.2) | 1.5 (1.4–1.6) | 1.2 (1.1–1.3) | 1.4 (1.1–1.6) | 1.2 (1.0–1.5) | 0.001 | 0.293 |
| White fish | 1.1 (0.9–1.3) | 1.0 (0.8–1.2) | 1.2 (1.1–1.3) | 1.2 (1.1–1.3) | 1.5 (1.2–1.7) | 1.4 (1.2–1.7) | 0.345 | 0.009 |
| Shellfish | 1 (0–2) | 0.1 (0.0–0.2) | 0 (0–0) | 0.2 (0.2–0.2) | 0.3 (0.2–0.4) | 0.2 (0.1–0.3) | 0.287 | 0.380 |
| Whole grain bread and cereals | 1.8 (1.3–2.2) | 1.8 (1.4–2.3) | 1.9 (1.7–2.1) | 2.5 (2.2–2.7) | 2.2 (1.6–2.7) | 3.4 (2.8–4.1) | 0.504 | 0.001 |
| White rice, bread and/or pasta | 5.5 (5.1–5.8) | 5.4 (5.1–5.8) | 5.2 (5.0–5.3) | 4.9 (4.7–5.1) | 5.0 (4.5–5.4) | 3.9 (3.3–4.4) | 0.217 | 0.001 |
| Legumes | 2.0 (1.7–2.2) | 1.9 (1.6–2.2) | 1.7 (1.6–1.7) | 1.8 (1.7–1.9) | 1.6 (1.4–1.7) | 1.8 (1.6–2.1) | 0.010 | 0.593 |
| Skimmed dairy products | 1.7 (1.2–2.2) | 2.2 (1.7–2.8) | 2.7 (2.5–3.0) | 3.4 (3.1–3.6) | 3.3 (2.7–3.9) | 4.2 (3.5–4.8) | 0.001 | 0.001 |
| Semi-skimmed dairy products | 2.8 (2.3–3.4) | 2.5 (1.9–3.1) | 2.9 (2.6–3.1) | 2.8 (2.6–3.1) | 2.0 (1.4–2.6) | 2.7 (2.1–3.4) | 0.051 | 0.574 |
| Full-fat dairy products | 4.7 (4.3–5.2) | 5.0 (4.6–5.5) | 4.3 (4.1–4.5) | 4.4 (4.2–4.6) | 4.6 (4.1–5.2) | 3.9 (3.3–4.5) | 0.166 | 0.008 |
| Supplemented dairy products | 1.1 (0.7–1.6) | 2.1 (1.6–2.7) | 1.4 (1.2–1.7) | 2.1 (1.6–2.7) | 1.0 (0.6–1.5) | 1.6 (1.1–2.2) | 0.214 | 0.476 |
| Butter | 1.8 (1.4–2.2) | 1.7 (1.3–2.1) | 1.6 (1.4–1.8) | 1.4 (1.2–1.5) | 1.4 (1.0–1.8) | 0.9 (0.6–1.3) | 0.458 | 0.029 |
| Red meat | 2.6 (2.2–2.8) | 2.3 (2.0–2.5) | 2.3 (2.2–2.4) | 1.9 (1.8–2.0) | 2.0 (1.7–2.3) | 1.6 (1.3–1.8) | 0.032 | 0.001 |
| Low-fat processed cold meat | 2.8 (2.4–3.3) | 2.2 (1.8–2.7) | 2.7 (2.5–2.9) | 2.4 (2.2–2.5) | 2.8 (2.3–3.2) | 2.3 (1.8–2.8) | 0.881 | 0.890 |
| Processed red meat | 1.1 (0.9–1.4) | 0.7 (0.5–0.8) | 0.7 (0.7–0.8) | 0.5 (0.4–0.5) | 0.5 (0.4–0.7) | 0.3 (0.1–0.4) | 0.001 | 0.001 |
| Poultry, turkey or rabbit | 3.2 (2.9–3.5) | 2.8 (2.6–3.1) | 3.0 (2.8–3.1) | 2.8 (2.7–2.9) | 2.8 (2.5–3.1) | 2.8 (2.5–3.1) | 0.119 | 0.955 |
| Commercial sauces | 1.1 (0.9–1.4) | 0.5 (0.3–0.7) | 0.7 (0.6–0.8) | 0.4 (0.3–0.4) | 0.8 (0.5–1.1) | 0.3 (0.1–0.5) | 0.008 | 0.250 |
| Juices and/or sweetened drinks | 4.7 (4.3–5.1) | 4.8 (4.4–5.1) | 3.3 (3.3–3.8) | 2.8 (2.6–3.0) | 3.1 (2.5–3.6) | 0.8 (0.4–1.2) | 0.001 | 0.001 |
| Pastries and biscuits | 4.6 (4.1–5.0) | 4.6 (4.2–5.0) | 4.8 (4.6–5.0) | 4.2 (3.9–4.4) | 4.3 (3.8–4.8) | 3.3 (2.7–3.8) | 0.133 | 0.001 |
| Coffees | 6.0 (5.0–7.1) | 4.2 (3.4–5.0) | 7.1 (6.5–7.7) | 4.1 (3.7–4.5) | 7.1 (5.9–8.4) | 4.6 (3.7–5.5) | 0.282 | 0.627 |
| Homemade sauces | 2 (0–3) | 1.4 (1.1–1.7) | 2 (1–3) | 2.6 (2.4–2.7) | 50 (5.9) | 2.8 (2.4–3.3) | 0.001 | 0.001 |
| EVOO mL/day | 20 (17–23) | 15 (13–17) | 29 (27–30) | 30 (28–32) | 33 (28–39) | 44 (40–49) | 0.001 | 0.001 |
| Nutrition Score | −1.5 (−2.0–−1.0) | −1.4 (−1.9–−0.9) | 0.5 (0.3–0.7) | 2.8 (2.6–3.1) | 1.8 (1.1–2.4) | 6.7 (6.1–7.2) | 0.001 | 0.0001 |
| MEDAS Score | 3.9 (3.7–4.2) | 4.5 (4.3–4.7) | 5.0 (4.8–5.1) | 6.7 (6.6–6.9) | 5.7 (5.4–6.1) | 9.0 (8.7–9.2) | 0.001 | 0.0001 |
| Physical activity Score ≥ 0 | 16 (11.8) | 11 (11–2) | 71 (11.4) | 41 (6.6) | 12 (10.4) | 6 (4.7) | 0.845 | 0.127 |
| Groups | ||||
|---|---|---|---|---|
| Low Adherence (n = 136/15.6%) | Moderate Adherence (n = 623/71.3%) | High Adherence (n = 115/13.1%) | p Trend | |
| GDM n (%) | 41 (30.1) | 121 (19.4) | 15 (13.0) | 0.001 |
| Crude OR (95% CI) | 1 | 0.56 (0.37–0.85) | 0.35 (0.18–0.67) | 0.003 |
| p | 0.006 | 0.002 | ||
| Insulin-treated GDM | 12 (29.3) | 32 (26.4) | 3 (20.0) | 0.512 |
| Crude OR (95% CI) | 1 | 0.55 (0.13–2.39) | N.A. | |
| p | 0.422 | |||
| Pregnancy-induced hypertension | 7 (5.1) | 23 (3.7) | 2 (1.7) | 0.155 |
| Crude OR (95% CI) | 1 | 0.71 (0.30–1.68) | 0.33 (0.07–1.60) | 0.376 |
| p | 0.432 | 0.168 | ||
| Urinary tract infection | 26 (19.1) | 53 (8.5) | 5 (4.3) | 0.0001 |
| Crude OR (95% CI) | 1 | 0.39 (0.24–0.66) | 0.19 (0.07–0.52) | 0.001 |
| p | 0.0001 | 0.001 | ||
| Emergency-CS | 8 (5.9) | 30 (4.8) | 2 (1.7) | 0.128 |
| Crude OR (95% CI) | 1 | 0.81 (0.36–1.81) | 0.28 (0.06–1.36) | 0.287 |
| p | 0.606 | 0.115 | ||
| Perineal trauma | 15 (11.0) | 58 (9.3) | 9 (7.8) | 0.383 |
| Crude OR (95% CI) | 1 | 0.83 (0.45–1.51) | 0.69 (0.29–1.63) | 0.683 |
| p | 0.538 | 0.392 | ||
| Prematurity (<37 GW) | 9 (6.6) | 13 (2.1) | 0 (0) | 0.001 |
| Crude OR (95% CI) | 1 | 0.30 (0.13–0.72) | N.A. | 0.026 |
| p | 0.007 | |||
| LGA > 90 centile | 5 (3.7) | 17 (2.7) | 0 (0.0) | 0.071 |
| Crude OR (95% CI) | 1 | 0.74 (0.27–2.03) | N.A. | |
| p | 0.552 | |||
| SGA < 10 centile | 11 (8.1) | 19 (3.0) | 0 (0) | 0.0001 |
| Crude OR (95% CI) | 1 | 0.36 (0.17–0.77) | N.A. | |
| p | 0.009 | |||
| NICU/observation | 5 (3.7) | 16 (2.6) | 1 (0.9) | 0.162 |
| Crude OR (95% CI) | 1 | 0.69 (0.25–1.92) | 0.23 (0.03–1.99) | 0.399 |
| p | 0.478 | 0.182 | ||
| Hyperbilurrubinemia | 11 (8.1) | 38 (6.1) | 4 (3.5) | 0.130 |
| Crude OR (95% CI) | 1 | 0.74 (0.37–1.48) | 0.41 (0.13–1.32) | 0.323 |
| p | 0.394 | 0.136 | ||
| CMFC | 40 (29.4) | 113 (18.1) | 10 (8.7) | 0.0001 |
| Crude OR (95% CI) | 1 | 0.53 (0.35–0.81) | 0.23 (0.11–0.48) | 0.0001 |
| p | 0.003 | 0.001 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assaf-Balut, C.; García de la Torre, N.; Fuentes, M.; Durán, A.; Bordiú, E.; Del Valle, L.; Valerio, J.; Jiménez, I.; Herraiz, M.A.; Izquierdo, N.; et al. A High Adherence to Six Food Targets of the Mediterranean Diet in the Late First Trimester is Associated with a Reduction in the Risk of Materno-Foetal Outcomes: The St. Carlos Gestational Diabetes Mellitus Prevention Study. Nutrients 2019, 11, 66. https://doi.org/10.3390/nu11010066
Assaf-Balut C, García de la Torre N, Fuentes M, Durán A, Bordiú E, Del Valle L, Valerio J, Jiménez I, Herraiz MA, Izquierdo N, et al. A High Adherence to Six Food Targets of the Mediterranean Diet in the Late First Trimester is Associated with a Reduction in the Risk of Materno-Foetal Outcomes: The St. Carlos Gestational Diabetes Mellitus Prevention Study. Nutrients. 2019; 11(1):66. https://doi.org/10.3390/nu11010066
Chicago/Turabian StyleAssaf-Balut, Carla, Nuria García de la Torre, Manuel Fuentes, Alejandra Durán, Elena Bordiú, Laura Del Valle, Johanna Valerio, Inés Jiménez, Miguel Angel Herraiz, Nuria Izquierdo, and et al. 2019. "A High Adherence to Six Food Targets of the Mediterranean Diet in the Late First Trimester is Associated with a Reduction in the Risk of Materno-Foetal Outcomes: The St. Carlos Gestational Diabetes Mellitus Prevention Study" Nutrients 11, no. 1: 66. https://doi.org/10.3390/nu11010066
APA StyleAssaf-Balut, C., García de la Torre, N., Fuentes, M., Durán, A., Bordiú, E., Del Valle, L., Valerio, J., Jiménez, I., Herraiz, M. A., Izquierdo, N., Torrejón, M. J., De Miguel, M. P., Barabash, A., Cuesta, M., Rubio, M. A., & Calle-Pascual, A. L. (2019). A High Adherence to Six Food Targets of the Mediterranean Diet in the Late First Trimester is Associated with a Reduction in the Risk of Materno-Foetal Outcomes: The St. Carlos Gestational Diabetes Mellitus Prevention Study. Nutrients, 11(1), 66. https://doi.org/10.3390/nu11010066