Measuring Quality of Life in Parents or Caregivers of Children and Adolescents with Celiac Disease: Development and Content Validation of the Questionnaire

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
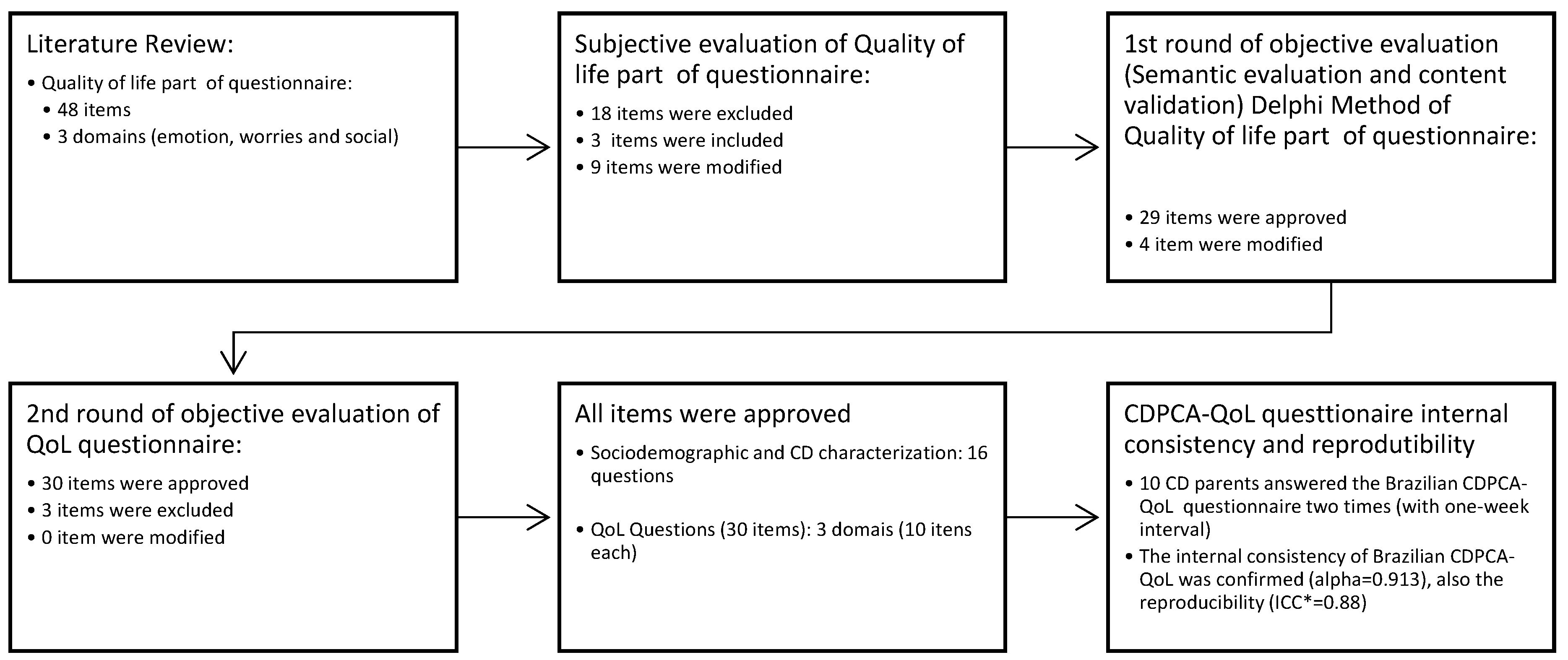
2.1. Development of the Questionnaire
2.2. Subjective Evaluation
2.3. Semantic Evaluation and Content Validation
2.4. Reproducibility Analysis
2.5. Brazilian Questionnaire (CDPCA-QoL) Application
2.6. Statistical Analysis
3. Results
3.1. Development of the Questionnaire
3.2. Factor Validity, Reproducibility, Responsiveness, and Internal Consistency of the Brazilian CDPCA-QoL Questionnaire
3.3. CDPCA-QoL Questionnaire Application
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- ESPGHAN. European Society Paediatric Gastroenterology, Hepatology and Nutrition guidelines for diagnosing coeliac disease. J. Pediatr. Gastroenterol. Nutr. 2019, 1–55. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Rubio-Tapia, A.; Assiri, A.; Newland, C.; Guandalini, S. Diagnosis of Celiac Disease. Gastrointest. Endosc. Clin. N. Am. 2012, 22, 661–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volta, U.; Molinaro, N.; Fusconi, M.; Cassani, F.; Bianchi, F.B. IgA antiendomysial antibody test. A step forward in celiac disease screening. Dig. Dis. Sci. 1991, 36, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Midhagen, G.; Järnerot, G.; Kraaz, W. Adult Coeliac Disease within a Defined Geographic Area in Sweden: A Study of Prevalence and Associated Diseases. Scand. J. Gastroenterol. 1988, 23, 1000–1004. [Google Scholar] [CrossRef] [PubMed]
- Feighery, C. Fortnightly review: Coeliac disease. BMJ 1999, 319, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Hörnell, A. Living Well With Celiac Disease? J. Pediatr. Gastroenterol. Nutr. 2008, 47, 544–546. [Google Scholar] [CrossRef] [PubMed]
- de Lorenzo, C.M.; Xikota, J.C.; Wayhs, M.C.; Nassar, S.M.; de Souza Pires, M.M. Evaluation of the quality of life of children with celiac disease and their parents: A case–control study. Qual. Life Res. 2012, 21, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Pratesi, C.; Häuser, W.; Uenishi, R.; Selleski, N.; Nakano, E.; Gandolfi, L.; Pratesi, R.; Zandonadi, R.; Pratesi, C.B.; Häuser, W.; et al. Quality of Life of Celiac Patients in Brazil: Questionnaire Translation, Cultural Adaptation and Validation. Nutrients 2018, 10, 1167. [Google Scholar] [CrossRef]
- Häuser, W.; Gold, J.; Stein, J.; Caspary, W.F.; Stallmach, A. Health-related quality of life in adult coeliac disease in Germany: Results of a national survey. Eur. J. Gastroenterol. Hepatol. 2006, 18, 747–754. [Google Scholar] [CrossRef]
- Araújo, H.M.C.; Araújo, W.M.C. Coeliac disease. Following the diet and eating habits of participating individuals in the Federal District, Brazil. Appetite 2011, 57, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Comino, I.; Moreno, M.d.L.; Sousa, C. Role of oats in celiac disease. World J. Gastroenterol. 2015, 21, 11825–11831. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Card, T.; Ciclitira, P.J.; Swift, G.L.; Nasr, I.; Sanders, D.S.; Ciacci, C. Support for patients with celiac disease: A literature review. United Eur. Gastroenterol. J. 2015, 3, 146–159. [Google Scholar] [CrossRef]
- Skjerning, H.; Mahony, R.O.; Husby, S.; DunnGalvin, A. Health-related quality of life in children and adolescents with celiac disease: Patient-driven data from focus group interviews. Qual. Life Res. 2014, 23, 1883–1894. [Google Scholar] [CrossRef] [PubMed]
- Spezia, F.M.; Clark, F.S. Quality of Life for Parents of Children and Adolescents With Type 1 Diabetes. Diabetes Educ. 1998, 24, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Kara, A. Evaluation of Psychopathology and Quality of Life in Children with Celiac Disease and their Parents. Gazi Med. J. 2019, 30, 43–47. [Google Scholar] [CrossRef]
- Macedo, E.C.; da Silva, L.R.; Paiva, M.S.; Ramos, M.N.P.; Macedo, E.C.; da Silva, L.R.; Paiva, M.S.; Ramos, M.N.P. Burden and quality of life of mothers of children and adolescents with chronic illnesses: An integrative review. Rev. Lat. Am. Enferm. 2015, 23, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Castilhos, A.C.; Gonçalves, B.C.; Macedo e Silva, M.; Lanzoni, L.A.; Metzger, L.R.; Kotze, L.M.S.; Nisihara, R.M. Quality of life evaluation in celiac patients from Southern Brazil. Arq. Gastroenterol. 2015, 52, 171–175. [Google Scholar] [CrossRef]
- Sverker, A.; Hensing, G.; Hallert, C. ’Controlled by food’–lived experiences of coeliac disease. J. Hum. Nutr. Diet. 2005, 18, 171–180. [Google Scholar] [CrossRef]
- Sverker, A.; Östlund, G.; Hallert, C.; Hensing, G. Sharing life with a gluten-intolerant person? the perspective of close relatives. J. Hum. Nutr. Diet. 2007, 20, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Zingone, F.; Iavarone, A.; Tortora, R.; Imperatore, N.; Pellegrini, L.; Russo, T.; Dorn, S.D.; Ciacci, C. The Italian translation of the Celiac Disease-specific Quality of Life Scale in celiac patients on gluten free diet. Dig. Liver Dis. 2013, 45, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Stallmach, A.; Caspary, W.F.; Stein, J. Predictors of reduced health-related quality of life in adults with coeliac disease. Aliment. Pharmacol. Ther. 2007, 25, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.R.; Marcon, M.; Brill, H.; Liu, A.; Radmanovich, K.; Mileski, H.; Nasser, R.; Alzaben, A.; Carroll, M.W.; Yap, J.; et al. Adherence to the Gluten-free Diet and Health-related Quality of Life in an Ethnically Diverse Pediatric Population With Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Litzelman, K.; Catrine, K.; Gangnon, R.; Witt, W.P. Quality of life among parents of children with cancer or brain tumors: The impact of child characteristics and parental psychosocial factors. Qual. Life Res. 2011, 20, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, L.; Kulich, K.; Deschaseaux, C.; Blackburn, S.; Maguire, L.; Strömberg, A. The Caregiver Burden Questionnaire for Heart Failure (CBQ-HF): Face and content validity. Health Qual. Life Outcomes 2013, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Aksan, A.; Mercanlıgil, S.M.; Häuser, W.; Karaismailoğlu, E. Validation of the Turkish version of the Celiac Disease Questionnaire (CDQ). Health Qual. Life Outcomes 2015, 13, 82. [Google Scholar] [CrossRef]
- Marchese, A.; Klersy, C.; Biagi, F.; Balduzzi, D.; Bianchi, P.I.; Trotta, L.; Vattiato, C.; Zilli, A.; Rademacher, J.; Andrealli, A.; et al. Quality of life in coeliac patients: Italian validation of a coeliac questionnaire. Eur. J. Intern. Med. 2013, 24, 87–91. [Google Scholar] [CrossRef]
- Pasquali, L. Psicometria. Rev. Esc. Enferm. USP 2009, 43, 992–999. [Google Scholar] [CrossRef]
- de Lima, T.C.; Gallani, M.C.B.J.; Freitas, M.I.P. de Content validation of an instrument to characterize people over 50 years of age living with human immunodeficiency virus/acquired immunodeficiency syndrome. Acta Paul. Enferm. 2012, 25, 4–10. [Google Scholar] [CrossRef]
- Farage, P.; Puppin Zandonadi, R.; Cortez Ginani, V.; Gandolfi, L.; Pratesi, R.; de Medeiros Nóbrega, Y.K. Content Validation and Semantic Evaluation of a Check-List Elaborated for the Prevention of Gluten Cross-Contamination in Food Services. Nutrients 2017, 9, 36. [Google Scholar] [CrossRef]
- Conti, M.A.; Scagliusi, F.; Kawamura De Oliveira Queiroz, G.; Hearst, N.; Cordás, T.A. Cross-cultural adaptation: Translation and Portuguese language content validation of the Tripartite Infl uence Scale for body dissatisfaction. Cad. Saude Publica 2010, 26, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Nursing Research: Principles and Methods; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004; ISBN 0781737338. [Google Scholar]
- Wendisch, C. Avaliação da Qualidade de Unidades de Alimentação e Nutrição (UAN) Hospitalares: Construção de um Instrumento; Rio de Janeiro: Fiocruz, Brazil, 2010. [Google Scholar]
- Sociedade Brasileira de Pediatria. Manual de Orientação do Departamento de Nutrologia: Alimentação do Lactente ao Adolescente, Alimentação na Escola, Alimentação Saudável e Vínculo Mãe-Fi lho, Alimentação Saudável e Prevenção de Doenças, Segurança Alimentar, 3rd ed.; SBP: Rio de Janeiro, Brazil, 2012; ISBN 978-85-88520-22-6. [Google Scholar]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Third Ten Years of the World Health Organization, 1st ed.; World Health Organization: Geneva, Switzerland, 2008; ISBN 978-92-4-156366-6. [Google Scholar]
- Fagerdahl, A.-M.; Boström, L.; Ulfvarson, J.; Bergström, G.; Ottosson, C. Translation and validation of the wound-specific quality of life instrument Cardiff Wound Impact Schedule in a Swedish population. Scand. J. Caring Sci. 2014, 28, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Klassen, A.F.; Klaassen, R.; Dix, D.; Pritchard, S.; Yanofsky, R.; O’Donnell, M.; Scott, A.; Sung, L. Impact of Caring for a Child With Cancer on Parents’ Health-Related Quality of Life. J. Clin. Oncol. 2008, 26, 5884–5889. [Google Scholar] [CrossRef] [PubMed]
- Witt, W.P.; Litzelman, K.; Wisk, L.E.; Spear, H.A.; Catrine, K.; Levin, N.; Gottlieb, C.A. Stress-mediated quality of life outcomes in parents of childhood cancer and brain tumor survivors: A case-control study. Qual. Life Res. 2010, 19, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Byström, I.-M.; Hollén, E.; Fälth-Magnusson, K.; Johansson, A. Health-Related Quality of Life in Children and Adolescents with Celiac Disease: From the Perspectives of Children and Parents. Gastroenterol. Res. Pract. 2012, 2012, 986475. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, J.C.; Kumar, P.; Dutta, A.K.; Basu, S.; Kumar, A. Assessment of dietary compliance to Gluten Free Diet and psychosocial problems in Indian children with celiac disease. Indian J. Pediatr. 2010, 77, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.; Rosenblum, S. Activities, Participation and Quality of Life Concepts in Children and Adolescents with Celiac Disease: A Scoping Review. Nutrients 2017, 9, 929. [Google Scholar] [CrossRef]
- Saxena, S.; Carlson, D.; Billington, R.; Orley, J. The WHO quality of life assessment instrument (WHOQOL-Bref): The importance of its items for cross-cultural research. Qual. Life Res. 2001, 10, 711–721. [Google Scholar] [CrossRef]
- Farage, P.; Zandonadi, R.P.; Ginani, V.C.; Gandolfi, L.; Nakano, E.Y.; Pratesi, R. Gluten-free diet: From development to assessment of a check-list designed for the prevention of gluten cross-contamination in food services. Nutrients 2018, 10, 1274. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 2008; ISBN 9780199231881. [Google Scholar]
- Streiner, D.L. Starting at the Beginning: An Introduction to Coefficient Alpha and Internal Consistency Starting at the Beginning: An Introduction to Coefficient Alpha and Internal Consistency. J. Pers. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Davidson, D.J.; Freudenburg, W.R. Gender and Environmental Risk Concerns. Environ. Behav. 1996, 28, 302–339. [Google Scholar] [CrossRef]
- Chen, M. Consumers’ health and taste attitude in Taiwan. Br. Food J. 2013, 115, 526–540. [Google Scholar] [CrossRef]
- Lee, A.R.; Wolf, R.; Contento, I.; Verdeli, H.; Green, P.H.R. Coeliac disease: The association between quality of life and social support network participation. J. Hum. Nutr. Diet. 2016, 29, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Herbert, L.J.; Clary, L.; Owen, V.; Monaghan, M.; Alvarez, V.; Streisand, R. Relations among school/daycare functioning, fear of hypoglycaemia and quality of life in parents of young children with type 1 diabetes. J. Clin. Nurs. 2015, 24, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Warschburger, P.; Kühne, D. Psychosocial determinants of quality of life in parents of obese children seeking inpatient treatment. Qual. Life Res. 2014, 23, 1985–1995. [Google Scholar] [CrossRef]
- Dardas, L.A.; Ahmad, M.M. Quality of life among parents of children with autistic disorder: A sample from the Arab world. Res. Dev. Disabil. 2014, 35, 278–287. [Google Scholar] [CrossRef]
- Jacobsson, L.R.; Friedrichsen, M.; Göransson, A.; Hallert, C. Impact of an Active Patient Education Program on Gastrointestinal Symptoms in Women With Celiac Disease Following a Gluten-Free Diet. Gastroenterol. Nurs. 2012, 35, 200–206. [Google Scholar] [CrossRef]
- Taylor, E.; Dickson-Swift, V.; Anderson, K. Coeliac disease: The path to diagnosis and the reality of living with the disease. J. Hum. Nutr. Diet. 2013, 26, 340–348. [Google Scholar] [CrossRef]
- Zandonadi, R.P.; Botelho, R.B.A.; Araújo, W.M.C. Psyllium as a Substitute for Gluten in Bread. J. Am. Diet. Assoc. 2009, 109, 1781–1784. [Google Scholar] [CrossRef]
- Araújo, H.M.C.; Araújo, W.M.C.; Botelho, R.B.A.; Zandonadi, R.P. Doença celíaca, hábitos e práticas alimentares e qualidade de vida. Rev. Nutr. 2010, 23, 467–474. [Google Scholar] [CrossRef]
- Zandonadi, R.P.; Botelho, R.B.A.; Gandolfi, L.; Ginani, J.S.; Montenegro, F.M.; Pratesi, R. Green Banana Pasta: An Alternative for Gluten-Free Diets. J. Acad. Nutr. Diet. 2012, 112, 1068–1072. [Google Scholar] [CrossRef] [PubMed]
- de Lima, B.R.; Botelho, R.B.A.; Zandonadi, R.P. Gluten-Free Pasta: Replacing Wheat with Chickpea. J. Culin. Sci. Technol. 2019, 17, 1–8. [Google Scholar] [CrossRef]
- Mehra, S.; Leffler, D.A.; Pallav, K.; Tariq, S.; Shah, S.; Green, P.H.; Hansen, J.; Dennis, M.; Kelly, C.P. Socioeconomic Status Influences Celiac Disease Diagnosis. Gastroenterology 2011, 140, S-438. [Google Scholar] [CrossRef]
- Tuominen, U.; Blom, M.; Hirvonen, J.; Seitsalo, S.; Lehto, M.; Paavolainen, P.; Hietanieni, K.; Rissanen, P.; Sintonen, H. The effect of co-morbidities on health-related quality of life in patients placed on the waiting list for total joint replacement. Health Qual. Life Outcomes 2007, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Feldman, J.M.; Ortega, A.N.; Koinis-Mitchell, D.; Kuo, A.A.; Canino, G. Child and Family Psychiatric and Psychological Factors Associated With Child Physical Health Problems. J. Nerv. Ment. Dis. 2010, 198, 272–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludvigsson, J.F.; Roy, A.; Lebwohl, B.; Green, P.H.R.; Emilsson, L. Anxiety and depression in caregivers of individuals with celiac disease—A population-based study. Dig. Liver Dis. 2017, 49, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Cabizuca, M.; Marques-Portella, C.; Mendlowicz, M.V.; Coutinho, E.S.F.; Figueira, I. Posttraumatic stress disorder in parents of children with chronic illnesses: A meta-analysis. Health Psychol. 2009, 28, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef]


{kind=link}
| Domain | N | Cronbach’s alpha (95% CI) | Floor Effect 1 | Ceiling Effect 2 |
|---|---|---|---|---|
| Emotional | 10 | 0.830 (0.786–0.868) | 0% | 2.7% |
| Worries | 10 | 0.821 (0.775–0.861) | 0% | 0% |
| Social | 10 | 0.829 (0.785–0.867) | 0% | 0.7% |
| TOTAL | 30 | 0.913 (0.892–0.932) | 0% | 0% |
| Domain | ||||
|---|---|---|---|---|
| Variable | Emotional M (SD) | Worries M (SD) | Social M (SD) | TOTAL M (SD) |
| Overall (n = 150) | 37.89 (7.37) | 25.49 (8.35) | 38.93 (7.76) | 102.31 (20.06) |
| Gender (n = 148) | ||||
| Female (n = 132) | 37.64 (7.32) A | 25.40 (8.34) A | 38.65 (7.71) A | 101.70 (19.76)A |
| Male (n = 16) | 40.06 (7.09) A | 25.81 (7.79) A | 41.06 (7.90) A | 106.94 (20.26)A |
| p * | 0.212 | 0.852 | 0.241 | 0.319 |
| Age (n = 147) | ||||
| Up to 30 years (n = 10) | 38.80 (7.64) A | 27.80 (7.61) A | 40.40 (6.35) A | 106.00 (20.53)A |
| 31 a 40 (n = 64) | 37.25 (6.94) A | 24.00 (7.54) A | 38.30 (6.89) A | 99.55 (18.18)A |
| 41 a 50 (n = 60) | 38.02 (8.04) A | 26.22 (9.18) A | 38.45 (8.70) A | 102.68 (22.18)A |
| Over 50 (n = 13) | 38.77 (6.34) A | 25.39 (8.38) A | 41.54 (8.36) A | 106.85 (18.27)A |
| p ** | 0.893 | 0.335 | 0.492 | 0.538 |
| Child/adolescent CD Diagnostic Time (n = 150) | ||||
| Up to 11 months (n = 8) | 35.88 (10.68) A | 26.75 (8.86) A | 39.50 (9.67) A | 102.13 (27.04) A |
| 12 a 23 months (n = 37) | 37.16 (6.37) A | 24.49 (7.24) A | 38.46 (8.10) A | 100.11 (18.13) A |
| 24 a 35 months (n = 18) | 37.22 (7.87) A | 21.39 (9.24) A | 37.22 (8.02) A | 95.83 (21.06) A |
| 36 a 59 months (n = 23) | 36.87 (7.61) A | 27.00 (7.07) A | 38.83 (6.73) A | 102.70 (17.81) A |
| Over 60 months (n = 64) | 39.13 (7.27) A | 26.52 (8.86) A | 39.64 (7.74) A | 105.28 (20.71) A |
| p ** | 0.507 | 0.148 | 0.815 | 0.447 |
| Education Level (n = 150) | ||||
| Elementary school (n = 15) | 36.73 (8.44) A | 23.00 (7.93) A | 38.20 (8.61) A | 97.93 (22.30) A |
| High School (n = 38) | 38.47 (6.18) A | 22.82 (7.76) A | 40.68 (5.47) A | 101.97 (15.12) A |
| College (n = 48) | 38.06 (7.73) A | 25.69 (7.78) A,B | 38.77 (8.85) A | 102.52 (21.54) A |
| Graduate or above (n = 49) | 37.63 (7.69) A | 28.12 (8.82) B | 37.94 (7.87) A | 103.69 (21.60) A |
| p ** | 0.877 | 0.016 | 0.412 | 0.813 |
| Marital status (n = 149) | ||||
| With partners (n = 135) | 37.97 (7.23) A | 25.33 (8.16) A | 39.05 (7.69) A | 102.36 (19.72 A |
| Without partners (n = 14) | 36.86 (9.05) A | 26.93 (10.52) A | 37.50 (8.79) A | 101.29 (24.51) A |
| p * | 0.593 | 0.500 | 0.479 | 0.851 |
| Occupation (n = 148) | ||||
| No (n = 37) | 37.32 (8.09) A | 23.54 (8.60) A | 38.92 (8.81) A | 99.78 (22.35) A |
| Yes (n = 111) | 38.07 (7.20) A | 26.04 (8.23) A | 38.88 (7.49) A | 102.99 (19.44) A |
| p * | 0.597 | 0.116 | 0.981 | 0.404 |
| Age of child with CD (n = 148) | ||||
| Up to 5 years (n = 25) | 37.40 (6.73) A | 22.84 (5.70) A | 38.16 (7.41) A | 98.40 (15.38) A |
| 6 a 10 (n = 59) | 38.25 (7.45) A | 25.25 (8.65) A | 39.03 (7.71) A | 105.54 (20.32) A |
| 11 a 15 (n = 46) | 36.83 (7.32) A | 26.02 (8.61) A | 38.43 (7.74) A | 101.28 (20.44) A |
| Over 16 (n = 18) | 40.22 (7.39) A | 28.50 (8.93) A | 40.94 (8.38) A | 109.67 (21.58) A |
| p ** | 0.382 | 0.162 | 0.647 | 0.312 |
| Gender of child with CD (n = 150) | ||||
| Female (n = 93) | 38.34 (7.40) A | 25.86 (8.54) A | 39.63 (7.27) A | 103.84 (19.76) A |
| Male (n = 57) | 37.16 (7.33) A | 24.88 (8.08) A | 37.77 (8.44) A | 99.81 (20.48) A |
| p * | 0.340 | 0.486 | 0.154 | 0.234 |
| Family income (n = 148) | ||||
| <1 MW *** (n = 14) | 37.64 (8.46) A | 20.07 (7.07) A | 39.43 (8.81) A | 97.14 (21.57) A |
| 1 a 3 MW (n = 36) | 36.25 (7.37) A | 22.25 (6.83) A,B | 38.11 (6.50) A | 96.61 (16.77) A |
| 3 a 6 MW (n = 32) | 38.38 (7.50) A | 26.75 (8.18) A,B,C | 39.41 (8.26) A | 104.53 (21.14) A |
| 6 a 9 MW (n = 24) | 36.25 (6.67) A | 25.96 (8.15) A,B,C | 37.83 (7.83) A | 100.04 (19.03) A |
| 9 a 12 MW (n = 16) | 39.00 (8.41) A | 27.75 (7.82) B,C | 37.44 (9.23) A | 104.19 (21.97) A |
| > 12 MW (n = 26) | 40.46 (6.49) A | 29.65 (9.39) C | 40.73 (7.58) A | 110.85 (20.82) A |
| p ** | 0.255 | 0.001 | 0.704 | 0.096 |
| Use of antidepressant or anti-anxiety medication (n = 150) | ||||
| No (n = 123) | 38.41 (7.43) A | 25.67 (8.38) A | 39.14 (7.65) A | 103.22 (20.24) A |
| Yes (n = 27) | 35.52 (6.73) A | 24.67 (8.34) A | 37.96 (8.35) A | 98.15 (19.05) A |
| p * | 0.064 | 0.575 | 0.478 | 0.236 |
| Does the child have any other illness besides the CD? (n = 148) | ||||
| No (n = 107) | 39.23 (6.71) A | 26.00 (8.22) A | 40.05 (7.12) A | 105.28 (18.57) A |
| Yes (n = 41) | 34.49 (8.08) B | 24.29 (8.76) A | 35.73 (8.64) B | 94.51 (22.25) B |
| p * | 0.000 | 0.269 | 0.002 | 0.003 |
| Do you have another relative with the CD? (n = 150) | ||||
| No (n = 99) | 38.63 (6.86) A | 25.07 (8.02) A | 39.38 (7.22) A | 103.08 (18.81) A |
| Yes (n = 51) | 36.47 (8.16) A | 26.29 (9.00) A | 38.04 (8.73) A | 100.80 (22.42) A |
| p * | 0.090 | 0.397 | 0.316 | 0.512 |
| Are you celiac? (n = 150) | ||||
| No (n = 128) | 37.86 (6.99) A | 24.98 (7.90) A | 38.88 (7.49) A | 101.72 (18.65) A |
| Yes (n = 22) | 38.09 (9.51) A | 28.45 (10.34) A | 39.18 (9.38) A | 105.73 (27.17) A |
| p * | 0.892 | 0.071 | 0.868 | 0.389 |
| Does your child experience discomfort or CD symptoms with gluten consumption? (n = 136) | ||||
| No (n = 22) | 35.14 (6.95) A | 25.91 (8.16) A | 38.64 (6.61) A | 99.68 (18.84) A |
| Yes (n = 114) | 37.74 (7.38) A | 25.30 (8.55) A | 38.41 (8.12) A | 101.45 (20.72) A |
| p * | 0.129 | 0.758 | 0.903 | 0.711 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abreu Paiva, L.M.; Gandolfi, L.; Pratesi, R.; Harumi Uenishi, R.; Puppin Zandonadi, R.; Nakano, E.Y.; Pratesi, C.B. Measuring Quality of Life in Parents or Caregivers of Children and Adolescents with Celiac Disease: Development and Content Validation of the Questionnaire. Nutrients 2019, 11, 2302. https://doi.org/10.3390/nu11102302
Abreu Paiva LM, Gandolfi L, Pratesi R, Harumi Uenishi R, Puppin Zandonadi R, Nakano EY, Pratesi CB. Measuring Quality of Life in Parents or Caregivers of Children and Adolescents with Celiac Disease: Development and Content Validation of the Questionnaire. Nutrients. 2019; 11(10):2302. https://doi.org/10.3390/nu11102302
Chicago/Turabian StyleAbreu Paiva, Liliane Maria, Lenora Gandolfi, Riccardo Pratesi, Rosa Harumi Uenishi, Renata Puppin Zandonadi, Eduardo Yoshio Nakano, and Claudia B. Pratesi. 2019. "Measuring Quality of Life in Parents or Caregivers of Children and Adolescents with Celiac Disease: Development and Content Validation of the Questionnaire" Nutrients 11, no. 10: 2302. https://doi.org/10.3390/nu11102302
APA StyleAbreu Paiva, L. M., Gandolfi, L., Pratesi, R., Harumi Uenishi, R., Puppin Zandonadi, R., Nakano, E. Y., & Pratesi, C. B. (2019). Measuring Quality of Life in Parents or Caregivers of Children and Adolescents with Celiac Disease: Development and Content Validation of the Questionnaire. Nutrients, 11(10), 2302. https://doi.org/10.3390/nu11102302