The Effect of Coffee Consumption on the Prevalence of Diabetes Mellitus: The 2012–2016 Korea National Health and Nutrition Examination Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
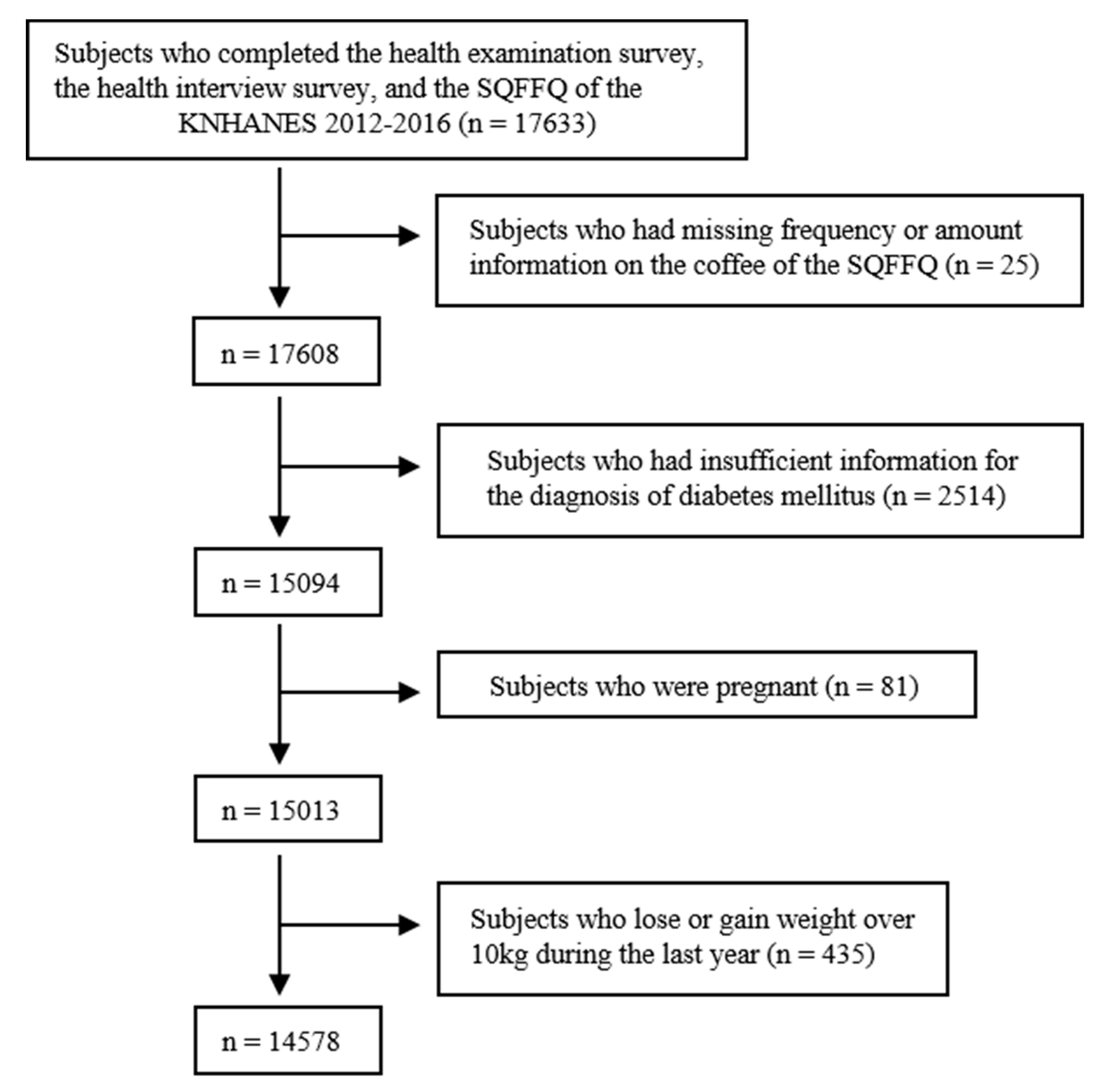
2.2. Subjects
2.3. Nutrition Survey
2.4. Health Interviews and Examinations
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Pattern of Coffee Consumption
3.3. The Association between Coffee Intake and Covariates
3.4. The Univariate Association between the Prevalence of Diabetes and Amount of Coffee Consumption
3.5. The Multivariate Association between the Prevalence of Diabetes and amount of Coffee Consumption with the Adjustment of Other Covariates
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. Korea Health Statistics 2016: Korea National Health and Nutrition Examination Survey (KNHANES VII-1). Available online: https://knhanes.cdc.go.kr/knhanes/sub04/sub04_03.do?classType = 7 (accessed on 25 September 2018).
- Youngsook.Oh. GAIN Report: Korea-Republic of, Coffee Market Brief Update. Available online: https://gain.fas.usda.gov/Recent%20GAIN%20Publications/Coffee%20Market%20Brief%20Update_Seoul%20ATO_Korea%20-%20Republic%20of_12-31-2015.pdf (accessed on 13 October 2018).
- Noh, J. The Diabetes Epidemic in Korea. Endocrinol. Metab. 2016, 31, 349–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlstrom, M.; Larsson, S.C. Coffee consumption and reduced risk of developing type 2 diabetes: A systematic review with meta-analysis. Nutr. Rev. 2018, 76, 395–417. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Zhang, D.; Jiang, W. Coffee and caffeine intake and incidence of type 2 diabetes mellitus: A meta-analysis of prospective studies. Eur. J. Nutr. 2014, 53, 25–38. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. Guideline for Analyzing the Data from the Seventh Korea National Health and Nutrition Examination Survey 2016–2017 (KNHANES VII). Available online: https://knhanes.cdc.go.kr/knhanes/sub03/sub03_06_02.do (accessed on 25 September 2018).
- Maruyama, K.; Kokubo, Y.; Yamanaka, T.; Watanabe, M.; Iso, H.; Okamura, T.; Miyamoto, Y. The reasonable reliability of a self-administered food frequency questionnaire for an urban, Japanese, middle-aged population: The Suita study. Nutr. Res. 2015, 35, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.W.; Song, S.; Lee, J.E.; Oh, K.; Shim, J.; Kweon, S.; Paik, H.Y.; Joung, H. Reproducibility and validity of an FFQ developed for the Korea National Health and Nutrition Examination Survey (KNHANES). Public Health Nutr. 2015, 18, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Kim, N.S.; Lee, B.K.; Park, S. Carbohydrate Intake Exhibited a Positive Association with the Risk of Metabolic Syndrome in Both Semi-Quantitative Food Frequency Questionnaires and 24-Hour Recall in Women. J. Korean Med. Sci. 2017, 32, 1474–1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Zimmet, P.; Shaw, J. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef] [PubMed]
- Kim, H.J.; Cho, S.; Jacobs, D.R., Jr.; Park, K. Instant coffee consumption may be associated with higher risk of metabolic syndrome in Korean adults. Diabetes Res. Clin. Pract. 2014, 106, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Kim, K.; Park, S.M. Association between the Prevalence of Metabolic Syndrome and the Level of Coffee Consumption among Korean Women. PLoS ONE 2016, 11, e0167007. [Google Scholar] [CrossRef] [PubMed]
- van Dam, R.M.; Dekker, J.M.; Nijpels, G.; Stehouwer, C.D.; Bouter, L.M.; Heine, R.J. Coffee consumption and incidence of impaired fasting glucose, impaired glucose tolerance, and type 2 diabetes: The Hoorn Study. Diabetologia 2004, 47, 2152–2159. [Google Scholar] [CrossRef] [PubMed]
- Arnlov, J.; Vessby, B.; Riserus, U. Coffee consumption and insulin sensitivity. JAMA 2004, 291, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- van Dam, R.M.; Hu, F.B. Coffee consumption and risk of type 2 diabetes: A systematic review. JAMA 2005, 294, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Noda, M.; Inoue, M.; Kadowaki, T.; Tsugane, S. Psychological factors, coffee and risk of diabetes mellitus among middle-aged Japanese: A population-based prospective study in the JPHC study cohort. Endocr. J. 2009, 56, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Oba, S.; Nagata, C.; Nakamura, K.; Fujii, K.; Kawachi, T.; Takatsuka, N.; Shimizu, H. Consumption of coffee, green tea, oolong tea, black tea, chocolate snacks and the caffeine content in relation to risk of diabetes in Japanese men and women. Br. J. Nutr. 2010, 103, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Odegaard, A.O.; Pereira, M.A.; Koh, W.P.; Arakawa, K.; Lee, H.P.; Yu, M.C. Coffee, tea, and incident type 2 diabetes: The Singapore Chinese Health Study. Am. J. Clin. Nutr. 2008, 88, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Kim, K.; Ahn, Y.; Yang, M.; Lee, J.E. Habitual coffee intake, genetic polymorphisms, and type 2 diabetes. Eur. J. Endocrinol. 2015, 172, 595–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, F.; Oh, J.; Lee, K.; Cho, M.S. The effect of coffee consumption on food group intake, nutrient intake, and metabolic syndrome of Korean adults—2010 KNHANES (V-1). NFS J. 2016, 4, 9–14. [Google Scholar] [CrossRef]
- Akash, M.S.; Rehman, K.; Chen, S. Effects of coffee on type 2 diabetes mellitus. Nutrition 2014, 30, 755–763. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Young Adult (Age 19–39) | Middle-Aged Adult (Age 40–64) | ||||
|---|---|---|---|---|---|
| Women (N = 5,579,373) | Men (N = 6,130,535) | Women (N = 7,416,029) | Men (N = 7,119,478) | p | |
| Mean Age (years) | 29.38 ± 0.15 a | 29.51 ± 0.16 a | 51.02 ± 0.12 b | 50.48 ± 0.14 c | <0.0001 |
| Body Weight (kg) | 56.66 ± 0.20 a | 73.56 ± 0.29 b | 58.61 ± 0.14 c | 71.02 ± 0.20 d | <0.0001 |
| BMI (kg/m2) | 21.80 ± 0.07 a | 24.16 ± 0.09 b | 23.72 ± 0.06 c | 24.49 ± 0.06 d | <0.0001 |
| Current Smoker | 411,539 (7) | 2,555,421 (42) | 301,593 (4) | 2,858,968 (40) | <0.0001 |
| Heavy Drinker | 763,917 (14) | 1,706,586 (28) | 714,970 (10) | 2,851,558 (40) | <0.0001 |
| Physically Active | 2,240,542 (41) | 2,969,281 (49) | 2,801,378 (38) | 2,531,374 (36) | <0.0001 |
| Income Level | <0.0001 | ||||
| Low Income | 369,342 (7) | 490,542 (8) | 786,214 (11) | 529,770 (7) | |
| Mid-Low Income | 1,432,383 (26) | 1,488,747 (24) | 1,777,991 (24) | 1,574,359 (22) | |
| Mid-High Income | 1,917,837 (35) | 2,102,974 (34) | 2,193,064 (30) | 2,243,656 (32) | |
| High Income | 1,821,332 (33) | 2,042,590 (33) | 2,633,432 (36) | 2,723,137 (39) | |
| Education Level | <0.0001 | ||||
| High School or Under | 2,331,315 (42) | 2,997,834 (50) | 5,414,623 (74) | 4,052,194 (58) | |
| College or Higher | 3,203,207 (58) | 3,057,928 (50) | 1,943,892 (26) | 2,972,194 (42) | |
| Systolic BP (mmHg) | 105.03 ± 0.2 a | 115.15 ± 0.28 b | 116.24 ± 0.28 c | 120.62 ± 0.3 d | <0.0001 |
| Diastolic BP (mmHg) | 69.84 ± 0.18 a | 76.48 ± 0.24 b | 75.47 ± 0.17 c | 80.84 ± 0.2 d | <0.0001 |
| Fasting Glucose (mg/dL) | 90.25 ± 0.35 a | 92.5 ± 0.34 b | 98.57 ± 0.39 c | 104.13 ± 0.46 d | <0.0001 |
| HbA1c (%) | 5.38 ± 0.01 a | 5.42 ± 0.01 b | 5.74 ± 0.01 c | 5.84 ± 0.02 d | <0.0001 |
| Hypertension | 257,519 (5%) | 1,318,652 (22%) | 241,172 (33%) | 3,340,347 (47%) | <0.0001 |
| Hypertriglyceridemia | 486,991 (9) | 1,901,180 (31) | 1,768,660 (24) | 3,245,247 (46) | <0.0001 |
| Reduced HDL | 1,597,322 (29) | 1,126,280 (18) | 3,103,717 (42) | 1,926,039 (27) | <0.0001 |
| Total Energy Intake (kcal/day) | 1966.4 ± 16.34 a | 2607.5 ± 22.22 b | 1729.2 ± 9.99 c | 2274.4 ± 15.26 d | <0.0001 |
| Young Adult (Age 19–39) | Middle-Aged Adult (Age 40–64) | ||||
|---|---|---|---|---|---|
| Women (N = 5,579,373) | Men (N = 6,130,535) | Women (N = 7,416,029) | Men (N = 7,119,478) | p | |
| Mean Consumption Frequency/Week (tsp) | |||||
| 8.01 ± 0.18 a | 10.4 ± 0.26 b | 10.68 ± 0.14 b | 15.12 ± 0.21 c | <0.0001 | |
| Consumption Amount/Intake | |||||
| 1tsp | 2,377,591 (43%) | 314,370 (51%) | 5,334,981 (72%) | 5,682,974 (80%) | <0.0001 |
| 2tsp | 784,604 (14%) | 832,930 (14%) | 749,002 (10%) | 520,995 (7%) | |
| 3tsp or more | 1,471,631 (26%) | 1,244,819 (20%) | 520,955 (7%) | 427,880 (6%) | |
| Consumption Amount/Day (tsp) | |||||
| 1.97 ± 0.05 a | 2.24 ± 0.07 b | 1.97 ± 0.03 a | 2.72 ± 0.05 c | <0.0001 | |
| Young Adult (Age 19–39) | Middle-Aged Adult (Age 40–64) | ||||||
|---|---|---|---|---|---|---|---|
| Women (N = 5,579,373) | Men (N = 6,130,535) | Women (N = 7,416,029) | Men (N = 7,119,478) | ||||
| β | p | β | p | β | p | β | p |
| −0.4158 | <0.001 | −0.3485 | <0.001 | −0.4095 | <0.001 | −0.3212 | <0.001 |
| Young Adult (Age 19–39) | Middle-Aged Adult (Age 40–64) | |||||||
|---|---|---|---|---|---|---|---|---|
| Women (N = 5,579,373) | Men (N = 6,130,535) | Women (N = 7,416,029) | Men (N = 7,119,478) | |||||
| β | p | β | p | β | p | β | p | |
| Mean age (years) | 0.054 | <0.0001 | 0.127 | <0.0001 | −0.061 | <0.0001 | −0.056 | <0.0001 |
| Body weight (kg) | 0.009 | 0.108 | 0.015 | 0.008 | 0.009 | 0.034 | 0.008 | 0.08 |
| BMI (kg/m2) | 0.016 | 0.281 | 0.046 | 0.012 | −0.002 | 0.821 | 0.008 | 0.569 |
| Current smoker | 1.225 | <0.0001 | 1.347 | <0.0001 | 1.352 | <0.0001 | 1.236 | <0.0001 |
| Frequent alcohol consumption | 0.690 | <0.0001 | 0.524 | 0.001 | 0.574 | <0.0001 | 0.049 | 0.66 |
| Physically active | 0.267 | <0.0001 | −0.221 | 0.148 | −0.149 | 0.019 | −0.041 | 0.699 |
| Income level | ||||||||
| Low income | ref | ref | ref | ref | ||||
| Mid-low income | −0.104 | 0.952 | 0.478 | 0.033 | 0.207 | 0.053 | 0.535 | 0.016 |
| Mid-high income | 0.314 | 0.063 | 0.859 | <0.0001 | 0.288 | 0.005 | 0.550 | 0.005 |
| High income | 0.627 | 0.001 | 1.034 | <0.0001 | 0.560 | <0.0001 | 0.606 | 0.001 |
| Education level | ||||||||
| High school or under | ref | ref | ref | ref | ||||
| College or more | 0.366 | 0.001 | 0.641 | <0.0001 | 0.646 | <0.0001 | 0.202 | 0.06 |
| Fasting glucose (mg/dL) | 0.002 | 0.486 | 0.008 | 0.104 | −0.002 | 0.115 | −0.004 | 0.021 |
| HbA1c (%) | 0.036 | 0.663 | 0.449 | 0.008 | −0.146 | <0.0001 | −0.066 | 0.245 |
| Total cholesterol (mg/dL) | 0.007 | <0.0001 | 0.009 | <0.0001 | 0.001 | 0.238 | 0.005 | <0.0001 |
| Triglyceride (mg/dL) | 0.001 | 0.2 | 0.001 | 0.004 | −0.001 | <0.0001 | 0.001 | 0.716 |
| HDL (mg/dL) | 0.009 | 0.104 | −0.021 | 0.002 | 0.014 | <0.0001 | −0.015 | <0.0001 |
| Total energy intake (kcal/day) | 0.000 | 0.147 | 0.000 | <0.0001 | 0.000 | <0.0001 | 0.000 | <0.0001 |
| Young Adult (Age 19–39) | Middle-Aged Adult (Age 40–64) | |||||||
|---|---|---|---|---|---|---|---|---|
| Women (N = 5,579,373) | Men (N = 6,130,535) | Women (N = 7,416,029) | Men (N = 7,119,478) | |||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| DM | ||||||||
| Model 1 | 0.861 (0.716–1.004) | 0.079 | 0.977 (0.880–1.075) | 0.653 | 0.918 (0.851–0.986) | 0.023 | 0.934 (0.880–0.989) | 0.022 |
| Model 2 | 0.874 (0.727–1.021) | 0.117 | 0.977 (0.882–1.071) | 0.631 | 0.929 (0.861–0.997) | 0.048 | 0.939 (0.883–0.994) | 0.038 |
| High fasting glucose | ||||||||
| Model 1 | 0.941 (0.874–1.009) | 0.098 | 0.985 (0.941–1.029) | 0.510 | 0.946 (0.908–0.984) | 0.007 | 0.961 (0.930–0.993) | 0.018 |
| Model 2 | 0.948 (0.880–1.016) | 0.147 | 0.976 (0.930–1.022) | 0.316 | 0.952 (0.914–0.990) | 0.018 | 0.958 (0.927–0.990) | 0.011 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, Y.; Park, Y.; Choi, S.K.; Ahn, S.; Ohn, J.H. The Effect of Coffee Consumption on the Prevalence of Diabetes Mellitus: The 2012–2016 Korea National Health and Nutrition Examination Survey. Nutrients 2019, 11, 2377. https://doi.org/10.3390/nu11102377
Lim Y, Park Y, Choi SK, Ahn S, Ohn JH. The Effect of Coffee Consumption on the Prevalence of Diabetes Mellitus: The 2012–2016 Korea National Health and Nutrition Examination Survey. Nutrients. 2019; 11(10):2377. https://doi.org/10.3390/nu11102377
Chicago/Turabian StyleLim, Yejee, Youngmi Park, Sun Kyu Choi, Soyeon Ahn, and Jung Hun Ohn. 2019. "The Effect of Coffee Consumption on the Prevalence of Diabetes Mellitus: The 2012–2016 Korea National Health and Nutrition Examination Survey" Nutrients 11, no. 10: 2377. https://doi.org/10.3390/nu11102377
APA StyleLim, Y., Park, Y., Choi, S. K., Ahn, S., & Ohn, J. H. (2019). The Effect of Coffee Consumption on the Prevalence of Diabetes Mellitus: The 2012–2016 Korea National Health and Nutrition Examination Survey. Nutrients, 11(10), 2377. https://doi.org/10.3390/nu11102377