Dietary and Plasma Carboxymethyl Lysine and Tumor Necrosis Factor-α as Mediators of Body Mass Index and Waist Circumference among Women in Indonesia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
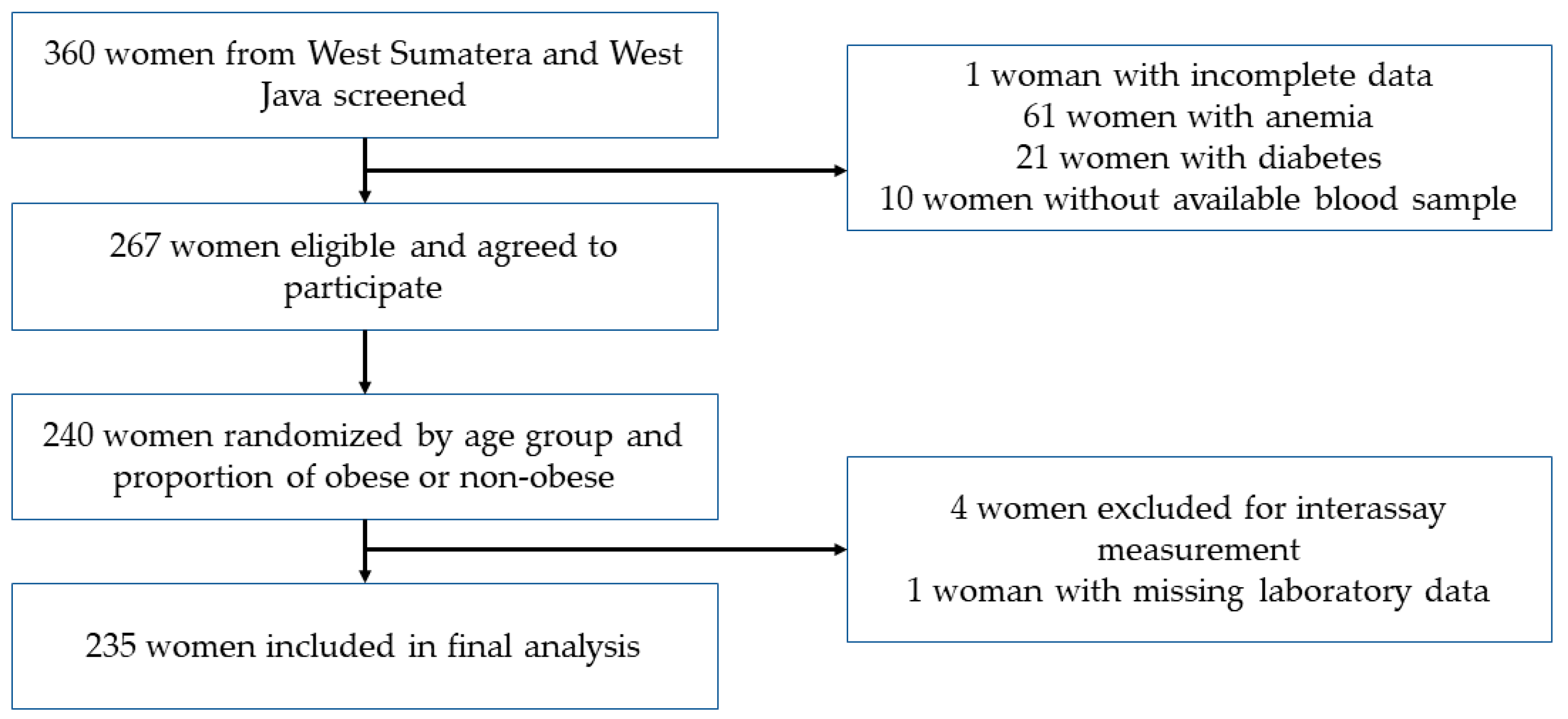
2.1. Subjects and Study Design
2.2. Dietary Carboxymethyl Lysine
2.3. Anthropometric Assessments
2.4. Physical Activity
2.5. Measurement of Plasma CML and Plasma TNF-α
2.6. Statistical Analysis
3. Results
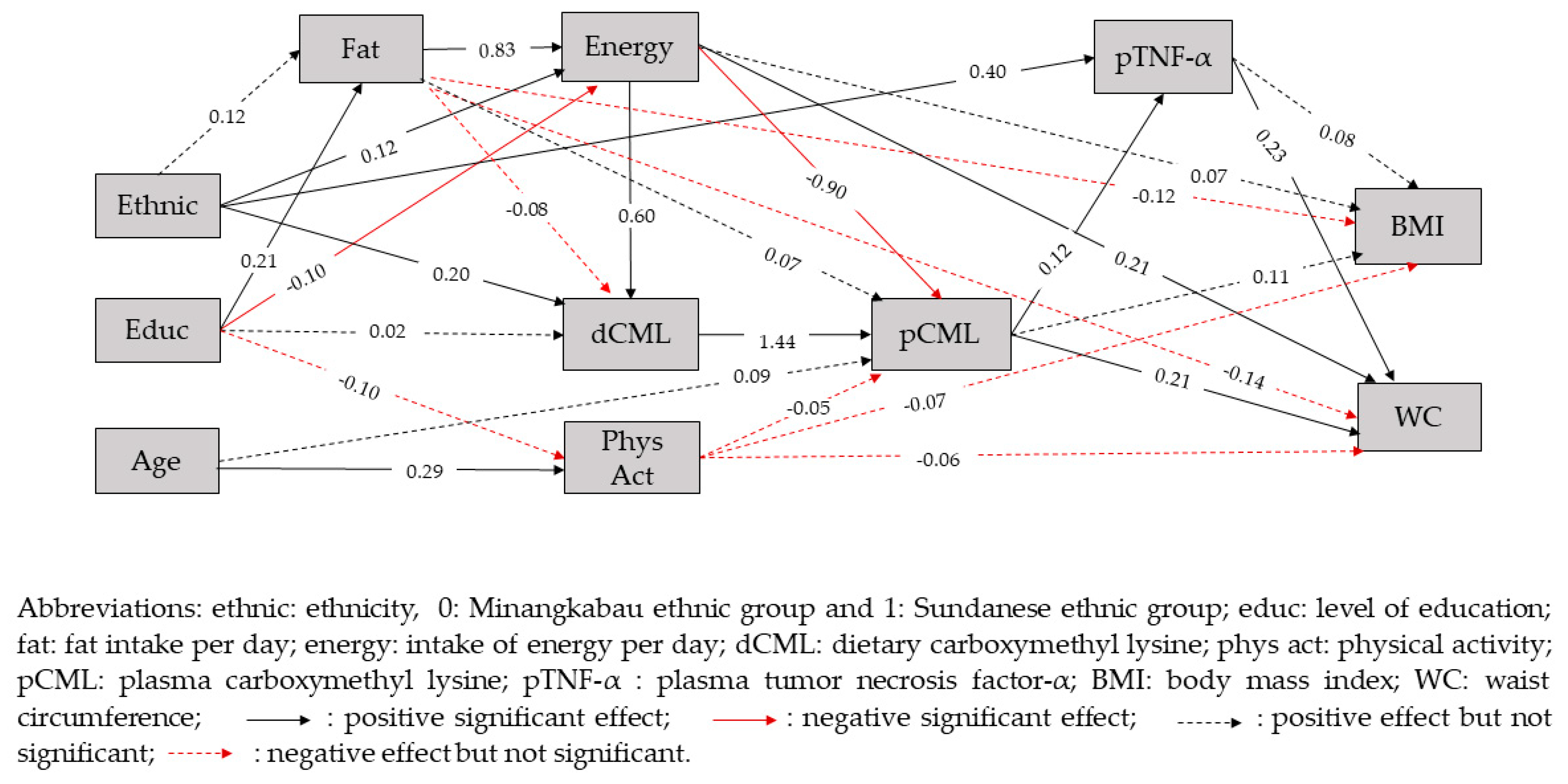
SEM Pathways
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harbuwono, D.S.; Pramono, L.A.; Yunir, E.; Subekti, I. Obesity and central obesity in Indonesia: Evidence from a national health survey. Med. J. Indones 2018, 27, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Badan Penelitian dan Pengembangan Kesehatan KKRI [National Institute of Health Research and Development Ministry of Health of the Republic of Indonesia]. Hasil Riset Kesehatan Dasar (RISKESDAS) Indonesia. 2018. [Google Scholar]
- Hardinsyah. Analysis intake of fat, sugar, and salt of Indonesians. Gizi Indon 2011, 34, 92–100. [Google Scholar]
- Caballero, B. The global epidemic of obesity: An overview. Epidemiol Rev. 2007, 29, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M. Nutrition transition and the global diabetes epidemic. Curr. Diab. Rep. 2015, 15, 64. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. The global nutrition transition: The pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Kellow, N.J.; Coughlan, M.T. Effect of diet-derived advanced glycation end products on inflammation. Nutr. Rev. 2015, 73, 737–759. [Google Scholar] [CrossRef]
- Kellow, N.J.; Savige, G.S. Dietary advanced glycation end-product restriction for the attenuation of insulin resistance, oxidative stress and endothelial dysfunction: A systematic review. Eur. J. Clin. Nutr. 2013, 67, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Semba, R.D.; Arab, L.; Sun, K.; Nicklett, E.J.; Ferrucci, L. Fat mass is inversely associated with serum carboxymethyl-lysine, an advanced glycation end product, in adults. J. Nutr. 2011, 141, 1726–1730. [Google Scholar] [CrossRef]
- Uribarri, J.; Cai, W.; Peppa, M.; Goodman, S.; Ferrucci, L.; Striker, G.; Vlassara, H. Circulating glycotoxins and dietary advanced glycation endproducts: Two links to inflammatory response, oxidative stress, and aging. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Snelson, M.; Coughlan, M.T. Dietary advanced glycation end products: Digestion, metabolism and modulation of gut microbial ecology. Nutrients 2019, 11, 215. [Google Scholar] [CrossRef] [Green Version]
- Ottum, M.S.; Mistry, A.M. Advanced glycation end products: Modifiable environmental factors profoundly mediate insulin resistance. J. Clin. Biochem. Nutr. 2015, 57, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koschinsky, T.; He, C.-J.; Mitsuhashi, T.; Bucala, R.; Liu, C.; Buenting, C.; Heitmann, K.; Vlassara, H. Orally absorbed reactive glycation products (glycotoxins): An environmental risk factor in diabetic nephropathy. Proc. Natl. Acad. Sci. USA 1997, 94, 6474–6479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uribarri, J.; Woodruff, S.; Goodman, S.; Cai, W.; Chen, X.; Pyzik, R.; Yong, A.; Striker, G.E.; Vlassara, H. Advanced glycation end products in foods and a practical guide to their reduction in the diet. J. Am. Diet. Assoc. 2010, 110, 911–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaens, K.H.J.; Ferreira, I.; van de Waarenburg, M.P.H.; van Greevenbroek, M.M.; van der Kallen, C.J.H.; Dekker, J.M.; Nijpels, G.; Rensen, S.S.; Stehouwer, C.D.A.; Schalkwijk, C.G. Protein-bound plasma Nε-(carboxymethyl) lysine is inversely associated with central obesity and inflammation and significantly explain a part of the central obesity–related increase in inflammation: The Hoorn and CODAM studies. Arter. Thromb Vasc. Biol. 2015, 35, 2707–2713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.K.; Rai, M.; Rehkopf, D.H.; Abrams, B. Educational attainment and obesity: A systematic review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2013, 14, 989–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arroyo-Johnson, C.; Mincey, K.D. Obesity epidemiology worldwide. Gastroenterol Clin. North. Am. 2016, 45, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Drenth, H.; Zuidema, S.U.; Krijnen, W.P.; Bautmans, I.; Smit, A.J.; van der Schans, C.; Hobbelen, H. Advanced glycation end products are associated with physical activity and physical functioning in the older population. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1545–1551. [Google Scholar] [CrossRef]
- Gu, Q.; Wang, B.; Zhang, X.F.; Ma, Y.P.; Liu, J.D.; Wang, X.Z. Contribution of receptor for advanced glycation end products to vasculature-protecting effects of exercise training in aged rats. Eur. J. Pharmacol. 2014, 741, 186–194. [Google Scholar] [CrossRef]
- Maessen, M.F.H.; Schalkwijk, C.G.; Verheggen, R.J.H.M.; Aengevaeren, V.L.; Maria, T.E.H.; Eijsvogels, T.M.H. A comparison of dicarbonyl stress and advanced glycation endproducts in lifelong endurance athletes vs. sedentary controls. J. Sci. Med. Sport. 2017, 20, 921–926. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, K.; Muniandy, S.; Ismail, I.S.; Saif-Ali, R.; Al-Hamodi, Z. Evaluation of Nε-carboxymethyl lysine and lipid peroxidation in multiethnic Malaysian subjects with type 2 diabetes mellitus. J. Clin. Biochem. Nutr. 2007, 41, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Bastos, D.M.; Monaro, É.; Siguemoto, É.; Séfora, M. Maillard reaction products in processed food: Pros and cons. In Food Industrial Processes-Methods and Equipment; Benjamin, V., Ed.; InTech: Rijeka, Croatia, 2012; pp. 281–300. Available online: https://www.intechopen.com/books/food-industrial-processes-methods-and-equipment/maillard-reaction-products-in-processed-food-pros-and-cons (accessed on 4 November 2019). [CrossRef] [Green Version]
- Sadowska-Bartosz, I.; Bartosz, G. Prevention of protein glycation by natural compounds. Molecules 2015, 20, 3309–3334. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, T.; Barto, R.; Ten Brink, H.J.; Schalkwijk, C.G. Measurement of Nε-(carboxymethyl)lysine and Nε-(carboxyethyl)lysine in human plasma protein by stable-isotope-dilution tandem mass spectrometry. Clin. Chem. 2004, 50, 1222–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semba, R.D.; Ang, A.; Talegawkar, S.; Crasto, C.; Dalal, M.; Jardack, P.; Traber, M.G.; Ferrucci, L.; Arab, L. Dietary intake associated with serum versus urinary carboxymethyl-lysine, a major advanced glycation end product, in adults: The Energetics Study. Eur. J. Clin. Nutr. 2012, 66, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, W.; He, J.C.; Zhu, L.; Peppa, M.; Lu, C.; Uribarri, J.; Vlassara, H. High levels of dietary advanced glycation end products transform low-density lipoprotein into a potent redox-sensitive mitogen-activated protein kinase stimulant in diabetic patients. Circulation 2004, 110, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Lan, K.-C.; Chiu, C.-Y.; Kao, C.-W.; Huang, K.-H.; Wang, C.-C.; Huang, K.-T.; Tsai, K.-S.; Sheu, M.-L.; Liu, S.H. Advanced glycation end-products induce apoptosis in pancreatic islet endothelial cells via NF-κB-activated cyclooxygenase-2/prostaglandin E2 up-regulation. PLoS ONE 2015, 10, e0124418. [Google Scholar] [CrossRef]
- Gupta, A.; Uribarri, J. Dietary advanced glycation end products and their potential role in cardiometabolic disease in children. Horm. Res. Paediatr. 2016, 85, 291–300. [Google Scholar] [CrossRef]
- Lipoeto, N.I.; Agus, Z.; Oenzil, F.; Masrul, M.; Wattanapenpaiboon, N.; Wahlqvist, M.L. Contemporary Minangkabau food culture in West Sumatra, Indonesia. Asia Pacific J. Clin. Nutr. 2001, 10, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Budiningsih, S.; Ohnot, Y.; Prihartono, J.; Dillon, D.S.; Tjahjadi, G.; Soetrisno, E.; Hardjolukito, E.; Ramli, M.; Darwis, I.; Tjindarbumi, D.; et al. Breast cancer risk factors among Sundanese and other ethnic groups in Indonesia. Med. J. Indones 1999, 8, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Uribarri, J.; Cai, W.; Woodward, M.; Tripp, E.; Goldberg, L.; Pyzik, R.; Yee, K.; Tansman, L.; Chen, X.; Mani, V.; et al. Elevated serum advanced glycation endproducts in obese indicate risk for the metabolic syndrome: A link between healthy and unhealthy obesity? J. Clin. Endocrinol. Metab. 2015, 100, 1957–1966. [Google Scholar] [CrossRef]
- Foroumandi, E.; Alizadeh, M.; Kheirouri, S.; Asghari Jafarabadi, M. Exploring the role of body mass index in relationship of serum nitric oxide and advanced glycation end products in apparently healthy subjects. PLoS ONE 2019, 14, e0213307. [Google Scholar] [CrossRef]
- Stefani, S.; Ngatidjan, S.; Paotiana, M.; Sitompul, K.A.; Abdullah, M.; Sulistianingsih, D.P.; Shankar, A.H.; Agustina, R. Dietary quality of predominantly traditional diets is associated with blood glucose profiles, but not with total fecal Bifidobacterium in Indonesian women. PLoS ONE 2018, 13, e0208815. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.; Chou, C.-P. Practical issue in structural modeling. Socio. Meth. Res. 1987, 16, 78–117. [Google Scholar] [CrossRef]
- Ministry of Health of the Republic of Indonesia. Buku Foto makanan. In Survei konsumsi makanan individu [Book of Food Dish Photographs from Survey of Individual Food Consumption]; Pusat Teknologi Terapan Kesehatan dan Epidemiologi Klinik Badan Penelitian dan Pengembangan Kesehatan Kementerian Kesehatan Indonesia; Ministry of Health of the Republic of Indonesia: Bogor, Indonesia, 2014. [Google Scholar]
- Liman, P.B.; Djuwita, R.; Agustina, R. Database development of carboxymethyl lysine content in foods consumed by Indonesian women in two selected provinces. J. Int. Dent. Med. Res. 2019, 12, 268–277. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A Report of the american college of cardiology/American heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Sciomer, S.; Moscucci, F.; Maffei, S.; Gallina, S.; Mattioli, A. Prevention of cardiovascular risk factors in women: The lifestyle paradox and stereotypes we need to defeat. Eur. J. Prev. Cardiol. 2018, 26, 2047487318810560. [Google Scholar] [CrossRef]
- Bots, S.H.; Peters, S.A.E.; Woodward, M. Sex differences in coronary heart disease and stroke mortality: A global assessment of the effect of ageing between 1980 and 2010. BMJ Glob. Health 2017, 2, e000298. [Google Scholar] [CrossRef] [Green Version]
- Marais, G.A.B.; Gaillard, J.M.; Vieira, C.; Plotton, I.; Sanlaville, D.; Gueyffier, F.; Lemaitre, J.F. Sex gap in aging and longevity: Can sex chromosomes play a role? Biol. Sex Differ. 2018, 9, 33. [Google Scholar] [CrossRef]
- Crimmins, E.M.; Shim, H.; Zhang, Y.S.; Kim, J.K. Differences between Men and Women in Mortality and the Health Dimensions of the Morbidity Process. Clin. Chem. 2019, 65, 135–145. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.T.; Van der Fels-Klerx, H.J.; Van Boekel, M.A.J.S. N ϵ-(carboxymethyl)lysine: A review on analytical methods, formation, and occurrence in processed food, and health impact. Food Rev. Int. 2014, 30, 36–52. [Google Scholar] [CrossRef]
- Semba, R.D.; Beck, J.; Sun, K.; Egan, J.M.; Carlson, O.D.; Varadhan, R.; Ferrucci, L. Relationship of a dominant advanced glycation end product, serum carboxymethyl-lysine, and abnormal glucose metabolism in adults: The Baltimore Longitudinal Study of Aging. J. Nutr. Health Aging. 2010, 14, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaens, K.H.J.; Goossens, G.H.; Niessen, P.M.; van Greevenbroek, M.M.; van der Kallen, C.J.H.; Niessen, H.W.; Rensen, S.S.; Buurman, W.A.; Greve, J.W.M.; Blaak, E.E.; et al. Nε-(carboxymethyl)lysine-receptor for advanced glycation end product axis is a key modulator of obesity-induced dysregulation of adipokine expression and insulin resistance. Arter. Thromb. Vasc. Biol. 2014, 34, 1199–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Greevenbroek, M.; Schalkwijk, C.; Stehouwer, C. Obesity-associated low grade inflammation in type 2 diabetes mellitus: Causes and consequences. Neth. J. Med. 2013, 71, 174–187. [Google Scholar] [PubMed]
- Jung, U.J.; Choi, M.-S. Obesity and its metabolic complications: The role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int. J. Mol. Sci. 2014, 15, 6184–6223. [Google Scholar] [CrossRef] [Green Version]
- Park, H.S.; Park, J.Y.; Yu, R. Relationship of obesity and visceral adiposity with serum concentrations of CRP, TNF-α and IL-6. Diabetes Res. Clin. Pract. 2005, 69, 29–53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Body Mass Index | Waist Circumference | ||||
|---|---|---|---|---|---|---|
| Non-Obese (n = 121) | Obese (n = 114) | p-Value a | Non-Central Obesity (n = 104) | Central Obesity (n = 131) | p-Value b | |
| Age (years) | 36 (28–43) ‡ | 38 (31–44) ‡ | 0.541 | 36 (27–43) ‡ * | 38 (32–44) ‡ * | 0.031 |
| Age group in years (n, %) | ||||||
| 19–40 | 78 (64.5) | 72 (63.2) | 0.942 | 70 (67.3) | 80 (61.1) | 0.394 |
| 41–50 | 43 (35.5) | 42 (36.8) | 34 (32.7) | 51 (38.9) | ||
| Education (n, %) | ||||||
| Low | 31 (25.6) | 40 (35.1) | 0.151 | 31 (29.8) | 40 (30.5) | >0.999 |
| Middle | 90 (74.4) | 72 (63.2) | 73 (70.2) | 91 (69.5) | ||
| Ethnic group (n, %) | ||||||
| Minangkabau | 67 (55.4) | 50 (43.9) | 0.102 | 63 (60.6) * | 54 (41.2) * | 0.005 |
| Sundanese | 54 (44.6) | 64 (56.1) | 41 (39.4) | 77 (58.8) | ||
| Physical activity (n, %) | ||||||
| Inactive | 85 (70.2) | 89 (78.1) | 0.172 | 74 (71.2) | 100 (76.3) | 0.368 |
| Active | 36 (29.8) | 25 (21.9) | 30 (28.8) | 31 (23.7) | ||
| Variable | Body Mass Index | Waist Circumference | ||||
|---|---|---|---|---|---|---|
| Non-Obese (n = 121) | Obese (n = 114) | p-Value a | Non-Central Obese (n = 104) | Central Obese (n = 131) | p-Value b | |
| Dietary CML (mg/day) | 2.1 (1.7–2.9) ‡ | 2.3 (1.7–3.2) ‡ | 0.206 | 2.1 (1.7–2.6) ‡ * | 2.3 (1.7–3.4) ‡ * | 0.040 |
| Plasma CML (ng/mL) | 22.3 (17.2–27.3) ‡ | 22.2 (17.3–30.2) ‡ | 0.177 | 21.0 (16.8–26.8) ‡ * | 23.2 (18.4–30.1) ‡ * | 0.026 |
| TNF-α (IU/mL) | 0.64 (0.51–0.92) ‡ | 0.72 (0.54–1.08) ‡ | 0.095 | 0.62 (0.48–0.77) ‡ ** | 0.76 (0.54–1.22) ‡ ** | <0.001 |
| Effect | β (95% CI) | p-Value | Effect | β (95% CI) | p-Value |
|---|---|---|---|---|---|
| Direct effect on WC | Direct effect on BMI | ||||
| pTNF-α | 0.23 (0.11, 0.35) | <0.001 ** | pTNF-α | 0.08 (−0.06, 0.20) | 0.131 |
| pCML | 0.21 (0.09, 0.33) | 0.001 * | pCML | 0.11 (−0.02, 0.24) | 0.046 |
| Fat | −0.14 (−0.34, 0.07) | 0.095 | Fat | −0.12 (−0.34, 0.10) | 0.136 |
| Energy | 0.21 (0.00, 0.41) | 0.025 * | Energy | 0.07 (−0.15, 0.29) | 0.263 |
| Phys Act | −0.06 (−0.18, 0.06) | 0.155 | Phys Act | −0.07 (−0.20, 0.05) | 0.132 |
| Direct effect on pTNF-α | Direct effect on intake of fat | ||||
| Ethnic | 0.40 (0.28, 0.49) | <0.001 ** | Educ | 0.21 (0.08, 0.33) | 0.001 ** |
| pCML | 0.12 (0.00, 0.24) | 0.024 * | Ethnic | 0.12 (−0.02, 0.24) | 0.041 |
| Direct effect on pCML | Direct effect on intake of energy | ||||
| dCML | 1.44 (0.70, 3.23) | <0.001 ** | Ethnic | 0.12 (0.05, 0.19) | 0.001 * |
| Energy | −0.90 (−2.21, −0.31) | 0.001 * | Fat | 0.83 (0.78, 0.87) | <0.001 ** |
| Fat | 0.07 (−0.27, 0.54) | 0.347 | Educ | −0.10 (−0.18, 0.03) | 0.003 * |
| Age | 0.09 (−0.05, 0.21) | 0.100 | |||
| Phys Act | −0.05 (−0.18, 0.08) | 0.238 | |||
| Direct effect on dCML | Direct effect on physical activity | ||||
| Ethnic | 0.20 (0.10, 0.30) | <0.001 ** | Age | 0.29 (0.17, 0.40) | <0.001 ** |
| Energy | 0.60 (0.42, 0.77) | <0.001 ** | Educ | −0.10 (−0.22, 0.02) | 0.053 |
| Educ | 0.02 (−0.05, 0.10) | 0.261 | |||
| Fat | −0.08 (−0.26, 0.11) | 0.208 | |||
| Body Mass Index | Waist Circumference | |||
|---|---|---|---|---|
| Effect | β (95%CI) | p-Value | β (95%CI) | p-Value |
| Effects of ethnicity on BMI or WC | ||||
| Sum of indirect effects | 0.07 (0.01, 0.14) | 0.014 * | 0.18 (0.12, 0.25) | <0.001 ** |
| Specific indirect effect | ||||
| via energy, dCML, pCML, and pTNF-α | 0.00 (0.00, 0.01) | 0.148 | 0.00 (0.00, 0.01) | 0.025 * |
| via energy, dCML, and pCML | 0.01 (0.00, 0.04) | 0.046 | 0.02 (0.00, 0.07) | 0.001 * |
| via energy, pCML, and pTNF-α | 0.00 (−0.01, 0.00) | 0.149 | 0.00 (−0.01, 0.00) | 0.025 |
| via energy and pCML | −0.01 (−0.05, 0.00) | 0.047 | −0.02 (−0.07, 0.00) | 0.002 * |
| via energy | 0.01 (−0.02, 0.04) | 0.264 | 0.02 (0.00, 0.06) | 0.025 |
| via dCML, pCML, and pTNF-α | 0.00 (0.00, 0.01) | 0.148 | 0.01 (0.00, 0.02) | 0.024 * |
| via dCML and pCML | 0.03 (−0.01, 0,08) | 0.046 | 0.06 (0.02, 0.11) | 0.001 * |
| via pTNF-α | 0.03 (−0.02, 0.08) | 0.131 | 0.09 (0.04, 0.15) | <0.001 ** |
| Effects of education level on BMI or WC | ||||
| Sum of indirect effects | 0.00 (0.02, 0.03) | 0.343 | 0.01 (−0.01, 0.05) | 0.168 |
| Specific indirect effect | ||||
| via fat, energy, dCML, pCML, and pTNF-α | 0.00 (0.00, 0.01) | 0.149 | 0.00 (0.00, 0.02) | 0.025 |
| via fat, energy, dCML, and pCML | 0.02 (0.00, 0.06) | 0.046 | 0.03 (0.01, 0.10) | 0.001 * |
| via fat, energy, pCML, and pTNF-α | 0.00 (−0.01, 0.00) | 0.149 | 0.00 (−0.02, 0.00) | 0.025 |
| via fat, energy, and pCML | −0.02 (−0.07, 0.00) | 0.047 | −0.03 (−0.10, 0.01) | 0.002 * |
| via fat and energy | 0.01 (−0.03, 0.24) | 0.278 | 0.03 (0.00, 0.09) | 0.025 |
| via energy, dCML, pCML, and pTNF-α | 0.00 (0.00, 0.00) | 0.150 | 0.00 (−0.01, 0.00) | 0.027 |
| via energy, dCML, and pCML | −0.01 (−0.04, 0.00) | 0.049 | −0.02 (−0.06, 0.00) | 0.004 * |
| via energy, pCML and pTNF-α | 0.00 (0.00, 0.00) | 0.151 | 0.00 (0.00, 0.01) | 0.028 |
| via energy and pCML | 0.01 (0.00, 0.04) | 0.049 | 0.02 (0.00, 0.06) | 0.004 * |
| via energy | −0.01 (−0.04, 0.02) | 0.265 | −0.02 (−0.05, 0.00) | 0.028 |
| Effects of fat intake on BMI or WC | ||||
| Total effects | ||||
| Sum of indirect effects | 0.06 (−0.13, 0.238) | 0.278 | 0.17 (−0.01, 0.34) | 0.034 |
| Specific indirect effect | ||||
| via energy, dCML, pCML, and pTNF-α | 0.01 (−0.01, 0.03) | 0.148 | 0.02 (0.00, 0.07) | 0.024 * |
| via energy, dCML, and pCML, | 0.08 (−0.01, 0.27) | 0.046 | 0.14 (0.04, 0.41) | 0.001 * |
| via energy, pCML, and pTNF-α | −0.01 (−0.03, 0.01) | 0.148 | −0.02 (−0.07, 0.00) | 0.025 * |
| via energy and pCML | −0.08 (−0.28, 0.01) | 0.046 | −0.15 (−0.42, −0.04) | 0.001 * |
| via energy | 0.06 (−0.124, 0.24) | 0.263 | 0.17 (0.00, 0.34) | 0.025 * |
| Effects of energy intake on BMI or WC | ||||
| Sum of indirect effects | 0.00 (−0.04, 0.03) | 0.395 | −0.01 (−0.07, 0.05) | 0.388 |
| Specific indirect effect | ||||
| via dCML, pCML, and pTNF-α | 0.01 (−0.01, 0.04) | 0.148 | 0.02 (0.00, 0.08) | 0.022 * |
| via dCML and pCML | 0.09 (−0.02, 0.33) | 0.046 | 0.17 (0.05, 0.49) | 0.001 * |
| via pCML and pTNF-α | −0.01 (−0.04, 0.01) | 0.148 | −0.02 (−0.09, 0.00) | 0.025 * |
| via pCML | −0.10 (−0.34, 0.02) | 0.046 | −0.18 (−0.51, −0.05) | 0.001 * |
| Effects of dCML on BMI or WC | ||||
| Sum of indirect effects | 0.17 (−0.01, 0.52) | 0.032 | 0.33 (0.12, 0.83) | <0.001 ** |
| Specific indirect effect | ||||
| via pCML, and pTNF-α | 0.01 (−0.01, 0.06) | 0.148 | 0.04 (0.00, 0.13) | 0.024 * |
| via pCML | 0.16 (−0.03, 0.50) | 0.046 | 0.29 (0.10, 0.75) | 0.001 * |
| Effects of pCML on BMI or WC Sum of indirect effects | ||||
| via pTNF-α | 0.01 (−0.01, 0.03) | 0.148 | 0.03 (0.00, 0.07) | 0.024 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liman, P.B.; Agustina, R.; Djuwita, R.; Umar, J.; Permadhi, I.; Helmizar; Hidayat, A.; Feskens, E.J.M.; Abdullah, M. Dietary and Plasma Carboxymethyl Lysine and Tumor Necrosis Factor-α as Mediators of Body Mass Index and Waist Circumference among Women in Indonesia. Nutrients 2019, 11, 3057. https://doi.org/10.3390/nu11123057
Liman PB, Agustina R, Djuwita R, Umar J, Permadhi I, Helmizar, Hidayat A, Feskens EJM, Abdullah M. Dietary and Plasma Carboxymethyl Lysine and Tumor Necrosis Factor-α as Mediators of Body Mass Index and Waist Circumference among Women in Indonesia. Nutrients. 2019; 11(12):3057. https://doi.org/10.3390/nu11123057
Chicago/Turabian StyleLiman, Patricia Budihartanti, Rina Agustina, Ratna Djuwita, Jahja Umar, Inge Permadhi, Helmizar, Adi Hidayat, Edith J.M. Feskens, and Murdani Abdullah. 2019. "Dietary and Plasma Carboxymethyl Lysine and Tumor Necrosis Factor-α as Mediators of Body Mass Index and Waist Circumference among Women in Indonesia" Nutrients 11, no. 12: 3057. https://doi.org/10.3390/nu11123057
APA StyleLiman, P. B., Agustina, R., Djuwita, R., Umar, J., Permadhi, I., Helmizar, Hidayat, A., Feskens, E. J. M., & Abdullah, M. (2019). Dietary and Plasma Carboxymethyl Lysine and Tumor Necrosis Factor-α as Mediators of Body Mass Index and Waist Circumference among Women in Indonesia. Nutrients, 11(12), 3057. https://doi.org/10.3390/nu11123057