Effect of Macronutrient Composition on Appetite Hormone Responses in Adolescents with Obesity

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
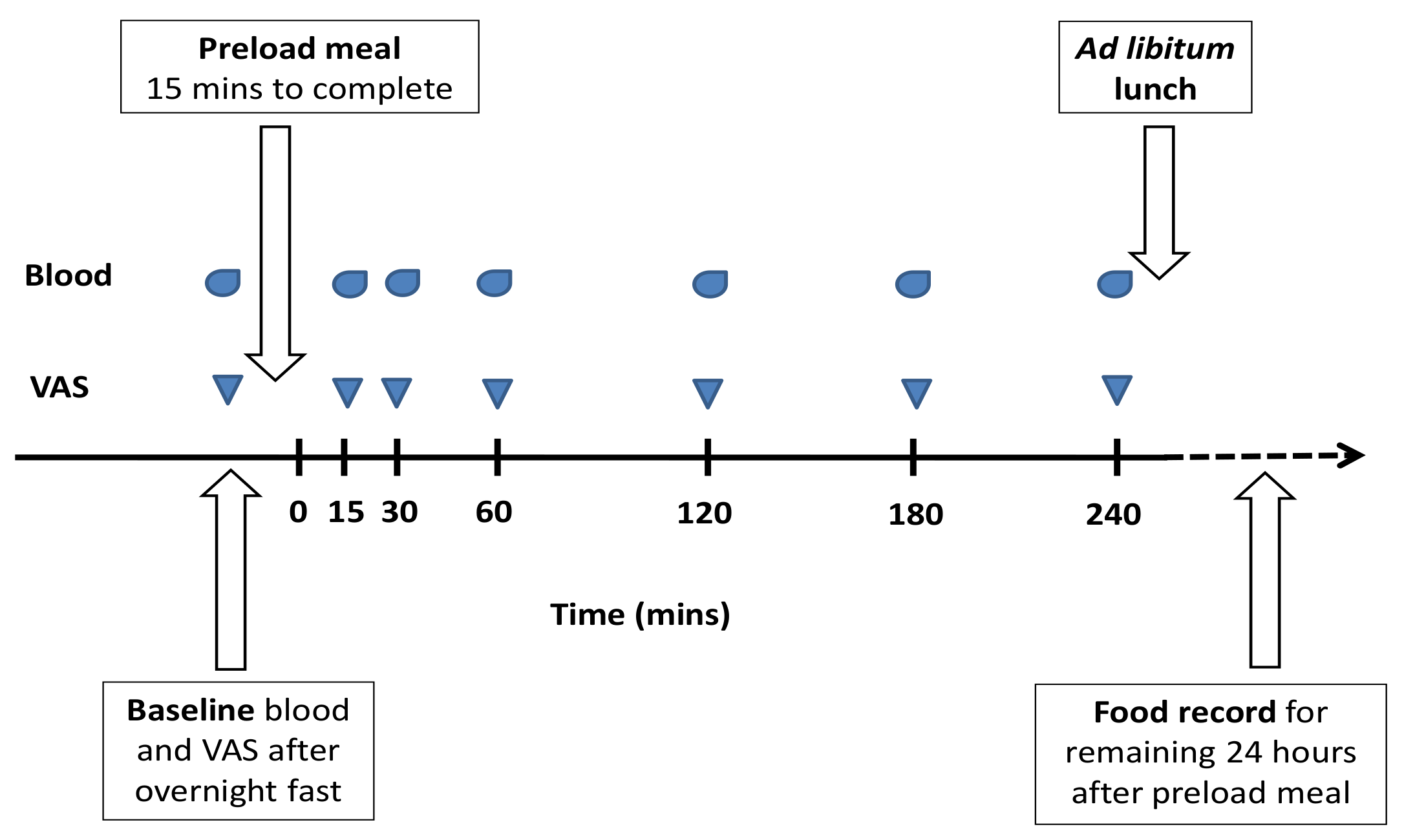
2.1. Study Design and Testing Procedures
2.2. Test Meals
2.3. Participant Recruitment
2.4. Anthropometry and Body Composition
2.5. Blood Sampling and Analysis
2.6. Statistical Analysis
3. Results
3.1. Participants’ Baseline Characteristics
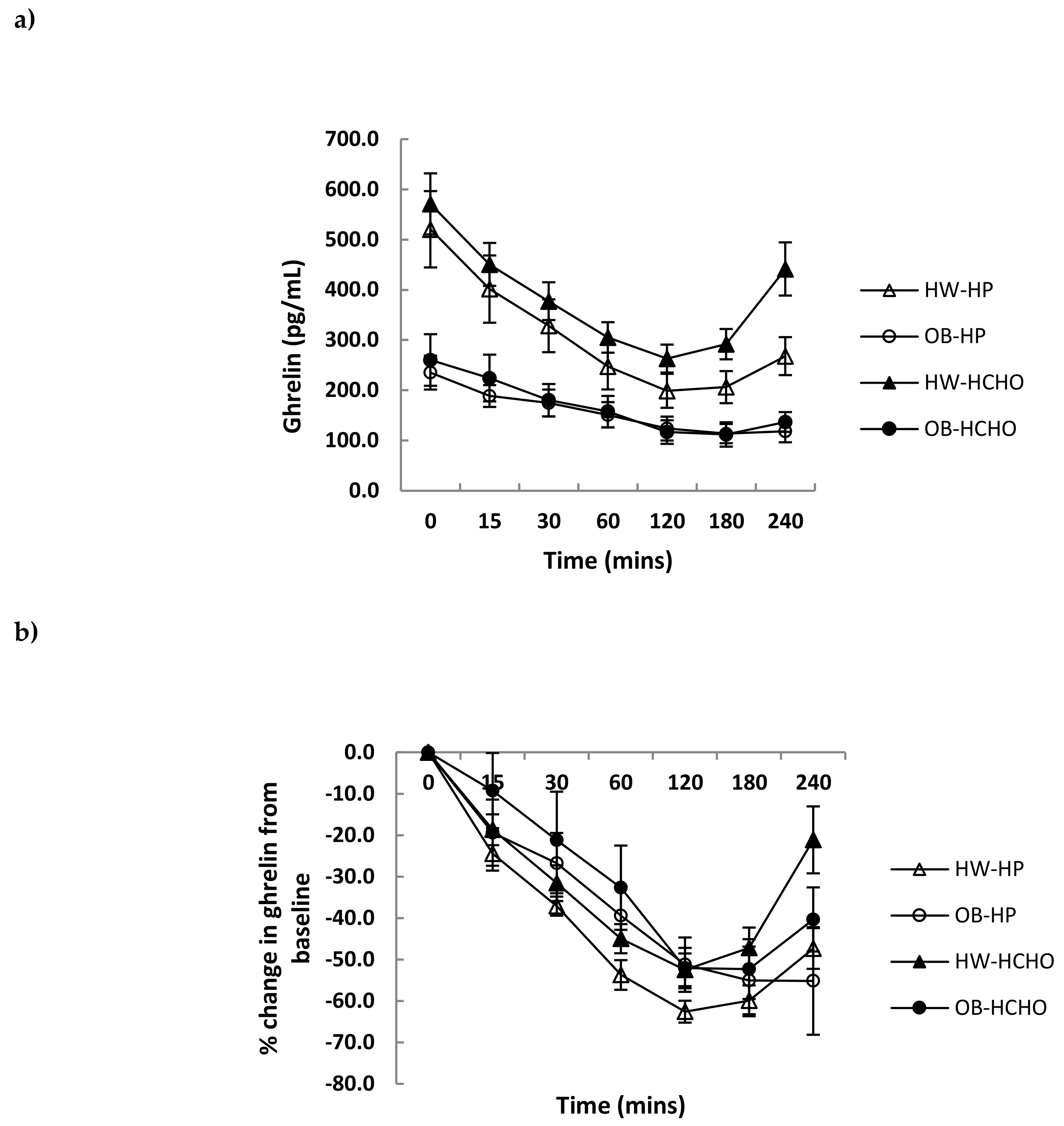
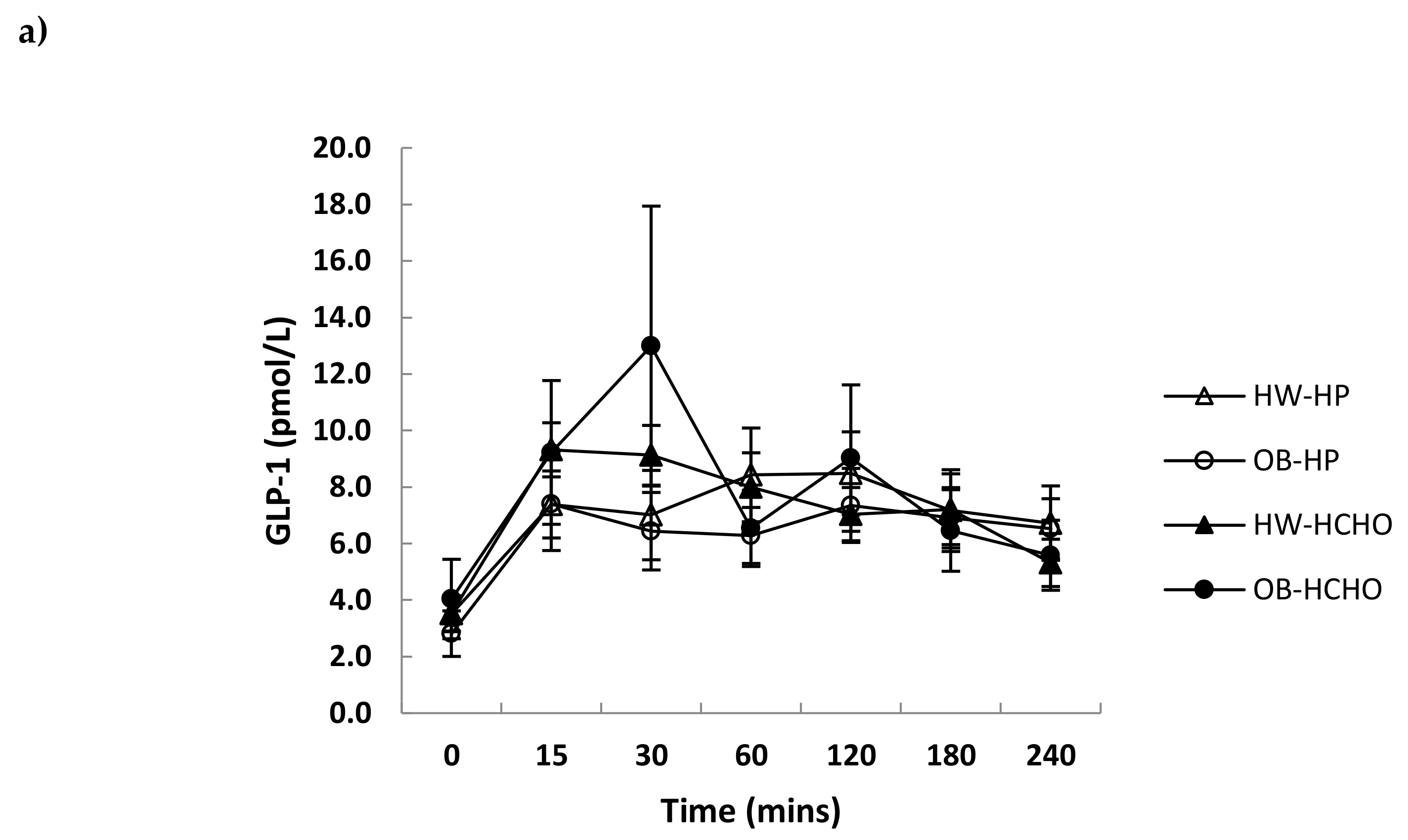
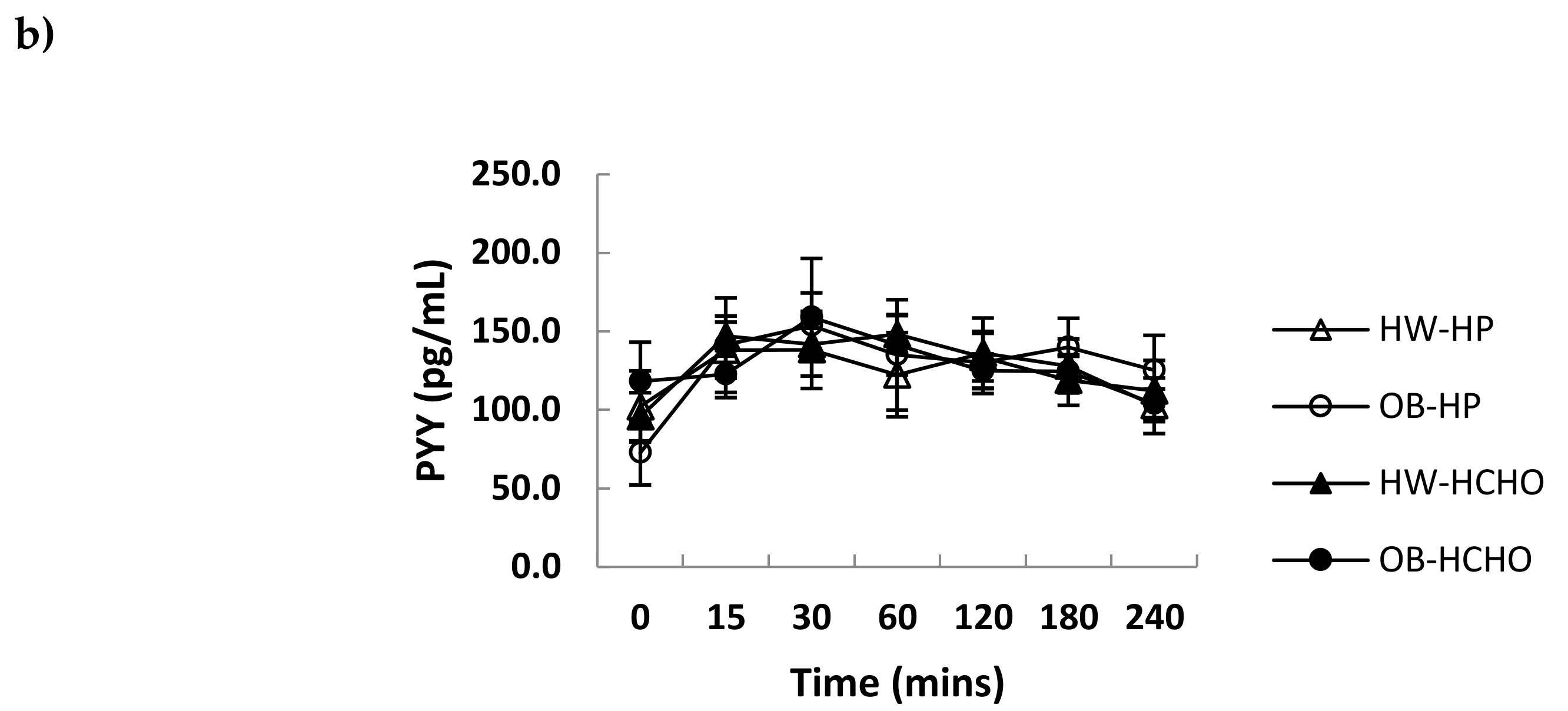
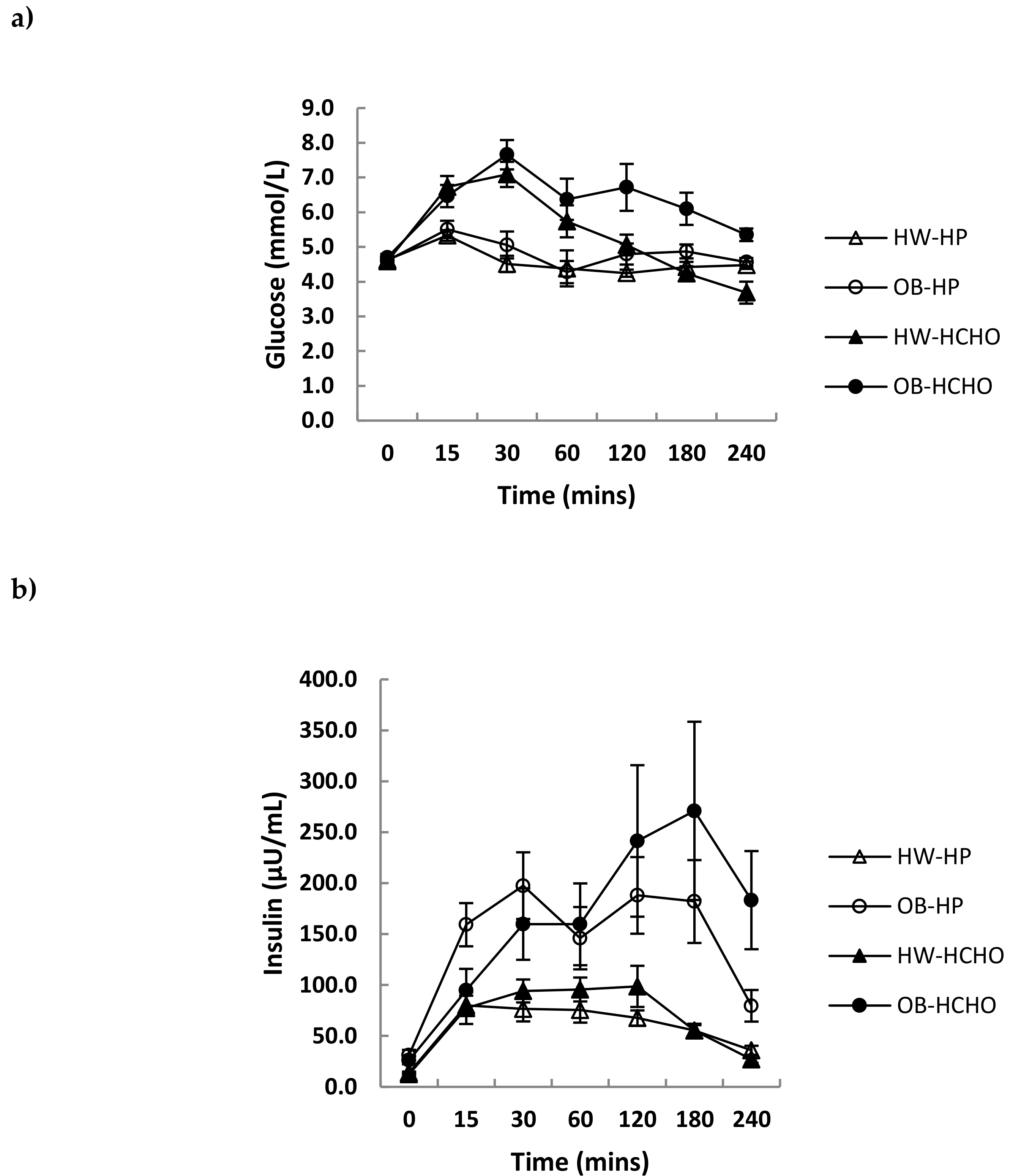
3.2. Postprandial Hormone Responses
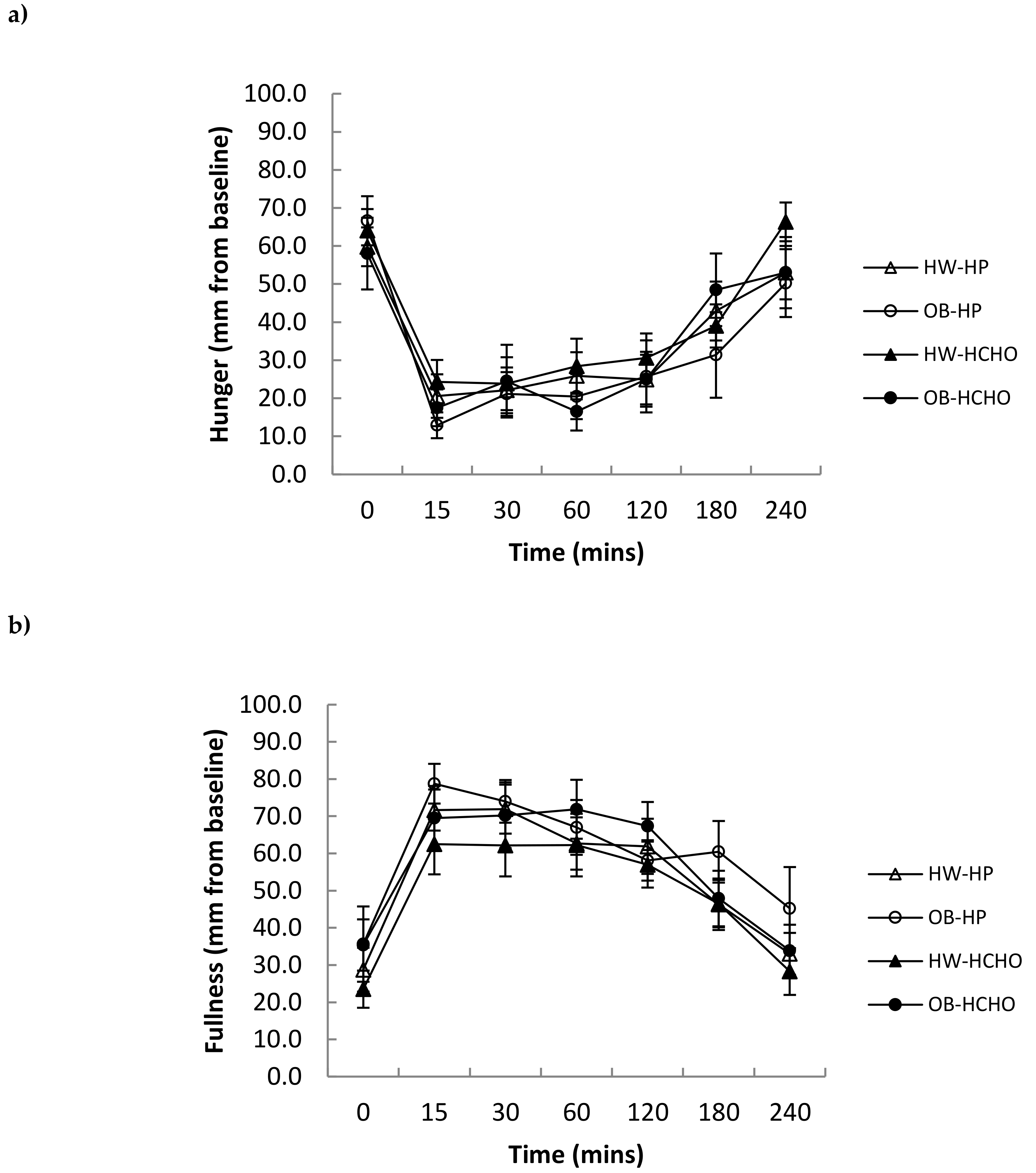
3.3. Self-Reported Appetite and Energy Intake
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J. Am. Coll. Cardiol. 2014, 63, 2985–3023. [Google Scholar] [CrossRef] [PubMed]
- Halton, T.L.; Hu, F.B. The effects of high protein diets on thermogenesis, satiety and weight loss: A critical review. J. Am. Coll. Nutr. 2004, 23, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Leidy, H.J.; Clifton, P.M.; Astrup, A.; Wycherley, T.P.; Westerterp-Plantenga, M.S.; Luscombe-Marsh, N.D.; Woods, S.C.; Mattes, R.D. The role of protein in weight loss and maintenance. Am. J. Clin. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Delzenne, N.; Blundell, J.; Brouns, F.; Cunningham, K.; De Graaf, K.; Erkner, A.; Lluch, A.; Mars, M.; Peters, H.P.; Westerterp-Plantenga, M. Gastrointestinal targets of appetite regulation in humans. Obes. Rev. 2010, 11, 234–250. [Google Scholar] [CrossRef] [PubMed]
- Foster-Schubert, K.E.; Overduin, J.; Prudom, C.E.; Liu, J.; Callahan, H.S.; Gaylinn, B.D.; Thorner, M.O.; Cummings, D.E. Acyl and total ghrelin are suppressed strongly by ingested proteins, weakly by lipids, and biphasically by carbohydrates. J. Clin. Endocrinol. Metab. 2008, 93, 1971–1979. [Google Scholar] [CrossRef]
- Van der Klaauw, A.A.; Keogh, J.M.; Henning, E.; Trowse, V.M.; Dhillo, W.S.; Ghatei, M.A.; Farooqi, I.S. High protein intake stimulates postprandial GLP1 and PYY release. Obesity 2013, 21, 1602–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smeets, A.J.; Soenen, S.; Luscombe-Marsh, N.D.; Ueland, O.; Westerterp-Plantenga, M.S. Energy expenditure, satiety, and plasma ghrelin, glucagon-like peptide 1, and peptide tyrosine-tyrosine concentrations following a single high-protein lunch. J. Nutr. 2008, 138, 698–702. [Google Scholar] [CrossRef]
- Batterham, R.L.; Heffron, H.; Kapoor, S.; Chivers, J.E.; Chandarana, K.; Herzog, H.; Le Roux, C.W.; Thomas, E.L.; Bell, J.D.; Withers, D.J. Critical role for peptide YY in protein-mediated satiation and body-weight regulation. Cell Metab. 2006, 4, 223–233. [Google Scholar] [CrossRef] [Green Version]
- Le Roux, C.W.; Patterson, M.; Vincent, R.P.; Hunt, C.; Ghatei, M.A.; Bloom, S.R. Postprandial plasma ghrelin is suppressed proportional to meal calorie content in normal-weight but not obese subjects. J. Clin. Endocrinol. Metab. 2005, 90, 1068–1071. [Google Scholar] [CrossRef]
- Brennan, I.M.; Luscombe-Marsh, N.D.; Seimon, R.V.; Otto, B.; Horowitz, M.; Wishart, J.M.; Feinle-Bisset, C. Effects of fat, protein, and carbohydrate and protein load on appetite, plasma cholecystokinin, peptide YY, and ghrelin, and energy intake in lean and obese men. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 303, G129–G140. [Google Scholar] [CrossRef]
- Nguo, K.; Walker, K.Z.; Bonham, M.P.; Huggins, C.E. Systematic review and meta-analysis of the effect of meal intake on postprandial appetite-related gastrointestinal hormones in obese children. Int. J. Obes. 2016, 40, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Lomenick, J.P.; Melguizo, M.S.; Mitchell, S.L.; Summar, M.L.; Anderson, J.W. Effects of meals high in carbohydrate, protein, and fat on ghrelin and peptide YY secretion in prepubertal children. J. Clin. Endocrinol. Metab. 2009, 94, 4463–4471. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Tsai, P.M.; Mendes, N.; Miller, K.K.; Klibanski, A. Increased carbohydrate induced ghrelin secretion in obese vs. normal-weight adolescent girls. Obesity 2009, 17, 1689–1695. [Google Scholar] [CrossRef] [PubMed]
- Whatmore, A.J.; Hall, C.M.; Jones, J.; Westwood, M.; Clayton, P.E. Ghrelin concentrations in healthy children and adolescents. Clin. Endocrinol. 2003, 59, 649–654. [Google Scholar] [CrossRef]
- Dietitians’ Pocket Book; Curtin University of Technology: School of Public Health, Department of Nutrition, Dietetics and Food Science: Perth, Australia, 2004.
- Kowalski, K.C.; Crocker, P.R.; Donen, R.M. The physical activity questionnaire for older children (PAQ-C) and adolescents (PAQ-A) manual. Coll. Kinesiol. Univ. Sask. 2004, 87, 1–38. [Google Scholar]
- Marshall, W.A.; Tanner, J.M. Variations in pattern of pubertal changes in girls. Arch. Dis. Child. 1969, 44, 291–303. [Google Scholar] [CrossRef]
- Marshall, W.A.; Tanner, J.M. Variations in the pattern of pubertal changes in boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef]
- Houtkooper, L.B.; Going, S.B.; Lohman, T.G.; Roche, A.F.; Van Loan, M. Bioelectrical impedance estimation of fat-free body mass in children and youth: A cross-validation study. J Appl Physiol. 1992, 72, 366–373. [Google Scholar] [CrossRef]
- Haroun, D.; Croker, H.; Viner, R.M.; Williams, J.E.; Darch, T.S.; Fewtrell, M.S.; Eaton, S.; Wells, J.C. Validation of BIA in obese children and adolescents and re-evaluation in a longitudinal study. Obesity 2009, 17, 2245–2250. [Google Scholar] [CrossRef]
- Lomenick, J.P.; Clasey, J.L.; Anderson, J.W. Meal-related changes in ghrelin, peptide YY, and appetite in normal weight and overweight children. Obesity 2008, 16, 547–552. [Google Scholar] [CrossRef]
- Mittelman, S.D.; Klier, K.; Braun, S.; Azen, C.; Geffner, M.E.; Buchanan, T.A. Obese adolescents show impaired meal responses of the appetite-regulating hormones ghrelin and PYY. Obesity 2010, 18, 918–925. [Google Scholar] [CrossRef] [PubMed]
- English, P.J.; Ghatei, M.A.; Malik, I.A.; Bloom, S.R.; Wilding, J.P. Food fails to suppress ghrelin levels in obese humans. J. Clin. Endocrinol. Metab. 2002, 87, 2984. [Google Scholar] [CrossRef] [PubMed]
- Roth, C.L.; Reinehr, T. Roles of gastrointestinal and adipose tissue peptides in childhood obesity and changes after weight loss due to lifestyle intervention. Arch. Pediatr. Adolesc. Med. 2010, 164, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.; Leichner, P.; Wong, A.C.; Ghatei, M.A.; Kieffer, T.J.; Bloom, S.R.; Chanoine, J.P. Ghrelin, peptide YY, glucose-dependent insulinotropic polypeptide, and hunger responses to a mixed meal in anorexic, obese, and control female adolescents. J. Clin. Endocrinol. Metab. 2005, 90, 2161–2168. [Google Scholar] [CrossRef] [PubMed]
- Lomenick, J.P.; White, J.R.; Smart, E.J.; Clasey, J.L.; Anderson, J.W. Glucagon-like peptide 1 and pancreatic polypeptide responses to feeding in normal weight and overweight children. J. Pediatr. Endocrinol. Metab. 2009, 22, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Tomasik, P.; Sztefko, K.; Starzyk, J. Entero-insular axis in children with simple obesity. Pediatr. Endocrinol. Diabetes Metab. 2009, 15, 63–69. [Google Scholar]
- Beglinger, S.; Meyer-Gerspach, A.C.; Graf, S.; Zumsteg, U.; Drewe, J.; Beglinger, C.; Gutzwiller, J.P. Effect of a test meal on meal responses of satiation hormones and their association to insulin resistance in obese adolescents. Obesity 2014, 22, 2047–2052. [Google Scholar] [CrossRef] [Green Version]
- Bowen, J.; Noakes, M.; Trenerry, C.; Clifton, P.M. Energy intake, ghrelin, and cholecystokinin after different carbohydrate and protein preloads in overweight men. J. Clin. Endocrinol. Metab. 2006, 91, 1477–1483. [Google Scholar] [CrossRef]
- Belza, A.; Ritz, C.; Sorensen, M.Q.; Holst, J.J.; Rehfeld, J.F.; Astrup, A. Contribution of gastroenteropancreatic appetite hormones to protein-induced satiety. Am. J. Clin. Nutr. 2013, 97, 980–989. [Google Scholar] [CrossRef] [Green Version]
- Hall, W.L.; Millward, D.J.; Long, S.J.; Morgan, L.M. Casein and whey exert different effects on plasma amino acid profiles, gastrointestinal hormone secretion and appetite. Br. J. Nutr. 2003, 89, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Leidy, H.J.; Racki, E.M. The addition of a protein-rich breakfast and its effects on acute appetite control and food intake in breakfast-skipping adolescents. Int. J. Obes. 2010, 34, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Leidy, H.J.; Bales-Voelker, L.I.; Harris, C.T. A protein-rich beverage consumed as a breakfast meal leads to weaker appetitive and dietary responses v. a protein-rich solid breakfast meal in adolescents. Br. J. Nutr. 2011, 106, 37–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stull, A.J.; Apolzan, J.W.; Thalacker-Mercer, A.E.; Iglay, H.B.; Campbell, W.W. Liquid and solid meal replacement products differentially affect postprandial appetite and food intake in older adults. J. Am. Diet. Assoc. 2008, 108, 1226–1230. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, C.; Caudwell, P.; Finlayson, G.; Webb, D.L.; Hellstrom, P.M.; Naslund, E.; Blundell, J.E. Comparison of postprandial profiles of ghrelin, active GLP-1, and total PYY to meals varying in fat and carbohydrate and their association with hunger and the phases of satiety. J. Clin. Endocrinol. Metab. 2013, 98, E847–E855. [Google Scholar] [CrossRef] [PubMed]
- Chanoine, J.P.; Mackelvie, K.J.; Barr, S.I.; Wong, A.C.; Meneilly, G.S.; Elahi, D.H. GLP-1 and appetite responses to a meal in lean and overweight adolescents following exercise. Obesity 2008, 16, 202–204. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OB (n = 8) | HW (n = 12) | p-value | |
|---|---|---|---|
| Age years (range) | 16.1 ±0.4 (11.0–17.5) | 16.0 ±0.6 (11.0–19.0) | 0.921 |
| Male/female, n | 4/4 | 4/8 | 0.648 b |
| Tanner stage a | 4.0 ± 2.0 | 4.0 ± 4.0 | 0.642 b |
| Weight (kg) | 98.3 ± 7.9 | 55.7 ± 2.7 | 0.001 |
| Weight z-score | 2.1 ± 0.2 | 0.1 ± 0.2 | <0.001 |
| Height (cm) | 169.0 ± 2.2 | 164.6 ± 2.3 | 0.213 |
| BMI (kg/m2) | 34.4 ± 2.6 | 20.5 ± 0.8 | 0.001 |
| BMI z-score | 2.1 ± 0.1 | 0 ± 0.2 | <0.001 |
| Waist (cm) | 106.7 ± 5.9 | 73.2 ± 1.5 | 0.001 |
| Fat mass (kg) | 37.3 ± 7.7 | 13.9 ± 1.8 | 0.001 |
| % body fat | 36.3 ± 4.8 | 24.3 ± 2.3 | 0.023 |
| Insulin (µU/mL) c | 34.0 ± 24.0 | 13.7± 5.2 | 0.008 |
| Glucose (mmol/L) | 4.7 ± 0.1 | 4.6 ± 0.1 | 0.663 |
| HOMA | 5.9 ± 0.9 | 2.7 ± 0.2 | 0.012 |
| Ghrelin (pg/mL) | 248.0 ± 41.6 | 546.1 ± 65.0 | 0.001 |
| GLP-1 (pmol/L) | 3.4 ± 1.1 | 3.5 ± 0.6 | 0.934 |
| Leptin (pg/mL) | 26.7 ± 5.2 | 6.2 ± 1.3 | 0.001 |
| PYY (pg/mL) d | 98.9 ± 13.9 | 95.4 ± 20.5 | 0.891 |
| High Protein | High Carbohydrate | p-Value Wt | p-Value Meal | p-Value Wt × Meal | |||
|---|---|---|---|---|---|---|---|
| OB (n = 8) | HW (n = 12) | OB (n = 8) | HW(n = 12) | ||||
| Ghrelin (pg/mL/4h) | −23361 ± 3919 | −64135 ± 9539 | −28432 ± 6909 | −57592 ± 8984 | 0.008 | 0.851 | 0.149 |
| Glucose b (mmol/L/4h) | 52 ± 141 | 15 ± 24 | 342 ± 421 | 212 ± 233 | 0.020 | <0.001 | 0.019 |
| Insulin (µU/mL/4h) | 30726 ± 6230 | 11556 ± 1417 | 42384 ± 12274 | 14732 ± 1816 | 0.005 | 0.046 a | 0.236 |
| GLP-1 b (pmol/L/4h) | 911 ± 458 | 750 ± 380 | 638 ± 1233 | 819 ± 544 | 0.943 | 0.719 | 0.837 |
| PYY c (pg/mL/4h) | 14861 ± 6415 | 6719 ± 2127 | 6735 ± 2409 | 8354 ± 1920 | 0.488 | 0.354 | 0.177 |
| High Protein | High Carbohydrate | p-Value Wt | p-Value Meal | p-Value Wt × Meal | |||
|---|---|---|---|---|---|---|---|
| OB (n = 8) | HW (n = 12) | OB (n = 8) | HW(n = 12) | ||||
| Lunch (kJ) | 3982 ± 402 | 3205 ± 299 | 3918 ± 427 | 3362 ± 265 | 0.128 | 0.851 | 0.653 |
| 24 h food record (kJ) | 7288 ± 2062 | 6110 ± 538 | 7403 ± 1004 | 6271 ± 656 | 0.262 | 0.903 | 0.984 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguo, K.; Bonham, M.P.; Truby, H.; Barber, E.; Brown, J.; Huggins, C.E. Effect of Macronutrient Composition on Appetite Hormone Responses in Adolescents with Obesity. Nutrients 2019, 11, 340. https://doi.org/10.3390/nu11020340
Nguo K, Bonham MP, Truby H, Barber E, Brown J, Huggins CE. Effect of Macronutrient Composition on Appetite Hormone Responses in Adolescents with Obesity. Nutrients. 2019; 11(2):340. https://doi.org/10.3390/nu11020340
Chicago/Turabian StyleNguo, Kay, Maxine P Bonham, Helen Truby, Elizabeth Barber, Justin Brown, and Catherine E Huggins. 2019. "Effect of Macronutrient Composition on Appetite Hormone Responses in Adolescents with Obesity" Nutrients 11, no. 2: 340. https://doi.org/10.3390/nu11020340
APA StyleNguo, K., Bonham, M. P., Truby, H., Barber, E., Brown, J., & Huggins, C. E. (2019). Effect of Macronutrient Composition on Appetite Hormone Responses in Adolescents with Obesity. Nutrients, 11(2), 340. https://doi.org/10.3390/nu11020340