Effect of Alpha-Lipoic Acid Supplementation on Endothelial Function and Cardiovascular Risk Factors in Overweight/Obese Youths: A Double-Blind, Placebo-Controlled Randomized Trial

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Study Design
2.3. Ultrasound Measures of the Diameter and Flow-Mediated Dilation of the Brachial Artery
2.4. Clinical and Laboratory Data
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Effects of ALA on FMD (Main Outcome) and Clinical and Metabolic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, F.B.; Lavie, C.; Blair, S.N. Obesity and cardiovascular disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C. Prevalence of obesity and severe obesity in US children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed]
- Cote, A.T.; Harris, K.C.; Panagiotopoulos, C.; Sandor, G.G.; Devlin, A.M. Childhood obesity and cardiovascular dysfunction. J. Am. Coll. Cardiol. 2013, 62, 1309–1319. [Google Scholar] [CrossRef] [PubMed]
- McCrindle, B.W. Cardiovascular consequences of childhood obesity. Can. J. Cardiol. 2015, 31, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.M.; Shimokawa, H.; Feletou, M.; Tang, E.H. Endothelial dysfunction and vascular disease—A 30th anniversary update. Acta Physiol. 2017, 219, 22–96. [Google Scholar] [CrossRef] [PubMed]
- Favero, G.; Paganelli, C.; Buffoli, B.; Rodella, L.F.; Rezzani, R. Endothelium and its alterations in cardiovascular diseases: Life style intervention. Biomed Res. Int. 2014, 2014, 801896. [Google Scholar] [CrossRef]
- Montero, D.; Walther, G.; Perez-Martin, A.; Roche, E.; Vinet, A. Endothelial dysfunction, inflammation, and oxidative stress in obese children and adolescents: Markers and effect of lifestyle intervention. Obes. Rev. 2012, 13, 441–455. [Google Scholar] [CrossRef]
- Tibullo, D.; Li Volti, G.; Giallongo, C.; Grasso, S.; Tomassoni, D.; Anfuso, C.D.; Lupo, G.; Amenta, F.; Avola, R.; Bramanti, V. Biochemical and clinical relevance of alpha lipoic acid: Antioxidant and anti-inflammatory activity, molecular pathways and therapeutic potential. Inflamm. Res. 2017, 66, 947–959. [Google Scholar] [CrossRef]
- Pashaj, A.; Xia, M.; Moreau, R. α-Lipoic acid as a triglyceride-lowering nutraceutical. Can. J. Physiol. Pharmacol. 2015, 93, 1029–1041. [Google Scholar] [CrossRef]
- Shay, K.P.; Moreau, R.F.; Smith, E.J.; Smith, A.R.; Hagen, T.M. Alpha-lipoic acid as a dietary supplement: Molecular mechanisms and therapeutic potential. Biochim. Biophys. Acta 2009, 1790, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kataoka, H.; Hirabayashi, N.; Makita, M. Analysis of lipoic acid by gas chromatography with flame photometric detection. Methods Enzymol. 1997, 279, 166–176. [Google Scholar] [PubMed]
- Lodge, J.K.; Youn, H.D.; Handelman, G.; Konishi, T.; Matsugo, S.; Mathur, V.V.; Packer, L. Natural sources of lipoic acid: Determination of lipoyllysine released from protease-digested tissues by high performance liquid chromatography incorporating electrochemical detection. J. Appl. Nutr. 1997, 49, 3–11. [Google Scholar]
- Hermann, R.; Niebch, G.; Borbe, H.O.; Fieger-Büschges, H.; Ruus, P.; Nowak, H.; Riethmüller-Winzen, H.; Peukert, M.; Blume, H. Enantioselective pharmacokinetics and bioavailability of different racemic α-lipoic acid formulations in healthy volunteers. Eur. J. Pharm. Sci. 1996, 4, 167–174. [Google Scholar] [CrossRef]
- Estrada, D.E.; Ewart, H.S.; Tsakiridis, T.; Volchuk, A.; Ramlal, T.; Tritschler, H.; Klip, A. Stimulation of glucose uptake by the natural coenzyme alpha-lipoic acid/thioctic acid: Participation of elements of the insulin signaling pathway. Diabetes 1996, 45, 1798–1804. [Google Scholar] [CrossRef] [PubMed]
- Baydas, G.; Yilmaz, O.; Celik, S.; Yasar, A.; Gursu, M.F. Effects of certain micronutrients and melatonin on plasma lipid, lipid peroxidation, and homocysteine levels in rats. Arch. Med. Res. 2002, 33, 515–519. [Google Scholar] [CrossRef]
- Vasdev, S.; Ford, C.A.; Parai, S.; Longerich, L.; Gadag, V. Dietary alpha-lipoic acid supplementation lowers blood pressure in spontaneously hypertensive rats. J. Hypertens. 2000, 18, 567–573. [Google Scholar] [CrossRef]
- Vasdev, S.; Ford, C.A.; Parai, S.; Longerich, L.; Gadag, V. Dietary lipoic acid supplementation prevents fructose-induced hypertension in rats. Nutr. Metab. Cardiovasc. Dis. 2000, 10, 339–346. [Google Scholar]
- Sola, S.; Mir, M.Q.; Cheema, F.A.; Khan-Merchant, N.; Menon, R.G.; Parthasarathy, S.; Khan, B.V. Irbesartan and lipoic acid improve endothelial function and reduce markers of inflammation in the metabolic syndrome: Results of the Irbesartan and Lipoic Acid in Endothelial Dysfunction (ISLAND) study. Circulation 2005, 111, 343–348. [Google Scholar] [CrossRef]
- Heinisch, B.B.; Francesconi, M.; Mittermayer, F.; Schaller, G.; Gouya, G.; Wolzt, M.; Pleiner, J. Alpha-lipoic acid improves vascular endothelial function in patients with type 2 diabetes: A placebo-controlled randomized trial. Eur. J. Clin. Investig. 2010, 40, 148–154. [Google Scholar] [CrossRef]
- Scaramuzza, A.; Giani, E.; Redaelli, F.; Ungheri, S.; Macedoni, M.; Giudici, V.; Bosetti, A.; Ferrari, M.; Zuccotti, G.V. Alpha-lipoic acid and antioxidant diet help to improve endothelial dysfunction in adolescents with type 1 diabetes: A pilot trial. J. Diabetes. Res. 2015, 2015, 474561. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Pacifico, L.; Anania, C.; Martino, F.; Cantisani, V.; Pascone, R.; Marcantonio, A.; Chiesa, C. Functional and morphological vascular changes in pediatric nonalcoholic fatty liver disease. Hepatology 2010, 52, 1643–1651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacifico, L.; Arca, M.; Anania, C.; Cantisani, V.; Di Martino, M.; Chiesa, C. Arterial function and structure after a 1-year lifestyle intervention in children with nonalcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 1010–1016. [Google Scholar] [CrossRef] [PubMed]
- McMackin, C.J.; Widlansky, M.E.; Hamburg, N.M.; Huang, A.L.; Weller, S.; Holbrook, M.; Gokce, N.; Hagen, T.M.; Keaney, J.F., Jr.; Vita, J.A. Effect of combined treatment with alpha-Lipoic acid and acetyl-L-carnitine on vascular function and blood pressure in patients with coronary artery disease. J. Clin. Hypertens. 2007, 9, 249–255. [Google Scholar] [CrossRef]
- West, S.G.; McIntyre, M.D.; Piotrowski, M.J.; Poupin, N.; Miller, D.L.; Preston, A.G.; Wagner, P.; Groves, L.F.; Skulas-Ray, A.C. Effects of dark chocolate and cocoa consumption on endothelial function and arterial stiffness in overweight adults. Br. J. Nutr. 2014, 111, 653–661. [Google Scholar] [CrossRef]
- Ziegler, D.; Nowak, H.; Kempler, P.; Vargha, P.; Low, P.A. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: A meta-analysis. Diabet. Med. 2004, 21, 114–121. [Google Scholar] [CrossRef]
- Park, S.; Karunakaran, U.; Jeoung, N.H.; Jeon, J.H.; Lee, I.K. Physiological effect and therapeutic application of alpha lipoic acid. Curr. Med. Chem. 2014, 21, 3636–3645. [Google Scholar] [CrossRef]
- Heitzer, T.; Finckh, B.; Albers, S.; Krohn, K.; Kohlschütter, A.; Meinertz, T. Beneficial effects of alpha-lipoic acid and ascorbic acid on endothelium-dependent, nitric oxide-mediated vasodilation in diabetic patients: Relation to parameters of oxidative stress. Free Radic. Biol. Med. 2001, 31, 53–61. [Google Scholar] [CrossRef]
- Xiang, G.D.; Sun, H.L.; Zhao, L.S.; Hou, J.; Yue, L.; Xu, L. The antioxidant alpha-lipoic acid improves endothelial dysfunction induced by acute hyperglycaemia during OGTT in impaired glucose tolerance. Clin. Endocrinol. 2008, 68, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Xiang, G.; Pu, J.; Yue, L.; Hou, J.; Sun, H. α-lipoic acid can improve endothelial dysfunction in subjects with impaired fasting glucose. Metabolism. 2011, 60, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Namazi, N.; Larijani, B.; Azadbakht, L. Alpha-lipoic acid supplement in obesity treatment: A systematic review and meta-analysis of clinical trials. Clin. Nutr. 2018, 37, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Ostadmohammadi, V.; Lankarani, K.B.; Tabrizi, R.; Kolahhdooz, F.; Khatibi, S.R.; Asemi, Z. The effects of alpha-lipoic acid supplementation on glucose contro and lipid profiles among patients with metabolic diseases: A systematic review and meta-analysis of randomized controlled trials. Metabolism 2018, 87, 56–69. [Google Scholar] [CrossRef] [PubMed]
- Saboori, S.; Falahi, E.; Eslampour, E.; Zeinali Khosroshahi, M.; Yousefi Rad, E. Effects of alpha-lipoic acid supplementation on C-reactive protein level: A systematic review and meta-analysis of randomized controlled clinical trials. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 779–786. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Controls (n = 22) | Obese | p * | |
|---|---|---|---|---|
| Placebo (n = 32) | ALA (n = 32) | |||
| Age, years | 11.2 ± 2.8 | 11.1 ± 2.1 | 11.5 ± 1.9 | 0.64 |
| Male gender, n (%) | 13 (59.1) | 20 (62.5) | 16 (50.0) | 0.58 |
| Prepubertal status, n (%) | 4 (18.2) | 2 (6.25) | 2 (6.25) | 0.25 |
| Weight, kg | 38.8 ± 14.8 | 60.8 ± 15.2 | 64.2 ± 14.1 | <0.0001 |
| BMI | 17.7 ± 2.3 | 26.0 ± 2.8 | 27.4 ± 3.5 | <0.0001 |
| BMI-SDS | −0.01 ± 0.68 | 1.94 ± 0.33 | 1.94 ± 0.46 | <0.0001 |
| Waist circumference, cm | 65.2 ± 11.2 | 86.0 ± 10.7 | 85.0 ± 14.6 | <0.0001 |
| Waist-to-height ratio | 0.45 ± 0.08 | 0.57 ± 0.09 | 0.56 ± 0.06 | <0.0001 |
| Systolic BP, mmHg | 98.2 ± 12.2 | 116.8 ± 7.1 | 117.0 ± 9.0 | <0.0001 |
| Diastolic BP, mmHg | 70.0 ± 7.1 | 70.5 ± 7.1 | 69.4 ± 7.9 | <0.0001 |
| ALT, U/L | 13.5 (12.0–16.5) | 16.0 (14.0–38.0) | 18.0 (14.0–23.0) | 0.01 |
| TC, mg/dL | 151 (132–162) | 162 (133–182) | 172 (147–192) | 0.012 |
| HDL-C, mg/dL | 58 (50–64) | 48 (40–53) | 49 (46–60) | 0.005 |
| LDL-C, mg/dL | 75 (63–89) | 90 (68–114) | 95 (79–123) | 0.005 |
| TG, mg/dL | 50 (46–70) | 93 (77–118) | 95 (72–129) | <0.0001 |
| Glucose, mg/dL | 85.0 ± 7.0 | 82.4 ± 7.7 | 83.8 ± 6.0 | 0.35 |
| Insulin, μU/mL | 7.2 (5.1–9.7) | 15.3 (11.0–22.3) | 16.2 (11.9–24.9) | <0.0001 |
| HOMA-IR | 1.34 (1.0–1.9) | 3.01 (2.26–5.19) | 3.37 (2.27–5.0) | <0.0001 |
| 2-hour glucose, mg/dL | ND | 94.5 ± 15.7 | 94.7 ± 10.9 | 0.61 |
| 2-hour insulin, µU/mL | ND | 41.7 (27.6–92.7) | 45.2 (30.8–76.4) | 0.40 |
| HSCRP, μg/L | 350 (300–725) | 1400 (925–2675) | 1250 (925–1675) | <0.0001 |
| Variables | Controls | Obese | p * | |
|---|---|---|---|---|
| Placebo | ALA | |||
| Basal brachial artery diameter, mm | 3.35 (3.1–3.7) | 2.9 (2.55–3.2) | 2.8 (2.65–3.15) | 0.0001 |
| Peak brachial artery diameter, mm | 4.0 (3.8–4.7) | 3.3 (3.1–3.6) | 3.4 (3.1–3.65) | 0.0001 |
| FMD, % | 24.0% (17.8–28.0) | 12.5 (4.0–20.0) | 12.5 (6.8–23.0) | 0.045 |
| Variables | Placebo | ALA | |||||
|---|---|---|---|---|---|---|---|
| Baseline | End of Study | p * | Baseline | End of Study | p * | p † | |
| Weight, kg | 60.8 ± 15.2 | 61.2 ± 13.6 | 0.32 | 64.2 ± 14.1 | 64.1 ± 14.6 | 0.35 | 0.94 |
| BMI-SDS | 1.94 ± 0.33 | 1.89 ± 0.35 | 0.16 | 1.94 ± 0.46 | 1.89 ± 0.45 | 0.46 | 0.97 |
| WC, cm | 86.0 ± 10.7 | 86.2 ± 9.3 | 0.65 | 85.0 ± 14.6 | 86.7 ± 9.9 | 0.38 | 0.24 |
| Waist-to-height ratio | 0.57 ± 0.09 | 0.56 ± 0.05 | 0.99 | 0.56 ± 0.09 | 0.56 ± 0.06 | 0.69 | 0.25 |
| Systolic BP, (mm Hg) | 116.8 ± 7.1 | 114.5 ± 8.5 | 0.31 | 117.0 ± 9.0 | 117.7 ± 10.4 | 0.78 | 0.74 |
| Diastolic BP, (mm Hg) | 70.5 ± 7.1 | 69.0 ± 7.7 | 0.39 | 69.4 ± 7.9 | 69.1 ± 12.6 | 0.95 | 0.25 |
| ALT, U/L | 16 (14–38) | 16 (12–23) | 0.30 | 19 (14–23) | 19 (14–24) | 0.68 | 0.25 |
| TC, mg/dL | 162 (133–182) | 165 (133–179) | 0.44 | 172 (147–192) | 169 (136–188) | 0.09 | 0.64 |
| HDL-C, mg/dL | 48 (40–53) | 46 (38–52) | 0.15 | 49 (46–60) | 51 (44–56) | 0.13 | 0.12 |
| LDL-C, mg/dL | 90 (68–114) | 91 (72–112) | 0.17 | 95 (79–123) | 93 (74–114) | 0.057 | 0.62 |
| TG, mg/dL | 93 (77–118) | 90 (68–115) | 0.13 | 95 (72–129) | 90 (76–113) | 0.15 | 0.11 |
| Glucose, mg/dL | 82.4 ± 7.7 | 80.9 ± 17.7 | 0.51 | 83.8 ± 6.0 | 83.1 ± 16.8 | 0.89 | 0.15 |
| Insulin, μU/mL | 15.3 (11.0–22.3) | 16.3 (10.9–20.0) | 0.35 | 16.2 (11.9–24.9) | 17.0 (12.1–23.9) | 0.68 | 0.90 |
| HOMA-IR | 3.01 (2.26–5.19) | 3.18 (2.19–5.19) | 0.44 | 3.37 (2.27–5.0) | 3.41 (2.0–4.94) | 0.87 | 0.50 |
| HSCRP, μg/L | 1400 (925–2675) | 1100 (500–3200) | 0.99 | 1250 (925–1675) | 1100 (800–2250) | 0.18 | 0.56 |
| Variables | Placebo | ALA | |||||
|---|---|---|---|---|---|---|---|
| Baseline | End of Study | p * | Baseline | End of Study | p * | p † | |
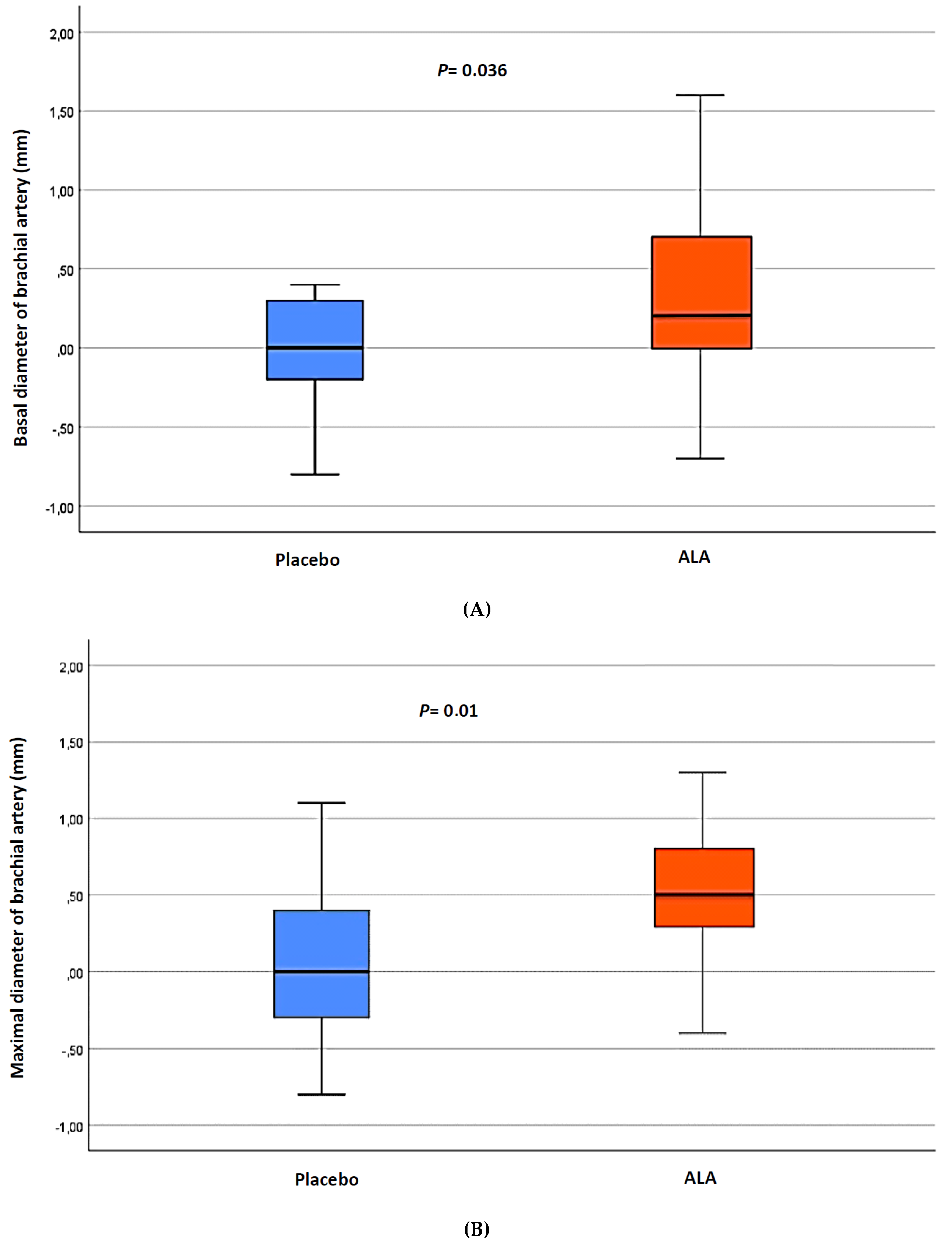
| Basal brachial artery diameter, mm | 2.9 (2.5–3.2) | 2.9 (2.8–3.2) | 0.062 | 2.8 (2.6–3.1) | 3.3 (3.1–3.6) | 0.011 | 0.036 |
| Peak brachial artery diameter, mm | 3.3 (3.1–3.6) | 3.4 (3.1–3.6) | 0.29 | 3.4 (3.1–3.6) | 3.9 (3.7–4.2) | 0.001 | 0.01 |
| FMD, % | 12.5 (4.0–20.0) | 12.5 (5.5–18.2) | 0.24 | 12.5 (6.8–23.0) | 16.7 (10.9–23.9) | 0.28 | 0.13 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tromba, L.; Perla, F.M.; Carbotta, G.; Chiesa, C.; Pacifico, L. Effect of Alpha-Lipoic Acid Supplementation on Endothelial Function and Cardiovascular Risk Factors in Overweight/Obese Youths: A Double-Blind, Placebo-Controlled Randomized Trial. Nutrients 2019, 11, 375. https://doi.org/10.3390/nu11020375
Tromba L, Perla FM, Carbotta G, Chiesa C, Pacifico L. Effect of Alpha-Lipoic Acid Supplementation on Endothelial Function and Cardiovascular Risk Factors in Overweight/Obese Youths: A Double-Blind, Placebo-Controlled Randomized Trial. Nutrients. 2019; 11(2):375. https://doi.org/10.3390/nu11020375
Chicago/Turabian StyleTromba, Luciana, Francesco Massimo Perla, Giovanni Carbotta, Claudio Chiesa, and Lucia Pacifico. 2019. "Effect of Alpha-Lipoic Acid Supplementation on Endothelial Function and Cardiovascular Risk Factors in Overweight/Obese Youths: A Double-Blind, Placebo-Controlled Randomized Trial" Nutrients 11, no. 2: 375. https://doi.org/10.3390/nu11020375
APA StyleTromba, L., Perla, F. M., Carbotta, G., Chiesa, C., & Pacifico, L. (2019). Effect of Alpha-Lipoic Acid Supplementation on Endothelial Function and Cardiovascular Risk Factors in Overweight/Obese Youths: A Double-Blind, Placebo-Controlled Randomized Trial. Nutrients, 11(2), 375. https://doi.org/10.3390/nu11020375