A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future?

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Outcome Measures
2.3. Inclusion and Exclusion Criteria
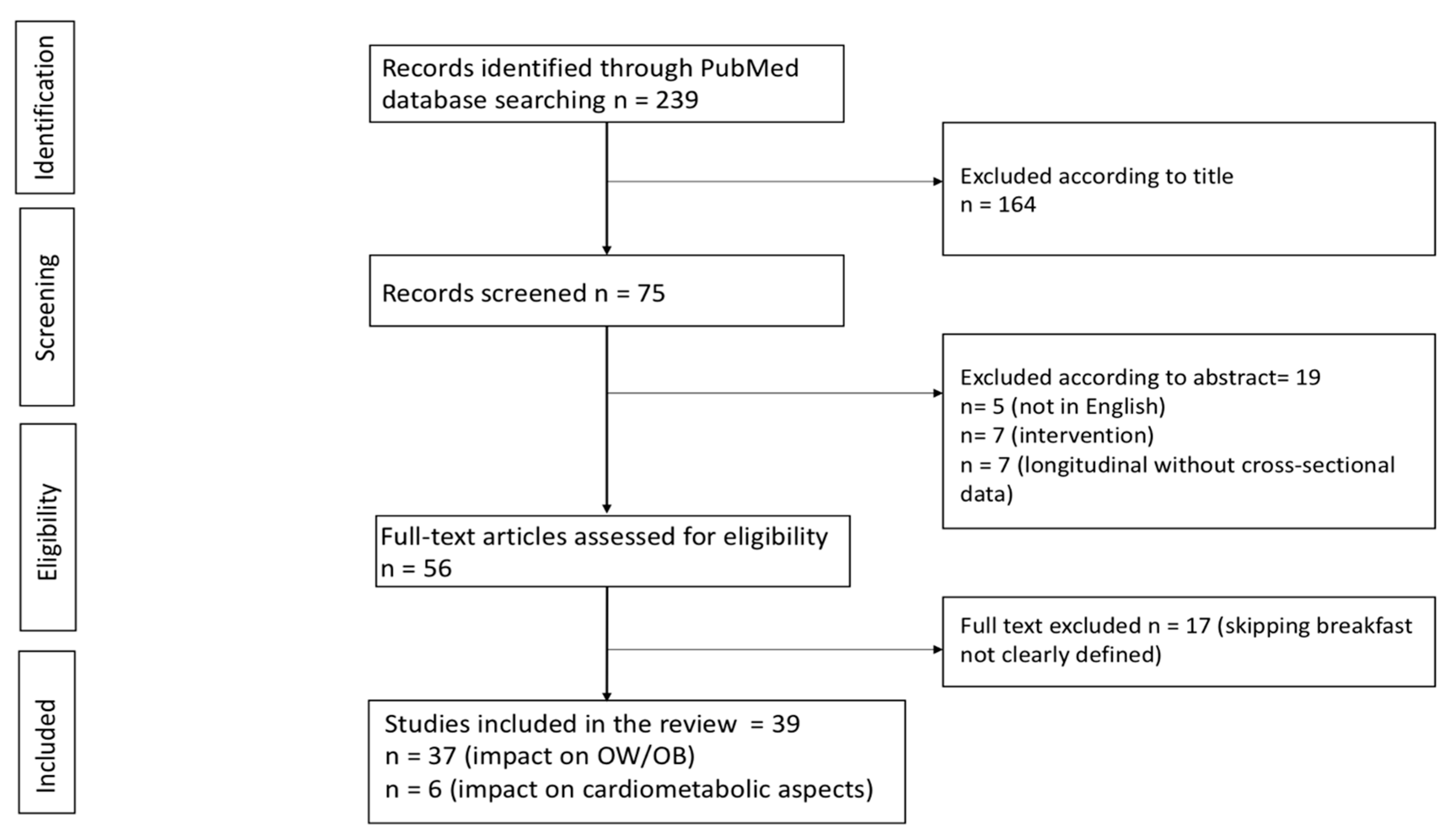
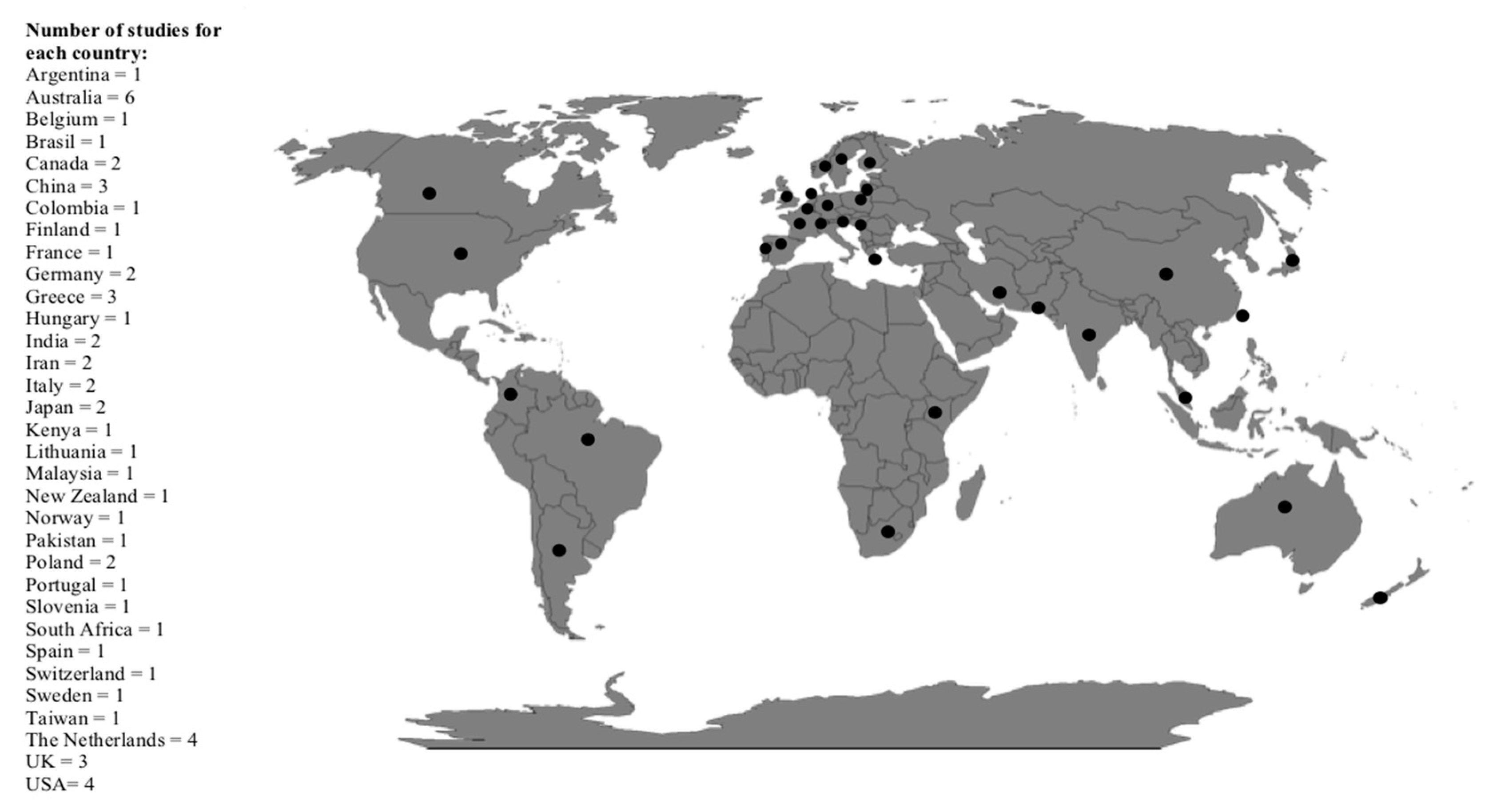
2.4. Identification of Relevant Studies
2.5. Data Extraction, Synthesis, and Quality Assessment
3. Results
3.1. Association of Skipping Breakfast with Overweight/Obesity
3.2. Association of Skipping Breakfast with Metabolic and Nutritional Aspects
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Moraeus, L.; Lissner, L.; Yngve, A.; Poortvliet, E.; Al-Ansari, U.; Sjöberg, A. Multi-level influences on childhood obesity in Sweden: Societal factors, parental determinants and child/’s lifestyle. Int. J. Obes. 2012, 36, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.M.A.; van Raaij, J.M.A.; Yngve, A.; Sjöberg, A.; Kunešová, M.; Duleva, V.; Petrauskiene, A.; Rito, A.I.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Health-risk behaviours on nutrition and physical activity in 6–9-year-old schoolchildren. Public. Health. Nutr. 2015, 18, 3108–3124. [Google Scholar] [CrossRef] [PubMed]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [CrossRef] [PubMed]
- Delva, J.; Omalley, P.M.; Johnston, L.D. Racial/ethnic and socioeconomic status differences in overweight and health-related behaviors among American students: National trends 1986–2003. J. Adolesc. Health. 2006, 39, 536–545. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Ruszczynski, M. Systematic review demonstrating that breakfast consumption influences body weight outcomes in children and adolescents in Europe. Crit. Rev. Food Sci. Nutr. 2010, 50, 113–119. [Google Scholar] [CrossRef]
- Affenito, S.G.; Thompson, D.; Dorazio, A.; Albertson, A.M.; Loew, A.; Holschuh, N.M. Ready-to-eat cereal consumption and the School Breakfast Program: Relationship to nutrient intake and weight. J. Sch. Health. 2013, 83, 28–35. [Google Scholar] [CrossRef]
- Ask, A.S.; Hernes, S.; Aarek, I.; Johannessen, G.; Haugen, M. Changes in dietary pattern in 15 years old adolescents following a 4 month dietary intervention with school breakfast—a pilot study. Nutr. J. 2006, 5, 33. [Google Scholar] [CrossRef]
- Utter, J.; Scragg, R.; Schaaf, D.; Fitzgerald, E.; Wilson, N. Correlates of body mass index among a nationally representative sample of New Zealand children. Int. J. Pediatr. Obes. 2007, 2, 104–113. [Google Scholar] [CrossRef]
- Vereecken, C.; Dupuy, M.; Rasmussen, M.; Kelly, C.; Nansel, T.R.; Al Sabbah, H.; Baldassari, D.; Jordan, M.D.; Maes, L.; Niclasen, B.V.; et al. Breakfast consumption and its socio-demographic and lifestyle correlates in schoolchildren in 41 countries participating in the HBSC study. Int. J. Public Health 2009, 54, 180–190. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.J.; Gall, S.L.; McNaughton, S.A.; Blizzard, L.; Dwyer, T.; Venn, A.J. Skipping breakfast: Longitudinal associations with cardiometabolic risk factors in the Childhood Determinants of Adult Health Study. Am. J. Clin. Nutr. 2010, 92, 1316–1325. [Google Scholar] [CrossRef] [PubMed]
- Dialektakou, K.D.; Vranas, P.B. Breakfast skipping and body mass index among adolescents in Greece: Whether an association exists depends on how breakfast skipping is defined. J. Am. Diet. Assoc. 2008, 108, 1517–1525. [Google Scholar] [CrossRef] [PubMed]
- Dubois, L.; Girard, M.; Kent, M.P.; Farmer, A.; Tatone-Tokuda, F. Breakfast skipping is associated with differences in meal patterns, macronutrient intakes and overweight among pre-school children. Public Health Nutr. 2008, 12, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.; Teyhan, A.; Maynard, M.J.; Cruickshank, J.K. Ethnic differences in overweight and obesity in early adolescence in the MRC DASH study: The role of adolescent and parental lifestyle. Int. J. Epidemiol. 2008, 37, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Duncan, J.S.; Schofield, G.; Duncan, E.K.; Rush, E.C. Risk factors for excess body fatness in New Zealand children. Asia Pac. J. Clin. Nutr. 2008, 17, 138–147. [Google Scholar] [PubMed]
- Croezen, S.; Visscher, T.L.; Ter Bogt, N.C.; Veling, M.L.; Haveman-Nies, A. Skipping breakfast, alcohol consumption and physical inactivity as risk factors for overweight and obesity in adolescents: Results of the E-MOVO project. Eur. J. Clin. Nutr. 2009, 63, 405–412. [Google Scholar] [CrossRef]
- Nagel, G.; Wabitsch, M.; Galm, C.; Berg, S.; Brandstetter, S.; Fritz, M.; Klenk, J.; Peter, R.; Prokopchuk, D.; Steiner, R.; et al. Determinants of obesity in the Ulm Research on Metabolism, Exercise and Lifestyle in Children (URMEL-ICE). Eur. J. Pediatr. 2009, 168, 1259–1267. [Google Scholar] [CrossRef]
- Sun, Y.; Sekine, M.; Kagamimori, S. Lifestyle and overweight among Japanese adolescents: The Toyama Birth Cohort Study. J. Epidemiol. 2009, 19, 303–310. [Google Scholar] [CrossRef]
- Maddah, M.; Nikooyeh, B. Factors associated with overweight in children in Rasht, Iran: Gender, maternal education, skipping breakfast and parental obesity. Public Health Nutr. 2010, 13, 196–200. [Google Scholar] [CrossRef]
- Isacco, L.; Lazaar, N.; Ratel, S.; Thivel, D.; Aucouturier, J.; Doré, E.; Meyer, M.; Duché, P. The impact of eating habits on anthropometric characteristics in French primary school children. Child Care Health Dev. 2010, 36, 835–842. [Google Scholar] [CrossRef]
- Deshmukh-Taskar, P.; Nicklas, T.A.; Radcliffe, J.D.; O’Neil, C.E.; Liu, Y. The relationship of breakfast skipping and type of breakfast consumed with overweight/obesity, abdominal obesity, other cardiometabolic risk factors and the metabolic syndrome in young adults. The National Health and Nutrition Examination Survey (NHANES): 1999–2006. Public Health Nutr. 2013, 16, 2073–2082. [Google Scholar] [CrossRef] [PubMed]
- So, H.K.; Nelson, E.A.; Li, A.M.; Guldan, G.S.; Yin, J.; Ng, P.C.; Sung, R.Y. Breakfast frequency inversely associated with BMI and body fatness in Hong Kong Chinese children aged 9-18 years. Br. J. Nutr. 2011, 106, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Tin, S.P.; Ho, S.Y.; Mak, K.H.; Wan, K.L.; Lam, T.H. Breakfast skipping and change in body mass index in young children. Int. J. Obes. 2011, 35, 899–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushtaq, M.U.; Gull, S.; Mushtaq, K.; Shahid, U.; Shad, M.A.; Akram, J. Dietary behaviors, physical activity and sedentary lifestyle associated with overweight and obesity, and their socio-demographic correlates, among Pakistani primary school children. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuriyan, R.; Tinku, T.; Sumithra, S.; Lokesh, D.P.; Sheth, N.R.; Joy, R.; Bhat, S.; Kurbad, A.V. Potential Factors Related to Waist Circumference in Urban South Indian Children. Indian Pediatrics. 2012, 49, 16. [Google Scholar] [CrossRef]
- Kyeariazis, I.; Rekleiti, M.; Saridi, M.; Beliotis, E.; Toska, A.; Souliotis, K.; Wozniak, G. Prevalence of obesity in children aged 6–12 years in Greece: Nutritional behaviour and physical activity. Arch. Med. Sci. 2012, 8, 859–864. [Google Scholar] [CrossRef]
- Van Lippevelde, W.; Te Velde, S.J.; Verloigne, M.; Van Stralen, M.M.; De Bourdeaudhuij, I.; Manios, Y.; Bere, E.; Vik, F.N.; Jan, N.; Fernández Alvira, J.M.; et al. Associations between family-related factors, breakfast consumption and BMI among 10- to 12-year-old European children: The cross-sectional ENERGY-study. PLoS One 2013, 8, e79550. [Google Scholar] [CrossRef]
- Januszek-Trzciąkowska, A.; Małecka-Tendera, E.; Klimek, K.; Matusik, P. Obesity risk factors in a representative group of Polish prepubertal children. Arch. Med. Sci. 2014, 10, 880–885. [Google Scholar] [CrossRef]
- Kupers, L.K.; de Pijper, J.J.; Sauer, P.J.J.; Stolk, R.P.; Corpeleijn, E. Skipping breakfast and overweight in 2- and 5-year-old Dutch children—The GECKO Drenthe cohort. Int. J. Obes. 2014, 38, 569–571. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Nicklas, T.A.; Fulgoni, V.L. Nutrient intake, diet quality, and weight measures in breakfast patterns consumed by children compared with breakfast skippers: NHANES 2001–2008. AIMS Public Health. 2015, 2, 441–468. [Google Scholar] [CrossRef]
- Smetanina, N.; Albaviciute, E.; Babinska, V.; Karinauskiene, L.; Albertsson-Wikland, K.; Petrauskiene, A.; Verkauskiene, R. Prevalence of overweight/obesity in relation to dietary habits and lifestyle among 7–17 years old children and adolescents in Lithuania. BMC Public Health. 2015, 15, 1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakrzewski, J.K.; Gillison, F.B.; Cumming, S.; Church, T.S.; Katzmarzyk, P.T.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Denstel, K.D.; Fogelholm, M.; et al. Associations between breakfast frequency and adiposity indicators in children from 12 countries. Int. J. Obes. 2015, 5, S80–S88. [Google Scholar] [CrossRef] [PubMed]
- Wijtzes, A.I.; Jansen, W.; Bouthoorn, S.H.; van Lenthe, F.J.; Franco, O.H.; Hofman, A.; Jaddoe, V.W.V.; Raat, H. Meal-skipping behaviors and body fat in 6-year-old children. J. Pediatr. 2016, 168, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Fayet-Moore, F.; Kim, J.; Sritharan, N.; Petocz, P. Impact of Breakfast Skipping and Breakfast Choice on the Nutrient Intake and Body Mass Index of Australian Children. Nutrients 2016, 8, 487. [Google Scholar] [CrossRef] [PubMed]
- Alsharairi, N.A.; Somerset, S.M. Skipping breakfast in early childhood and its associations with maternal and child BMI: A study of 2–5-year-old Australian children. Eur. J. Clin. Nutr. 2016, 70, 450–455. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; McConnell, A.; Tuck, K.; Petocz, P. Breakfast and breakfast cereal choice and its impact on nutrient and sugar intakes and anthropometric measures among a nationally representative sample of australian children and adolescents. Nutrients 2017, 9, 1045. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; Breslin, M.C.; McNaughton, S.A.; Gall, S.L.; Blizzard, L.; Venn, A.J. Skipping breakfast among Australian children and adolescents; findings from the 2011–2012 National Nutrition and Physical Activity Survey. Aust. N. Z. J. Public Health 2017, 41, 572–578. [Google Scholar] [CrossRef]
- Gotthelf, S.J.; Tempestti, C.P. Breakfast, nutritional status, and socioeconomic outcome measures among primary school students from the City of Salta: A cross-sectional study. Arch. Argent. Pediatr. 2017, 115, 424–431. [Google Scholar] [CrossRef]
- Nilsen, B.B.; Yngve, A.; Monteagudo, C.; Tellström, R.; Scander, H.; Werner, B. Reported habitual intake of breakfast and selected foods in relation to overweight status among seven- to nine-year-old Swedish children. Scand. J. Public Health 2017, 45, 886–894. [Google Scholar] [CrossRef]
- Kesztyüs, D.; Traub, M.; Lauer, R.; Kesztyüs, T.; Steinacker, J.M. Skipping breakfast is detrimental for primary school children: Cross-sectional analysis of determinants for targeted prevention. BMC Public Health 2017, 17, 258. [Google Scholar] [CrossRef]
- Zalewska, M.; Maciorkowska, E. Selected nutritional habits of teenagers associated with overweight and obesity. Peer. J. 2017, 5, e3681. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, J.D.; Palla, L.; Pot, G.K. Breakfast consumption and nutrient intakes in 4–18-year-olds: UK National Diet and Nutrition Survey Rolling Programme (2008–2012). Br. J. Nutr. 2017, 118, 280–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tee, E.S.; Nurliyana, A.R.; Norimah, A.K.; Mohamed, H.J.B.J.; Tan, S.Y.; Appukutty, M.; Hopkins, S.; Thielecke, F.; Ong, M.K.; Ning, C.; et al. Breakfast consumption among Malaysian primary and secondary school children and relationship with body weight status - Findings from the MyBreakfast Study. Asia Pac. J. Clin. Nutr. 2018, 27, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Archero, F.; Ricotti, R.; Solito, A.; Carrera, D.; Civello, F.; Di Bella, R.; Bellone, S.; Prodam, F. Adherence to the mediterranean diet among school children and adolescents living in northern Italy and unhealthy food behaviors associated to overweight. Nutrients 2018, 10, 1322. [Google Scholar] [CrossRef] [PubMed]
- Shafiee, G.; Kelishadi, R.; Qorbani, M.; Motlagh, M.E.; Taheri, M.; Ardalan, G.; Taslimi, M.; Poursafa, P.; Heshmat, R.; Larijani, B. Association of breakfast intake with cardiometabolic risk factors. Pediatr. 2013, 89, 575–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, C.Y.; Huang, Y.C.; Lo, W.T.C.; Wahlqvist, M.L.; Lee, M.S. Breakfast is associated with the metabolic syndrome and school performance among Taiwanese children. Res. Dev. Disabil. 2015, 44, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Marlatt, K.L.; Farbakhsh, K.; Dengel, D.R.; Lytle, L.A. Breakfast and fast food consumption are associated with selected biomarkers in adolescents. Prev. Med. Rep. 2016, 3, 49–52. [Google Scholar] [CrossRef] [Green Version]
- Monzani, A.; Rapa, A.; Fuiano, N.; Diddi, G.; Prodam, F.; Bellone, S.; Bona, G. Metabolic syndrome is strictly associated with parental obesity beginning from childhood. Clin. Endoc. 2013, 81, 45–51. [Google Scholar] [CrossRef]
- Osawa, H.; Sugihara, N.; Ukiya, T.; Ishizuka, Y.; Birkhed, D.; Hasegawa, M.; Matsukubo, T. Metabolic syndrome, lifestyle, and dental caries in japanese school children. Bull. Tokyo Dent. Coll. 2015, 56, 233–241. [Google Scholar] [CrossRef]
- Reddan, J.; Wahlstrom, K.; Reicks, M. Children’s perceived benefits and barriers in relation to eating breakfast in schools with or without Universal School Breakfast. J. Nutr. Educ. Behav. 2002, 34, 47–52. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K.; American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; Stroke Council. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- Oosterman, J.E.; Kalsbeek, A.; la Fleur, S.E.; Belsham, D.D. Impact of nutrients on circadian rhythmicity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 308, R337–R350. [Google Scholar] [CrossRef]
- Walker, J.L.; Ardouin, S.; Burrows, T. The validity of dietary assessment methods to accurately measure energy intake in children and adolescents who are overweight or obese: A systematic review. Eur. J. Clin. Nutr. 2018, 72, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Fleig, D.; Randler, C. Association between chronotype and diet in adolescents based on food logs. Eat. Behav. 2009, 10, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Broussard, J.L.; Van Cauter, E. Disturbances of sleep and circadian rhythms: Novel risk factors for obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Roßbach, S.; Diederichs, T.; Nöthlings, U.; Buyken, A.E.; Alexy, U. Relevance of chronotype for eating patterns in adolescents. Chronobiol. Int. 2018, 35, 336–347. [Google Scholar] [CrossRef] [PubMed]
- Dhurandhar, E.J. True, true, unrelated? A review of recent evidence for a causal influence of breakfast on obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, A.; Schwab, U.; Kolehmainen, M.; Pirkola, J.; Järvelin, M.R.; Laitinen, J. Associations of meal frequency and breakfast with obesity and metabolic syndrome traits in adolescents of Northern Finland Birth Cohort 1986. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, M.; Gustafsson, P.E.; Wennberg, P.; Hammarström, A. Poor breakfast habits in adolescence predict the metabolic syndrome in adulthood. Public Health Nutr. 2015, 18, 122–129. [Google Scholar] [CrossRef]
- Nas, A.; Mirza, N.; Hägele, F.; Kahlhöfer, J.; Keller, J.; Rising, R.; Kufer, T.A.; Bosy-Westphal, A. Impact of breakfast skipping compared with dinner skipping on regulation of energy balance and metabolic risk. Am. J. Clin. Nutr. 2017, 105, 1351–1361. [Google Scholar] [CrossRef]
- Ballon, A.; Neuenschwander, M.; Schlesinger, S. Breakfast skipping is associated with increased risk of type 2 diabetes among adults: A systematic review and meta-analysis of prospective cohort studies. J. Nutr. 2018, 149, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Jakubowicz, D.; Wainstein, J.; Landau, Z.; Raz, I.; Ahren, B.; Chapnik, N.; Ganz, T.; Menaged, M.; Barnea, M.; Bar-Dayan, Y.; et al. Influences of Breakfast on Clock Gene Expression and Postprandial Glycemia in Healthy Individuals and Individuals With Diabetes: A Randomized Clinical Trial. Diabetes Care 2017, 40, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Dhurandhar, E.J.; Dawson, J.; Alcorn, A.; Larsen, L.H.; Thomas, E.A.; Cardel, M.; Bourland, A.C.; Astrup, A.; St-Onge, M.P.; Hill, J.O.; et al. The effectiveness of breakfast recommendations on weight loss: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Sievert, K.; Hussain, S.M.; Page, M.J.; Wang, Y.; Hughes, H.J.; Malek, M.; Cicuttini, M.F. Effect of breakfast on weight and energy intake: Systematic review and meta-analysis of randomised controlled trials. BMJ 2019, 364, l42. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Minguez, J.; Dashti, H.S.; Madrid-Valero, J.J.; Madrid, J.A.; Saxena, R.; Scheer, F.A.; Ordoñana, J.R.; Garaulet, M. Heritability of the timing of food intake. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Mathias, P.C.; Elmhiri, G.; de Oliveira, J.C.; Delayeare-Orthez, C.; Barella, L.F.; Tófolo, L.P.; Fabricio, G.S.; Chango, A.; Abdennebi-Najar, L. Maternal diet, bioactive molecules, and exercising as reprogramming tools of metabolic programming. Eur. J. Nutr. 2014, 53, 711–722. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference (Author, year, n) | Study Subjects | Methods | Skipping Breakfast Definition | Breakfast Evaluation Method | OB/OW Definition | Prevalence of Breakfast Skippers | Results | Impact of Skipping Breakfast on OW/OB |
|---|---|---|---|---|---|---|---|---|
| Dialektakou 2008 [12] | N = 811, aged 14.9–21.2 years, M and F, Greece | Cross-sectional, self-reported questionnaires, measured height and weight | 24 definitions evaluating breakfast consumption on the day of data collection, during the whole year, during the previous week, and on weekends/holidays | Not specified | Age- and sex-specific BMI cut-offs according to IOTF criteria | 3.6–74.7% (according to different definitions) | Fewer breakfast-skipping variables associated with BMI than with OW/OB. Fewer associations when controlling for potential confounders. Fewer associations for variables corresponding to some definitions. | ↑ |
| Dubois 2008 [13] | N = 1549; aged 44–56 months, M and F, Canada | Longitudinal study, parent-report questionnaires, measured height and weight (cross-sectional data considered) | Frequency of breakfast eating: (1) yes, every morning; (2) regularly but not every day; (3) only on occasion; and (4) never. Categories 2 to 4 were classified as ‘breakfast skippers’ | Eating behavior questionnaire (Enquete sociale et de sante’ aupres des enfants et des adolescents Quebecois -Health and Social Survey of Quebec Children and Adolescents) and a 24 h dietary recall interview | Age- and sex-specific BMI z-score cut-offs according to CDC criteria | 10% | ↑ intake of energy, carbohydrates or servings of grain products in breakfast skippers | ↑ |
| Harding 2008 [14] | N = 6599, aged 11–13 years, M and F, UK | Cross-sectional, self-reported questionnaires, measured height and weight | Number of eaten breakfasts per week (Every day; 3–4 days a week; 1–2 days a week; Never or hardly ever) | http://www.sphsu.mrc.ac.uk/studies/dash/ Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to IOTF criteria | 32.6–53% not eating breakfast every day | Increased risk for obesity in breakfast skippers (girls OR 1.74, 95% CI 1.30–2.34; boys OR 2.06; CI 1.57–2.70) | ↑ |
| Duncan 2008 [15] | N = 1229, aged 5–11 years, M and F, New Zeland | Cross-sectional, proxy questionnaire administered to the parents, measured height and weight, BIA | Number of eaten breakfasts in the last full week (0–7 days per week) | 7-day recall | Boys and girls were classified as “overfat” if their % BF exceeded 25% and 30% (respectively) | 1.3 (non-overfat)–2.6% (overfat) never eat breakfast in a week | Breakfast skippers had increased odds of overfat compared with those who had breakfast for five or more days/week. | ↑ |
| Croezen 2009 [16] | N = 25176, aged 13–16 years, M and F, The Netherlands | Cross-sectional, detailed Internet questionnaire, under supervision of instructed teachers following a standardized protocol, self-reported body weight and height | Number of eaten breakfasts per week (0–7 days per week) | Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to Cole’s definition | 29.3–39.2% | Skipping breakfast >2 times/week associated with OW (adjusted OR 1.68 (CI 1.43–1.97) in 13–14 year-aged, and 1.32 (CI 1.14–1.54) in 15–16 year-aged subjects); skipping breakfast every day associated with OB | ↑ |
| Nagel 2009 [17] | N = 1079, aged 6.2–9.2 years, M and F, Germany | Cross-sectional, self-reported questionnaires compiled by children and parents, measured weight, height, upper arm and waist circumference, skin fold thickness | Breakfast consumption before school (yes/no) | Not specified | Age- and sex-specific BMI cut-offs according to IOTF criteria | 13.4% | Breakfast skippers had increased risk for OW (OR 1.73, 95%CI 1.13–2.64) and OB (OR 2.50, 95% CI 1.19–5.29) | ↑ |
| Sun 2009 [18] | N = 5753, aged 12–13 years, M and F, Japan | Cross-sectional, self-reported questionnaires, measured height and weight | Frequency of eating breakfast: daily, almost daily, sometimes, and rarely | Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to IOTF criteria | 1.1% of boys and 0.7% of girls ate breakfast rarely | Skipping breakfast (i.e., eating breakfast rarely) was associated with OW (in boys only after adjustment for age, parental OW and lifestyle variables) | ↑ |
| Maddah 2010 [19] | N = 6635, aged 6–11 years, M and F, Iran | Cross-sectional, self-reported questionnaire given to the parents, measured weight and height | Breakfast skipping (yes/no) | Not specified | Age- and sex-specific BMI cut-offs according to IOTF criteria | Not reported | Higher prevalence of OW/OB in breakfast skippers than in breakfast eaters (boys: 23.6% versus 16.9%, girls: 23.5% versus 17.1%) | ↑ |
| Isacco 2010 [20] | N = 278, aged 6–10 years, M and F, France | Cross-sectional, self-reported questionnaire compiled by the parents in the presence of their child, measured weight, height, WC and skin fold thickness | Frequency of eating breakfast: every day, sometimes, never | Food frequency questionnaire | Age- and sex-specific BMI z-score cut-offs according to CDC criteria | 1.4% never ate breakfast | higher BMI z-score, skinfolds and WC in breakfast skippers | ↑ |
| Deshmukh-Taskar 2010 [21] | N = 9659, aged 9–18 years, M and F, USA | Cross-sectional, self-reported data on 24-h recall methodology over two days (assisted by parent/caregivers for children aged 6 to 11 years), measured weight, height and WC | Breakfast skippers: those who consumed no food or beverages, excluding water, at breakfast | 24-h recall http://www.cdc.gov/nchs/data/nhanes/dr-1-5.pdf. | Age- and sex-specific BMI z-score cut-offs according to CDC criteria | 20% of children, 31.5% of adolescents | Breakfast skippers had higher BMI z-scores and a higher waist circumference than ready-to-eat cereal and other breakfast consumers. Higher prevalence of obesity in breakfast skippers than ready-to-eat cereal consumers | ↑ |
| So 2011 [22] | N = 11570, aged 9–18 years, M and F, Hong Kong | Cross-sectional, self-reported questionnaires, measured height and weight, and BIA | Breakfast skippers (ate breakfast 0–2 times/week); semi-skippers (ate breakfast 3–4 times/week); non-skippers (ate breakfast 5–7 times/week) | Rapid Dietary behavior Assessment questionnaire (daily and weekly dietary behaviors, validated against the 24 h recall nutrient intake data in a smaller sample) | Age- and sex-specific BMI cut-offs according to IOTF criteria | 8% of primary school students and 14% of secondary school students | Breakfast skippers had higher BMI, BMI z-scores and BF% than their counterparts | ↑ |
| Tin 2011 [23] | N = 113457, aged 9–10 years, M and F, Hong Kong | Longitudinal, 2-year follow-up, self-reported questionnaires, measured height and weight (cross-sectional data considered) | Breakfast skippers those who chose ‘no breakfast at all’ | Not specified | Age- and sex-specific BMI cut-offs according to IOTF criteria | 5.3% of boys, 5.2% of girls | Higher mean BMI in breakfast skippers both at baseline (β 0.77, 95% CI 0.67–0.87) and 2 years later (β 0.86, 95% CI 0.78–0.95) | ↑ |
| Mushtaq 2011 [24] | N = 1860, aged 5–12 years, M and F, Pakistan | Cross-sectional, questionnaires administered to the children by senior medical students, measured height and weight | Skipping breakfast once or more in the past week | 7-day recall | BMI z-scores calculated based on the WHO criteria | 8% | Breakfast skippers were significantly more likely to be overweight (15% versus 9%) and obese (13% versus 7%) than breakfast eaters (p = 0.002). Skipping breakfast was associated with overweight among girls (p < 0.001). Skipping breakfast as independent predictor of OW (OR 1.82, 95% CI 1.22–2.71) | ↑ (OW in girls) |
| Kuriyan 2012 [25] | N = 8444 (4707 aged 3–10 years; N = 3737 aged 10–16 years), M and F, Bangalore | Cross-sectional, parent/student-report questionnaires, measured height and weight, WC | Breakfast skipping (yes/no) | Not specified | Indian Academy of Pediatrics cut-off for BMI; WC > 75th percentile for classifying abdominal obesity | Not reported | - | ⇔ WC in children aged 3–10 years ↑ WC in children aged 10–16 years |
| Kyeariazis 2012 [26] | N = 2374, aged 6–12 years, M and F, Greece | Cross-sectional, self-reported questionnaires, measured height and weight | Breakfast skipping (yes/no) | Closed format questions in the form of multiple choice Questions | Age- and sex-specific BMI cut-offs according to Cole’s definition | Not reported | Skipping breakfast had a positive association with OB | ↑ |
| Van Lippevelde 2013 [27] | N = 6374, aged 10–12 years, M and F, Belgium, Greece, Hungary, the Netherlands, Norway, Slovenia, Spain, and Switzerland | Cross-sectional, self-reported questionnaires compiled by the children during school-time, measured weight and height | Breakfast frequency per week (0–7) calculated by adding up the breakfasts usually had on schooldays per week (0–5) and on weekend days per week (0–2) | http://projectenergy.eu Food frequency questionnaire | BMI z-scores calculated based on the WHO criteria | Not reported | Children’s breakfast consumption negatively related to children’s BMI-z-score | ↑ |
| Januszek-Trzciąkowska 2014 [28] | N = 2571, aged 7–9 years, M and F, Poland | Cross-sectional, self-reported questionnaire compiled by the parents, measured weight and height | Breakfast frequency: always, usually never | Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to IOTF criteria | 10.3% in girls, 9.1% in boys | Increased OB risk in girls irregularly or never eating breakfast (always versus usually, OR 2.71, 95% CI 1.33–5.51; always versus never OR 1.63, 95% CI 1.08–2.47) | ↑ only for girls |
| Kupers 2014 [29] | T1: 2 years of age; N = 1488 T2: 5 years of age; N = 1366 M and F, The Netherlands | Longitudinal; parent-report questionnaires; measured height and weight (cross-sectional data considered) | Breakfast frequency per week (0–7), categorized as “eating breakfast daily” (7 times per week) or “not eating breakfast daily” (<7 times per week) | Food frequency questionnaire | Age- and sex-specific BMI cut-offs according Dutch reference growth charts | At T1, 3.0% of the children did not eat breakfast daily; at T2, 5.3% | No association between skipping breakfast and overweight, neither at age 2 nor at age 5 | ⇔ |
| O’Neil 2015 [30] | N = 14200, aged 2–18 years, M and F, USA | Cross-sectional, self-reported questionnaires (complied by parents/guardians of 2–5 year children; by 6–11 year children assisted by an adult; older children provided their own recall), measured weight and height | 24-h dietary recall: no breakfast or 11 possible breakfast patterns | 24-h dietary recall interviews using an automated multiple-pass method http://www.cdc.gov/nchs/data/nhanes/nhanes_03_04/DIETARY_MEC.pdf. | Age- and sex-specific BMI cut-offs according to CDC criteria | 18.7% | Mean BMI z-scores were lower among consumers of five breakfast patterns (grain/lower fat milk/sweets/fruit juice, pre-sweetened ready-to-eat cereal/whole milk, soft drinks/fruit juice/grain/potatoes, ready-to-eat cereal/whole milk, and cooked cereal/milk/fruit juice), compared to breakfast skippers. | ↑ |
| Smetanina 2015 [31] | N = 3990, aged 7–17 years, M and F, Lithuania | Cross-sectional, self-reported questionnaires (parents of younger age (7–9 years old) participants filled-in the questionnaire at home and older children and adolescents filled-in it themselves at school), measured weight and height | breakfast eating frequency per week: “Everyday” (“Everyday” and “4–6 times per week”), “1–3 times per week”, and “Never” | Modified WHO questionnaires (conducted by Health behavior in School-aged Children (HBSC) and COSI study groups).Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to IOTF criteria | Never eating breakfast: 6.2% in underweight, 6.5% in NW, 9.6% in OW/OB | The prevalence of subjects never having breakfast was significantly higher in OW/OB than in NW (9.6% versus 6.5%) | ↑ |
| Zakrzewski 2015 [32] | N = 6841, aged 9–11 years, M and F, Australia, Brasil, Canada, China, Colombia, Finland, India, Kenya, Portugal, South Africa, UK, US | Cross-sectional, self-reported questionnaires, measured height, weight and BF% | Breakfast frequency per week (separately for weekdays and weekend days). 1. Three-category definition: weekly breakfast frequency coded as rare (0–2 days per week), occasional (3–5 days per week) and frequent (6–7 days per week). 2. Two-category definition: weekly breakfast frequency recoded as less than daily (0–6 days per week) or daily (7 days per week). | Food frequency questionnaire | BMI z-scores calculated based on the WHO criteria | Breakfast consumption: 6.3% rarely, 27.7% less than daily | Frequent breakfast consumption was associated with lower BMI z-scores compared with occasional (p < 0.0001) and rare (p < 0.0001) consumption, as well as lower BF% compared with occasional (p < 0.0001) and rare (p < 0.0001). | ↑ |
| Wijtzes 2016 [33] | N = 5913, T1: 4 years of age T2: 6 years of age, M and F, The Netherlands | Longitudinal, parent-report questionnaires, measured height and weight, percent fat mass by dual-energy X-ray absorptiometry (at age 6 years) (cross-sectional data considered) | At age 4 years: weekly consumption of breakfast (“never,” “1–2 days per week,” “3–4 days per week,” “5–6 days per week,” and “every day”, coded as 1–5); At age 6 years: the number of days of breakfast consumption assessed separately for weekdays (coded as 0–5) and weekend days (coded as 0–2), and the scores were summed to calculate total weekly consumption (0–7). Breakfast skipping defined as consumption <7 days per week | Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to IOTF criteria | Not reported | Breakfast skipping at age 4 years associated with increased % fat mass at age 6 years (β = 1.38; 95% CI: 0.36–2.40) | ↑ |
| Fayet-Moore 2016 [34] | N = 4487, aged 2–16 years, M and F, Australia | Cross-sectional, computer-assisted interview based on 24-h recall methodology over two days from participants or their caregivers, measured height and weight | Breakfast skippers were children who did not consume an energy containing food or beverage during breakfast on 2 recall days | 24-h recall methodology | BMI z-score or centile adjusted for age and sex was calculated using the US CDC 2000 growth reference chart | 4% | Higher prevalence for OW/OB in breakfast skippers than in breakfast consumers (21.2% and 23.2% versus 16.4% and 16.5%, respectively) | ↑ |
| Alsharairi 2016 [35] | T1 (2006): N = 4601, 2–3 age of years T2 (2008): N = 4381, 4–5 years of age, M and F, Australia | Cross-sectional and longitudinal study, face-to-face mother’s interview, measured height and weight | Breakfast consumption in the day of interview (yes/no) | Not specified | Age- and sex-specific BMI cut-offs according to IOTF criteria | Not reported | OB boys at T1 (OR 2.38, 95% CI: 1.04–5.43) and T2 (OR 2.32, 95% CI: 1.01–5.32) and OB girls at T2 (OR 2.26, 95% CI: 1.14–4.46) were more likely to skip breakfast compared with non-overweight | ↑ |
| Fayet-Moore 2017 [36] | N = 2812, aged 2–18 years, M and F, Australia | Cross-sectional, face-to-face interviews, measured height and weight | Breakfast skipping or eating during the 24 h prior to the interview day | 24-h recall methodology | Age- and sex-specific BMI cut-offs according to the WHO criteria | 9% | No associations between anthropometric measures and breakfast or breakfast cereal choice were found Breakfast skippers: ↑ higher saturated fat intake ↓ intakes of dietary fibers and most micronutrients (p < 0.001) | ⇔ |
| Smith 2017 [37] | N = 1592, aged 2–17 years, M and F, Australia | Cross-sectional, computer-assisted interview based on 24-h recall methodology (for 2–5 year children completed by an adult; for 6–8-years an adult was interviewed with help from the child; 9–11 year children were interviewed directly with assistance from an adult; 12–17-year were interviewed directly, with the adult remaining in the room for those aged 12–14 years); measured weight and height | Breakfast skippers if they did not define an eating occasion as ‘breakfast’ in the 24-h recall or the energy intake for the “breakfast” occasion was <210 kJ | 24-h recall methodology | Age- and sex-specific BMI cut-offs according to Cole’s definition | 11.8% of boys and 14.8% girls skipped on one day and 1.4% boys and 3.8% girls skipped on both days | The odds of skipping breakfast were progressively higher with increasing BMI category | ↑ |
| Gotthelf 2017 [38] | N = 2083, aged 9–13 years, M and F, Argentina | Cross-sectional, self-reported questionnaires compiled by children and parents, measured weight and height | Breakfast habit: eating breakfast on the day of the survey (yes/no). Frequency: always (6–7 days/week), sometimes (2–5 days/week), never (0–1 day/week). | Food frequency questionnaire | BMI z- scores calculated based on the WHO criteria | 64.1% of students from peri-urban schools and 46.1% of students from urban schools | Among breakfast skippers, 40.7% of the girls and 54.7% of the boys were OW/OB. A higher probability of skipping breakfast was associated with obesity. | ↑ |
| Nilsen 2017 [39] | N = 2620, aged 7–9 years, M and F, Sweden | Cross-sectional, proxy questionnaire filled out by the parents or guardians, measured height and weight | Number of eaten breakfasts over a typical week (Every day; most days, i.e., 4–6 days a week; some days, i.e., 1–3 days a week; Never) | Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to Swedish national growth reference | 4.6% | Association between OW/OB and not having breakfast every day (OR 1.9 (CI 1.18–3.13)) | ↑ |
| Kesztyus 2017 [40] | N = 1943, aged 7.1 ± 0.6 years, M and F, Germany | Cross-sectional, proxy questionnaire administered to the parents, measured height, weight and WC | 4-point scale, the results were subsequently dichotomized for analyses (never, rarely versus often, always) | Food frequency questionnaire | Age- and sex-specific BMI cut-offs according to Swedish national growth reference; abdominal obesity as WHtR >0.5 or >0.47 for girls and 0.48 for boys | 13.1% | Skipping breakfast associated with OW (crude OR 2.02 (CI 1.18–3.43)), OB (crude OR 1.94 (CI 1.03–3.66)), abdominal OB with WHtR >0.5 (crude OR 2.51 (CI 1.63–3.88)), abdominal OB with WHtR >0.47/0.48 (crude OR 2.20 (CI 1.58–3.07)) | ↑ |
| Zalewska 2017 [41] | N = 1999, aged 18 years, M and F, Poland | Cross-sectional, self-reported questionnaires, measured height and weight | Breakfast habit: skipped, <8 AM, ≥8 AM | Not specified | BMI calculated based on the WHO criteria | 25% | No difference in the prevalence of breakfast skippers between NW and OW/OB | ⇔ |
| Coulthard 2018 [42] | N = 1686, aged 4–18 years, M and F, UK | Cross-sectional, 4-day food diary to be completed by the children, or their parent for those aged 11 years and under, measured weight and height | Those consuming breakfast every diary day, those consuming breakfast on at least one but not all diary days, and those not consuming breakfast on any diary day | 4-day food diary | Age- and sex-specific BMI cut-offs according to Cole’s definition (1990 UK charts) | 19.9% of girls and 14.5% of boys | No differences in weight status by breakfast eating habits. The overall nutritional profile of the children in terms of fiber and micronutrient intake was superior in frequent breakfast consumers (micronutrients: folate, calcium, iron and iodine (p < 0.01) | ⇔ |
| Tee 2018 [43] | N = 8332, aged 6–17 years, M and F, Malaysia | Cross-sectional, self-administered questionnaire with assistance to children aged 10 years and above, proxy questionnaire administered to the parent for children aged 6 to 9 years; measured weight and height | Breakfast skippers (ate breakfast 0–2 days/week), irregular breakfast eaters (ate breakfast 3–4 days/week) and regular breakfast eaters (ate breakfast ≥5 days/week) | Food frequency questionnaire | BMI z-scores calculated based on the WHO criteria | 9.3% in primary school children and 15.9% in secondary school children | Compared to regular breakfast eaters, the risk of being OW/OB was higher in 6–12 years boys who skipped breakfast (OR 1.71, 95%CI 1.26–2.32), in 6–12 years girls (OR 1.36, 95% CI = 1.02–1.81) and in 12–17 years girls (OR 1.38, 95% CI 1.01–1.90) | ↑ |
| Archero 2018 [44] | N = 669, aged 6–16 years, M and F, Italy | Cross-sectional, self-reported questionnaires compiled by the children during school-time, in the presence of a teachers and medical staff, measured weight and height | Breakfast skipping (yes/no) | Italian version KIDMED index, a questionnaire of dichotomous (positive/negative) items | Age- and sex-specific BMI cut-offs according to IOTF criteria | 14.8% in primary school children and 21.9% in secondary school children | OW/OB skipped breakfast more frequently than NW (chi-squared 3.556, p < 0.04). Increased risk for OW/OB in non-Italian breakfast skippers (OR 16.05, CI 95% 1.93–133.27, p < 0.01) | ↑ |
| Smith 2010 [11] | T1 (1985): N = 6559; 9–15 years of age T2 (2004–2006): 26–36 years of age M and F, Australia | The Childhood Determinants of Adult Health (CDAH) study. T1: self-report questionnaires; were measured: height and weight. T2: self-report questionnaires; were measured: height, weight, waist WC and BP; a venous blood sample was collected for lipid profile and glucose metabolism | T1: Breakfast consumption was assessed by using the question “Do you usually eat something before school?” “Yes” or “no” T2: Skipping breakfast was defined as not eating between 06.00 and 09.00 | T1: Not specified. T2: Food-frequency questionnaire | Age- and sex-specific BMI cut-offs according to Cole’s cut-off | Skipping breakfast: 14.2% in childhood; 27.5% in adulthood | In both childhood and adulthood: ↑ WC (mean difference: 4.63 cm; 95% CI: 1.72, 7.53 cm) | ↑ |
| Shafiee 2013 [45] | N = 5625, subjects aged 10–18 years; M and F, Iran | The third survey of the national school-based surveillance system (CASPIAN-III); parent-report questionnaires; were measured: height, weight, waist WC and BP; a venous blood sample was collected for lipid profile and glucose metabolism | Subjects were classified into three groups: “regular breakfast eater” (6–7 days/week), “often breakfast eater” (3–5 days/week), and “seldom breakfast eater” (0–2 days/week) | Likert scale questionnaire | Age- and sex-specific BMI cut-offs according to the WHO growth reference standards | The % of subjects classified as: “regular”47.3%, “often” 23.7% and “seldom”29.0%, breakfast eaters | ↑ (p < 0.001) | ↑ |
| Ho 2015 [46] | N = 2401, elementary school children; M and F, Taiwan | Elementary School Children’s Nutrition and Health Survey in Taiwan (NAHSIT); self-report questionnaire; were measured: height, weight, WC and BP; a venous blood sample was collected for lipid profile and glucose metabolism | Breakfast consumption was assessed by using the question “How often do you eat breakfast in a week?” The answer could range from 0 to 7 times. The frequency was classified into three groups, including 0–4, 5–6, and 7 times per week | 24-h recall; food-frequency questionnaire The Youth Healthy Eating Index for the United States of America (US—YHEI) modified to YHEI—Taiwan (YHEI—TW): indicator of dietary quality | Not reported | % Breakfast frequency (times/week): 5.4% (0–4) 5.9% (5–6) 88.7% (7) | ↑ (Children who consumed breakfast daily: ↓ BMI (17.9 kg/m2; p = 0.009); ↓ WC (58.6 cm; p = 0.005)) | ↑ |
| Marlatt, 2016 [47] | N = 367, subjects aged 11–18 years; M and F, Minneapolis | Cross-sectional study; self-report survey; were measured: height, weight, % body fat, and BP; a venous blood sample was collected for lipid profile and glucose metabolism | Breakfast consumption was expressed as average number of days/week that breakfast was consumed | Self-report survey using validated questions (Nelson MC, Lytle LA, 2009. Development and evaluation of a brief screener to estimate fast-food and beverage consumption among adolescents. J Am Diet Assoc; 109, 730–734; 24-h recalls | Age- and sex-specific BMI cut-offs according to the CDC Growth Charts, (2000) | Not reported | ↑ BMI and % body fat | ↑ |
| Reference (Author, Year, n) | Study Subjects | Methods | Skipping Breakfast Definition | Breakfast Evaluation Method | OW/OB Definition | Prevalence of Breakfast Skippers | Association of Skipping Breakfast with OW/OB | Association of Skipping Breakfast with Blood Pressure | Association of Skipping Breakfast with Lipid Profile | Association of Skipping Breakfast with Glucose Metabolism | Association of Skipping Breakfast with Metabolic Syndrome | Association of Skipping Breakfast with Nutrient Intake |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Smith2010 [11] | T1 (1985): N = 6559; 9–15 years of age. T2 (2004–2006): 26–36 years of age. M and F, Australia | The Childhood Determinants of Adult Health (CDAH) study. T1: self-report questionnaires; were measured: height and weight. T2: self-report questionnaires; were measured: height, WC and BP; a venous blood sample was collected for lipid profile and glucose metabolism | T1: Breakfast consumption was assessed by using the question “Do you usually eat something before school?” “Yes” or “no”. T2: Skipping breakfast was defined as not eating between 06.00 and 09.00 | T1: Not specified T2: Food-frequency questionnaire | Age- and sex-specific BMI cut-offs according to Cole’s cut-off | Skipping breakfast: 14.2% in childhood; 27.5% in adulthood | In both childhood and adulthood: ↑ WC (mean difference: 4.63 cm; 95% CI: 1.72, 7.53 cm) | Not reported | ↑ Total (mean difference: 0.40 mmol/L; 95% CI: 0.13, 0.68 mmol/L) and LDL-cholesterol (mean difference: 0.40 mmol/L; 95% CI: 0.16, 0.64 mmol/L) | In both childhood and adulthood: ↑ fasting insulin (mean difference: 2.02 mU/L; 95% CI: 0.75, 3.29 mU/L) | Not reported | Not reported |
| Monzani 2013 [48] | N = 489, subjects aged 6.7 to 13 years; M and F, Italy | Population-based, cross-sectional study; self-reported questionnaire; were measured: height, weight, WC, and BP; a venous blood sample was collected for lipid profile, uric acid and glucose metabolism | Breakfast consumption: yes/no | Not specified | MetS according to modified NCEP-ATP III criteria of Cruz and Goran | Not reported | Not reported | Not reported | Not reported | Not reported | In school-children aged 10.1–13 years: no breakfast consumption (OR = 5.0, 95% CI = 1.5–17.2, p = 0.02) was ↑ in those with MetS | Not reported |
| Shafiee 2013 [45] | N = 5625, subjects aged 10–18 years; M and F, Iran | The third survey of the national school-based surveillance system (CASPIAN-III); parent-report questionnaires; were measured: height, weight, waist circumference (WC) and blood pressure (BP); a venous blood sample was collected for lipid profile and glucose metabolism | Subjects were classified into three groups: “regular breakfast eater” (6–7days/week), “often breakfast eater” (3–5days/week), and “seldom breakfast eater” (0–2 days/week) | Likert scale questionnaire | Age- and sex-specific BMI cut-offs according to the WHO growth reference standards Metabolic syndrome (MetS) was defined based on the Adult Treatment Panel III (ATP III) criteria modified for the pediatric age group | The % of subjects classified as: “regular”47.3%, “often” 23.7% and “seldom”29.0%, breakfast eaters | ↑ (p < 0.001) | ↑ (p < 0.001) | ↑ Triglycerides, LDL-cholesterol (p < 0.001) ↓ HDL-cholesterol | Not reported | ↑ (OR 1.96, 95% CI 1.18–3.27) | Not reported |
| Ho 2015 [46] | N = 2401, elementary school children; M and F, Taiwan | Elementary School Children’s Nutrition and Health Survey in Taiwan (NAHSIT); self-report questionnaire; were measured: height, weight, circumference waist (WC) and blood pressure (BP); a venous blood sample was collected for lipid profile and glucose metabolism | Breakfast consumption was assessed by using the question “How often do you eat breakfast in a week?” The answer could range from 0 to 7 times. The frequency was classified into three groups, including 0–4, 5–6, and 7 times per week | 24-h recall; food-frequency questionnaire. The Youth Healthy Eating Index for the United States of America (US-YHEI) modified to YHEI-Taiwan (YHEI-TW): indicator of dietary quality | MetS was defined based on criteria from Cook | % Breakfast frequency (times/week): 5.4% (0–4) 5.9% (5–6) 88.7% (7) | ↑ (Children who skipped breakfast daily: BMI (17.9 kg/m2; p = 0.009); WC (58.6 cm; p = 0.005)) | ↑ (Children who consumed breakfast daily: systolic BP (97.0 mmHg; p = 0.007); diastolic BP (57.3 mmHg; p = 0.02) Children who consumed breakfast daily versus children who consumed breakfast 0–4 times per week: risks of high blood pressure (OR = 0.37, 95% CI = 0.19–0.71)) | HDL-cholesterol (Children who consumed breakfast daily: ↑ HDL cholesterol (59.5 mg/dL; p = 0.03)) | ⇔ | ↑ (Children who consumed breakfast daily: prevalence of MetS (2.89%) Children who consumed breakfast daily versus children who consumed breakfast 0–4 times per week: risks of MetS (OR = 0.22, 95% CI = 0.09–0.51)) | YHEI-TW scores (Children who consumed breakfast daily versus those who consumed breakfast 0–4 times per week: ↑ intakes of: saturated fat, cholesterol, vitamins A, B1, B2, calcium, phosphorus, magnesium, and potassium; ↑ YHEI-TW scores (better dietary quality)) |
| Osawa 2015 [49] | N = 689, subjects aged 10–13 years; M and F, Japan | Cross-sectional study; self-report questionnaire; were measured: height, weight, WC and BP; a venous blood sample was collected for lipid profile and glucose metabolism | Breakfast consumption was assessed by using the question “Do you have breakfast every day? (Yes, alone/Yes, with family/Seldom/No) | Food-frequency questionnaire designed by members of the Ichikawa Dental Association | MetS was defined based on criteria identified by the Japanese Society of Internal Medicine, the Japan Society for the Study of Obesity and the Ministry of Health, Labour and Welfare in Japan | Not reported | Not reported | Not reported | Not reported | Not reported | Not eating breakfast was associated significantly with MetS or high risk MetS (OR: 2.70, 95% CI: 1.01–7.23, p < 0.05) | Not reported |
| Marlatt, 2016 [47] | N = 367, subjects aged 11–18 years; M and F, Minneapolis | Cross-sectional study; self-report survey; were measured: height, weight, BF%, and blood pressure BP; a venous blood sample was collected for lipid profile and glucose metabolism | Breakfast consumption was expressed as average number of days/week breakfast was consumed | Self-report survey using validated questions (Nelson MC, Lytle LA, 2009. Development and evaluation of a brief screener to estimate fast-food and beverage consumption among adolescents. J Am Diet Assoc; 109, 730–734; 24-h recalls | Age- and sex-specific BMI cut-offs according to the CDC Growth Charts, (2000) MetS was defined based on the Adult Treatment Panel III (ATP III) criteria | Not reported | ↑ BMI and % body fat | ⇔ | ⇔ | ↑ HOMA-IR | ↑ MetS cluster score | Not reported |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monzani, A.; Ricotti, R.; Caputo, M.; Solito, A.; Archero, F.; Bellone, S.; Prodam, F. A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future? Nutrients 2019, 11, 387. https://doi.org/10.3390/nu11020387
Monzani A, Ricotti R, Caputo M, Solito A, Archero F, Bellone S, Prodam F. A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future? Nutrients. 2019; 11(2):387. https://doi.org/10.3390/nu11020387
Chicago/Turabian StyleMonzani, Alice, Roberta Ricotti, Marina Caputo, Arianna Solito, Francesca Archero, Simonetta Bellone, and Flavia Prodam. 2019. "A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future?" Nutrients 11, no. 2: 387. https://doi.org/10.3390/nu11020387
APA StyleMonzani, A., Ricotti, R., Caputo, M., Solito, A., Archero, F., Bellone, S., & Prodam, F. (2019). A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future? Nutrients, 11(2), 387. https://doi.org/10.3390/nu11020387